Article Text

Abstract
Objectives Effective policies are an important tool for reducing tobacco use. We examine student perceptions of the existing no-smoking policy in the country’s largest national university and identify perceived barriers to its implementation. We explore student support for a 100% tobacco-free campus policy.
Design We conducted a cross-sectional survey using a self-administered on-line questionnaire.
Setting This study was conducted at Qatar University (QU), the largest national institution of higher education in Qatar.
Participants A total of 199 students participated out of a stratified random sample of students aged ≥18 years with active registration in the Spring 2020 semester.
Primary and secondary outcome measures We assessed students’ knowledge of and attitudes towards QU’s current no-smoking policy, the perceived barriers to its implementation, and support for a 100% tobacco-free policy.
Results Only 26% (95% CI 19.97 to 32.03) and 16.6% (95% CI 11.70 to 22.49) of respondents correctly identified the current policy on traditional and electronic cigarettes, respectively. Less than 30% of respondents held positive attitudes towards policy enforcement, and more male respondents reported positive attitudes towards compliance than women. Support for a 100% tobacco-free policy was at 77.2%, but it was significantly lower among tobacco users compared with non-users (35.9% and 91.8%, respectively; p<0.001). Failure to establish clear penalties, opposition from smoking students, and lack of cessation services were perceived as major barriers to implementation.
Conclusions Clear and comprehensive tobacco-free policies are important tools for creating environments conducive to rejecting smoking and seeking cessation support. The findings underscore the need to increase awareness about the policy, advocate for clear penalties for violations, and promote cessation services on campus. Qualitative research is needed to further understand perceived barriers to successful enforcement of the policy.
- health & safety
- health policy
- public health
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is one of very few studies in the region that focus on structural public health interventions addressing tobacco use among youth, who form a large segment of the population in the Eastern Mediterranean Region.
A stratified random sample was drawn from students of the largest national university in Qatar, which offers good representation of the target population despite a low response rate.
Using an anonymous self-administered questionnaire is likely to reduce social desirability bias.
The response rate in the study was characteristically low for internet-based questionnaires of college students.
The study did not include university faculty and staff.
Introduction
The tobacco epidemic is one of the greatest threats to public health worldwide.1 According to the WHO global report on trends of tobacco smoking 2000–2025, one-fifth (19.9%) of youth aged 15 years and older are tobacco smokers (33.7% males and 6.2% females).2 Tobacco consumption leads to psychological addiction3 and increases the risk of cardiovascular and respiratory diseases, diabetes and cancer.4 Annually, eight million individuals die worldwide because of tobacco use, including more than seven million deaths caused by direct tobacco use and 1.2 million deaths caused by exposure to either secondhand smoke (ie, smoke from burning tobacco products) or the smoke exhaled by a smoker.1
Individuals between the ages of 15 and 29 account for roughly 30% of the population of the Middle East and North Africa.5 The Eastern Mediterranean Region (EMR) is one of the fastest-growing consumers of tobacco products worldwide. By 2025, tobacco use prevalence will increase by 25% compared with other regions like Europe, Asia and North America.6 In addition to the high prevalence of cigarette smoking in the Middle East, new tobacco products are on the rise, including waterpipe smoking and electronic cigarettes.7 8
Tobacco use among university students is a significant public health problem in the EMR. In Lebanon, one study found that 40% of private and public university students were tobacco smokers.9 Similarly, a recent systematic review of smoking prevalence among university students in 12 Arab countries found high rates of smoking among students, especially in Egypt (46.7%), Kuwait (46%) and Saudi Arabia (42.3%).10 In contrast, tobacco use among university students in the USA for example was estimated at 14.3%.11
Tobacco-free campus policies: student attitudes and barriers to implementation
Smoke-free policies reduce tobacco product use among youth.12 Within university campuses, they have a positive impact on health and are associated with lower smoking rates among students,13 reduced secondhand smoke exposure, increased socialisation, and fewer cigarette butts on campuses.14 15 Globally, several universities have implemented smoke-free policies within their campuses, including universities in the USA, Australia, Canada and the UK.16–19 However, very few campuses in the EMR seem to have such policies, and they are difficult to identify. In 2008, the American University of Beirut in Lebanon implemented a no-smoking policy across all campus areas (including student residence halls and campus buildings), except private faculty residences, and smoking was restricted to designated areas.20 King Saud University, which is one of the largest universities in Saudi Arabia, implemented the Totally Smoke Free University Campus Policy.21 However information on the existence and implementation of such policies is not readily available from other university campuses.
