Article Text

Abstract
Objectives It is essential to have simple, reliable and valid tests to measure children’s functional capacity in schools or medical practice. The 1-minute sit-to-stand (STS) test is a quick fitness test requiring little equipment or space that is increasingly used in both healthy populations and those with chronic disease. We aimed to provide age-specific and sex-specific reference values of STS test in healthy children and adolescents and to evaluate its short-term reliability and construct validity.
Design setting and participants Cross-sectional convenience sample from six public schools and one science fair in central Europe. Overall, 587 healthy participants aged 5–16 years were recruited and divided into age groups of 3 years each.
Outcomes 1-minute STS. To evaluate short-term reliability, some children performed the STS test twice. To evaluate construct validity, some children also performed a standing long jump (SLJ) and a maximal incremental exercise test.
Results Data from 547 youth aged 5–16 years were finally included in the analyses. The median number of repetitions in 1 min in males (females) ranged from 55 [95% CI: 38 to 72] (53 [95% CI: 35 to 76]) in 14–16-year olds to 59 [95% CI: 41 to 77] (60 [95% CI: 38 to 77]) in 8–10-year olds. Children who repeated STS showed a learning effect of on average 4.8 repetitions more than the first test (95% limits of agreement: −6.7 to 16.4). Moderate correlations were observed between the STS and the SLJ (r=0.48) tests and the maximal exercise test (r=0.43).
Conclusions The reported STS reference values can be used to interpret STS test performance in children and adolescents. The STS appears to have good test–retest reliability, but a learning effect of about 10%. The association of STS with other measures of physical fitness should be further explored in a larger study and technical standards for its conduct are needed.
- paediatrics
- primary care
- public health
- sports medicine
Data availability statement
Data are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Large sample size (N=547).
Reference values according to sex and age group (5–7 years, 8–10 years, 11–13 years and 14–16 years).
Evaluation of test–retest reliability and construct validity.
Convenience sample, not a population-based sample.
Not all outcomes have been measured on each participant.
Introduction
Physical fitness is widely understood to be an indicator of an individual’s overall health status as well as an important predictor of morbidity and mortality.1 2 A wide range of fitness tests have been developed for the assessment of muscular strength (eg, grip strength test, standing long jump (SLJ) test and isokinetic dynamometry3–6) and aerobic capacity (eg, 6-minute walk test (6MWT), cardiopulmonary exercise on a treadmill or stationary bike and 20-metre multistage fitness test7–9) in healthy individuals as well as in people suffering from chronic diseases.2
One increasingly used functional capacity test is the 1-minute sit-to-stand (STS) test,10 which evaluates how many times per minute an individual is able to stand up and sit down on a chair standardised for height.2 The STS is an attractive alternative to other tests for the assessment of overall physical fitness as it is simple, quick, requires only a chair and a stopwatch and is possible even in small spaces, indicating that it can equally be used as an exercise test or a screening instrument. It has previously been evaluated in adults, especially those with chronic conditions such as chronic obstructive pulmonary disease (COPD)1 11 or cystic fibrosis.7 Increasing interest has been shown to the use of STS as a test of functional exercise capacity in children, both healthy12 13 and with chronic conditions.14 In small samples, STS has been observed to correlate well with the 6MWT14 and with final heart rate13 during the test.
In recent years, several studies provided reference values for the STS in adults, but to our knowledge no age-specific standard values are available for healthy children and adolescents.2 Standard values are needed to interpret the exercise capacity of children and youth, both healthy and with various diseases, in a wide range of settings. Some prediction models and overall references including large age ranges, however, exist.13 Data concerning construct validity and test–retest reliability in healthy children and adolescents are also lacking.
We aimed to measure STS test performance in healthy children and adolescents in order to provide age-specific and sex-specific reference values, to assess short-term reliability, and to evaluate construct validity. Based on the adult literature,15 we hypothesised that the STS test is reliable and valid in youth and that performance increases with age and lean mass. To examine the construct validity of STS, we compared repetitions of STS with other commonly used functional capacity outcomes including SLJ and a bicycle test.
