Article Text

Abstract
Purpose Prescription opioids (POs) are widely prescribed for chronic non-cancer pain but are associated with several risks and limited long-term benefit. Large, linked data sources are needed to monitor their harmful effects. We developed and characterised a retrospective cohort of people dispensed POs.
Participants We used a large linked administrative database to create the Opioid Prescribing Evaluation and Research Activities cohort of individuals dispensed POs for non-cancer pain in British Columbia (BC), Canada (1996–2015). We created definitions to categorise episodes of PO use based on a review of the literature (acute, episodic, chronic), developed an algorithm for inferring clinical indication and assessed patterns of PO use across a range of characteristics.
Findings to date The current cohort includes 1.1 million individuals and 3.4 million PO episodes (estimated to capture 40%–50% of PO use in BC). The majority of episodes were acute (81%), with most prescribed for dental or surgical pain. Chronic use made up 3% of episodes but 88% of morphine equivalents (MEQ). Across the acute to episodic to chronic episode gradient, there was an increasing prevalence of higher potency POs (hydromorphone, oxycodone, fentanyl, morphine), long-acting formulations and chronic pain related indications (eg, back, neck, joint pain). Average daily dose (MEQ) was similar for acute/episodic but higher for chronic episodes. Approximately 7% of the cohort had a chronic episode and chronic pain was the characteristic most strongly associated with chronic PO use. Individuals initiating a chronic episode were also more likely to have higher social/material deprivation and previous experience with a mental health condition or a problem related to alcohol or opioid use. Overall, these findings suggest our episode definitions have face validity and also provide insight into characteristics of people initiating chronic PO therapy.
Future plans The cohort will be refreshed every 2 years. Future analyses will explore the association between POs and adverse outcomes.
- epidemiology
- mental health
- pain management
- public health
Data availability statement
Data are available upon reasonable request. The IDEAs cohort was made possible through a multi-agency collaboration, including BCCDC, BCCDC Public Health Laboratory, BC Cancer and BC Ministry of Health. The integrated data set involved the linkage of de-identified case, laboratory testing and cancer data with health services administrative data. Authorised users have access to de-identified data based on roles and projects. Access to the de-identified data is not permitted outside of Canada. Use of the data is limited to the objectives described in the Information Sharing Plan. Individuals interested in becoming external collaborators may contact Dr Naveed Janjua (naveed.janjua@bccdc.ca). BCCDC requires all internal and external researchers with access to analytical data sets to complete annual or more frequent privacy/confidentiality and information security and awareness training, sign confidentiality forms and complete a concept note and data request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The data source used to create the Opioid Prescribing Evaluation and Research Activities (OPERA) cohort has broad coverage of British Columbia’s population (approximately one-third), has extensive linkage to a range of administrative healthcare databases and is refreshed every 2 years.
The OPERA cohort captures dispensations from all community pharmacies across British Columbia regardless of payer (unlike similar linked registries created in other jurisdictions which are often limited to specific insurance plans) and the current cohort includes 1.1 million people dispensed prescription opioids (POs) (estimated to be 40%–50% of PO use in the province).
The definitions used to characterise patterns of PO use in the OPERA cohort (ie, acute, episodic, chronic) were informed by a review of the literature and recommendations contained therein.
We developed an algorithm to infer clinical indication for episodes of PO use, although indication remained unknown for about a quarter of episodes.
The cohort is primarily made up of individuals tested for HIV or hepatitis C virus (HCV) and therefore results may not be generalisable to the entire population. Importantly, however, HIV or HCV testing are broadly offered to certain populations in British Columbia (eg, baby boomers, pregnant people, sexually active individuals).
Introduction
In North America, prescription opioids (POs) play a large role in the management of acute and chronic pain. While synthetic opioids have been used medically for over a century, it was not until the mid-1990s that prescription rates increased dramatically in several high-income countries, particularly the USA and Canada.1 2 Increases can be attributed to a number of factors including a heightened focus on pain management and aggressive marketing by pharmaceutical companies.1 3 Almost one in eight people in Canada are prescribed opioids each year4 and Canada consistently ranks within the top three consumers of POs globally.2 5 6
Evidence continues to emerge demonstrating the harmful effects of POs (overdose, death, dependence, among others)7–11 and limited effectiveness in managing long-term pain.12 13 In general, guidelines do not recommend opioids as first-line therapy for chronic non-cancer pain,14 15 but access to non-opioid interventions is often limited. While short-term PO use is considered appropriate for severe acute pain, transition from acute to chronic use remains a concern.16–18 In several jurisdictions, interventions have been introduced to reduce the over-prescription, non-medical use and diversion of POs.14 15 19 20 However, studies suggest some interventions may have facilitated transitions to the illicit market and contributed to the current illicit opioid epidemics facing North America.21 22
There is a clear need to monitor patterns of PO use and their harmful effects. Large, centralised pharmacy databases with linkage to medical data are increasingly being used to create registries of people using POs and answer critical research questions.23–26 While these linked data sets are a rich source of information, many are limited to specific insurance plans (as opposed to all payers) and lack information on clinical indication. Also, there is no formally validated or standardised approach for using these data sets to define different patterns of PO use (eg, acute, episodic, chronic).27 28 Therefore, prior to proceeding to more in-depth analyses, it is important to characterise PO use within a specified data source and assess the validity of selected definitions to the extent possible.