Understanding student attitudes is essential for the successful implementation and effectiveness of campus tobacco-free policies.17 22 23 In one study in Australia, many participating students reported that smokers were unlikely to comply with no-smoking policies on campus and that penalties were needed.24 In another study, both smoking and non-smoking students held positive attitudes toward the enforcement of a no-smoking policy on campus, but most of the smoking respondents were concerned about creating a completely smoke-free campus and had a strong preference for designated areas where smoking would be permitted.17 In a study conducted among the students of the University of Birmingham, non-smoking students held more positive attitudes toward the tobacco cessation support and control services that were available on campus than smoking students did.25
Barriers to the successful implementation of smoke-free policies on campus include students’ lack of awareness about such policies, familiarity with policy boundaries,22 perceptions of their role in policy enforcement, student and staff beliefs that smoking is not a significant issue, opposition from smokers, and campus officials’ unwillingness to protect student and staff health.24 In addition, students consider lack of support from the university administration and staff members and the unavailability of tobacco cessation services to be barriers.24 26 Understanding barriers in the EMR is important for promoting effective tobacco-free policies among its youth.
Tobacco use in Qatar
Qatar is a state in the Arabian Gulf with a population of 2 878 506, of whom 12% are aged 15–24.27 The Global Adult Tobacco Survey (GATS)Qatar 2013 found that 12.6% of adults in Qatar were tobacco users. Non-Qatari men were more likely to use tobacco than Qatari men, and approximately 15% of tobacco users had at least a college education.28 Of tobacco users, 3.4 %, 0.7 % and <1% were shisha tobacco, smokeless tobacco and e-cigarette users, respectively. Between 2003 and 2014, smoking prevalence and cigarette accessibility and availability increased among Qatari youth.29 However, recent findings from theGlobal Youth Tobacco Survey 2018 show a slight decline in current tobacco smoking from 12.3% in 2013 to 10.8% among 13–15 year olds.30 The antitobacco legislation in Qatar prohibits smoking in enclosed public places (eg, vehicles, schools, hospitals, government institutions and restaurants) in accordance with the WHO Framework Convention on Tobacco Control that was signed in 2002.28
No-smoking policies at Qatar University
Qatar University (QU) is the oldest and largest national institution of higher education in Qatar. It has approximately 20 000 students (with 15 350 woemn students and 4264 men students registered for Spring 2020 semester) and over 1000 national and international faculty members. In 2013, QU enforced a no-smoking policy to which all faculty members, students, employees, and visitors were required to adhere. This policy prohibits smoking in university buildings, indoor and outdoor environments, and vehicles, and ‘No Smoking’ signs were hung at the entrance of each building. Smoking is allowed in designated areas, which are located at least 7.6 m away from QU buildings and have proper cigarette receptacles. Students can find a description of this policy in their handbooks, including penalties for violation. Smoking inside campus facilities is included under ‘category 2 non-academic violations’, the penalties for which can range from a written warning to expulsion from the University, at the discretion of the judicial committee (http://www.qu.edu.qa/static_file/qu/students/documents/Undergraduate-Student-Catalog-2020-2021-English.pdf).
The American Nonsmokers’ Rights Foundation provides a model for smoke-free and tobacco-free policies. Elements of a model policy include clear and detailed definition of terms, the need to remove any areas where tobacco use is allowed on campus, a clear statement on promotion and sponsorship policy, wide dissemination of the policy, and a clear statement of violations specific to smoke- and tobacco-use (https://no-smoke.org/model-policy-for-a-tobacco-free-college-university/). The current QU no-smoking policy allows smoking in designated areas, and the penalties for smoking-specific violations in the student handbook are not clear. It is noteworthy that the University is currently in the process of updating its no-smoking policy, but the new policy has not yet been approved.
