Article Text

Abstract
Objectives To identify and critically appraise published clinical practice guidelines (CPGs) regarding healthcare of gender minority/trans people.
Design Systematic review and quality appraisal using AGREE II (Appraisal of Guidelines for Research and Evaluation tool), including stakeholder domain prioritisation.
Setting Six databases and six CPG websites were searched, and international key opinion leaders approached.
Participants CPGs relating to adults and/or children who are gender minority/trans with no exclusions due to comorbidities, except differences in sex development.
Intervention Any health-related intervention connected to the care of gender minority/trans people.
Main outcome measures Number and quality of international CPGs addressing the health of gender minority/trans people, information on estimated changes in mortality or quality of life (QoL), consistency of recommended interventions across CPGs, and appraisal of key messages for patients.
Results Twelve international CPGs address gender minority/trans people’s healthcare as complete (n=5), partial (n=4) or marginal (n=3) focus of guidance. The quality scores have a wide range and heterogeneity whichever AGREE II domain is prioritised. Five higher-quality CPGs focus on HIV and other blood-borne infections (overall assessment scores 69%–94%). Six lower-quality CPGs concern transition-specific interventions (overall assessment scores 11%–56%). None deal with primary care, mental health or longer-term medical issues. Sparse information on estimated changes in mortality and QoL is conflicting. Consistency between CPGs could not be examined due to unclear recommendations within the World Professional Association for Transgender Health Standards of Care Version 7 and a lack of overlap between other CPGs. None provide key messages for patients.
Conclusions A paucity of high-quality guidance for gender minority/trans people exists, largely limited to HIV and transition, but not wider aspects of healthcare, mortality or QoL. Reference to AGREE II, use of systematic reviews, independent external review, stakeholder participation and patient facing material might improve future CPG quality.
PROSPERO registration number CRD42019154361.
- protocols & guidelines
- quality in health care
- sexual and gender disorders
- international health services
Data availability statement
Data sharing statement: Additional data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- protocols & guidelines
- quality in health care
- sexual and gender disorders
- international health services
Strengths and limitations of this study
First systematic review to identify and use a validated quality appraisal instrument to assess all international clinical practice guidelines (CPGs) addressing gender minority/trans health.
International CPGs were studied due to their influential status in gender minority/trans health, though further research is needed on national and local CPGs.
An innovative prioritisation exercise was performed to elicit stakeholders’ priorities and inform the setting of AGREE II (Appraisal of Guidelines for Research and Evaluation tool) quality thresholds, however these stakeholder priorities may not be applicable outside the UK.
An inclusive approach using wide criteria, extensive searches and approaching key opinion leaders should have allowed the study to identify all relevant international CPGs, however it is possible some may have been missed.
Introduction
Assessing the quality of clinical practice guidelines
Evidence-based practice integrates best available research with clinical expertise and the patient’s unique values and circumstances. High-quality clinical practice guidelines (CPGs) support high-quality healthcare delivery. They can guide clinicians and policymakers to improve care, reduce variation in clinical practice, thereby affecting patient safety and outcomes. The Institute of Medicine defines CPGs as: ‘statements that include recommendations intended to optimise patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options’,1 although other definitions exist.2 Recommendations are used alongside professional judgement, directly or within decision aids, in training and practice. CPGs are important but have limitations depending on evidence selection and development processes.3 Grading of Recommendations, Assessment, Development and Evaluation (GRADE) was developed to address the evidence that is selected and appraised during CPG development.4–6 Using a systematic approach and transparent framework for developing and presenting summaries of evidence, GRADE is the most widely adopted tool worldwide for grading the quality of evidence and making recommendations,7 but does not alone ensure a CPG is high quality. Strength of evidence is only one component of what makes a ‘good’ CPG; factors such as transparency, rigour, independence, multidisciplinary input, patient and public involvement, avoidance of commercial influences and rapidity8 9 should also be considered. Broader domains of CPG quality are included in the Appraisal of Guidelines for Research and Evaluation instrument AGREE II.10–12 Despite widely recognised principles and methods for developing sound CPGs, current research shows that guidelines on various topics lack appropriate uptake of systematic review methodologies in their development,13 give recommendations that conflict with scientific evidence14 or do not adequately take into account existing CPG quality and reporting assessment tools.15 This emphasises the ongoing need to appraise guidelines to ensure evidence-informed care.