In British Columbia (BC), Canada, the Integrated Data and Evaluative Analytics (IDEAs) platform is a large linked data set with broad capture of the province’s population (1.7 million; approximately one-third of the population) and linkage to a range of administrative healthcare databases, including dispensations from all community pharmacies in BC.29 In the absence of routine surveillance of POs, IDEAs is a potentially important data source to answer research questions about PO use in BC.
In this cohort profile, we describe the use of IDEAs to create a subcohort of individuals dispensed POs for non-cancer pain, herein referred to as the Opioid Prescribing Evaluation and Research Activities (OPERA) cohort. We also describe the development of definitions to assess patterns of PO use, characterise PO use among study participants and assess the face validity of the definitions. Future OPERA analyses will examine the association between patterns of use and adverse outcomes, including initiation of injection drug use (IDU) and harms secondary to drug use (eg, overdose, hepatitis C virus (HCV) and HIV, endocarditis).
Cohort description
Data sources
We used the IDEAs data platform (which was developed from the British Columbia Hepatitis Testers Cohort) to create the OPERA cohort.29 The databases integrated within IDEAs and their linkage have been described previously (online supplemental table 1).29 In brief, IDEAs includes all individuals tested for HCV or HIV at the BC Centre for Disease Control Public Health Laboratory (BCCDC-PHL) between 1992 and 2015, as well as cases of HIV (1980–2015), HCV (1990–2015), hepatitis B virus (1990–2015) and active tuberculosis included in the public health registries of reportable diseases in BC. The BCCDC-PHL performs ~95% of all HCV/HIV testing in the province and the public health registries capture all diseases reported in the province. These data are linked to data on medical visits (1990–2015), hospitalisations (1985–2015), emergency department visits (2012–2015), cancers (1923–2015) and deaths (1985–2015), as well as prescriptions dispensed from community pharmacies in BC (PharmaNet).
Supplemental material
Approximately 1.7 million individuals are currently included in IDEAs. Importantly, IDEAs contains historical data on all participants and is not limited to data collected after an individual meets the inclusion criteria. New individuals are added to IDEAs every 2 years.
Data on pharmacy dispensations are extracted from PharmaNet. Since 1996, PharmaNet has collected information on prescription medications dispensed from all community and hospital outpatient (medications dispensed for patient use at home) pharmacies across BC, regardless of payer. Data is entered into PharmaNet by the pharmacist at the time of dispensation and includes a range of patient, pharmacy, prescriber and medication information, including drug and product identification number, unit dose, quantity (number of units dispensed), days’ of drug supply (estimated number of treatment days in dispensation) and payer (public or private).
OPERA cohort eligibility criteria
We used the IDEAs platform to create a retrospective cohort of individuals dispensed at least one PO for non-cancer pain between 1996 and 2015 (the OPERA cohort). Eligible PO medications included oral, sublingual, buccal, rectal and transdermal formulations of codeine, tramadol, oxycodone, hydromorphone, morphine, fentanyl, meperidine, anileridine, buprenorphine, butorphanol, levorphanol, methadone, oxymorphone, pentazocine, propoxyphene and tapentadol.
Low-dose codeine formulations (<30 mg per tablet), PO formulations primarily used for cough suppression or opioid agonist therapy (OAT) and injectable PO formulations were not included in our eligibility criteria.30 To limit the cohort to PO use for non-cancer pain, we also excluded all PO dispensations occurring after a cancer or palliative care diagnosis (online supplemental table 2).
Characterising PO use
We characterised patterns of PO use using an episode approach, as commonly done by others.24 31 Only eligible PO formulations (as described above) were used to create episodes. An episode starts with an index PO dispensation in which no drug supply was available in the previous 6 months and ends after another 6-month gap in drug supply (episode end date=date drug supply ran out). In instances where the days’ supply of separate dispensations overlapped, overlapping calendar days were only counted once in calculating the number of episode days covered by drug supply. With this approach, each episode has three key distinct but related measures: episode length (number of days between episode start and end date), days’ of drug supply (number of calendar days within an episode covered by drug supply) and episode intensity/consistency of use (per cent of episode days covered by drug supply).