In 2019, QU joined the fifth cohort of the Tobacco Free Generation Campus Initiative, which is a programme by the American Cancer Society’s Tobacco Control Center providing grants to ‘accelerate and expand the adoption and implementation of 100% smoke- and tobacco-free policies on college and university campuses across the nation’. (https://www.cancer.org/health-care-professionals/center-for-tobacco-control/tobacco-free-generation-initative.html). QU is the first and only international organisation to join this cohort, with the aim of moving towards a 100% smoke-free and tobacco-free campus. In the context of this award, we set out to assess students’ knowledge and attitudes towards the existing policy to facilitate the promotion of a new policy that would ban all forms of tobacco on campus and strengthen the provision of cessation support services.
To date, most tobacco use studies from the region have focused on individual behaviour change and health education efforts, with few attempts to address structural interventions creating and sustaining environments for healthy behaviours. This is the first study to focus on systemic interventions, especially among university students. There is no available information about the level of compliance with QU policy and the rate of reported violations among QU students. The purpose of this study is to examine student perceptions of the current No Smoking policy and the perceived barriers to implementation on campus. Specifically, this study aimed to examine (1) student knowledge about the policy, (2) student attitudes towards compliance and enforcement of the existing policy, (3) the perceived barriers to implementation and (4) the extent to which students support a 100% tobacco-free, smoke-free and vape-free campus policy.
Methods
This cross-sectional study was conducted as a part of a larger project titled, “Informed by the bio-ecological model: A cross-sectional study to assess factors shaping tobacco product use among university students.” A stratified random sample of QU students (men and women, Qatari and non-Qatari, age ≥18 years, with active registration in the Spring 2020 semester) completed an online self-administered questionnaire. The required sample size (741) was calculated using Cochran’s formula31 (95% confidence level, 2.5% margin of error and cigarette smoking prevalence=14 %, as reported in a previous study).32
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research
Data collection
Data were collected anonymously using an online self-administered questionnaire, available to students in English and Arabic versions. The participants were selected using a stratified random sample. Students were grouped into four strata based on their nationality and gender (Qatari men, non-Qatari men, Qatari women, and non-Qatari women). An introductory email, including a consent form, was sent to the institutional email addresses of students. In anticipation of the very low response rates that characterise internet-based survey, questionnaires were sent to 9807 addresses from the University’s Institutional Research and Analytic Department. A reminder was sent once a week for 4 weeks. Participation was voluntary. Students were assured of the confidentiality of their responses and reminded that they could skip questions they did not wish to answer or withdraw their participation at any time.
Overview of the questionnaire
The literature on smoke-free university policies was reviewed to identify measurement items. The questionnaire was adapted from the GATS Qatar 2013,28 American Cancer Society Tobacco-Free Generation Campus Initiative: Cohort 5 Student Survey (2020–2021),33 QU’s no-smoking policy, and a validated questionnaire from an Australian study.24 The questionnaire was translated into Arabic by a research group, which consisted of QU public health students and faculty members. To evaluate item clarity and effectiveness, both versions were pretested on a group of public health students.
The questionnaire consisted of five sections: sociodemographic characteristics and smoking status, knowledge about the QU no-smoking policy, attitudes toward compliance and enforcement of the policy on campus, perceptions toward the quit support provided by QU, and the perceived barriers to implementation of the no-smoking policy. Questions on perceptions toward the quit support returned many missing values and were excluded from the analysis of results.
Study variables
This study examined tobacco use among students, as well as their knowledge about the University’s existing no-smoking policy, their attitudes toward policy implementation, the perceived barriers to implementation, and the extent of student support for a 100% tobacco-free policy.