Methods
Study design
This cross-sectional study was comprised of a convenience sample of children and adolescents aged 5–16 years. For the evaluation of short-term reliability, children and adolescents performed the STS test twice, with a break of 15 min between trials. To test construct validity, a subsample of children and adolescents additionally performed a maximal incremental exercise test on a cycle ergometer as a measure of aerobic capacity and the SLJ as a measure of muscular strength.
Population
A convenience sample of healthy children and adolescents aged 5–16 years from five public schools located in three different Swiss towns (Biel, Grenchen and Zurich) were contacted in January 2017 and asked to participate. In addition, one public school located in Potsdam, Germany participated in September 2019. Furthermore, we recruited children and adolescents during Scientifica, an open-door Swiss science fair organised by the University of Zurich and the Swiss Federal Institute of Technology in Zurich (ETH Zurich) in September 2017. We aimed to enrol at least 70 children per age category (5–7 years, 8–10 years, 11–13 years and 14–16 years), based on feasibility considerations.
Test results were stored anonymously in a database of the Epidemiology, Biostatistics and Prevention Institute of the University of Zurich, Switzerland. The Ethical Committee of the Canton of Zurich waived the need for ethical approval, as this study does not fall under the scope of the Human Research Act in Switzerland.16 Written informed consent (ie, signature by participant or parent/caregiver) is not mandatory since the study measurements included only minimal risks for the study participants and the data were collected anonymously. Swiss children did however provide their oral consent to participate. In Germany, all participants and their legal guardians were informed about potential risks and benefits of the study prior to enrolment and legal guardians provided their written informed consent.
Measurements
In order to estimate age-specific and sex-specific reference values, all children performed at least one STS test. For the evaluation of short-term reliability, some participants performed a second STS test. To test construct validity, a subset of children also performed either the maximal incremental exercise test for the assessment of aerobic capacity or the SLJ for the assessment of muscle strength.
Assessment of anthropometrics
Standing height (in cm, accuracy 0.5 cm), leg length (from the anterior inferior iliac spine to the lateral malleolus in 5 cm, accuracy 1 cm) and body mass (in kg, accuracy 100 g) were assessed. Body mass index (BMI) was calculated and z-scores derived.17 During the assessment of anthropometrics, children and adolescents wore sportswear and gym shoes (sneakers).
1-minute STS test
In the STS, children and adolescents had to stand up and sit down on a chair without arm rests as many times as possible within 1 min (working instructions are present in online supplemental material 1). The wooden chair was adapted to the individual height of the children, so that the angle of their knee joints was approximately 90° while sitting. Furthermore, the chair height (in cm) from the sitting plane to the floor was measured. During the test, participants had to keep their feet parallel and to put their hands on their waist in order to ensure that they would not use their arms to assist the movement.2 8 They were instructed to straighten their knees and stand up completely, and to touch the chair with the buttocks when sitting down. The instructor told the participants to complete as many STS repetitions as possible within 1 min. They were informed when 15 s were left, but they were not motivated by the instructor during the test. The number of fully completed and correct STS cycles after 1 min was recorded for the analysis. The STS test at schools was conducted by a single member of the study team. At Scientifica, six different people conducted the STS test precisely adhering to standard operational procedures.
Supplemental material
Maximal incremental exercise test on a stationary bike
A subset of children and adolescents completed an exercise test on a children’s bicycle ergometer (Corival Pediatric, Lode, Netherlands). The exercise test was based on the Godfrey protocol18 in which the children started at a different workload depending on their standing height and the workload was increased every 1 min depending on their standing height (ie, height <120 cm=10 W/min, height 120–150 cm=15 W/min and >150 cm=20 W/min) until exhaustion. During the test, the children wore a heart rate monitor (Polar RCX5TM). The children were told to pedal at ≥60 revolutions per minute (rpm). The test was stopped as soon as at least one of the following criteria was reached: subjective exhaustion ≥8 on a 0–10 modified Borg scale,19 heart rate ≥190 beats/min or the participants could not maintain a pedalling speed of at least 60 rpm. Maximal workload (Wmax) and maximal workload adjusted for body mass (Wmax/kg) were computed for the analysis.