Categorising PO episodes
We developed criteria to categorise PO episodes based on a review of the literature, with decisions informed by recommendations therein and those used by others. First, each episode was categorised as either acute or long-term based on episode length (table 1). Episodes with <90 episode days were considered acute and ≥90 days were long-term (episodic or chronic), as defined by the US-based Consortium to Study Opioid Risks and Trends group24 and used by others.25 28 Ninety days is a common threshold for several reasons: pain is generally considered chronic if persisting for longer than 3 months,14 32 3 months is an important clinical time point when PO effectiveness decreases and risks increase,13 33 and guidelines generally recommend 3 months as the optimal duration for an initial trial of POs for chronic pain (to be followed by an assessment of the harms/benefits of continuing therapy).14 32
Episode-level and individual-level criteria for categorising patterns of prescription opioids use, OPERA cohort
Next, we further classified long-term episodes as either episodic or chronic based on days’ of drug supply and episode intensity (table 1). We defined chronic episodes as long-term episodes with ≥90 days’ of drug supply and ≥50% episode intensity (table 1). Long-term episodes that did not meet the chronic definition were classified as episodic. The 50% episode intensity threshold is one of the cut-offs used by other research teams in BC to characterise long-term episodes (<20%=occasional, 20%–49%=regular/intermittent, 50%–89%=chronic, ≥90%=every day)30 31 and was empirically derived (represents the median value for long-term episodes with ≥90 days’ supply).31 It also agrees with the US CDC’s (Centers for Disease Control and Prevention) definition of long-term PO therapy (ie, ‘use of opioids on most days for >3 months’).15
Few studies directly incorporate consistency of use (episode intensity) into their long-term PO definitions.28 However, our team considered this parameter important for several reasons: inclusion was recommended in a systematic review of long-term PO therapy definitions,28 the US CDC definition of long-term therapy refers to consistency of use (ie, ‘most days’)15 27 and episode intensity has been used by other research teams in BC.30 31 Also, median episode intensity for long-term episodes in the OPERA cohort is low (18.6%), and lower intensity episodes are likely more suggestive of episodic than chronic use.
We also assigned each individual to a PO use category based on patterns of episodes over their follow-up time in the cohort (table 1).
Assessment of episode-level covariates
In the OPERA cohort, we measure a number of characteristics for each PO episode. These include episode type (acute, episodic, chronic), number of dispensations, episode length, days’ of drug supply, intensity of use, average daily dose in morphine equivalents (MEQ), most frequently prescribed PO medication (based on days’ of drug supply), concomitant use of other medications (benzodiazepines, gabapentinoids), inferred clinical indication, among others.
Average daily dose is estimated by summing the MEQ for all dispensations within an episode and dividing the cumulative MEQ by the sum of episode days (includes gaps in use) or days’ of drug supply. Dose for each dispensation is calculated by multiplying the quantity of units dispensed (eg, tablets) by unit dose. Unit dose is converted to MEQ using available conversion tables.34
Mutually exclusive indication is inferred for each episode using an algorithm developed by our team and adapted from others.35 36 The approach is summarised in online supplemental figure 1 and table 3. In brief, our stepwise hierarchical process includes (1) identifying dispensations prescribed by a dentist, (2) examining Canadian Classification of Diagnostic, Therapeutic and Surgical Procedures (CCP) and Canadian Classification of Health Interventions (CCI) procedure codes from hospitalisation records in the 5 days prior to episode start to identify dental-, obstetric- and surgery-related visits, (3) categorising International Classification of Diseases (ICD)-9 and ICD-10 diagnostic codes from physician/hospitalisation records in the 5 days prior to episode start into diagnostic pain clusters36 37 based on a list of ICD codes published by Mayhew et al36 and (4) reviewing an aggregate list of the most common diagnostic, billing and procedure codes from unassigned episodes and categorising them into existing or newly created clusters. Since a large proportion of episodes had no indication assigned after applying the preceding steps (eg, 33% of chronic episodes), we added a final step in which we assessed for lifetime history of chronic pain prior to episode start (online supplemental table 2).38 39
Individual-level covariates
The linked data sets can be used to measure a range of sociodemographics (eg, sex, geography, social/material deprivation)40 and health conditions (eg, mental illness, problems related to drug and alcohol use, IDU,41 HIV, HCV, chronic pain,38 39 Elixhauser Comorbidity Index42). More information on covariate measurement used in this paper can be found in online supplemental table 2.
Patient and public involvement in research
This cohort was developed without patient involvement due to the retrospective/administrative/de-identified nature of the data sources. Technical decisions related to cohort development were informed by a review of the literature. The OPERA cohort and research agenda were developed in response to concerns expressed by patients and the public regarding the contribution of POs to the illicit overdose crisis in BC. These concerns were brought forward to members of the research team through peer-based organisations of people with lived and living experience of substance use, the media, concerned friends and family members, providers and provincial committees involved in the overdose response. Interpretation and dissemination of OPERA findings will be informed by these committees and peer-based organisations.
Findings to date
Cohort creation
Overall, there were a total of 22 117 510 PO dispensations to 1 222 410 individuals between 1996 and 2015 (figure 1). After applying exclusions, 20 463 374 dispensations and 1 179 024 individuals were included in the OPERA cohort.
