Article Text

Abstract
Background Patient engagement in safety has shown positive effects in preventing or reducing adverse events and potential safety risks. Capturing and utilising patient-reported safety incident data can be used for service learning and improvement.
Objective The aim of this study was to characterise the nature of patient-reported safety incidents in primary care.
Design Secondary analysis of two cross sectional studies.
Participants Adult patients from Australian and English primary care settings.
Measures Patients’ self-reported experiences of safety incidents were captured using the validated Primary Care Patient Measure of Safety questionnaire. Qualitative responses to survey items were analysed and categorised using the Primary Care Patient Safety Classification System. The frequency and type of safety incidents, contributory factors, and patient and system level outcomes are presented.
Results A total of 1329 patients (n=490, England; n=839, Australia) completed the questionnaire. Overall, 5.3% (n=69) of patients reported a safety incident over the preceding 12 months. The most common incident types were administration incidents (n=27, 31%) (mainly delays in accessing a physician) and incidents involving diagnosis and assessment (n=16, 18.4%). Organisation of care accounted for 27.6% (n=29) of the contributory factors identified in the safety incidents. Staff factors (n=13, 12.4%) was the second most commonly reported contributory factor. Where an outcome could be determined, patient inconvenience (n=24, 28.6%) and clinical harm (n=21, 25%) (psychological distress and unpleasant experience) were the most frequent.
Conclusions The nature and outcomes of patient-reported incidents differ markedly from those identified in studies of staff-reported incidents. The findings from this study emphasise the importance of capturing patient-reported safety incidents in the primary care setting. The patient perspective can complement existing sources of safety intelligence with the potential for service improvement.
- primary care
- health services administration & management
- health & safety
Data availability statement
Data are available on reasonable request to the authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This research addressed important gaps in knowledge about patient reporting of safety incidents in primary care.
Our study described and categorised patient-reported safety incidents in diverse settings of England and Australia.
The study used a validated tool to collect qualitative data about patient perceptions of safety incidents.
Categorisation of safety incidents was performed by an expert panel using a structured framework called the Primary Care Patient Safety Classification.
The study was limited by lack of detail in some patient incident reports.
Introduction
Involving patients in safety incident prevention and harm reduction activities has gained traction over the past decade. Patient engagement in safety has shown positive effects in preventing or reducing adverse events, and increasing perception and awareness of potential safety risks.1–8 Patients’ observations and concerns play a critical and fundamental role towards the planning and the delivery of healthcare, ensuring their safety.9–13 Patients can offer a different perspective to safety incidents and risks, and often identify different types of safety incidents and outcomes than staff.3 7 12 Capturing and utilising patient-reported safety incident data can be used for service learning and improvement. Indeed, innovative and unique change ideas and interventions for making the health systems safer for patients have been implemented successfully using patient-reported data.14 15
However, most of the evidence describing the nature of patient-reported safety incidents has originated from the hospital setting,16 with primary care considered an emerging research area.17–26
A small number of studies have described the frequency of patient-reported safety incidents or errors, and harm in primary care.27–34 There was great variability in terms of the studies methodologies, and definitions used for safety incidents, errors and harm. Studies evaluating frequency of safety incidents ranged between 7.6% and 45%.28 30 31 34 Studies examining the frequency of error or experience of adverse event ranged between 9% and 20%.27 29 32 33 One study has categorised the level of harm with 41.7% of patients reporting a lot or severe harm from diagnostic mistakes, and 45.7% experiencing a lot or severe harm from treatment mistakes.28 The level of harm in the remaining studies occurred in between 7% and 29% of cases.31 33
Some patient-reported contributing factors to safety incidents have also been published including communication, the patient-provider relationship, access to care, care organisation, teamwork, information flow, continuity of care and patient-related factors (eg, medication non-adherence).27 29 31 35–40
We aimed to contribute to the developing evidence base by characterising the nature of patient-reported safety incidents in primary care. Secondary analysis of data collected from two studies investigating contributory factors to safety incidents in Australian and English primary care settings15 41 42 are reported in this paper.
Methods
The sampling and data collection strategies for the two studies investigating patient safety in primary care were similar, and used the same anonymous and validated questionnaire developed by researchers ALH and SJG41 in two locations. A detailed summary of the methods for study 1 and 2 have previously been described elsewhere15 41 42 and are briefly described below.
Study 1: validation study of the primary care patient measure of safety tool
Sampling frame
Nine primary care practices from within the Greater Manchester area agreed to participate in a study to determine the validity and reliability of the Primary Care Patient Measure of Safety (PC PMOS)41 questionnaire between April and September 2016. Practices were recruited using purposive and snowball sampling with the intention of ensuring a diverse range of participants with respect to practice size, practice location and deprivation levels. Online supplemental appendix 1 contains practice characteristic information.