Healthcare for gender minority/trans people
‘Trans’ is an umbrella term for individuals whose inner sense of self (gender identity) or how they present themselves using visual or behavioural cues (gender expression) differs from the expected stereotypes (gender) culturally assigned to their biological sex.16 'Gender minority' is an often-used alternative population description. Some gender minority/trans people may seek medical transition, which involves interventions such as hormones or surgery that alter physical characteristics and align appearance with gender identity. Patient numbers referred to UK gender identity clinics and length of waiting lists have increased in the last decade, particularly for adolescents,17 a phenomenon seen elsewhere.18 Gender minority/trans people may have continuing, sometimes complex, life-long healthcare needs whether they undergo medical transition or not. Gender minority/trans people may experience more mental health issues such as mood and anxiety disorders,19 substance use20 and higher rates of suicidal ideation.21 They may seek assistance with sexual health, mental health,22 substance use disorders,23 prevention and/or management of HIV24 as well as usual general health enquiries. However, they may encounter difficulties in accessing healthcare,25 reporting negative healthcare experiences,26 discrimination and stigma.27 28 Like all individuals, gender minority/trans people require high-quality evidence-based healthcare25 29 addressing general and specific needs.
Guidelines used internationally and in the UK
The quality of current guidelines on gender minority/trans health is unclear. The World Professional Association for Transgender Health (WPATH) Standards of Care Version 7 (SOCv7)30 represent normative standards for clinical care, acting as a benchmark in this field.31 Globally, many national and local guidelines32–35 are adaptations of, acknowledge being influenced by, or are intended to complement WPATH SOCv7,30 despite expressed reservations that WPATH SOCv730 is based on lower-quality primary research, the opinions of experts and lacks grading of evidence.36
In the UK, an advocacy group worked to incorporate WPATH SOCv730 into national practice.37 WPATH SOCv730 informs National Health Service (NHS) gender identity clinics38 and guidelines produced by the Royal College of Psychiatrists (without use of GRADE).39 No CPGs were available from the National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN), British Association of Gender Identity Specialists, or medical Royal Colleges, although the Royal College of General Practitioners issued a position statement on gender minority/trans healthcare in 2019.40 Assessing quality of international CPGs such as WPATH SOCv730 has practice implications for the NHS38 and private sector. CPGs with international scope may present additional challenges (eg, the implementability of key recommendations might not be easily translated among different contexts) but they seem to influence discourse around gender minority/trans health.36 No prior study has investigated the number and quality of guidelines to support the care and well-being of gender minority/trans people. The purpose of this research was to identify and critically appraise all published international CPGs relating to the healthcare of gender minority/trans people.
Methods
Approach/research design
The rationale was to identify the key CPGs available to healthcare practitioners in this field of clinical practice. Following preliminary searches, we chose international CPGs in view of WPATH’s influence within the UK and elsewhere, and to avoid ‘double-counting’. We considered AGREE II10–12 the most appropriate tool; it is the most comprehensively validated and evaluated instrument available for assessing CPGs,41 42 designed for use by non-expert stakeholders10 such as healthcare providers, practicing clinicians and educators.11 It benefits from clear instructions and prompts regarding scoring and several people applying the criteria independently (a minimum of two reviewers, but four are recommended). AGREE II synthesis calculates quality scores from 23 appraisal criteria organised into six key domains (scope and purpose, stakeholder involvement, rigour of development, clarity of presentation, applicability, editorial independence) and an overall assessment of ‘Recommend for use?’ (answer options; yes, no, yes if modified). This systematic review was conducted according to a pre-specified PROSPERO protocol https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=154361 uploaded 19 December 2019. The MEDLINE strategy was straightforward; although not formally processed,43 it was peer-reviewed by an information specialist.