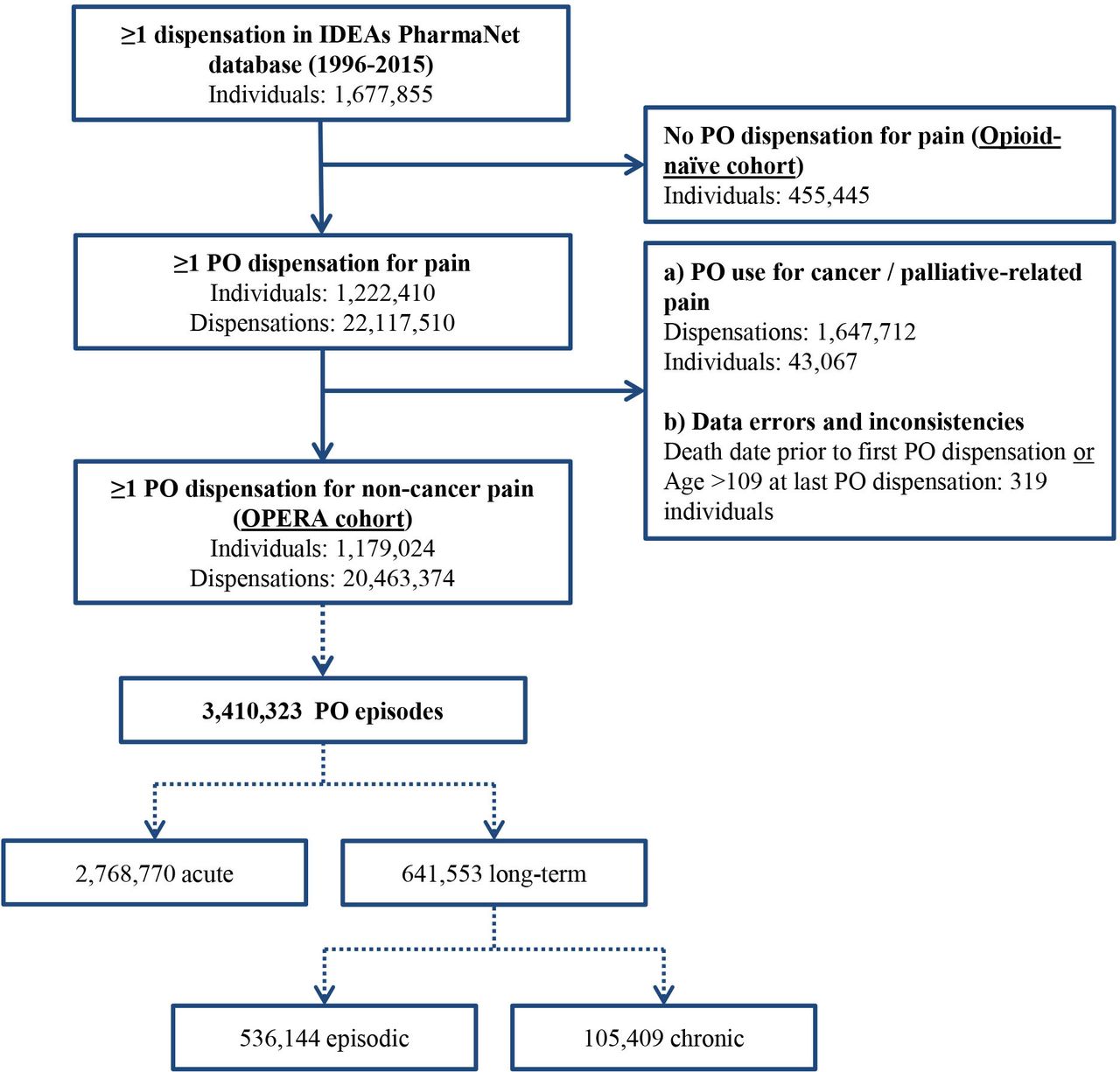
Study flow chart and breakdown of PO episode types, OPERA cohort, 1996–2015. Solid line indicates breakdown of individuals and dispensations. Dotted line indicates breakdown of PO episode types. IDEAs, Integrated Data and Evaluative Analytics platform; PO, prescription opioid; OPERA, Opioid Prescribing Evaluation and Research Activities.
Patterns of PO use
Similar to other studies, most PO use in the cohort was acute (figure 2 and table 2) and dispensed for dental or surgical pain (table 3), but chronic use contributed disproportionately to overall consumption of POs (figure 2).24 31 35

Distribution of episode-level and individual-level PO categorisations and their contribution to cumulative morphine equivalents in the OPERA cohort, 1996–2015. See table 1 for episode-level and individual-level definitions. Example interpretation: 81.2% of all episodes were acute and acute episodes made up 3.6% of all MEQ in cohort (episode-level); 70.4% of individuals had acute episodes only and these individuals made up 2.0% of all MEQ in cohort (individual-level). Individual-level MEQ calculated based on all PO use across an individual’s history (eg, all chronic, episodic and acute use). MEQ, morphine equivalents; PO, prescription opioids.
