Article Text

Abstract
Objectives Our main objective was to describe transgender people’s reasons for consulting a general practitioner (GP) outside of transition-related issues; the secondary objective was to study the qualitative aspects of the primary care visits for this population.
Design Descriptive, cross-sectional study in France.
Setting The study questionnaire was distributed online and to healthcare centres in France.
Participants Self-identified transgender people aged 18 and older.
Primary and secondary outcomes Reasons for consulting were collected retrospectively and classified according to the International Classification of Primary Care, second edition (ICPC-2). The answers to the open-ended questions were analysed qualitatively by theme and occurrences.
Results Out of 320 respondents, 50% visited their GP for a problem unrelated to their transition, with a total of 155 reported reasons. Procedures such as prescription renewal and administrative paperwork represented 33% of the reasons to visit, followed by general symptoms (15%). Benevolence from the physician was the most important criteria for a successful consultation.
Conclusion Transgender people visit their GP for reasons either related (50%) or unrelated (50%) to transition. When unrelated, reasons appear to be similar to the reasons found in the general population. Further research and training should be developed on comprehensive primary healthcare for transgender people to provide quality patient-centred care for transgender patients.
- primary care
- general medicine (see internal medicine)
- sexual and gender disorders
Data availability statement
Data may be obtained from a third party and are not publicly available. Following the requirements of the french CNIL, data are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To the best of our knowledge, this is the first study to explore transgender people’s reasons to visit their general practitioner outside of transition-related reasons.
All aspects of the study design, especially protocol and questionnaire, were discussed with members of a local trans civil rights organisation.
Our questionnaire was distributed through trans organisations and healthcare centres to reach as many members of the trans population as possible while reducing selection bias.
Memory bias may be the main limitation of our study due to its retrospective design.
Introduction
Between 1300 and 6500 individuals self-identify as transgender in France (between 0.002% and 0.01% of the general population), that is, with a gender identity or gender expression different from the sex that they were assigned at birth. These numbers are probably underestimated: the last survey of the transgender population in France was conducted in 2009,1 and used stigmatising terms such as transexual, associated with gender-affirming surgery and no longer relevant to describe gender diversity.2
Although the visibility of the transgender community has improved over the past 10 years, transgender people still suffer from stigma and discrimination in healthcare,2–4 with an impact on their use of medical resources. In a study published in 2011 by the French organisation, Chrysalide,5 16% of the respondents were denied a medical appointment because they were transgender, 35% gave up on medical care because of the physician’s prejudices and 75% had at least once felt uncomfortable in the presence of medical staff because of their transidentity. In the Trans Mental Health and Well-being in Ireland survey conducted in 2013 by the Transgender Equality Network Ireland,6 58% of the respondents reported that general health professionals used the wrong pronouns, either on purpose or by mistake, and 16% reported hurtful or insulting language about transgender people. Although discrimination in healthcare and lack of awareness among healthcare providers on transgender-related health issues are significant barriers to access healthcare for transgender patients, other barriers include health insurance policies and public policy.7
Most studies about transgender people’s health focus on transitioning, such as gender-affirming surgery and hormone therapy. A systematic review in 20158 found that among 75 studies published since 1977 on transgender people healthcare utilisation, 60% were about surgery and 20% on endocrinology. In the surveys published by the National Institute for Health Surveillance (Institut national de veille sanitaire, InVS) and the National Institute for Health and Medical Research (Institut national de la santé et de la recherche médicale, INSERM),9 10 most of the health-related questions were about transgender people’s progression in the transition process.
Most of the medical services for transgender people are provided by specialists, although a large part could be delivered by primary care providers.11 However, the stigma faced in healthcare by transgender people also impacts their utilisation of primary care.12 On the providers’ side, some data suggest that most primary care providers are willing to provide routine healthcare for transgender patients13 but only half are willing to continue gender-affirming hormone therapy.14 Some of the providers’ attitudes are related to their knowledge of transgender issues and previous encounters with transgender people or patients.
To provide the best quality of primary care to transgender patients, it seems important to identify what transgender people expect from primary care, in terms of healthcare needs (gender-affirming related or not) and of patient-provider communication. A 2018 study found that the main health concerns of transgender individuals included sexual health, transition-related matters, reproductive health, body positivity and self-esteem, and mental health.15
The primary objective of our study was to describe transgender population’s reasons for consulting a general practitioner (GP) other than reasons related to transitioning.
