Article Text

Abstract
Objectives To summarise current evidence on the use of pentoxifylline (PTX) to prevent contrast-induced nephropathy (CIN).
Methods The PubMed, Embase and CENTRAL databases were searched for randomised controlled trials including patients with and without PTX undergoing contrast media exposure. We analysed the incidence of CIN and serum creatinine changes before and after contrast media exposure. All statistical analyses were conducted with Review Manager V.5.3.
Results We finally enrolled in seven randomised controlled trials with a total of 1484 patients in this analysis. All of seven included studies were performed in patients undergoing angioplasty or stenting. The overall rates of CIN were 8.8% and 10.4% in the PTX groups and control groups, respectively. However, no significant reduction in the CIN rate was observed in the patients treated with PTX compared with the control groups (OR 0.81, 95% CI 0.57 to 1.13, I2=0, p=0.21). All studies reported no hospital mortality and the new requirement for dialysis during the trials.
Conclusion Perioperative administration of PTX to patients undergoing angioplasty did not significantly reduce the development of CIN but showed some weak tendency of lower serum creatinine increase. Based on the available trials, the evidence does not support the administration of PTX for the prevention of CIN. More trials with larger sample sizes are needed to evaluate the role of PTX in CIN prevention.
- radiation biology
- interventional radiology
- acute renal failure
- coronary intervention
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first meta-analysis to summarise current evidence of pentoxifylline for the prevention of contrast-induced nephropathy.
The results were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist and Cochrane handbook.
Given the small number of trials included in each analysis, we failed to assess publication bias and small study effects with funnel plots.
Introduction
Contrast-induced acute kidney injury (AKI), which is also known as contrast-induced nephropathy (CIN), is defined as the development of AKI following contrast medium exposure, without an alternative aetiology.1 With the wide application of cardiac catheterisations and nearly 30 million doses of contrast media injection annually,2 CIN constitutes the third leading cause of hospital-acquired AKI.3 CIN is associated with the in-hospital need for dialysis, long-term kidney failure and overall mortality and consequently prolongs hospital stay and increases the cost of hospitalisation.4 Even if serum creatinine (Scr) would recover to the baseline quickly in most CIN patients, these patients still suffer worse long-term outcomes than those without CIN.5 In light of the vast threat to people’s health and public costs, it has become imperative to research the prevention of CIN.
Pentoxifylline (PTX) is a methyl-xanthine derivative with powerful antioxidative, anti-inflammatory and anti-immunity properties. It is generally used to treat peripheral vascular diseases. PTX improves the flexibility and oxygen delivery capacity of red blood cells, resulting in improved haemodynamics. In addition, studies in animal models showed that PTX could effectively attenuate kidney injury induced by contrast media or Escherichia coli.6 7 In fact, several clinical trials have suggested that PTX may be a potential candidate for renal protection.8–10
PTX has been investigated in randomised controlled trials (RCTs) as a potential agent to prevent CIN.11–17 However, neither systematic reviews nor meta-analyses have been conducted to date to the best of our knowledge. Therefore, we performed this systematic review and meta-analysis of currently available RCTs to summarise and evaluate the renal protective capacity of PTX under contrast media stress.
Material and methods
Search strategy
We searched electronic databases (PubMed, Embase and Cochrane Central Register of Controlled Trials (Central)) for potential clinical trials up to 29 June 2020 with no language restriction, using combinations of the main terms ‘contrast-induced nephropathy’ and ‘pentoxifylline’. The details of the search strategy are shown in online supplemental appendix 1. Two authors (LW and DL) performed the literature search independently. We also checked relevant reviews and the reference lists of the original articles for further suitable publications.
Supplemental material
Study selection
LW and DL independently screened the titles, abstracts or full texts and assessed their eligibility. We included studies that met the following criteria: RCTs enrolled population underwent contrast media exposure, trials used PTX for prevention of CIN and trials reported CIN rate and/or Scr change after exposure. The exclusion criteria were: animal studies, non-RCTs and lack of necessary data. Any disagreements were resolved by discussion with a third author (WZ).