Inclusion and exclusion criteria
We defined a CPG as a systematically developed set of recommendations that assist practitioners and patients in the provision of healthcare in specific circumstances, produced after review and assessment of available clinical evidence.1 2 44–46 CPGs published after 1 January 2010 were eligible if they (or part thereof) specifically targeted patients/population with gender minority/trans status and/or gender dysphoria, were evidence-based, with some documentation of development methodology, had international scope (more than one country, defined as a Member State of the United Nations) and were an original source. We chose the time frame to focus on the most recent guidelines, currently applicable to practice and to include WPATH SOCv7.30 CPGs were eligible if they met the following inclusion criteria: participants/population was adults and/or children who are gender minority/trans with no exclusion due to comorbidities or age although differences/disorders in sex development (intersex) were excluded; exposure/intervention was any health intervention related to gender dysphoria or gender affirmation, or health concerns of gender minority/trans people, including screening, assessment, referral, diagnosis and interventions. We excluded previous versions of the same CPG. We used broad criteria because terminology has been in flux with changes made in both International Classification of Diseases and Diagnostic and Statistical Manual of Mental Disorders diagnostic criteria.16 There were no restrictions on setting or language.
Search strategy and guideline selection
We conducted the searches up to 11 June 2020 (CM), using search terms and appropriate synonyms (as Medical Subject Heading (MeSH) terms and text words) that we developed based on population and exposures (online supplemental table 1). We searched six databases (Embase, MEDLINE, Web of Science, PsycINFO, CINAHL, LILACS) and six CPG websites (Agency for Healthcare Research and Quality National Guideline Clearinghouse (NGC), eGuidelines and Guidelines, NICE National Library for Health, SIGN, EBSCO DynaMed Plus, Guidelines International Network Library) and the World Health Organization (WHO). The NGC closed in 2017 but CM hand-searched the archive. In addition to protocol, individual reviewers (IA, DC and MHJ) hand-searched four specialty journals (International Journal of Transgender Health, Transgender Health, LGBT Health, Journal of Homosexuality) to ensure key subject-relevant sources of abstracts were thoroughly checked. In order to find potential grey literature CPGs outwith the scholarly literature, two reviewers (IA and SD) independently performed four separate Google searches (not Google Scholar as misstated in the protocol) by using one generic (clinical practice guidelines) plus one specific term (transgender, gender dysphoria, trans health or gender minority) and examining the first 100 hits. We identified International Key Opinion Leaders (n=24) via publications known to reviewers (DC and SD) and contacted them via email, with one reminder, to identify further guidelines. Reference lists of relevant reviews and all full-text studies were hand-searched to identify any relevant papers or CPGs not found by database searching. Two reviewers (SB and SD) independently read all titles and abstracts and assessed for inclusion. If there was uncertainty or disagreement, or reasonable suspicion that the full-text might lead to another relevant CPG, the full-text was obtained. Non-English abstracts were Google-translated but if a possible CPG could not be reliably excluded, the full-text paper was obtained and translated. Where full-text publications could not be accessed, we contacted authors directly. Two reviewers (SB and either DC/MHJ) independently carried out full-text assessment to determine inclusion or exclusion from the systematic review based on the above criteria, and noted reasons for excluding full-texts. The whole team discussed uncertainties and disagreements to achieve consensus, with voting and final adjudication by the senior author (CM).