The secondary objectives were to describe transgender people’s utilisation of primary healthcare, the difficulties they face and their expectations regarding their GP.
Methods
We conducted a cross-sectional study among the transgender population in France.
Study population
Because of the discrimination they face, the transgender population is very discrete, they can be described as a hidden population.16 To reach as many people as possible, we used the snowball sampling approach, which consists in asking predetermined subjects to recruit further subjects they are acquainted with among a given population. In our study, the intermediaries were trans civil rights organisations, reproductive and sexual healthcare centres (such as Planned parenthood), HIV testing centres and university preventive medicine departments. Our recruitment plan was in accordance with previously published considerations on conducting transgender studies.16
Respondents would fill in an electronic questionnaire if they met the inclusion criteria of identifying as transgender, being 18 years or older and agreeing to participate in the study.
Questionnaire
The survey was available online from 1 November 2017 to 1 February 2018.
Questions regarding reasons to visit (primary objective) were as follow: ‘Was your last visit to your GP related to transition?’ (yes/no). ‘If no, what were the reason or reasons of this visit?’ (open-ended).
The questionnaire comprised a series of close-ended multiple-choice questions on respondents’ habits with their GPs, some questions on respondents’ demographic characteristics, and two open-ended questions about the problems met during consultations with GPs and about what respondents expected of their GP.
All questions were either facultative or included a ‘No answer’ proposition, so respondents would not feel compelled to give out personal information.
A translated version of the questionnaire is available as online supplemental material.
Supplemental material
Data collection
We contacted 13 trans civil rights organisations, the reproductive and sexual healthcare centres of 170 cities, the preventive medicine departments of 55 universities and the HIV testing centres in 111 cities spread across France. For trans organisations, we first sent a message explaining our study, then we asked the organisations to share the link to our survey on their websites and social network pages. Sexual health and HIV testing centres, and university preventive medicine departments were sent by email a poster to be displayed in waiting rooms to inform patients of our study. Posters included the website link and a flashcode leading to the questionnaire. Respondents were encouraged to share the questionnaire.
The reasons for visits were sorted by three authors (MG, SO, CM-F), using the second version of the International Classification of Primary Care (ICPC-2),17 developed by the World Organization of National Colleges, Academies and Academic Associations of General Practitioners/Family Physicians (WONCA).
Patients and public involvement statement
We met with the trans civil rights organisation Chrysalide representatives to discuss our project before we started to work on the protocol. We collaborated with Chrysalide representatives for every early aspect of the study: protocol, questionnaire design and sharing, to best fit our target population’s experience. Such a collaboration with community representatives is particularly important in transgender studies, given the stigma and discrimination faced by transgender people.16
Ethics and confidentiality
The study was anonymous and informed consent was obtained from respondents after a description of the study and information on data use. Our questionnaire was hosted on LimeSurvey Professional.
Data analysis
We ran descriptive analyses for all quantitative variables. The answers to open-ended questions were analysed qualitatively, with a thematic analysis and counting of occurrences in verbatims. The thematic analysis was triangulated: two authors (MG and SO) independently analysed the answers to the open-ended questions and coded the verbatims, a third author (CM-F) was consulted when there was a disagreement.
Data statement
Data are available on request.
Results
Sociodemographic characteristics
Out of the 320 respondents, 181 (57%) identified as transfeminine and 126 (39%) identified as transmasculine. Sixty-five per cent were 40-year-old or less. The majority of respondents were either employed (27%) or students (26%). Most respondents (n=240, 75%) had a non-gender compatible social security number. The sociodemographic characteristics of the respondents are presented in table 1. Most of the respondents (n=179, 56%) heard about the study from an association, 98 (31%) from a social network and 24 (8%) from a relative.
Demographic characteristics of the study population, N=320
Most of the respondents (93%) had a GP officially declared to the French Health System. More than half of the respondents (53%) found their GP by themselves without the help of a relative or an association.
For 31% of the respondents, the last consultation took place less than a month ago, and 49% less than 6 months ago.