Data extraction
Two independent reviewers (LW and DL) extracted data from each eligible study. Data extracted from studies included study characteristics, patient characteristics, details regarding PTX groups and control groups, and outcome assessments. Outcomes of interest for this study were the incidence of CIN and Scr changes after exposure.
Risk of bias
The risk of bias was assessed through the Cochrane Collaboration Tool. Six domains were evaluated: sequence generation for randomisation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other sources of bias. According to Cochrane Handbook,18 The risk of biases are classified into three categories: low risk, unclear risk and high risk. Low risk meant all categories were classified as low risk. Unclear risk means one category was classified as unclear risk. High risk means high risk of bias in one or more categories or an unclear risk in two or more categories.
Outcomes
The primary outcome was the incidence of CIN, defined as a minimum 0.5 mg/dL or 25% increase in Scr 48 hours after contrast media exposure. The secondary outcomes were Scr change after exposure, defined as the difference between Scr after and before the procedure, hospital mortality and the new requirement for dialysis. The general population was defined as having a Mehran score <11, and the high-risk patients were defined as the population with Mehran score ≥11. Subgroup analysis of low-risk and high-risk patients was performed when possible.
Statistical analysis
Meta-analysis was performed using Review Manager V.5.3. We used χ2 and I2 to verify the heterogeneity among the studies. Values of the index of under 25%, between 25% and 50% and over 50% indicated low, moderate and high heterogeneity, respectively. Statistical significance of heterogeneity was set at a p value of 0.05. If no substantial heterogeneity was observed (p≥0.05 or I2<50%), the fixed-effect model was used. Conversely, we presented the results with the random effect model. Mean difference and OR with the 95% CI were used to evaluate the continuous and binary variables, respectively. Sensitivity analysis was performed to detect the robustness and reliability of our results by sequentially omitting every single study. We used the funnel plot to evaluate the potential publication bias.