Standing long jump
In the SLJ,6 the children had to jump as far as they could in horizontal direction from an upright standing position. An arm swing prior to and during the jump was allowed. The jump distance between the starting line and the heel of the posterior foot was retained for the analysis. SLJ was repeated three times, of which the furthest distance was recorded as best trial. To adjust for children’s differing heights, SLJ performance was analysed as best distance divided by height.
Statistical analysis
Anthropometric data and STS test data were summarised as n and median (IQR) according to sex and age group (5–7 years, 8–10 years, 11–13 years and 14–16 years) and reported using percentiles 2.5%, 25%, 50%, 75% and 97.5%. We considered four definitions of STS outcome: best of two tests, first STS, last STS and mean first and second STS Test–retest reliability between first and second STS was assessed using the method of Bland and Altman,20 where mean difference in the two tests assesses their agreement, along with 95% limits of agreement. Construct validity was examined by comparing STS test to SLJ and maximal exercise test using Pearson’s correlation coefficient. We also considered partial correlations of the three anthropometric measures (ie, standing height, leg length and body mass) adjusting for age. Correlation coefficients of 0–0.19 were considered very weak, 0.2–0.39 weak, 0.4–0.59 moderate, 0.60–0.79 strong and 0.80–1.0 very strong.21 The statistical analysis was performed using the R programming language22 (R Version 4.0.3), and code is available in online supplemental material 2.
Supplemental material
Patient and public involvement
Participants were not involved in the design, recruitment or conduct of this study.
Results
Study population
Of the 587 participants, we excluded 13 because they were younger than 5 or older than 16 years, 8 had missing age or STS test and a further 19 were unmotivated to perform the tests, leaving a final number of 547 subjects. We divided the study population into four different age groups: 5–7 years, 8–10 years, 11–13 years and 14–16 years. Descriptive characteristics of each age group are shown in table 1. Overall, 373 (68%) participants performed the STS test twice, 43 (8%) performed the maximal exercise test and 72 (13%) did the SLJ (online supplemental table S1).
Study population including all participants aged 5–16 years with at least one STS test
Reference values for the STS
To define the reference values for the STS test in children and adolescents, we calculated the distribution of the STS test performance for each sex and age group (figure 1 and table 2). The median number of repetitions in 1 min in males (females) ranged from 55 (53) in 14–16-year olds to 61 (64) in 8–10-year olds. In most age groups, 50% of children achieved between 55 and 65 repetitions. No relevant differences in distribution of the number of repetitions were observed between the two genders. The age group 14–16 years showed the lowest median number of repetitions (females 53, males 55).

Comparison of STS test reference values (median, lines to Q1 and Q3, points for 2.5% and 97.5%) in children and adults (*as published in Strassmann et al2). Reference values in children are calculated based on the best of one or two STS tests, while for adults they are calculated based on a single STS test. STS, sit-to-stand.
We included the best STS test performance for the calculation of these reference values. Considering different definitions of STS (first measurement, last measurement, best of two measurements or mean of two repetitions) altered the reference values by approximately three to five repetitions (online supplemental table S2), with those including only the first measurement being lower than the other definitions.
Reliability
Figure 2A shows the correlation between the results of the two STS tests, whereas the Bland-Altman plot figure 2B shows the mean difference between the two test results as well as the distribution of the differences compared with the number of average repetitions. The second STS test had on average 4.8 more repetitions than the first STS test (95% limits of agreement: −6.7 to 16.4), indicating a clear learning effect.