Reasons for consulting
For 48% of respondents, the last visit with their GP was for a transition-related issue. Reasons unrelated to transition were cited by 135 respondents with a total of 155 reasons classified according to the ICPC-2. The most frequent ICPC-2 code was Process. The 52 coded process included 19 were medical follow-ups or prescription renewals and 18 were administrative procedures. The second most frequent code section was ‘General and unspecified (A)’ symptoms (23 occurrences) such as fever, weekness/tiredness or pain. Other code sections included ‘Musculoskeletal (L)’ (18 occurrences), ‘Respiratory (S)’ (15 occurrences) and ‘Psychological (P)’ (13 occurrences). The detailed results to our primary objective are presented in table 2.
Transgender people’s reasons to visit their general practitioner on their last visit, outside of transition-related reasons, classified by their International Classification of Primary Care, second version (ICPC-2) code
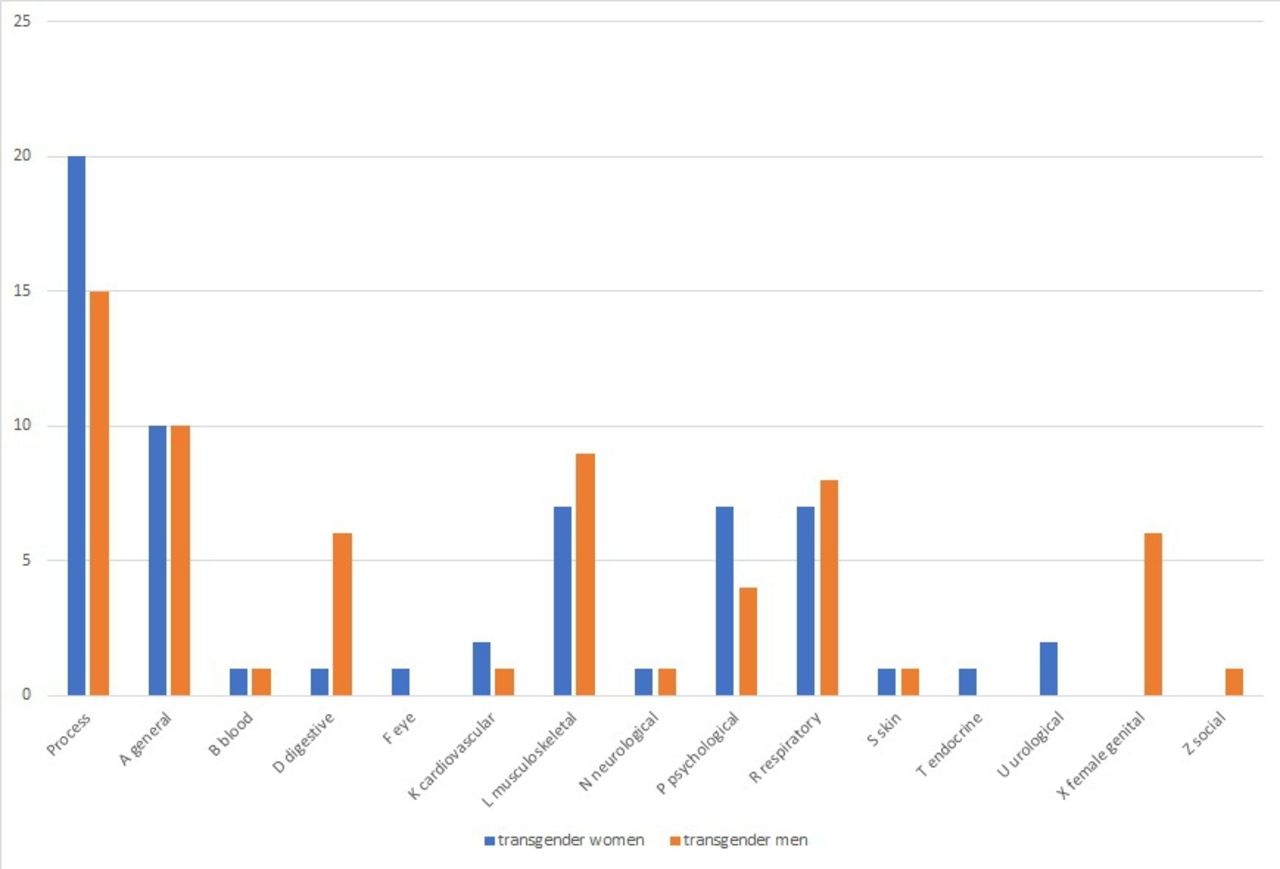
In post hoc analyses, we described reasons to visit according to age group and gender transition. Results are presented in figures 1 and 2. Numbers were too small to run comparative analyses between subgroups.