Supplemental material
Data collection
Adult patients were provided the PC PMOS questionnaire by practice administration staff or by direct approach from members of the research team when presenting for their appointment. Participation was voluntary. Patients who agreed to participate returned the questionnaire before or after the consultation or by post. Recruitment was considered achieved when a minimum of 50 patients from each of the nine respective general practices returned the questionnaire.
Study 2: feasibility study of an intervention using patient feedback for safety improvement in primary care
Sampling frame
Six primary care practices from the south-west region of Victoria, Australia participated in a study investigating the feasibility of a patient feedback for safety improvement intervention during 2018–2019.15 A mix of small and large practices were purposively recruited into the study. The practices were relatively homogeneous in terms of population characteristics.43 Online supplemental appendix 2 contains practice characteristic information.
Supplemental material
Data collection
Every adult (over 18 years) presenting for their appointment was invited by the practice receptionist to complete the PC PMOS over a 3-week period. Patients returned their surveys via a secure survey return box in the practice waiting room. Patient consent was implied by the completion and return of the PC PMOS questionnaire. A plain language statement acted as the coversheet for the PC PMOS questionnaire.
Questionnaire
Patient-reported safety incidents were collected using the PC PMOS tool.41 The PC PMOS is a 28-item survey covering nine latent conditions in the primary care environment influencing safety incidents, such as access to care, communication, information flow, organisation care and planning and task performance. Basic demographic data on patient age, gender and number of visits to the general practice in the previous 12 months were also collected.
The PC PMOS contains six free-text questions for patients to report any safety incidents, problems or harms they had experienced in primary care. These questions were adapted from the Patient Incident Reporting Tool (PIRT) developed for research concerning patient involvement in safety in the hospital setting.44–46 The questions were: (1) Have you experienced something that you thought was a safety concern or issue in the last 12 months at this practice? (yes or no); (2) If yes, please tell us what happened in as much detail as you can? (free text); (3) Why do you feel this was a ‘safety concern’ for you? (free text); (4) What do you think could be done to stop this from happening again to you or other patients, in the future? (free text); (5) Do you think it would have been possible to have stopped your experience from happening? (Five point Likert scale with response options: ‘definitely yes’, ‘probably yes’, ‘probably not’, ‘definitely not’ and ‘don’t know’); and (6) On a scale of 1 to 10 how serious do you think your ‘safety concern’ was? (score of 1 being ‘not serious at all’ and 10 being ‘extremely serious’). Questions 1 to 4 and 6 on the PIRT were self-derived using an expert panel consisting of patients, clinicians, and researchers who developed questions that were deemed meaningful, relevant and patient-friendly.45 Question 5 is a standardised risk preventability question used in previous studies investigating safety incidents.47 48 There was an ‘additional comments’ question with a free-text response at the end of the questionnaire which could also capture self-reported safety incidents (online supplemental appendix 3).
Supplemental material
Data analysis
Data from study 1 and 2 were extracted verbatim from the PC PMOS questionnaires to a secure encoded Microsoft Excel database. Data were then cleaned and categorised by the authors (ALH and SJG) using the Primary Care Patient Safety Classification (PISA) System.49 The PISA System was empirically developed using patient safety incident reports maintained by the National Health Service (NHS) in England and Wales, namely the National Reporting and Learning System.