Tobacco use was ascertained using the question “Do you currently use any tobacco product? This includes traditional cigarettes, e-cigarettes and other electronic vapor products, chewable tobacco, waterpipe/shisha?” with a ‘yes/no’ response option. Smoking among family members and close friends was ascertained by the question “Which of the following statements is true: My father is a current smoker; My mother is a current smoker; One or more of my siblings is a smoker; I have at least one close friend who smokes; No one in my family is a smoker; None of my close friends is a smoker.” Knowledge about the existing policy was measured using questions on whether and/or where traditional cigarettes and electronic cigarettes/ other electronic vapour products were allowed on campus: indoors; outdoors in specific locations, and an option of ‘don’t know’. Attitudes toward policy implementation in QU were assessed using eight statements, including two direct questions on perceptions of compliance and enforcement: “To what extent do people comply with the current campus tobacco product use policy on QU campus?” and “In your opinion, to what extent is the current tobacco product use policy enforced on QU campus?”, respectively. The response options for those questions were: ‘totally/ mostly/ somewhat/ not at all/ don’t know.’ Perceived barriers to policy implementation were examined using nine opinion statements, including the statement “Smoke-free policy is followed by students and staff members at QU” with five response options ranging from ‘strongly agree’ to ‘strongly disagree’. Finally, support for a 100% tobacco-free and smoke-free campus was assessed using the question: “To what extent do you support your campus becoming 100% smoke-free, tobacco-free, and vape-free, with all tobacco product use prohibited on campus?” with response options including: “strongly agree, moderately agree, neutral, moderately disagree, and strongly disagree.”
Statistical analysis
Data were analysed using the Statistical Package for the Social Sciences (SPSS) V.26. Descriptive statistics were computed to examine the categorical variables (eg, demographic characteristics, knowledge, attitudes and perceived barriers). Responses from colleges with less than 30 participants were grouped together. Responses from health-related colleges (Health Sciences, Medicine, Pharmacy and Dental Medicine) were combined under one category, QU Health (table 1). Participants’ attitudes toward No Smoking policy implementation on QU campus were examined by conducting descriptive analysis (table 2).
Socio-demographic characteristics and tobacco use of participants (N=199)
Participants’ attitudes towards ‘No Smoking’ policy implementation on Qatar University (QU) campus.
Due to the small number of observations in some cells, Fisher’s Exact test was used to examine bivariate associations. Results with p<0.05 were considered to be statistically significant. For the analysis of bivariate associations between attitude statements and sociodemographic and tobacco product use (table 3), the ‘totally’ and ‘mostly’ response options were combined into a single category. For the bivariate associations between support for a 100% tobacco-free policy and gender and tobacco use, the response options for ‘strongly agree’ and ‘moderately agree’ were combined into one category, and ‘strongly disagree’ and ‘moderately disagree’ were also combined. The neutral responses were dropped from table 4 due to the small number of respondents.
Association between participants’ sociodemographic characteristics, tobacco use, and their attitudes towards policy compliance and enforcement
Support for a 100% tobacco-free and smoke-free campus by gender and current tobacco use*
Results
The response rate in the study was 2% (199 respondents out of 9807 surveys sent). Approximately half of the respondents (48.2%) reported that they had at least one close friend who smokes, while less than one third (29.6%) reported that there were no smokers among their family members or close friends (table 1). Of the respondents themselves, approximately a quarter (25.6%) reported being current smokers, with fewer women reporting smoking, although the difference was not statistically significant (32.4% and 21.6%, respectively; p=0.096). Among students who reported using tobacco products, waterpipe/shisha, traditional cigarettes, and electronic cigarettes were the most commonly used types, respectively.
Knowledge of the no-smoking policy
Responses revealed a gap in student knowledge of the existing no-smoking policy (figure 1). Approximately, a quarter of the respondents (24.1 %) were unaware that the university had a no-smoking policy related to traditional cigarettes, and a third of respondents (33.7%) were unaware that there was a no-smoking policy related to electronic cigarettes. Only 26% reported correctly that the current no-smoking policy prohibits indoor smoking and allows outdoor smoking in specific campus locations.

Participants’ knowledge of current Qatar University policy on traditional and electronic cigarettes.