Reasons to visit by ICPC-2 code (International Classification of Primary Care) and by age group.

{kind=link}
{kind=link}
Reasons to visit by ICPC-2 code (International Classification of Primary Care) and by gender.
Transgender people’s expectations
Most respondents (43%) visited their GP as soon as they needed, 25% delayed their visit and 17% had already given up on a consultation. The main reason for postponing or waiving a consultation was apprehension of the physician’s remarks (47 occurrences among 151 entries). The second reason was financial issues (46 occurrences).
Regarding satisfaction, 53% of the respondents responded they were absolutely satisfied with the consultation, 31% that they were rather satisfied and 10% that they were rather unsatisfied. Among the respondents, 66% were addressed to using the right gender, and 27% were misgendered, although most respondents thought the misgendering was not malevolent.
Of the 320 respondents, 229 answered the open-ended question about problems they encountered during consultations at the GP’s office. The most recurring problem was misgendering, with 87 occurrences, either during the visit (54) or when making the appointment (33). Seventy-four entries were people specifying they did not meet any problem with their GP. All problems encountered are listed in table 3.
Problems encountered by transgender people when consulting in primary care
Of the 320 respondents, 248 answered the open-ended question about their views of a satisfactory consultation (table 4). Lack of judgement/benevolence was the most frequent answer (95 occurrences), before respect of their gender identity (75) and patient listening (70).
Characteristics of a satisfactory consultation for transgender people in primary care
Discussion
Main findings
We conducted a cross-sectional survey among transgender people in France to study their reasons for visiting their GP. Among the 320 respondents, 52% had last consulted their GP for a reason unrelated to gender transitioning. Among the cited reasons, the most frequent ICPC-2 codes were administrative and follow-up process and general and unspecified symptoms.
The most frequent problems encountered by respondents in primary care were misgendering and a lack of knowledge regarding transidentity from their primary care physician. But we also noted 25 occurrences of reported judgmental attitudes or inquisitiveness, and 20 occurrences when respondents were denied care or prescription because of their transidentity. In the 2011 study by Chrysalide,5 16% of the 187 respondents had been denied care because of their transidentity, and 35% had given up on some healthcare needs because of their experience of healthcare providers’ attitudes regarding transidentity. The discrimination faced by transgender people in healthcare settings can be explained in part by a lack of training of healthcare providers in gender-affirming healthcare; such a training should be included in healthcare students’ curriculum.18 However, a recent study suggests that transphobia rather than lack of training predicts providers knowledge of transgender healthcare.19 Transphobia must be addressed in society and in medical education to improve access to care for transgender people.
The inadequation of the social security number with the gender identity can be a hindrance for transgender patients, in their relationship with their GP and in the process of civil registration. In our study, 75% of respondents stated their social security number was not in accordance with their gender identity.
Strengths and limitations
To the best of our knowledge, this study is the first to explore transgender people’s reasons for consulting a GP, especially outside of transition-related problems.
Since trans civil rights organisations were our most frequent relays, we must consider a selection bias. The snowball sampling probably did not reach the people who were most isolated and precarious. However, the snowball method was the only one allowing us to reach so many people from a hidden population during a short time period. In comparison, organisation Chrysalide’s survey5 in 2011 got 187 responses, and the INSERM study in 2011 got 381 responses.10 We tried to lower the selection bias by involving sexual and university health centres but got very few responses.
Memory bias is also present due to the retrospective aspect of our study but could be limited by the fact that 80% of the respondents’ last consultation happened in the last 6 months. Desirability bias was lowered by the fact that the questionnaire was anonymous and that respondents were free not to answer any question that made them uncomfortable.
