Article Text

Abstract
Objective Hearing impairments (HIs) that progress or have later onset may have specific effects on language and cognitive development, but are difficult to suspect during routine primary care visits. Family concern regarding hearing is thought to represent an important risk factor requiring audiological examination. Yet it is not clear how successful parents are in recognising the consequences or specific suspect elements of HI in young children. The aim of this study is to verify whether parents of at-risk children recognise the presence of HI through a parental questionnaire that draws attention to auditory skills development and compares them with language and communication skills.
Design Observational study.
Setting From 2013 to 2019, parents were administered the Questionnaire on Hearing and Communication Abilities before audiological evaluation of their children at a secondary care institute.
Participants 309 Italian children (1–36 months old) at risk of HI.
Primary and secondary outcome measures Questionnaire sensitivity in predicting the presence and type of HI.
Results Parents report a decrease in auditory skills for children with sensorineural HI (Χ2(2)=14.4, p=0.003), with an increased concern expressed in 59% compared with 24% in normally hearing children. Both auditory (r=−0.18, p=0.002) and comprehension (r=−0.13, p=0.057) skills weakly but negatively correlated with a diagnosis of HI. On discriminant analysis, the positive predictive value of the questionnaire was 0.78, but with low sensitivity (0.39).
Conclusions Parents of children with a verified risk of HI have some capacity to recognise non-typical auditory behaviour. Thus, it is important to assess parental concerns during primary care health visits, and a targeted questionnaire on auditory abilities can complement existing screening procedures. However, given the low sensitivity of the questionnaire, we conclude that for a reliable detection of HIs that progress or have later onset an objective screening tool is always required.
- audiology
- paediatric otolaryngology
- primary care
Data availability statement
Data are available in a public, open access repository. Statistical code and anonymised raw data set are available from the OSF repository (https://osf.io/ex3rp/).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Parents’ recognition of age-appropriate auditory, language and communication abilities was evaluated as a possible tool for a more accurate recognition of hearing impairments that progress or have later onset.
The proposed targeted questionnaire follows in detail the developmental trajectories of the skills in question.
Children included in the study were referred for audiological assessment due to a certain risk of hearing impairment, which may have affected parental responses.
Due to the relatively low sample size in some of the age groups covered by the questionnaire, a more detailed analysis of the correlation between age and accuracy of parental recognition of hearing impairment was not possible.
The structure of the questionnaire only allowed for a limited analysis of the internal consistency of the questions on the questionnaire.
Introduction
Concerns have been continuously expressed in recent years regarding timely recognition of cases of hearing impairment (HI) that are not identified by universal newborn hearing screening (NHS), such as some forms of early-onset HI that are not apparent at birth or HIs that progress or have later onset.1 2 Timely recognition does do not concern only permanent sensorineural HIs. Otitis media with effusion is the most common cause of conductive HI, and although it may resolve spontaneously without complications it can be associated with prolonged HI, imposing a series of disadvantages on hearing sensitivity.3 Although several attempts have been made to introduce secondary screening to primary care health centres,4 5 most countries still lack an effective and affordable protocol for identification of children at risk of permanent or prolonged HI occurring after birth.6 To address this issue, the Joint Committee on Infant Hearing has identified a series of risk indicators that should prompt continued monitoring of hearing status, even if the NHS results were normal, emphasising that ‘family/caregiver concern regarding hearing, speech, language, or developmental delay and or developmental regression’ could represent the main alarming risk factor requiring a prompt referral to audiological services.2 7 Yet the ways in which to highlight a real concern are not well defined, and parents/caregivers may not easily understand what the specific suspect elements of HI are. Therefore, a questionnaire that would draw attention to children’s auditory skills could represent a focal point for parents/caregivers.