Supplemental material
Data extraction
Two reviewers (SB and SD) independently collected formal descriptive data of included CPGs. All ambiguities or discrepancies were referred to the team for discussion and to re-examine original texts and extract data. Information collected was title, author, year of publication, number of countries covered, originating organisation, audience, methods used, page and reference numbers (excluding accompanying materials) and funding. Key recommendations were extracted for comparison between CPGs. We searched for all text mentions of mortality or any measures of quality of life (QoL), and noted if accompanied by a citation. All patient facing material was extracted. In addition, we extracted data about publication outlet (journal/website), and whether the quantity of information pertaining to the health of gender minority/trans people represented a complete, partial or marginal proportion of recommendations in the CPG.
Outcomes
Outcomes were: the number and quality assessment scores (using AGREE II) of international CPGs addressing the health of gender minority/trans people; analysis and comparison of the presence or absence of information on estimated changes in mortality or QoL (any measure) following any specific recommended intervention, over any time interval; the consistency (or lack thereof) of recommendations across the CPGs; and the presence (or absence) of key messages for patients.
Quality assessment
All authors completed AGREE II video training, a practice assessment and two pilots whose results were discussed. The six reviewers (IA, SB, DC, SD, MHJ and CM) independently and anonymously completed quality scoring on every CPG by rating each of the items using the standard proforma on the My AGREE PLUS online platform (AGREE enterprise website),11 which also calculated group appraisal scores.
Patient and public involvement