Characteristics of prescription opioid episodes by episode type, OPERA cohort, 1996–2015
Inferred clinical indication by episode type, OPERA cohort, 1996–2015
As of the end of 2015, there were a total of 3 410 323 PO episodes (figure 1). The majority of episodes were acute (81.2%) and the remainder long-term. Approximately 67% and 82% of long-term episodes contained <90 days’ supply or <50% intensity, respectively. After further categorisation of long-term episodes, 15.7% (536 144) of all episodes were episodic and 3.1% (105 409) were chronic (figures 1 and 2). Chronic episodes made up 88.2% of the total MEQ in the cohort, followed by episodic (8.1%) and acute (3.6%) (figure 2).
By definition, chronic episodes contained more days’ supply and were more intense than episodic episodes (table 2). Most acute episodes involved only a single dispensation and therefore had the highest intensity. Episodic episodes likely represent a combination of PO use for intermittent long-term pain or repeat instances of PO use for unrelated acute incidents. Certain characteristics of episodic episodes, such as average daily dose and most frequently prescribed PO, were more similar to acute than chronic.
Of the 1 179 024 individuals in the cohort, 95.6% had ≥1 acute episode, 26.2% had ≥1 episodic episode and 7.4% had ≥1 chronic episode (online supplemental table 4). Based on our mutually exclusive hierarchical individual-level use categorisations (table 1), 70.4% (830 152) were classified as acute only, 22.2% (261 116) as episodic and 7.4% (87 756) as chronic (figure 2).
There was substantial overlap between types of use across the individual-level categorisations (online supplemental table 4). For example, 74.5% and 54.0% of individuals with chronic use also had ≥1 acute or episodic episode, respectively. However, the majority (83.0%) of chronic-exposed individuals had only one chronic episode.
Most common formulations
Of the 20 million PO dispensations, the most commonly dispensed were codeine (53.6%), oxycodone (14.8%), morphine (13.5%), hydromorphone (8.8%), tramadol (3.6%), fentanyl (1.5%), methadone (1.5%) and meperidine (1.4%). The vast majority (97.9%) of codeine dispensations were for 30 mg tablet formulations.
Codeine was the most frequently prescribed opioid across all episode types, with oxycodone, morphine and hydromorphone the next most common for chronic episodes and tramadol the second most common for acute episodes (table 2 and online supplemental table 5). The 2010 Canadian opioid prescribing guidelines suggested morphine, oxycodone or hydromorphone for severe chronic non-cancer pain, and codeine or tramadol for mild-to-moderate pain.43
Codeine was the most frequently prescribed PO for almost half of chronic episodes and a quarter of chronic episodes contained codeine only (table 2). While codeine is generally considered to have less dependence potential,44 a provincial report on PO-related deaths from 2009 to 2013 in BC found that almost 25% of deaths involved codeine (second only to methadone for maintenance treatment).45 A similar finding was observed in Ontario46 and a review of the literature concluded that ‘[w]eak opioids require at least as much vigilance as morphine, despite the major differences in their reputation and regulation’ largely due to codeine’s unpredictable pharmacokinetics.47
Higher doses and concomitant drug use
Previous studies have identified higher PO doses and concurrent benzodiazepine or gabapentinoid use as risk factors for overdose and mortality.7 9 48–51 Guidelines for chronic non-cancer pain generally recommend that clinicians use caution when prescribing daily doses ≥50 MEQ and avoid increasing to ≥90 MEQ.14 32 In our cohort, average daily doses ≥50 MEQ were present in about 1 in 10 acute/episodic episodes and 1 in 3 chronic episodes (increasing to 1 in 2 after exclusion of chronic episodes with codeine as the most frequently prescribed PO) (table 2 and online supplemental table 6). Further, about 70% and 40% of chronic episodes had an overlapping benzodiazepine or gabapentinoid dispensation, respectively (table 2).
Transitions from acute to long-term use
PO therapy for acute pain represents an important area for study due to the risk of transition to long-term use. However, given our approach to creating PO episodes (ie, a 6-month gap in drug supply is required to mark the end of an episode), the majority of these transitions would be captured within the same long-term episode. Regardless, we noted some evidence of acute to long-term transitions: the most common indications for long-term episodes were acute-related (dental, surgical) and surgical pain was one of the most common indications for chronic episodes (table 3).
Face validity of PO episode definitions
We assessed the face validity of our episode-level definitions (ie, the extent to which our definitions subjectively seemed to identify what they were supposed to identify) by examining the presence of expected trends across episode types and by comparing our findings to other literature.