A variety of questionnaires have been developed for caregivers or primary care professionals to use to investigate communication and language development in normally developing children.8 Others were developed to assess aural/oral performance mainly in children with hearing devices.9–12 For at least one of them, the Parents’ Evaluation of Aural/Oral Performance of Children (PEACH) Questionnaire, normative data were obtained for both children with HI and children with normal hearing (NH) in various languages,11–15 and it could therefore be also used for general purpose evaluation of hearing function in children, even though not intended as a screening tool to classify children with NH or hearing loss. Few isolated attempts were made to create questionnaires for parents to specifically evaluate hearing sensitivity and function in normally developing preschool children in order to identify children with speech-language and/or auditory impairment.16–18 These questionnaires were proposed as a low-cost screening tool to complement NHS. All mentioned questionnaires covered a relatively large age span without specific focus on the developmental course of auditory and language skills in the first years of life. Thus, a parental questionnaire, validated on a large sample, that would successfully complement NHS in identifying HIs that progress or have later onset, while taking into account the developmental course of speech-language and auditory skills in the first years of life, remains unavailable.
Here we present an observational analysis of parental assessment of auditory skills obtained through the Questionnaire on Hearing and Communication Abilities (QUAC), a structured questionnaire in Italian language for parents/caregivers of children between 1 and 36 months of age, adapted for various developmental stages and consisting of four scales representing four categories of skills: auditory skills (scale A), comprehension (scale C), production (scale P) and interaction (scale I). The questionnaire was proposed to parents/caregivers of children who underwent audiological diagnostic procedures based on various postnatal risk factors.
The main goal of the analysis was to establish whether parental assessment of auditory skills correlates with age-appropriate hearing abilities, whether it serves as a significant predictor of the presence of HI, and to which extent HI affects other skills (production, comprehension and (verbal and non-verbal) interaction). We hypothesised that parents/caregivers are attentive to their children’s auditory, language and communication skills, even more when a risk has already been raised though the postnatal risk assessment.
Methods
Study population
From 2013 until 2019, the QUAC was administered to parents of children examined at the otorhinolaryngology and audiology unit of a medical institute in Italy as part of a comprehensive audiological assessment. Children were born predominantly to families from the north-eastern provinces of Italy, with a variable sociocultural background. In total, 309 individual children aged 1–36 months (1–9 months: 137 children with NH and 33 with HI; 10–36 months: 87 children with NH and 52 with HI) who had completed both a comprehensive audiological examination and the parental questionnaire were included in the study. Children were referred for audiological evaluation for different reasons: 92 (29.8%) were further examined following the refer at the NHS, 104 (33.6%) due to medical concerns or risk factors reported at birth during recovery at the neonatology and neonatal intensive care unit, and 65 (21%) children were examined based on medical concerns or risk factors reported by their family paediatricians or educators. A relatively large number of children (50, 15.5%) were accepted after missing the NHS (because they were born at home or adopted from a non-European country). The distribution of reasons for accessing audiological services by presence or absence of HI is presented in Table 1.
Sample overview by age and reasons for accessing audiological examination
Testing procedure
All children received a diagnosis of their hearing status at the otorhinolaryngology and audiology unit. The final diagnosis of hearing status was obtained by cross-matching the results of otoscopy and objective and/or behavioural measurements of air and bone conduction hearing threshold. Hearing was categorised into six degrees—NH, unilateral HI, mild bilateral HI (30–40 dB), moderate bilateral HI (40–60 dB), moderate-severe bilateral HI (60–70 dB) and severe bilateral HI (>70 dB)—based on the average hearing threshold of the best ear in bilateral HI. The type of HI, a temporary/conductive (=1) or a permanent/sensorineural (=2) HI, was diagnosed as well, compared with NH (=0). The QUAC was compiled by the parents/caregivers in a quiet room of the outpatient clinic after or during the audiological assessment but before the final diagnosis was issued. Only the results of their first visit were included. A hearing technician or a speech therapist helped clarify the questions if needed.
The QUAC was composed by the audiologists, psychologists and speech therapists working at the otorhinolaryngology and audiology unit. The original language of the questionnaire is in Italian. The questionnaire, along with an English translation, is available in online supplemental files A1 and A2. The questionnaire is divided into 10 age ranges, and the total number of questions varies from 2 to 11 depending on the age range. The questions for each scale were based on the normal progression of children’s abilities in each age range (the list of the references that were used to create age-appropriate questions for each age range is available in online supplemental file A3). Infants younger than 2 months received only two questions (scale A), infants aged 2–9 months old received six to eight questions on auditory skills, production (scale P) and interaction (scale I), while older infants received questions from all four scales. Because of these differences, we separately analysed the results for infants younger than 10 months and for older children. The internal consistency of the questions in scale A per each age group was evaluated by calculating the Cronbach’s alpha. For other scales, calculating the internal consistency was not possible due to the low the number of questions per scale (1–3). Coefficients of ≥0.70 were considered to indicate good internal consistency.19 20 Parents responded with ‘always’, ‘sometimes’ or ‘never’, coded as 3, 2 and 1, respectively. The answers to each scale of questions were summed and normalised (transformed into proportions of maximum score). Each parent/caregiver was also asked to provide an overall estimate of the child’s hearing ability by answering the final question: ‘Do you think that your child can hear?’ The answers are coded as the following: 1=‘yes’, 0.5=‘I don’t know’ and 0=‘no’.