Results
Study selection and characteristics of included studies
Figure 1 shown the literature searching process. We found 109 records from the database. After exclusion of duplicates and irrelevant studies (21 reviews, 3 case reports, 10 animal studieds, 5 comments and 45 no relevant studies), we finally enrolled seven RCTs11–17 with a total of 1484 patients in this meta-analysis. The characteristics of the included trials were presented in table 1. All of seven included studies were performed in patients undergoing angioplasty or stenting. Five of seven trials enrolled patients from the general population11–15; one study enrolled diabetic patients,16 and the remaining six study enrolled high-risk patients.17 All the enrolled patients were prehydrated with normal saline. In addition, Aslanabadi’s and Barzi’s studies16 17 used 600 mg N-acetyl cysteine orally twice daily before and after the procedure. There were 740 patients in the PTX group and 744 in the control group.
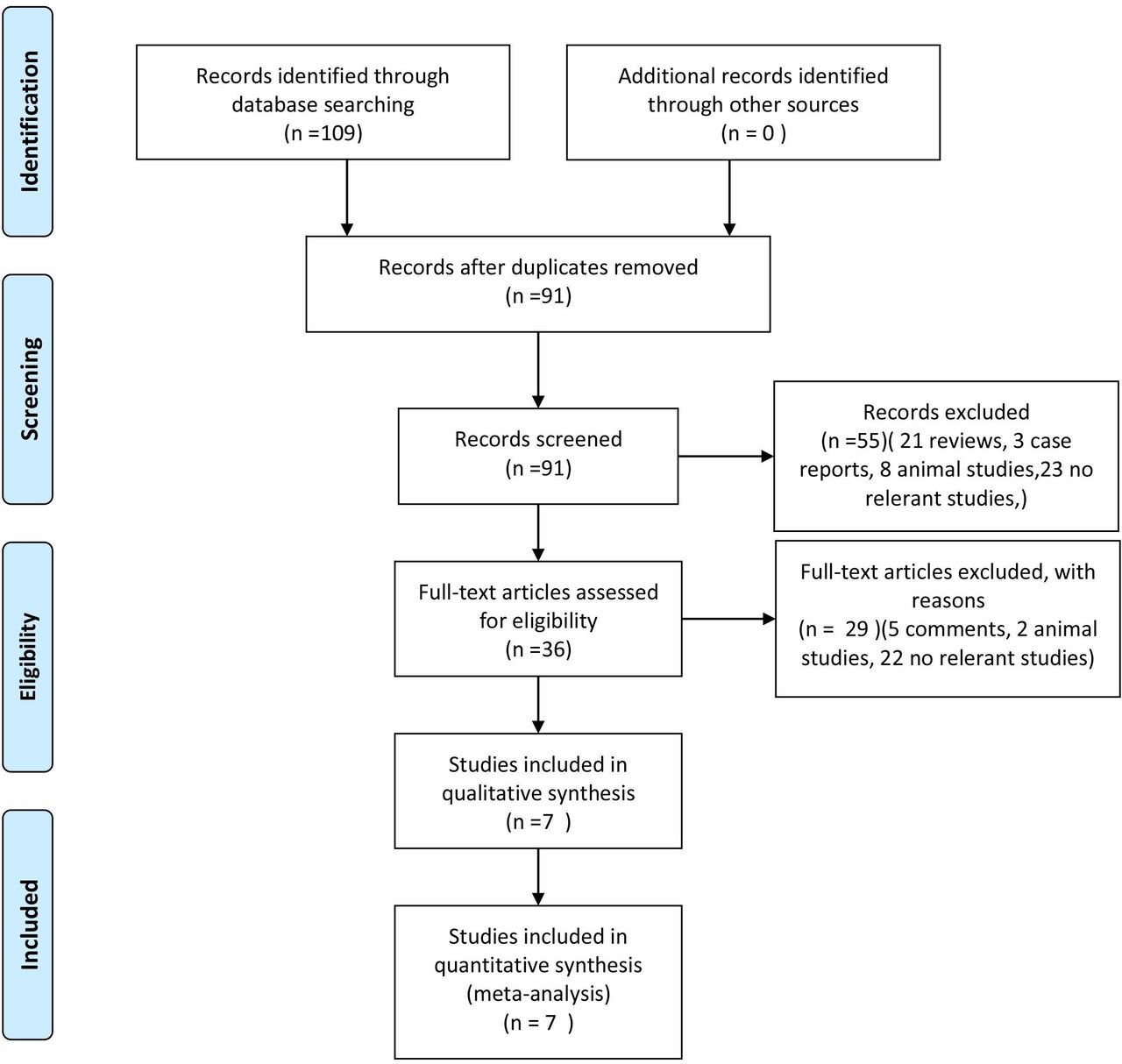
Flow chart of the literature searching process.
Baseline characteristics of included studies
Primary outcome
Data on the incidence of CIN were available in all studies included in this meta-analysis. The overall rates of CIN were 8.8% and 10.4% in the PTX groups and control groups, respectively. However, no significant reduction in the CIN rate was observed in the patients treated with PTX compared with the control groups (OR 0.81, 95% CI 0.57 to 1.13, I2=0, p=0.21) (figure 2). Similarly, the incidences of CIN were also comparable between groups in the the general population subgroups (OR 0.79, 95% CI 0.56 to 1.12, I2=8%, p=0.19) (figure 3).

Evaluation of the incidence of contrast-induced nephropathy between the pentoxifylline group and the control.

Evaluation of the incidence of contrast-induced nephropathy in the the general population subgroups between the pentoxifylline group and the control.
Secondary outcome
Data on Scr change after exposure were available in four of seven trials.13 15–17 However, the study report by Eshraghi et al 15 contributes most of the data. Thus the meta-analysis of Scr was waived. All studies reported no hospital mortality or the new requirement for dialysis during the trials.