The AGREE II instrument generates quality scores but does not set specific parameters for what constitutes high quality, recommending that decisions about defining such thresholds should be made prior to performing appraisals, considering relevant stakeholders and the context in which the CPG is used.11 To help set quality thresholds, we conducted an AGREE II domain prioritisation exercise in January 2020 via email, with one reminder. It was considered impossible to ensure comprehensive representation of international stakeholders. We chose the UK for feasibility, although validity might be limited to UK-based clinicians. Fifty-two UK service-user stakeholder groups and gender minority/trans advocacy organisations, identified via reviewer knowledge and internet searches (IA, SB, DC, SD, MHJ and CM), were informed about the study. They were invited to participate in a stakeholder prioritisation of the AGREE II domains, created using SurveyMonkey and with an option to remain anonymous (https://www.surveymonkey.co.uk/r/WLZ55NQ gives invitation wording, links to resources and protocol). The reviewer team performed an anonymous prioritisation for comparison.
Strategy for data and statistical analyses
Simple frequencies were used to present the stakeholder and reviewer priorities, and outcomes. Following team discussion of the prioritisation exercise results, no prespecified quality threshold score was used to define high or low quality, although colour was superimposed (≤30%, 31%–69% and ≥70%) on the final scores table to aid visual comparisons and interpretation.
Results
Search results
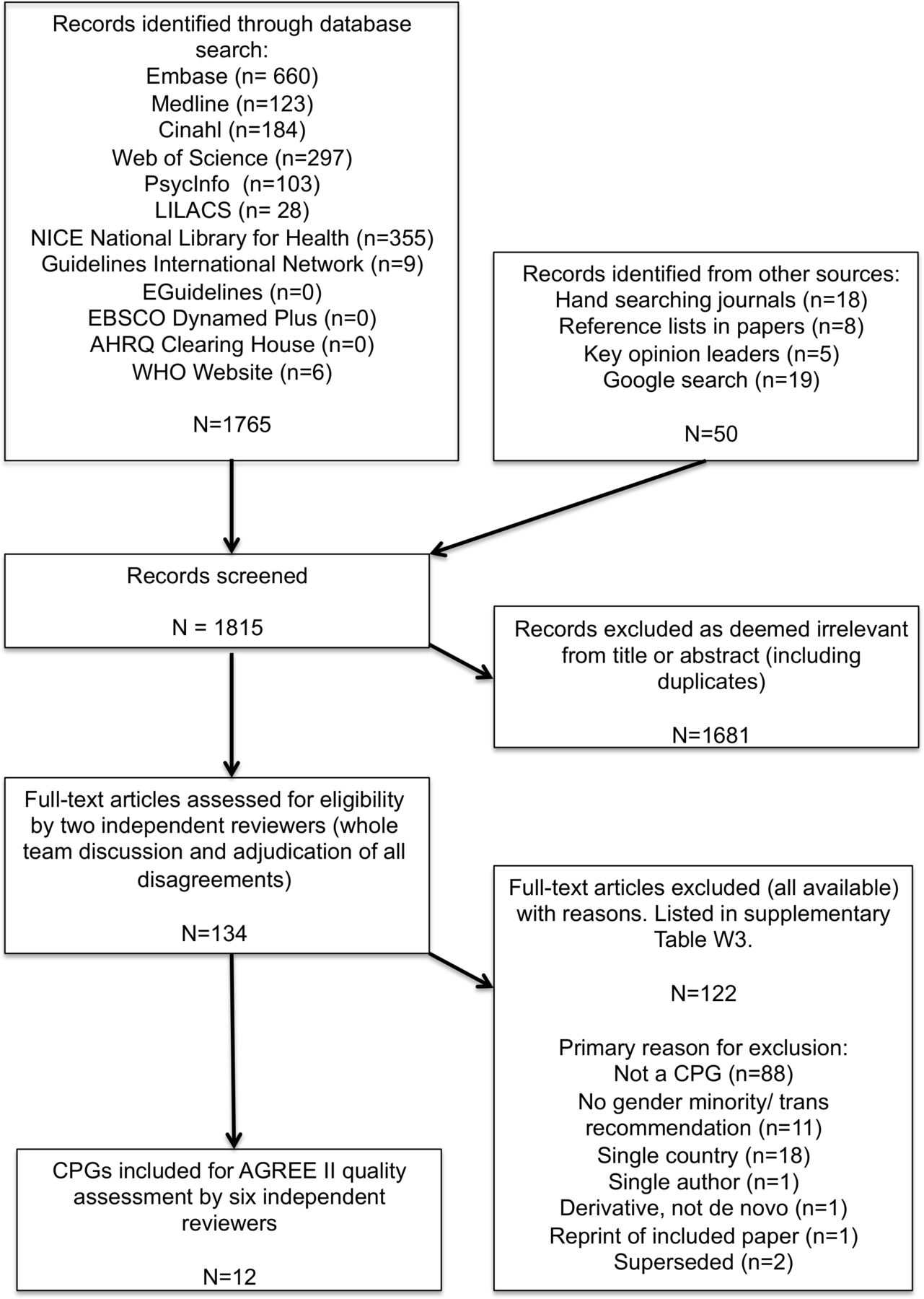
Figure 1 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart47) shows that 1815 citations were identified, of which 134 full-text publications were read (all available, three supplied by authors) and 122 excluded (online supplemental table W2 with reasons).

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. AGREE II, Appraisal of Guidelines for Research and Evaluation tool; CPG, clinical practice guideline; NICE, National Institute for Health and Care Excellence.
Data extraction
Table 1 shows the characteristics of the CPGs. Online supplemental tables W3 and W4 show raw data of key recommendations and mortality and QoL evidence.