Comparison to other studies
The French Éléments de la Consultation en médecine générale (ECOGEN) study20 published in 2014 used the ICPC-2 to classify the reasons for 20 613 consultations in primary care. In ECOGEN, the most frequent code was ‘Process’: treatment renewal. Then came ‘General and unspecified’, ‘Cardiovascular’, ‘Respiratory’ and ‘Musculoskeletal’ symptoms. A statistical comparison between our results and ECOGEN’s would be difficult because of sample size difference. Moreover, the description in ECOGEN was prospective and systematic when our data collection was retrospective. The main differences in our results compared with ECOGEN’s is a lower number of Cardiovascular codes and higher number of Psychological codes. This difference could be explained in part by a difference in the age of participants: almost 20% of ECOGEN participants were over 60 years old versus 10% in our study.
In the 2007 survey9 conducted by trans organisations and HIV prevention centres, 86% of the respondents had a declared GP. They were 93% in our study. In Chrysalide’s survey,5 35% of the respondents recognised having given up on primary care because of their apprehension of the medical staff’s judgement. They were 17% in our study. These results may reflect a better social acceptance of transgender people and awareness about transgender issues, leading to a better inclusion in the healthcare system.
In our study, 53% of the respondents declared being very satisfied by the last consultation with their GP, and 31% were rather satisfied. French’s Research, Study, Evaluation and Statistics Direction (Direction de la recherche, des études, de l'évaluation et des statistiques, DRESS) published a report21 in 2017 on the general population’s opinion about their GP. Of the 3023 respondents, 34% were very satisfied and 54% rather satisfied with their GP. In both this study and ours, the satisfaction rate is close to 80%.
Our findings were consistent with a recent qualitative study focusing on transgender persons’ experiences in a family medicine clinic22 where results showed that a positive experience included ‘respecting the gender identities of every patient and focusing on the whole person-not the transgender status of the patient’, in other words, providing patient-centred care. In other recent studies exploring transgender patients’ expectations regarding their primary care/family physician, patients expect their family physician to be able to provide comprehensive care, including routine primary care and transgender-specific healthcare23 (eg, hormone therapy). This could help not delaying care due to fear of discrimination in the healthcare setting.24 A greater perceived knowledge of transgender health issues by their family physician alleviates the discomfort reported by transgender patients when discussing such issues,25 adding to the case of specific training in transgender issues needed to family physicians in training.
Implications of the study
Our study found that when their medical needs are not related to gender transition, transgender people go to their GP for reasons which seem similar to those of the general population. However, half of the reasons to visit their GP were related to transition. The definition of ‘related’ or ‘unrelated’ to transition was given by the respondents themselves when they answered the survey. No interpretation was made by the investigators when analysing the data. Respondents expected their transidentity not to be the sole concern of their GP, with a respect for their intimacy when the reason for visit is unrelated to gender-affirming healthcare. However, they expected their GP to be aware of the specificities of transgender healthcare to avoid discrimination and negative attitudes. Lack of specific knowledge in primary care providers about transgender healthcare (and the subsequent need for transgender patients to educate their physician) is associated with a more frequent postponing or not seeking of medical care.26
Our findings add to the body of literature on patient-centred primary care for transgender patients. Primary care providers, including GPs, must be able to provide routine primary care for transgender patients, for either transition related or unrelated healthcare. Such healthcare requires specific knowledge, and patient-centred care is particularly appropriate in general practice. Family medicine trainees should benefit from medical education focusing on transgender-specific healthcare and issues.
Data availability statement
Data may be obtained from a third party and are not publicly available. Following the requirements of the french CNIL, data are not publicly available.
Ethics statements
Ethics approval
The study protocol was approved by the Ethics Committee of Lyon University College of General Practice (IRB: 2017-09-05-07) and by the CNIL (National Commission for Data and Liberties Protection).
Acknowledgments
The authors would like to acknowledge and thank the members of the association Chrysalide who discussed and worked on the study protocol and questionnaire. The authors thank the local College of teaching general practitioners (Collège lyonnais des généralistes enseignants, CLGE) who covered publication fees.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @GeluleMD
Contributors All authors (MG, SO, MF, CM-F) equally participated in the protocol design. MG and SO conducted the study. All authors (MG, SO, MF, CM-F) analysed the results. MG, SO and CM-F wrote the first draft of the paper. All authors (MG, SO, MF, CM-F) reviewed the different versions of the paper, and approved the final version of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Funding was provided by the local College of teaching general practitioners (Collège lyonnais des généralistes enseignants, CLGE) to cover publication fees.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.