Attitudes toward policy compliance and enforcement
Only 32.3% of the respondents held positive attitudes toward the level of policy compliance on campus, reporting that people totally or mostly complied with current smoking policy on QU campus, and more than 35% were unsure about the level of compliance (table 2). Approximately half of the respondents (56 %) reported that they had never or only rarely been exposed to secondhand smoke on campus, and almost 80% reported the same regarding exposure to secondhand vapour from electronic vapour products. However, they considered exposure to secondhand smoke (47.6 %) and vapour (31.5 %) to be a cause for concern.
With regard to policy enforcement, only 25.6% of respondents held positive attitudes towards the extent of policy enforcement on campus. Over half of the respondents (57.8 %) agreed that it was QU’s responsibility to reduce the risk of tobacco addiction by implementing policies that discourage tobacco use on campus. Approximately 75% of respondents agreed (strongly or somewhat) that it was QU’s responsibility to implement policies that ensure that individuals inhale smoke- and vapor-free air within the campus.
Factors associated with attitudes towards policy implementation
Attitudes towards policy compliance were significantly associated with gender in the bivariate analysis (table 3). Female respondents (45.7 %) tended to be unaware of the level of policy compliance on campus, and male respondents (35.4 %) were more likely to report that there was totally/mostly compliance with the policy (p<0.001).
Attitudes towards policy enforcement were significantly associated with gender and with tobacco use in the bivariate analysis, where 29.2% of male respondents reported that the policy was totally or mostly enforced, while over one half of female respondents (51.5%) did not know the extent to which the policy was enforced (p=0.003). One-third (34.8%) of tobacco users reported that the policy was totally or mostly enforced, while 47.5% of non-users reported not knowing the extent of policy enforcement on campus (p=0.020).
Perceived barriers to policy implementation
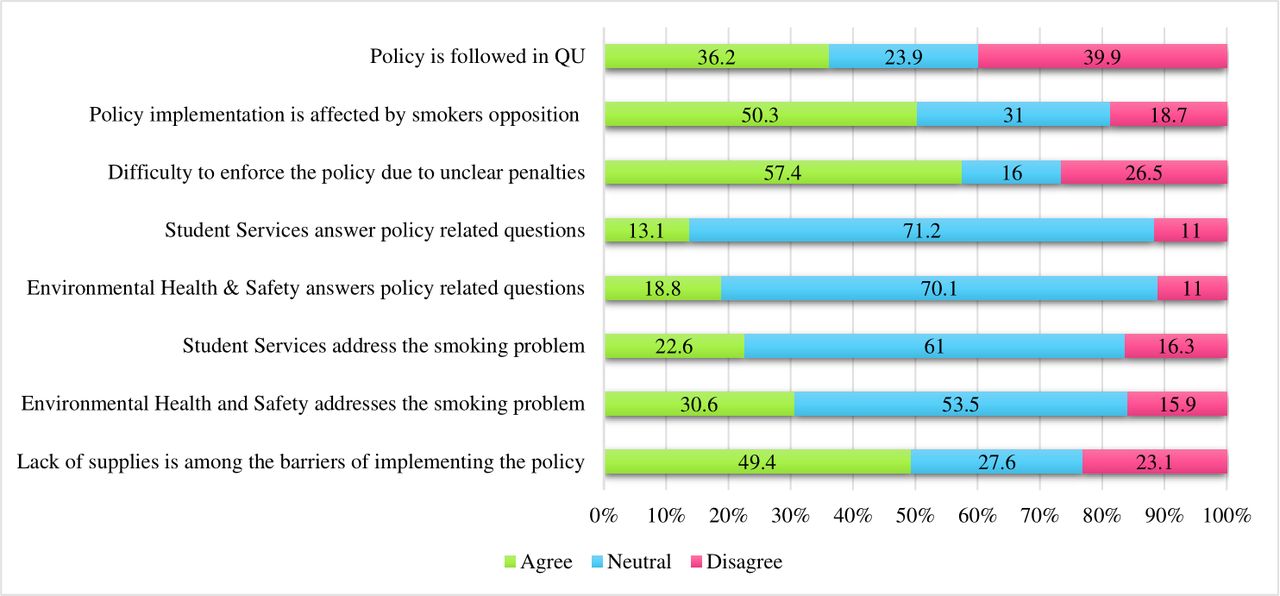
In the context of perception of barriers to policy implementation, approximately 40% of the respondents disagreed with the claim that QU students and staff members had been adhering to the smoke-free policy, and 57. 4% agreed that it would be difficult to enforce the smoke-free policy because there were no clear penalties for violations. They also considered opposition from smoking students and staff members (50.3 %) and a lack of resources such as no-smoking signs and cigarette receptacles (49.4 %) to be barriers to implementation (figure 2).