Supplemental material
Supplemental material
Supplemental material
Parents were informed about the use of clinical data for research purposes and gave their written consent to participate before the assessment.
Patient and public involvement
Before the start of the study, the questionnaire was piloted to parents and caregivers of various socioeconomic backgrounds to identify comprehension or intelligibility difficulties. Misinterpreted questions were corrected. The research and preliminary results have been presented and discussed at regional and national courses and conventions for speech pathologists, paediatricians and families of children with HI (national convention for paediatricians and interested public, ‘Per sentire, percorsi di intervento precoce in audiologia pediatrica’, September 2016; public courses for speech pathologists, ‘Sentire bene per comunicare meglio’, at the Institute for Maternal and Child Health - IRCCS “Burlo Garofolo” - Trieste, November 2018 and March and November 2019).
Data analysis
Statistical analyses were performed using R programming language. Shapiro-Wilk normality test was used to determine the normality of the variable distribution. Due to the unequal sample size and the non-normal distribution of scores of each scale of the questionnaire, we compared the scores based on the presence and type of HI using non-parametric Kruskal-Wallis test, with Wilcoxon’s test for post-hoc comparisons. Additionally, Spearman’s correlation coefficients were computed for multiple correlations between the variables of interest. The level of significance was set at 0.05. The linear discriminant analysis (LDA) technique was used to explore the ability of the questionnaire to classify a child as having HI or not, with separate analyses for the type of HI (sensorineural or conductive) and the age at which the analysis becomes a relatively reliable tool to recognise children with HI. The Bartlett’s test of homogeneity of covariance matrices showed that the variances of the questionnaire scales of subsets with and without HI were equal for all but the comprehension scale (where Bartlett’s K-squared (1)=6.997, p=0.008). We have therefore performed a set of LDAs. The quality of predictions of the LDA model can be measured through a cross-validation procedure that can measure the area under the receiver operating characteristic (ROC) curve (AUC) values of the non-parametrical ROC analysis for the overall representation of true and false positive rates at different cut-off values, based on which the optimum cut-off value for the highest sensitivity, specificity and positive predictive value (PPV) of the model can be selected. In our analysis, these measures were repetitively calculated for each LDA for randomly selected subsets of the main data set. The procedure was repeated 500 times to obtain stable results and the mean values are reported in the text. The output of the LDA with the performance closest to the mean values of the repeated procedure is reported in online supplemental file A4.
Supplemental material
Results
Of the children included in the sample, 224 were normally hearing (NH) children and 85 with mild to severe sensorineural or conductive HI. Figure 1 and Table 2 summarise the results of the questionnaire based on the type and grade of hearing loss in the final diagnosis. Figure 2 presents the results of the multiple correlations between the scores of scales A, I, C and P, the parents’ overall estimate of hearing, the estimated hearing threshold, and the type of hearing loss.