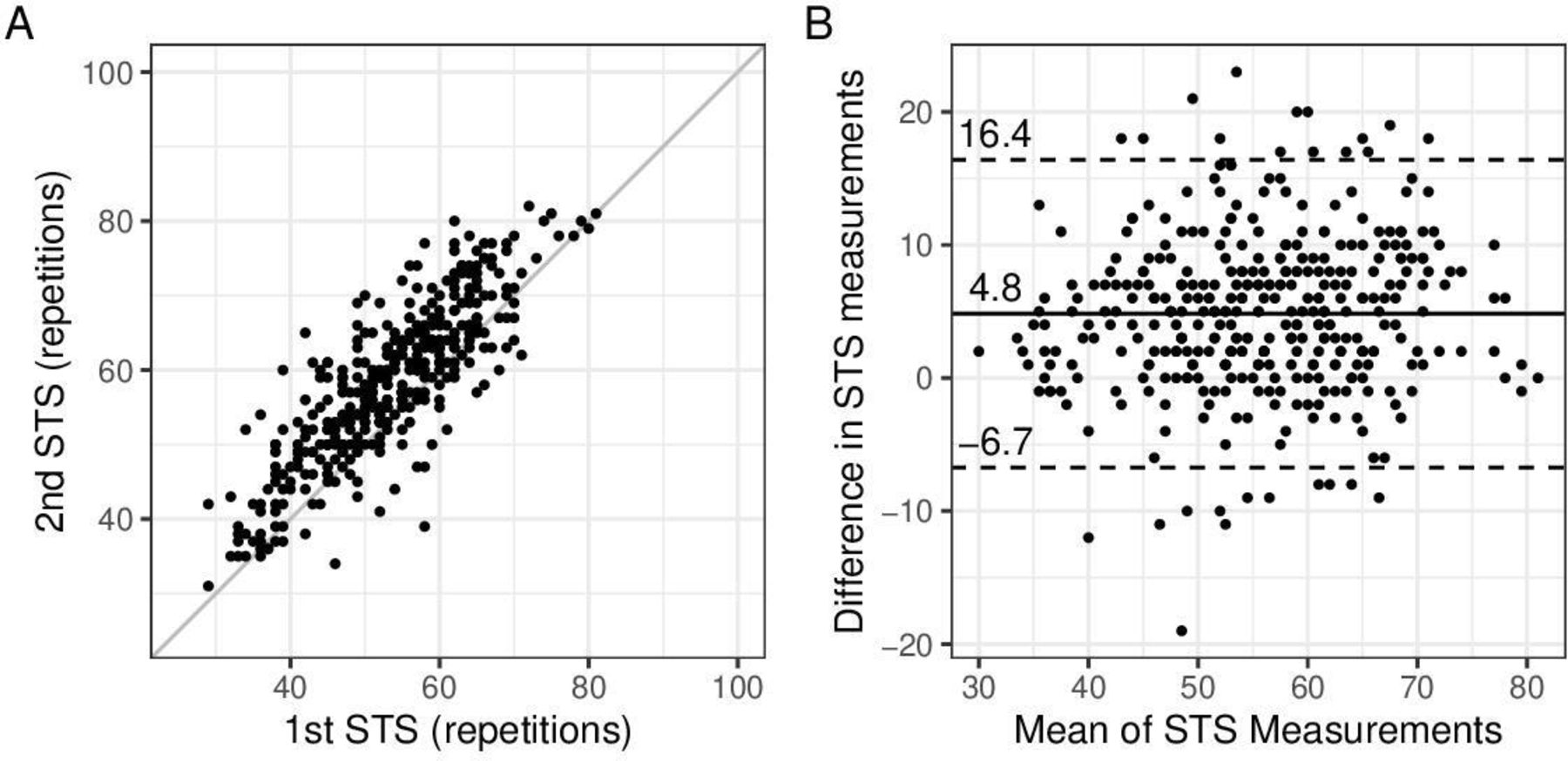
(A) Scatterplot showing the paired results of the first and the second sit-to-stand (STS) test (n=373, diagonal line indicates perfect agreement), (B) Bland-Altman plot showing the mean bias and the limits of agreement of the difference between the second and the first STS test.