{kind=link}
{kind=link}
Participants’ perception of barriers of policy implementation on Qatar University (QU) campus.
Support for a 100% tobacco-free and smoke-free campus
When asked about the extent of support for a policy that would make QU a 100% tobacco-free, smoke-free, and vape-free campus, 77.2% of respondents said they strongly or moderately agreed with the policy (table 4). Support for such a policy was not significantly associated with gender, but it was significantly associated with the use of tobacco products. Students who reported using tobacco products expressed much less support compared with non-users (35.9% and 91.8%, respectively; p<0.001).
Discussion
The study examined the knowledge and attitudes of students towards the no-smoking policy of the largest national university in Qatar. Awareness about no-smoking policies is essential to compliance within campuses.34 In this study, only 25.6% of respondents were aware of the current QU policy regarding the use of traditional cigarettes. Approximately one third of the students were unaware that the policy addressed electronic cigarettes and other vapour products, and over one third of respondents were unaware or unsure of the extent of compliance with the policy or its enforcement on campus. These results indicate a significant gap in awareness of the policy’s existence and scope, which in turn implies the need for wider and more visible dissemination.
Gender was significantly associated with attitudes towards policy compliance and enforcement in the bivariate analysis. Female respondents were less likely to report tobacco use (21.6 %) compared with male respondents (32.4%), although the difference was not statistically significant. Nevertheless, the lower prevalence of reported tobacco use among women may reflect both the lower prevalence of smoking among women seen nationally or the social stigma associated with women smoking in the Arab region generally. The social stigma of female tobacco use may lead women to underreport the behaviour despite assurances of the confidentiality of the survey responses.35 Another possible indication of the effect of social stigma is the finding that the majority of female respondents who reported using tobacco in this survey said that they did not do so on campus (67% of women compared with 17% of men tobacco users, data not shown). However, this finding could also be due to waterpipe being the most common tobacco product used among women, which is not a product that can be used on campus.
Tobacco use was also significantly associated with views on compliance with and enforcement of the current no-smoking policy on campus. Students who reported not using tobacco reported not being aware of the extent to which students complied with the policy or to which the policy was enforced. These responses may be due to not coming up against enforcement issues themselves. On the other hand, tobacco users were more likely to perceive compliance and enforcement levels to be high on compliance compared with non-users.
Approximately 40% of the participants disagreed with the claim that QU staff members and students had been adhering to the no-smoking policy. They considered the opposition from smoking students and staff members (50.3 %) and a lack of clear penalties for policy enforcement (57.4 %) to be barriers to policy implementation. Guillaumier et al found that a higher number of students (when compared with staff members) believed that smokers were unlikely to follow the policy, and they underscored the need for staff enforcement and penalties for policy violations.24
Almost 50% of our participants considered a lack of resources such as no-smoking signs and cigarette receptacles to be barriers. Such signs promote self-enforcement, serve as a reminder of smoke-free policies, and are a strong determinant of indoor smoking.36 37 A small proportion of respondents reported that student services or Environmental Health and Safety answered questions about the policy. Almost 70% of respondents were ‘neutral’ on these questions, likely reflecting lack of information about the existence of the policy and the need for its further dissemination. Harbison and Whitman also found that most of their participants considered a lack of support from their university administration and staff members to be a barrier to the implementation of smoke-free policies.26
Support for a 100% tobacco-free, smoke-free, and vape-free policy was high, at 77.2%. The proportion supporting such a policy is in line with the proportion who believed that it was the University’s responsibility to implement policies that provide a smoke-free and vape-free environment to students on campus (75%). Consistent with the literature on the factors that shape support for smoke-free policies, tobacco use was a significant determinant.38 Students who reported using tobacco were considerably less supportive of a 100% tobacco-free, smoke-free and vape-free campus policy. This finding points to the importance of providing much greater access to cessation support services in order to assist current tobacco users and to focus on them in health education and counselling more effectively. As the University is developing an updated policy on tobacco, the findings will also be useful for reporting on baseline support as well as the factors associated with attitudes towards policy and compliance.