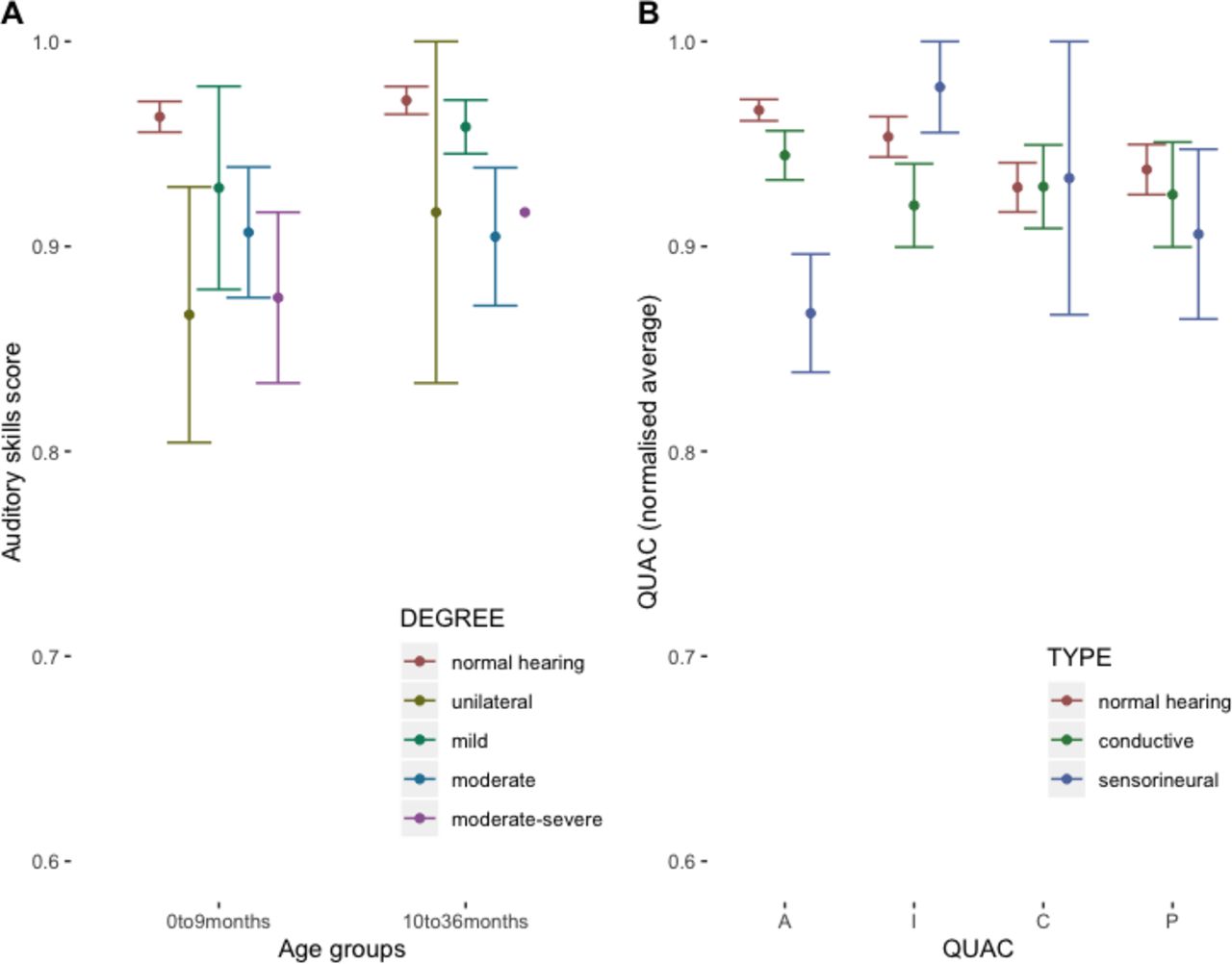
(A) Average score in auditory skills (scale A) from the questionnaire by age and degree of hearing impairment. (B) Average score in all four categories of the questionnaire (scales A, I, C and P) by age and type of hearing impairment. Error bars represent 95% CI. A, auditory scale; C, comprehension; I, interaction; P, production; QUAC, Questionnaire on Hearing and Communication Abilities.

{kind=link}
{kind=link}
Multiple correlation table. The direction of the correlation is marked with colours (blue: positive; red: negative), and the significant correlations (p<0.05) are marked with stars. A, auditory skills; C, comprehension; HI, hearing impairment; I, interaction; P, production.