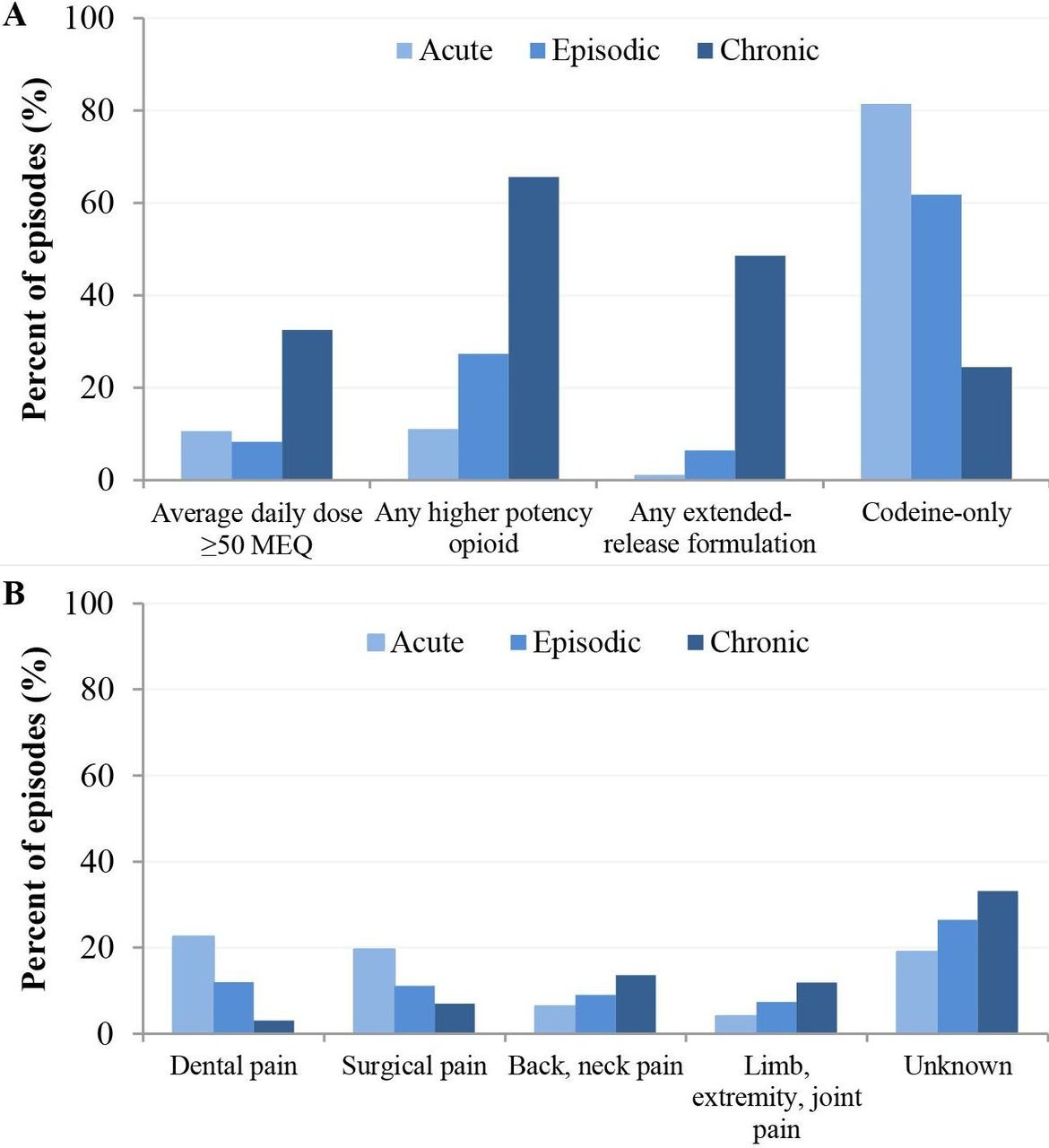
Our episode-level classifications appeared to have face validity. As would be expected, across the acute to chronic gradient, there was an increasing prevalence of higher potency POs (hydromorphone, oxycodone, fentanyl, morphine),4 long-acting formulations and chronic pain-related indications (eg, back, neck, joint pain) and a decreasing prevalence of codeine use and acute-related indications (eg, dental, surgical pain) (figure 3). Average daily dose (MEQ) was similar for acute/episodic but higher for chronic episodes. In accordance with guidelines, the majority of acute episodes (~70%) contained ≤7 days’ supply of medications (table 2).32 52 Half of chronic episodes were longer than 2.5 years and a quarter longer than 7 years (increasing to 3.5 and 8 years, respectively, when codeine-only episodes were excluded) (table 2), which is comparable to studies of people known to be using POs to manage non-cancer chronic pain.53–55 For example, at enrolment in a large Australian prospective cohort of individuals using morphine, oxycodone, buprenorphine, methadone or hydromorphone, half of the 1514 participants had been using POs for longer than 4 years and a quarter longer than 10 years.54
{kind=link}
{kind=link}
{kind=link}
Prevalence of episode characteristics by episode type. (A) Dose and prescription opioid formulation by episode type. (B) Inferred indication by episode type. Average daily dose uses days’ of drug supply as denominator. Higher potency opioids=hydromorphone, fentanyl, morphine or oxycodone. ‘Limb, extremity and joint pain’ indication also includes arthritic disorders, neuropathy and fibromyalgia. Average daily dose uses days’ of drug supply as the denominator. MEQ, morphine equivalents.