Strengths
This is the first study in the Arab region to focus on systemic interventions against tobacco use, rather than individual behaviour change, especially in this segment of the population. The probability-based sample was drawn from the student body of the largest national institution of higher education, which is a good representative of the broader population of this age group. Findings of this study can be helpful across institutions of higher education to ensure effectiveness of written policies. Despite the small sample size, the study will provide baseline information and enrich the literature regarding students’ perception of tobacco product use policy and the barriers of policy implementation on university campuses in the region. The findings point to the importance of raising awareness of existing policies. They also highlight the importance of understanding students’ perceptions of policy implementation (compliance and enforcement) to support formulating and disseminating effective policies that address the totality of tobacco use. The findings underscore the gaps in the existing smoking prohibition policy, which fails to address the use of other tobacco products such as electronic cigarettes and other vaping products. Another strength of this study, is the stratified random sampling strategy followed.
Limitations
The main limitation of the study is the low response rate, which is not unusual for campus studies using online questionnaires. Due to the low response rate, associations could not be examined in multivariate models. Responses may also have been affected by social desirability bias, despite assurances of the confidentiality of responses. The wording of the questions assessing prevalence of smoking may have led to underestimation of the prevalence of smoking in this study, as infrequent smokers or those who identify themselves as non-smokers may have answered the question ‘Do you currently use any tobacco product?’ in the negative. Finally, the study did not include staff members, who are also important stakeholders in this policy and whose views on compliance and enforcement should be ascertained.
Implications
Our study provides evidence for the need of education, advocacy efforts and policy modifications. The findings suggest a need to promote knowledge of the policy among students, faculty and staff. Advocacy efforts are needed to promote cessation services by the QU health centre on campus, availability of resources such as ashtrays and smoking signage, and clear penalties for policy enforcement. The findings also suggest planning for awareness campaigns to enhance knowledge of health impact of electronic/vaping tobacco products among students.
Future research should use a larger sample size and assess attitudes of faculty and staff in regard to policy implementation and barriers. Further, a qualitative study can be conducted to explore barriers to seeking/attending cessation services at QU, which may range from issues of availability (as we found in our study) and information about available services to issues of social stigma.
Conclusion
QU students possessed limited knowledge about the no-smoking policy. Female undergraduate students and non-smokers tended to be less aware of the level of policy compliance and enforcement on campus than male smokers, who reported positive attitudes. Failure to establish clear penalties, opposition from smokers, and a lack of resources were found to have hindered policy compliance and enforcement within the campus.
Educational campaigns should be conducted and messages should be posted on social media platforms to create awareness about the no-smoking policy. To improve compliance, strict enforcement should be undertaken and clear penalties should be established. Advocacy for policy improvement, cessation support and resources will reduce smoking within the QU campus.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
The study was reviewed and approved by the Qatar University Institutional Review Board (Research Ethics Approval No is QU-IRB 1188 E-2019).
Acknowledgments
We acknowledge the support provided by the Institutional Research and Analytic Department at Qatar University in the sampling and data collection process.
Open Access funding provided by the Qatar National Library.
References
Footnotes
Contributors GFA-J: conceptualisation of the study, questionnaire design, proposal and IRB writer/ approval recipient of the larger project which this study is part of, sampling design and data collection, statistical analysis and manuscript drafting. RK: questionnaire design, statistical analysis, and manuscript drafting. SA, HAL-K and AJA (public health students): statistical analysis and manuscript drafting supervised by GFA-J. HFAR: grant writer/recipient; conceptualisation; questionnaire design, manuscript drafting; critical review, and response to reviewers.
Funding This work was supported by the American Cancer Society Tobacco-Free Generation Campus Initiative Grant (ACS # 64331).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.