Data summary by degree and type of hearing impairment
Children diagnosed with HI received significantly lower scores for auditory skills (scale A) (mean (HI=0)=0.95; mean (HI=1)=0.91; Kruskal-Wallis Χ2(1)=9.7, p=0.002) and marginally lower scores for production (scale P) (mean (HI=0)=0.76; mean (HI=1)=0.69; Kruskal-Wallis Χ2(1)=3.2, p=0.073). For auditory skills (scale A) there were significant differences between children based on the type of HI, with post-hoc comparison showing that scores in scale A were significantly lower in children with sensorineural HI (Kruskal-Wallis Χ2(2)=14.4, p=0.001), while scores in scale P were significantly lower in children with conductive HI (Kruskal-Wallis Χ2(2)=7.5, p=0.04). Multiple correlation analysis (Figure 2) showed that both scales A and C correlated with hearing threshold (scale A: r=−0.25, p<0.001; scale C: r=−0.18, p=0.025), while only scale A correlated with type of HI (scale A: r=−0.19, p=0.001) as well as with other scales of the questionnaire (scale I: r=0.19, p=0.004; scale C: r=0.33, p<0.001; scale P: r=0.13, p=0.045). Parents’ overall estimate of child’s hearing ability was significantly lower in children with HI (Χ2(1)=−0.3, p<0.001) and negatively correlated with hearing threshold (r=−0.21, p=0.001) and type of HI (r=−0.32, p<0.001). Furthermore, parents’ overall estimate did not significantly depend on any of the risk factors that led to the audiological evaluation.
To determine the sensitivity and specificity of the questionnaire in predicting the diagnostic outcome of the audiological evaluation (the presence or absence of HI), we used the LDA models. Given that scales A and C correlated with hearing threshold, values from all four scales and their potential interactions were included in the model. The best performance of the model, with 78% children correctly classified as having HI or not (PPV=0.78), was achieved at sensitivity (true positive rate) and specificity (true negative rate) scores of 0.39 and 0.93. By changing the cut-off of the model to increase correctly recognised cases with HI, the number of falsely positive cases would increase significantly. Given that the percentage of children with HI in the population is relatively low, this would, however, mean a great number of children falsely identified to be at risk of HI. The AUC for the model was 0.66, which confirms the above observation. The output of the discriminant analysis, along with the predictions of the model at various cut-off values, is available in online supplemental file A4. Discriminant analysis was also used to predict correct classification into the type of HI. While ROC analysis was not possible given that the outcome was non-binary, the best performance of the model was computed for the sensorineural HI (PPV=0.62, sensitivity=0.45, specificity=0.84) and conductive HI (PPV=0.73, sensitivity=0.32, specificity=0.9). The output of the discriminant analysis for the type of HI and the confusion table are available in online supplemental file A5.
In the discriminant analysis that included all four questionnaire outcomes, only cases with complete answers in all four categories of questions could be included. Thus, the above results include the subgroup of children older than 9 months. To verify the power of the auditory skills scores in predicting HI in younger and older infants, we ran two separate discriminant analyses for the age groups younger than 10 months and from 10 months on. None of the infants younger than 10 months was correctly classified based on the scores from auditory skills only. In the older group, the best performance was achieved at a PPV of 0.67, with specificity and sensitivity of 0.93 and 0.23; the AUC was 0.58. The number of children who underwent the first audiological evaluation drastically decreased with age, and therefore a more detailed analysis of the sensitivity of the questionnaire across age groups was not possible.
Discussion
Parental concerns expressed during regular primary care visits indicate that several types of child developmental problems can be recognised through clinical judgements based on the information provided by parents,21 and that clusters of parental worries correlate with a child’s performance in a screening evaluation.22 In other words, parents can accurately evaluate their child’s developmental trajectories, and what they evaluate and refer to as ‘strange’, ‘unexpected’ or ‘a sense that there is a problem’ is often a reliable predictor of disability.23 24 The results of the QUAC parental questionnaire partly confirm these general insights: parents’ overall scores in auditory skills decrease significantly with severity of HI and are lower especially for children with sensorineural HI. Questions on production and interaction skills concerned (verbal or non-verbal) social activities of the child and were not directly related to auditory skills, which may explain why normally developing children did not differ in their language production and interactive skills regardless of their hearing status. Parents’ recognition of difficulties in auditory and comprehension skills is important; if untreated, such difficulties could lead to developmental delay. We therefore speculated whether parental developmental concerns regarding their children’s auditory abilities could usefully be taken into consideration in overall risk assessment.