Construct validity
The relationship between the number of repetitions in the STS test and the maximal exercise test and SLJ performance is illustrated in figure 3. The correlation between STS test and aerobic capacity (Watt per kilogram body mass) was r=0.43 (95% CI: 0.15 to 0.65) and SLJ (distance divided by standing height) r=0.48 (95% CI: 0.28 to 0.64).

{kind=link}
{kind=link}
{kind=link}
Scatterplot showing the correlation between the mean of the best sit-to-stand (STS) test result and (A) the maximal incremental exercise test on a stationary bike (n=43), and (B) the standing long jump test (SLJ) (n=72).
While SLJ and maximal aerobic capacity both increased with age (r=0.44 SLJ, r=0.39 Wmax), STS test decreased slightly with age (r=−0.14) (online supplemental figure S1). When adjusting for age using partial correlation, the association was weak to moderate: maximal aerobic exercise test and STS test, correlation r=0.36 (95% CI: 0.07 to 0.60); SLJ and STS test r=0.42 (95% CI: 0.20 to 0.59) (online supplemental figure S2).
Discussion
This study provides age-stratified and sex-stratified reference values for the 1-minute STS test based on the results of a large sample (N=547) of 5–16-year old healthy children and adolescents, which can be used to interpret STS test performance in this population. Reference values are necessary to correctly interpret an individual’s STS test performance, and to identify individuals with decreased exercise capacity. While there were no significant differences between male and female participants, 14–16-year olds generally performed less well than other age groups. Short-term test–retest reliability was high, although there was a clear learning effect of approximately five repetitions out of a total range of 40–80 repetitions. STS showed a weak to moderate association with maximal aerobic exercise capacity and lower limb muscle strength.
Concerning construct validity, our study showed only a weak correlation between STS and maximal exercise capacity, in contrast with other studies examining subjects with cystic fibrosis.7 8 23 A low correlation was also observed between STS and SLJ, as a proxy for lower limb muscle power, and between STS and BMI (z-scores), as a proxy for muscle mass.
The main strengths of this study are the large sample size (N=547), to our knowledge the largest study to date of STS test in healthy children and adolescents, as well as the consideration of different age groups. A limitation of this study is that it is based on a convenience sample, not a population-based sample, and that the sample on which the examination of construct validity is based is not a random subsample. A learning effect could only be evaluated in a subpopulation of children (n=373, 68%) for which two STS tests were available. However, computing reference values for STS test based on this subset had only a small impact on the STS test percentiles (ie, differences of min −2 to max 2 repetitions across age groups and sexes). Additionally, the maximal exercise test and SLJ used to assess construct validity were not measured in all subjects.
There have been few other studies of STS test in children. A recent study in Belgium12 assessed construct validity and test–retest reliability of STS in a sample of 52 children aged 8–18 years, comparing it to the 6MWT and final heart rate. Similarly to our study, they found a learning effect in the number of STS repetitions between the first and second trial (mean difference 2.5 repetitions, 95% CI: 1.5 to 3.5), suggesting that at least one practice test is needed to ensure an accurate estimate of functional exercise capacity. The same research group also developed a predictive model for STS in healthy 6–12-year olds (n=238),13 focusing on individual characteristics (age, sex, height and weight) and final heart rate during STS. They reported differing mean repetitions of 47 in girls and 54 in boys, while we observed the same median of 61 in both boys and girls in this age range. Gender differences may have occurred due to only two different chair heights (46 cm chair for participants 140 cm or taller, otherwise 32 cm chair) instead of individually adapted height as in our study (median 40 cm, range 24–50.5 cm), that may have induced an advantage of one gender or a disadvantage for the other in a rather small and heterogeneous sample with a large age range. Our study is the largest study of STS in children to date and is the only study to provide reference values for a healthy population of children and adolescents in different age categories.