Characteristics of people with chronic PO use
Matched case–control analyses were used to identify characteristics associated with being an individual with a chronic episode. The purpose of this analysis was to identify differences in sociodemographic and clinical characteristics between the individual-level user types in table 1. We matched participants with a chronic PO episode (cases) to three different types of controls who did not have record of chronic PO use (PO-naïve, acute-only, episodic; table 1). Each case was matched 1:1:1:1 on birth year to each type of control (additional details on methods are described in notes of table 4). Index date for measurement of characteristics was start date of first chronic episode for cases and for controls it was the index date of their matched case (thereby controlling for differences in age). In these matched case–control analyses, history of chronic pain was the characteristic most strongly associated with being an individual with a chronic episode (table 4). This finding further supports the face validity of our episode definitions.
Characteristics by individual-level PO use categories and predictors of chronic use identified in multivariable case–control analyses, OPERA cohort, 1996–2015
In addition to chronic pain, individuals initiating a chronic episode were also more likely to have higher social/material deprivation and prior experience with a major mental illness (28.2%) or a problem related to opioid (7.7%) or alcohol (16.5%) use (table 4). Taken together, these findings support a 2019 report by the Canadian Pain Task Force (CPTF) noting that the burden of chronic pain is not distributed equally and that ‘social determinants can lead to a complex interplay between chronic pain, mental health and substance use disorders.’56 Indeed, studies have identified a higher prevalence of chronic pain among people who use drugs56–59 and noted the ‘complex demographic and clinical profiles’54 of people with long-term PO use.23 31 54 Guidelines for chronic non-cancer pain generally recommend caution when prescribing opioids to people who may be at higher risk of adverse PO-related outcomes, such as people who use drugs or have a psychiatric disorder.14 32 However, adequate non-opioid options are often unavailable and unmet pain management needs can negatively impact quality of life and could potentially lead to the use of illicit drugs to treat pain (and a subsequent increased risk of harms, such as overdose).56 58 60 61 The CPTF report states that it is important to ‘promote shared decision-making between healthcare professionals and people living with pain’ and ‘support opioid prescribing that balances the benefits and harms of these medications based on the needs of the individual’.56
Strengths and limitations
We created a large retrospective cohort of more than 1 million individuals dispensed POs for non-cancer pain in BC over a 20-year period (1996–2015). Based on a review of the literature and recommendations therein, we developed criteria to categorise patterns of PO use at the episode-level and individual-level. These criteria incorporate intensity/consistency of PO use, which is recommended in the literature but uncommon in other studies. To assess the face validity of these categorisations and provide a methodological reference for future OPERA publications, we compared episode types and individuals across a range of characteristics. Findings to date suggest our episode definitions have face validity. Future OPERA analyses will examine the association between patterns of use and adverse outcomes, including initiation of IDU and harms secondary to drug use (eg, overdose, HCV and HIV, endocarditis).
OPERA is one of the largest linked cohorts of people using POs available worldwide, will be refreshed every 2 years and has extensive linkage to administrative healthcare databases. A one-time descriptive analysis of all individuals in BC has been conducted by another research team and analysed trends over time between 2005 and 2012.31 Based on the sample size of this other analysis, we estimate that the OPERA cohort captures approximately 40%–45% of individuals dispensed POs and 45%–50% of long-term PO use in the province. Importantly, the OPERA cohort includes all community pharmacy dispensations regardless of payer—unlike similar linked registries in other jurisdictions which are often limited to specific insurance plans. Of note, studies using centralised pharmacy data from state-wide prescription drug monitoring programmes in the USA are beginning to emerge and will be valuable data sources.26 62
Results from our cohort may not be generalisable to the BC population. While we estimate that the OPERA cohort captures 40%–50% of PO use in the province, it is primarily made up of individuals tested for HIV or HCV.29 Therefore, people at higher risk for HIV/HCV infection are likely overrepresented in the cohort, potentially leading to a higher prevalence of certain characteristics (eg, substance use problems). Importantly, however, HIV or HCV testing is broadly offered to certain populations (eg, baby boomers, pregnant people, sexually active individuals). Also, while we attempted to limit our cohort to POs dispensed for non-cancer pain, we likely also included use for other reasons (eg, euphoric effects, dependence, off-label OAT).