The questionnaire was originally designed to account for the fast developmental changes in the first 3 years of life and was therefore divided into 10 age groups. We hoped to be able to observe a gradual improvement in parents’ ability to recognise children’s untypical behaviour across these age groups. However, the number of children gradually decreased with age, and therefore only two larger age groups were created, while a more detailed analysis of the sensitivity of the questionnaire across the age groups was not possible. For younger infants with HI, parents in this study were not successful in detecting the decrease or change in auditory skills. This result may be related to the fact that it may be more difficult to observe the auditory responses of very young infants. Moreover, most of the young infants (95%) were brought to the centres as a routine follow-up from the screening assessment at birth, or if the screening was missed due to home labour or other factors, which could contribute to the overall lack of increased concern regarding their children’s hearing. Conversely, only 6% of young infants in the tested sample were referred for audiological evaluation as a consequence of medical or parental concern, and only one of them was subsequently diagnosed with a mild conductive HI. This also means that the established NHS programmes7 cover a vast majority of infants at risk of HI younger than 10 months.
All children included in the study were admitted to the institute due to a certain risk of HI. Therefore, parents in this study may have been overall more concerned about their children’s hearing than an unbiased random sample of parents and consequently more attentive to their auditory behaviour. Nonetheless, the majority of parents did not correctly recognise the decrease in auditory and language skills in children with HI. The discriminant analyses, built to assess the sensitivity of the questionnaire to recognise children with HI, showed that with the optimal model performance the classification of children with HI was at most 39% correct (with an overall PPV of 0.78), when all four scales from the questionnaire were included, that is, the data from children older than 9 months. While a different cut-off of the model would yield a higher percentage of correctly recognised HIs, the resulting high number of falsely selected children would confirm the unreliability of the questionnaire. Again, such results can be attributed to the young age of the participants; hearing deficit may be difficult to notice in very young children, especially if it had not (yet) caused a significant change in their behaviour. The questionnaire was designed specifically to address the skills in children younger than 3 years and we therefore lack the results in an older testing group. Previous studies assessing the sensitivity of questionnaires for children up to 18 years report an overall better ability of the tool in correctly recognising HI in children. While some lack a detailed analysis of the potential differences in sensitivity across ages,15 17 18 the validations of PEACH questionnaire similarly report a decreased sensitivity for children below 24 months.13 Therefore, one possible conclusion is that children tested with the present questionnaire are too young and that parents were thus not able to correctly assess their auditory behaviour. Another possible conclusion is that while questionnaires of this type may raise awareness of children’s auditory skills and the specific HI suspect elements and can be of assistance in assessing paediatric risk during regular primary care visits,25 they are not sensitive enough to represent a reliable diagnostic tool for recognising HIs that progress or have later onset.
With the presented targeted questionnaire, parents evaluated auditory skills significantly lower in older children with (moderate to severe) HI. Thus, the questionnaire may serve as a risk assessment tool that can detect parental developmental concerns at paediatric visits. However, the questionnaire cannot represent a reliable diagnostic tool to recognise HIs that progress or have later onset. For a reliable detection of HI in primary care units, an objective screening tool may be required.
Data availability statement
Data are available in a public, open access repository. Statistical code and anonymised raw data set are available from the OSF repository (https://osf.io/ex3rp/).
Ethics statements
Ethics approval
The study was conducted according to the 1964 WMA Helsinki Declaration and its later amendments, under the framework of the research project 17/17 approved by the institutional ethical review board, nominated by the Italian Ministry of Health (Ufficio per la Ricerca Clinica IRCCS Burlo Garofolo).
Acknowledgments
We thank Sara Pintonello, Federica Decaro, Raffaella Marchi, Pietro Cossu, Eleonora Tonon, Agnese Feresin and Sara Ghiselli for data acquisition and digitalisation of the data set, Lorenzo Monasta for statistical advice, and the parents for their participation in the study. We would also like to thank Professor Harvey Dillon for a thorough review of the manuscript. Addressing his comments significantly contributed to its quality and readability.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EO, SBa and AS wrote the manuscript. AS and SP analysed the data. EC, SBo and EO prepared the questionnaire. All authors have reviewed the content of the article and have approved the final version submitted for publication.
Funding This research received funding from the Institute for Maternal and Child Health - IRCCS 'Burlo Garofolo', Trieste, within research grant RC 17/17.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.