We provided reference values for STS test in healthy participants aged 6–16. Although there were no differences between males and females, older participants (14–16 years) performed less well on average than those in younger age groups, even though muscle mass and strength are still increasing at this age. We suspected that weaker performance of this age group might be related to greater height or longer leg length, but only weak correlations were observed (online supplemental figure S3) between STS test and height (r=−0.16, 95% CI: −0.24 to −0.08) or leg length (r=−0.13, 95% CI: −0.24 to −0.02) or ratio of leg length to height (r=0.09, 95% CI: −0.02 to 0.21). Adjusting for age using partial correlation did not increase the strength of the associations between STS test and height (r=−0.10, 95% CI: −0.18 to −0.02, adjusted for age) or leg length (r=0.02, 95% CI: −0.10 to 0.13, adjusted for age) or the ratio of leg length to height (r=0.08, 95% CI: −0.04 to 0.19, adjusted for age). It cannot be excluded that the age differences in STS test performance were due to lack of motivation or decreased physical activity commonly found during adolescence.24 However, it could also be that performance in STS reaches its peak by the age of 11 and then decreases in accordance to physical activity levels.25 This hypothesis would be consistent with the findings of a study of STS in adults, which reported STS test values for 20–24-year olds which were lower than what we observed in 14–16-year olds, indicating that STS test performance decreases steadily with age (figure 1).2 However, as there is no data available for 17–19-year olds, it would be necessary to include such participants in future studies to verify this hypothesis.
Reference values of the sit-to-stand test in children and adolescents (N=547)
Regarding construct validity, the weak to moderate correlation we observed between STS test and maximal exercise capacity (Wmax) suggests that neither maximal nor submaximal12 aerobic capacity may not be one of the major determinants of exercise in health children and adolescents, and therefore it is possible that STS test is not best suited to assess aerobic capacity in this population. Correlation with SLJ as a measure of lower limb muscle power was also weak, despite STS test having been shown previously to be moderately associated with muscle strength in patients with COPD.1 In a predominantly normal weight population as described here, one would suggest that BMI serves as a proxy measure for muscle mass, and would therefore be related to STS test. However, only a weak correlation was observed here between BMI and STS test. The prediction model proposed by Reychler et al13 suggests that sex, age, weight and final heart rate explain approximately 24% of STS test performance. Taken together, these findings suggest that the STS test can be taken neither as an aerobic performance test, nor as a pure strength test, as has been observed in other studies,1 but may also include skills like balance and coordination.
The results of this study suggest various avenues for future research. First, a systematic review of STS test should be undertaken to determine the current state of evidence in both children and adults. Second, technical standards for proper conduct of STS test are needed, especially for use in children (eg, where a standard size chair may be too large). Third, further studies are needed to evaluate the learning effect over multiple STS test measurements, to provide standard values for other racial or ethnic groups and in other geographic regions, and to better validate STS test against other measures of physical fitness such as anaerobic exercise capacity measured by a Wingate anaerobic test26 27 or steep ramp test.28 Such a study should also include 17–19-year olds as data on subjects in this age group are missing in both the present study and in the previously published2 reference values for STS test in adults.
Conclusions
This study provides reference values for the STS test in healthy children and adolescents aged 5–16 years. Reference values help to interpret the performances achieved in STS and to detect individuals with decreased physical performance. Further investigation is needed to clarify whether the STS primarily demands muscle strength or aerobic capacity in children and adolescents.
Code availability
The R script is available in online supplemental material 2.
Data availability statement
Data are available upon reasonable request to the corresponding author.
Ethics statements
Ethics approval
The study protocol was approved by the local ethical commission of the University of Potsdam (submission No. 45/2019). The ethical commission of the Canton of Zurich waived the need for ethical approval, as this study did not fall under the scope of the Human Research Act in Switzerland.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SRH and TF are joint first authors.
Contributors SRH, SK and TR made substantial contributions to conception and design. JS, TF, SK and TR contributed to data collection. SRH carried out data analysis. SRH, JS, UG, SK and TR interpreted the data. SRH and TF wrote the first draft of the manuscript and all authors were involved in revising it critically for important intellectual content. All authors provide final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note TR and SK are joint last authors.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.