Risk of bias assessment and sensitivity analysis
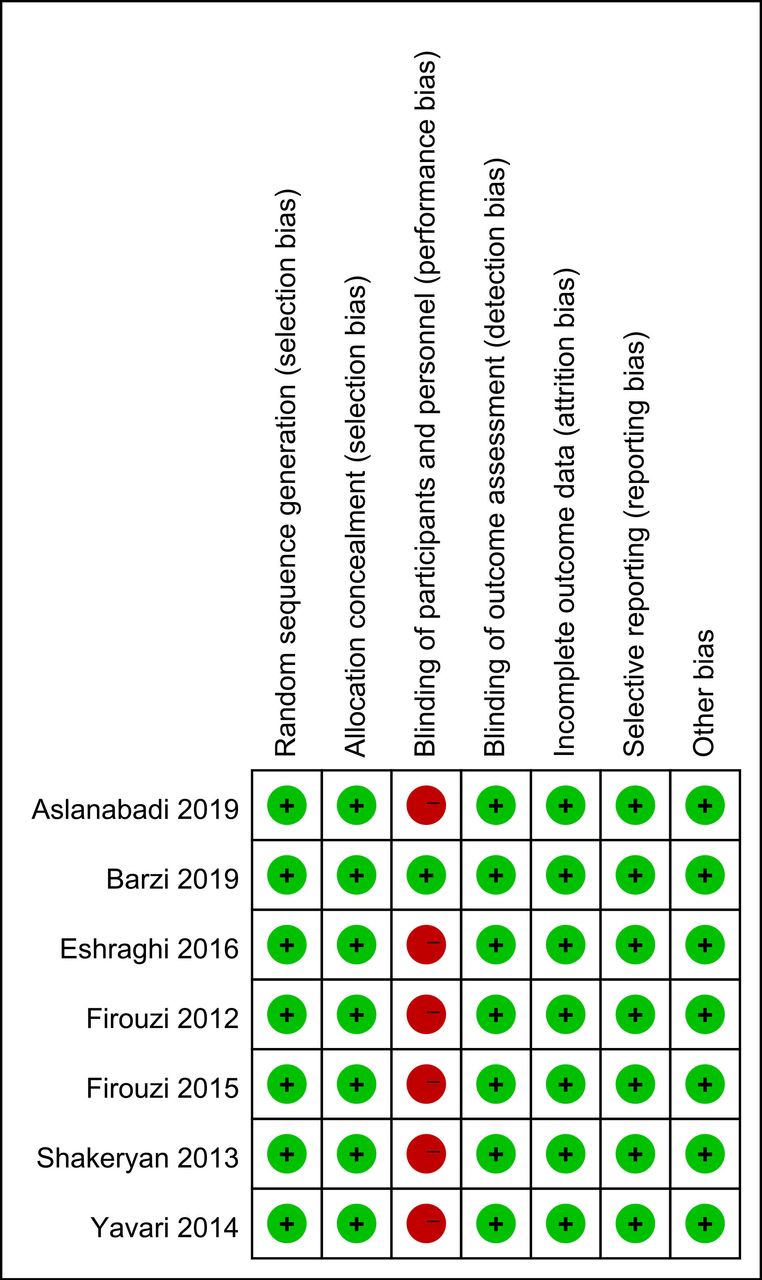
The risk of bias is presented in figure 4. Six studies did not use the placebo as control and were thus not blinded.11–16 However, the development of CIN and Scr changes are objectively defined and hence less likely to bias. Outcome assessors in all trials were blinded to the trial protocol. All trials were free of selective outcome reporting.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of bias assessment of included studies.
Given the limited number of studies included in this meta-analysis, the funnel plot is not applicable for evaluating the publication bias and small-study effects.
Sensitivity analysis was performed by sequentially omitting every single study. CIN rate remained comparable between groups after excluding each trial, indicating that our results were reliable and not skewed by a single dominant study.
Discussion
This is the first systematic review and meta-analysis to summarise current evidence of PTX for the prevention of CIN. The results suggested that perioperative administration of PTX to patients undergoing angioplasty or PCI significantly lower Scr increase but did not significantly reduce the development of AKI.
Our primary outcome was the incidence of CIN. There was no significant impact of PTX on this predefined primary outcome. A reasonable explanation was that although we pooled seven studies with a total of 1484 patients in this meta-analysis, the number of CIN rates was limited. Therefore, the CIs for the CIN prevention effect of PTX treatment are wide and low statistical power results in poor precision. Consequently, the results of these trials should be cautiously interpreted, and more trials with larger sample sizes are needed to evaluate the role of PTX in CIN prevention.