Several additional limitations warrant mention. Data on PO use (eg, dose, duration) is inferred from administrative pharmacy data and may not reflect actual use. For example, dispensed POs may not have been consumed and could have been diverted. Also, due to overlapping dispensations, average daily dose is likely overestimated and episode length underestimated. Further, some episodes are truncated by the start/end dates of our study, leading to reduced episode length. Our ability to study acute to long-term transitions is limited by the requirement of a 6-month gap without drug supply to mark the end of a PO episode. While we are able to infer clinical indication for a large proportion of episodes, it remained unknown for a sizeable proportion, similar to another study.24 However, expected trends in indications across episode types were present regardless of whether episodes with an unknown indication were included in the denominator (table 3 and online supplemental table 7). Another limitation is our reliance on diagnostic codes from physician and hospitalisation records which can lead to misclassification of health conditions and inferred indications. Further, diagnostic codes in the 5 days prior to initiation of an opioid episode may be unrelated to indication. While we comprehensively assessed the face validity of our episode-level PO definitions in this paper, formal validation is still lacking. Finally, the descriptive statistics in our analysis are unlikely to have been consistent across our study period. We intend to assess the evolution of PO patterns over time in future analyses, although some studies examining time trends in BC have already been published.31
In conclusion, our large linked administrative cohort will be a valuable tool for answering research questions about PO use in BC. Future OPERA analyses will evaluate the association between different patterns of PO use and adverse outcomes, the intended/unintended impacts of PO-related policies and the effectiveness of individual-level interventions to reduce adverse outcomes.
Collaboration
We are open to collaborating on projects related to POs. The IDEAs cohort was made possible through a multi-agency collaboration, including BCCDC, BCCDC-PHL, BC Cancer and BC Ministry of Health. The integrated data set involved the linkage of de-identified case, laboratory testing and cancer data with health services administrative data. Authorised users have access to de-identified data based on roles and projects. Access to the de-identified data is not permitted outside of Canada. Use of the data is limited to the objectives described in the Information Sharing Plan. Individuals interested in becoming external collaborators may contact Dr Naveed Janjua (naveed.janjua@bccdc.ca). BCCDC requires all internal and external researchers with access to analytical data sets to complete annual or more frequent privacy/confidentiality and information security and awareness training, sign confidentiality forms and complete a concept note and data request.
Data availability statement
Data are available upon reasonable request. The IDEAs cohort was made possible through a multi-agency collaboration, including BCCDC, BCCDC Public Health Laboratory, BC Cancer and BC Ministry of Health. The integrated data set involved the linkage of de-identified case, laboratory testing and cancer data with health services administrative data. Authorised users have access to de-identified data based on roles and projects. Access to the de-identified data is not permitted outside of Canada. Use of the data is limited to the objectives described in the Information Sharing Plan. Individuals interested in becoming external collaborators may contact Dr Naveed Janjua (naveed.janjua@bccdc.ca). BCCDC requires all internal and external researchers with access to analytical data sets to complete annual or more frequent privacy/confidentiality and information security and awareness training, sign confidentiality forms and complete a concept note and data request.
Ethics statements
Ethics approval
This study was approved by the University of British Columbia Research Ethics Board (H14-01649).
Acknowledgments
We acknowledge the assistance of the Provincial Health Services Authority, BC Ministry of Health and BC Cancer staff involved in data access, procurement and management. This work was carried out on the unceded traditional and ancestral territories of the Coast Salish peoples. We gratefully acknowledge the residents of British Columbia whose data are integrated in the IDEAs data platform / British Columbia Hepatitis Testers Cohort; Alexis Crabtree, Kate Smolina and Kathy McInnes for developing the list of prescription opioids and morphine equivalent conversions used in this analysis; and Mayhew et al (DOI: 0.1016/j.jpain.2019.05.006) for developing and publicly posting the ICD codes for identifying diagnostic pain clusters (codes/clusters were adapted in our paper to infer clinical indication; see Mayhew et al manuscript for the publicly accessible GitHub link).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Primary investigators (JAB, NZJ, RP) and co-investigators (TG, RCD, RFB, MO) of the OPERA project initiated and conceived of the project. NZJ leads the IDEAs/BC-HTC and MA, SW and AY are involved in data management. OPERA project administration/supervision is provided by JAB, RP, NZJ and MA. JAB, NZJ, RP, JW and YA planned and designed the analyses. MC and YA created the analytical data set with assistance from SW and AY. JW conducted the analysis and wrote the manuscript. MC, YA, RP, AM, TG, RCD, RFB, MO, SW, AY, MA, NZJ and JAB critically revised the manuscript and contributed to interpretation of the data. All authors read and approved the final version of the manuscript.
Funding This work was supported by BC Centre for Disease Control and the Canadian Institutes of Health Research (PJT-156117, NHC–142832).
Disclaimer All inferences, opinions and conclusions drawn in this manuscript are those of the authors, and do not reflect the opinions or policies of the Data Steward(s).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.