General characteristics of included clinical practice guidelines (n=12)
Number and characteristics of clinical practice guidelines
Twelve CPGs (table 1) originated from: WHO (n=3),48–50 WPATH (n=2),30 51 professional specialist/special-interest societies (n=4),52–55 small groups of experts (n=2)56 57 and one consortium.58 All were published in English, in journals,51–57 the organisation’s website48–50 58 or both.30 Guideline development methodology was variable, including use of systematic reviews (table 1). Ten CPGs had no external review, eight had no update plans. Gender minority/trans health recommendations made up complete (n=5),30 51 53 55 57 partial (n=4)48–50 56 or marginal (n=3)52 54 58 focus of content. CPGs contained 10 to 155 pages, and 20 to 505 references. Funding sources were wide-ranging and sometimes multiple, from government agencies, professional societies, charities and private donations. Two CPGs provided no funding details.52 56
A 13th CPG was excluded post-scoring as it had been superseded by a 2020 version without recommendations for gender minority/trans people.59 It was arguable if four included CPGs did meet criteria: one had not been withdrawn48; one contained minimal relevant content52; one might not have been intended as a CPG30 (although WPATH SOCv7’s stated overall goal is ‘to provide clinical guidance for health professionals’30 it contains no list of key recommendations nor auditable quality standards, yet is widely used to compare procedures covered by US providers60 61); one variously described itself as ‘position statement’ and ‘position study’ (stating it did ‘not aim to provide detailed clinical guidelines for professionals such as… [named]30 53’, but evidence was obviously linked to key recommendations for clinicians55). After discussion it was decided not to exclude these borderline CPGs, as the definition of CPG in the protocol was intended to favour an inclusive approach.
Quality prioritisation and assessment
Results of the domain prioritisation by stakeholders (n=19 replies, response rate 39% excluding 3 ‘undeliverable’) and reviewers (n=6) showed that stakeholders prioritised stakeholder involvement, whereas the reviewer team prioritised methodological rigour (online supplementary table W5). No stakeholder asked for clarification or more information.
Table 2 shows AGREE II scores by domain (8%–94%), and overall (11%–94%). The quality scores have a wide range and heterogeneity. Five CPGs focused on trans people as a key population for HIV and other blood-borne infections (overall assessment scores 69%–94%). Six CPGs concerned transition-specific interventions (overall assessment scores 11%–56%). Transition-related CPGs tended to lack methodological rigour and rely on patchier, lower-quality primary research. The two prioritised domain scores were usually comparable with the overall AGREE II quality assessment (ranges; stakeholder involvement 14%–93%, methodological rigour 17%–87%). Four CPGs obtained a majority opinion ‘recommend for use’,48–50 58 five CPGs had unanimous ‘do not recommend’30 51 55–57 and three had minority support with division about the extent of ‘yes, if modified’52–54 (table 2). Despite wide variation there was a pattern; HIV and blood-borne infection guidelines48–50 54 58 were higher quality, and those focusing on transition were lower quality.30 53 55–57
AGREE II (Appraisal of Guidelines for Research and Evaluation tool) domain percentages and overall assessment of included guidelines, and summary of mortality/quality of life measures (n=12)
Content
Four CPGs concerning HIV prevention, transmission and care48–50 54 and one public health guideline on population screening for blood-borne viruses,58 contained recommendations for gender minority/trans people as a ‘key population’. Three CPGs were devoted to overall transition care for all gender minority/trans people,30 53 55 two to an aspect of transition51 56 and one to transition in a specific group.57 One oncology communication guideline contained a single recommendation relating to gender minority/trans people.52 No international guidelines were found that addressed primary care, psychological support/mental health interventions, or general medical/chronic disease care (such as cardiovascular, cancer or elderly care).
Mortality and quality of life
Six CPGs referred to mortality30 48 50 53 54 58 and eight to QoL30 48 49 51 53–55 58 (table 2). Online supplemental table W4 shows all extractions of sentences relating to mortality or morbidity, associated references and which CPGs included no such data. More robust evidence was linked to the recommendations in the HIV and blood-borne virus CPGs whereas there was little, inconsistent data and poorer linking to evidence in transition-related CPGs.
Consistency of recommendations across the CPGs
Online supplemental table W5 contains all extracted key recommendations where these could be distinguished. It shows little overlap of topic content across the CPGs. Many recommendations in WHO 201148 and 201650 were similar, but not identical, the former not being stood down after the latter was published. No statements were highlighted by the WPATH SOCv730 authors as key recommendations, and it proved impossible for all six reviewers independently performing data extraction to identify them. The total number of extracted recommendations ranged between 0 and 168 with little consistency or agreement on what passages were selected. Some extracted statements might have been intended as recommendations or standards, but many were flexible, disconnected from evidence and could not be used by individuals or services to benchmark practice. After discussion of this incoherence within WPATH SOCv730 and our inability therefore to compare recommendations across all CPGs, it was decided not to revisit inclusions post hoc but to abandon this protocol aim.