However, it is interesting to note that perioperative therapy with PTX did reduce Scr changes in some studies,13 15–17 although the reduction was small (just 0.01–0.04 mg/dL). In a database analysis, Weisbord and colleagues19 reported that even a small increase (0.25–0.50 mg/dL) in postoperative Scr was associated with adverse outcomes in the coronary arteriography population. Losito and colleagues20 also showed that the increase in Scr below the AKI threshold (a 20% increase) is still closely correlated with increased long-term mortality. It would be interesting to study whether the reduction of Scr change and adverse outcomes would show a dose–response effect. Therefore, PTX’s impact on Scr may raise growing interest in future studies as a potential agent for renoprotection to CIN. Besides, compared with de novo drug development for CIN prevention, repurposing PTX obviously saves money and time, and it can be speedily applied in clinical practice.
Effective prevention strategies and strengthened management are the keys to reduce the CIN incidence. Choosing the optimal contrast medium, reducing contrast volume and personalised hydration are direct and effective strategies to reduce CIN. In addition, remote ischaemic preconditioning and statins have potential benefits for patients at risk for CIN, but their efficacy needs further study.21–27
CIN is a kind of AKI with complex and poorly understood mechanisms. Several studies have found that contrast media would lead to renal vascular contraction and a subsequent decrease of peripheral medullary blood flow, resulting in renal tubular anoxia and oxidative stress injury.28 29 Besides, a higher concentration of contrast agent in the renal tubular leads to viscosity increase and results in tubule blocked.30 PTX is a methyl-xanthine derivative with multiple biochemical properties and is commonly used to treat peripheral vascular disease caused by peripheral vascular disease.31 PTX is a non-selective inhibitior of phosphodiesterases, which can increase the intracellular levels of cyclic adenosine monophosphate (cAMP), leading to an improvement of oxygen delivery and a decrease of oxygen free radicals production.32 This property, together with its capability of reducing blood viscosity and therefore increasing intraglomerular pressure,33 34 supporting the speculation on underlying renoprotective effects of PTX. Prehydration and posthydration with intravenous saline or even drinking a few cups of broth can also reduce the blood viscosity, and periprocedural hydration may be the most effective preventive measure for patients at risk of CIN. However, hydration may increase the risk of heart failure, arrhythmia and short-term mortality in high-risk patients. Therefore, the reduction in blood viscosity of PTX should not be ignored.
The present study had several limitations. First, most studies used Scr to evaluate the renal function, and only three trials reported Scr changes before and after contrast media exposure. Future studies should use more sensitive markers to assess the renal function, allowing a comprehensive evaluation of the renal condition. Second, given the small number of trials included in each analysis, we failed to assess the publication bias and small study effects with funnel plots. Third, it would have been interesting to know if PTX treatment in subgroups such as the elderly and women would also be favourable compared with control. However, we failed to make a subgroup analysis because of lacking data. Fourth, some included studies were single-blinded, single-centre designs, so the possibility of bias cannot be ruled out. However, all studies used objective indicators (eg, Scr) to evaluate CIN. Nevertheless, a prospective multicentre, double-blind, placebo-controlled study would make the conclusions more convincing.
Current evidence barely strong enough to support the renoprotection of PTX to CIN. If we assume that the CIN incidence in PTX treated group is 8% and 11% in control group, with a noninferiority limit of 1.5% with power of at least 80% and one-side type 1 error rate of 2.5%. More than 1000 participants are needed. More trials with larger sample sizes are needed to evaluate the role of PTX in CIN prevention.
Conclusion
Perioperative administration of PTX to patients undergoing angioplasty did not significantly reduce the development of CIN but showed some weak tendency of a lower Scr increase. Based on the available trials, the evidence does not support the administration of PTX for the prevention of CIN. More trials with larger sample sizes are needed to evaluate the role of PTX in CIN prevention.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design: DL. Administrative support: YY and WZ. Provision of study materials or patients: LW and DL. Collection and assembly of data: LW and DL. Data analysis and interpretation: LW and DL. Manuscript writing: all authors. Final approval of manuscript: all authors.
Funding This study was supported by the National Natural Science Foundation of China (2017YFC1308102).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.