Patient facing material
No patient-facing material was found in any guideline.
Discussion
Statement of principal findings
Variable quality international CPGs regarding gender minority/trans people’s healthcare contain little, conflicting information on mortality and QoL, no patient facing messages and inconsistent use of systematic reviews in generating recommendations. A major finding is that the scope of the guidelines is confined to HIV/STI prevention or management of transition with an absence of guidelines relating to other medical issues. WPATH SOCv730 cannot be considered ‘gold standard’.
Strengths and weaknesses of this study
Strengths include protocol preregistration, stakeholder involvement, piloting all stages, an extensive systematic search without language restriction for any relevant current guidelines, wide inclusion criteria including grey literature, use of key opinion leaders, close attention to avoidance of bias, double full-text reading and data entry and careful presentation of results. Six trained reviewers, exceeding AGREE II recommendations,11 compensated for expected variation in scoring. Extensive searches should have mitigated loss of CPGs. Limitations include some uncertainty about stakeholder understanding despite a good response rate, and generalisability of the prioritisation only to the UK; stakeholders elsewhere might have different priorities. Focusing only on international CPGs might have missed higher quality national and local CPGs derived from them or written de novo. The social acceptance and consequent healthcare system coverage of gender minority/trans health related interventions vary among different countries, which may limit the space for international and multinational guidelines. While the search strategy yielded an oncology communication CPG with a single recommendation for gender minority/trans people,52 other general health CPGs with similar solo statements might have been missed.
Comparison with other studies, discussing important differences in results
This is the first systematic review using a validated quality appraisal instrument of international CPGs addressing gender minority/trans health. It may act as a benchmark to monitor and improve population healthcare. CPG quality results correspond with, and quantitatively confirm, previously noted concerns about the evidence-base36 62 63 and variable use of quality assessment in systematic reviews,64–66 in a healthcare field with unknown or unclear longitudinal outcomes.17 AGREE II has been applied to CPGs in other medical areas, including cancer,67 diabetes,68 pregnancy69 and depression.70 These exercises tend to show room for improvement. Developers have been criticised for not using methodological rigour when writing reliable evidence-based guidelines,71 as well as not implementing high-quality CPGs.72 Thus, finding poor quality CPGs is not confined to this area of healthcare.73 Improvement messages are generalisable to other specialties.
Meaning of the study: possible explanations
The finding of higher-quality, but narrow, focus on gender minority/trans people’s healthcare for blood-borne infections may relate to the global HIV pandemic and the WHO applying twin lenses of public health and human rights (ie, the population as ‘means’ and ‘ends’). The lower-quality CPGs focus on transition. WPATH SOCv730 originated nearly a decade ago from a special-interest association; diagnostic criteria and CPG methodology have since changed. Although HIV and transition are important, it is puzzling to have found so little else, maybe suggesting CPGs for gender minority/trans people have been driven by provider-interests rather than healthcare needs. Including gender minority/trans people in guidelines can be considered a matter of health equity, where CPGs have a role to play.74 GRADE suggests CPG developers may consider equity at various stages in creating guidelines, such as deciding guideline questions, evidence searching and assembly of the guideline group.75 How CPGs may impact more vulnerable members of society should be reflected-upon during guideline development,76 and implementation.77
Implications for clinicians, UK and international policymakers and patients
Clinicians should be made aware that gender minority/trans health CPGs outside of HIV-related topics are linked to a weak evidence base, with variations in methodological rigour and lack of stakeholder involvement. While patient care plans ought to take into account the individual needs of each gender minority/trans person, a gap appears to exist between clinical practice and research in this field.78 Clinicians should proceed with caution, explain uncertainties to patients and recruit to research.
Policymakers ought to invest in both primary research and high-quality systematic reviews in areas relevant for CPG and service development. Organisations producing guidelines and aspiring to higher-level quality could use more robust methods, handling of competing interests79 80 and quality assessment. CPG developers should label key recommendations clearly. Although editorial independence was lowest priority for stakeholders, independent external review is important to avoid biases and bad practices, examine use of resources, resist commercial interests and gain widespread credibility outside the field.
The UK is fortunate in being familiar with developing priority-setting partnerships (eg, James Lind Initiative81) and generating suites of clinical questions that might cover all steps in patient pathways (eg, in partnership with Cochrane Collaboration82). These could underpin multidisciplinary and funded research priorities whose results feed into future better evidence-based CPGs. Implications for UK education and curricular content (eg, new gender identity healthcare credentials83), should be carefully scrutinised.
Internationally, CPG development and implementation will vary depending on local country contexts and available resources. Those countries with quality assurance agencies might use them for external assurance. Countries might reconsider the wisdom of adapting low-quality ‘off the shelf’ international CPGs without due assessment of the evidence for recommendations (eg, using the GRADE-ADOLOPMENT framework84). WHO demonstrates how CPGs can achieve high quality.
Patients should be positively encouraged to engage with CPG development as stakeholders. The lack of patient-facing material should be addressed, especially as medical and non-medical online material contains jargon, is unreliable and potentially misleading.85 Future CPGs should be populated with patient-facing decision aids (eg, fact boxes86 and icon arrays87) that explain sizes of benefits and harms to support informed patient choice. Patients and carers will benefit from a more focused approach to throughout-life healthcare. As the figures for gender minority/trans patients increase within the NHS and internationally, so does the need for consistent guidance to clinicians across specialisms on specific risks to, and means of treating, this population. Current patients should be welcomed to contribute, where they are comfortable, to any research being undertaken by their clinicians, in order to improve data and future practice for gender minority/trans health.
Unanswered questions and future research
This study should be replicated as new iterations of international CPGs become available. It can be applied to national guidelines and countries should perform their own stakeholder prioritisation. When ‘best available evidence’ is poor, quality improvement can be driven both from inside and outside the field. International guideline developers require more primary research for this population, and impetus from clinicians and scientists to build a better evidence base using robust data from randomised controlled trials and long-term observational cohort studies, especially regarding chronic diseases, health behaviours, substance use, screening and how interventions (eg, hormones) might impact on long-term health (eg, risk of cardiovascular and thromboembolic disease). Mortality and QoL data are required to address questions of clinical and cost-effectiveness.
Conclusion
Gender minority/trans health in current international CPGs seems limited to a focus on HIV or transition-related interventions. WPATH SOCv730 is due for updating and this study should be used positively to accelerate improvement. Future guideline developers might better address the holistic healthcare needs of gender minority/trans people by enhancing the evidence-base, upgrading the quality of CPGs and increasing the breadth of health topics wherein this population is considered.
Data availability statement
Data sharing statement: Additional data are available upon request.
Acknowledgments
We thank Richard Wakeford and Leena Järveläinen (information specialists, British Library and Turku University Library), Gillian Claire Evans (German translations), Sarah Peitzmeier, Sam Winter, Christina Richards and Riittakerttu Kaltiala (opinion leaders), Paul Seed (statistician), researchers who shared copies of their papers, the UK stakeholders who participated in the prioritisation exercise and the peer reviewers whose feedback improved the work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The authors were involved as follows: SB, IA, CM conception. All authors (SD, DC, IA, MHJ, SB, CM) were involved in design, execution, analysis, drafting manuscript and critical discussion; all were responsible for revision and final approval of the manuscript. All authors had full access to all the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. CM acts as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.