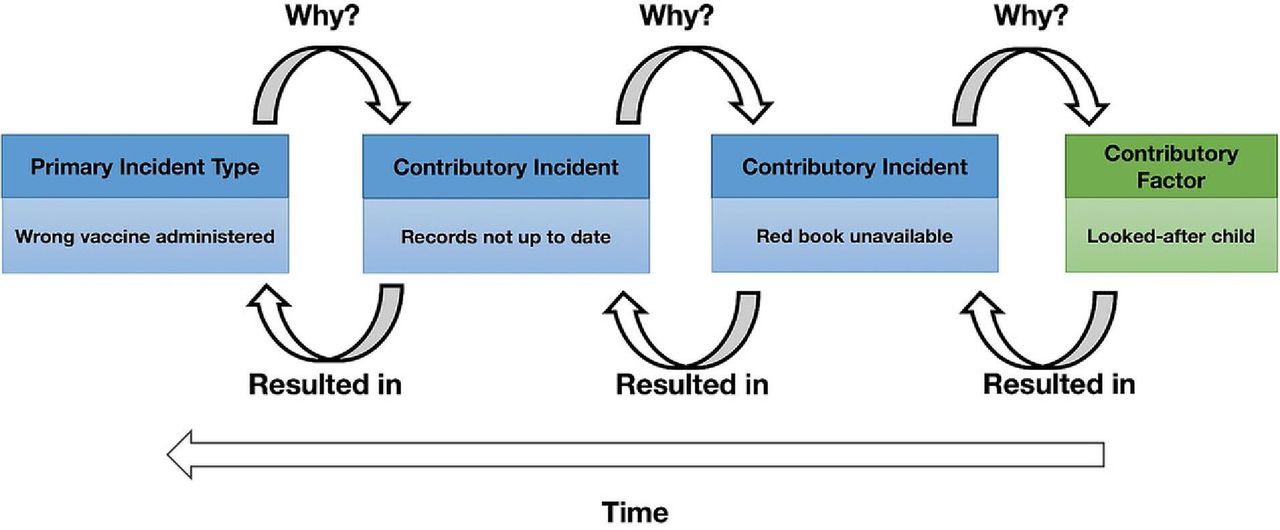
Each report underwent data coding using multi-axial frameworks to describe incident types (primary and contributory), potential contributory factors, incident outcomes and harm severity.49 50 Primary incidents included those proximal (chronologically) to the patient outcome, whereas contributory incidents included those that contributed to the occurrence of another incident. Contributory factors to a safety incident are defined as ‘issues that did not directly cause, but contributed to, the occurrence of an incident’.49 Multiple codes for incident type, contributory factor and incident outcome were applied to each report where necessary. This process was both deductive and inductive. Codes from the framework were used where appropriate and inductive codes were generated when there was no code available in the framework. The codes were applied systematically and chronologically according to recursive incident analysis rules developed by the Australian Patient Safety Foundation.51 This permitted modelling of the steps preceding and leading to primary incidents (eg, contributory incidents and factors, which, in turn, resulted in patient outcomes). Figure 1 illustrates how the recursive model for incident analysis works in practice.

{kind=link}
Example of codes from the Primary Care Patient Safety (PISA) Classification System using the recursive model for incident analysis. Reproduced with permission from the authors. Originally published by Carson-Stevens et al.70
An international expert panel was devised to review the patient-reported safety incident data and help form consensus on the final incident, contributory factors and outcome category codes. The multidisciplinary panel consisting of patient safety academic clinicians (n=4) and patient representatives (n=2) were recruited using the study team’s known networks in the patient safety in primary care field. Expert panel members were asked to objectively review the codes and provide a response; ‘agree’, ‘disagree’ or ‘unsure’. A justification and an alternative code was suggested by the expert when ‘disagree’ or ‘unsure’ options were selected.
When the patient-reported data did not correspond with the PISA System codes, specific self-derived codes were developed by authors ALH and SJG and the expert panel members. When there was not enough information contained in the patient incident report to accurately classify an incident, contributory factor, or outcome, a specific code was used (eg, unknown, insufficient detail, unclear).
Once coding was completed by the expert panel, two authors (ALH and SJG) reviewed the codes assigned to each patient-reported safety incident. Interrater reliability was assessed by calculating kappa scores for ALH and SJG and a third coder. Kappa scores indicated substantial agreement for the incident type, contributory factor and outcome codes (k=0.867, k=0.828, and k=0.965, respectively).52
The final codes were determined by ALH and SJG using consensus of reviewer agreement, and their explanations and comments corresponding to particular patient-reported safety incidents.
Descriptive summaries were generated to describe the frequency of incident types, contributory factors and incident outcomes (type of harm). Quantitative data were analysed using IBM SPSS Statistics V.23.
Descriptive statistics for the preventability and seriousness of the safety incident were generated. Patients self-reported data for the preventability and seriousness of the safety incident questions. Preventability categories were collapsed into ‘preventable’ and ‘not preventable’ categories.47 48 The continuous seriousness of the incident scale was classified into three categories ‘not serious at all’ (scores 1–3), ‘moderately serious’ (scored 4–7) and ‘extremely serious’ (8-10). A serious and preventable variable was created which included incidents that were classified as ‘preventable’ and ‘extremely serious’.53
Patient-related factors associated with reporting a safety incident were explored. P values are based on χ2 test for the categorical variable (gender), and independent sample t tests for the continuous variables (age, frequency of visits, mean PC PMOS score).
The frequency of safety incidents was calculated using the number of incident reports provided from the total sample of questionnaires returned.
Patient and public involvement
Two patient representatives formed part of the expert panel who reviewed the patient-reported safety incident data and helped form consensus on the final incident, contributory factors and outcome category codes.
Results
A total of n=1329 patients completed the PC PMOS questionnaire in both Study 1 and 2 (n=490 Study 1, n=839 Study 2). From study 1 and 2, there were a total of n=69 patient-reported safety incidents (n=41 Study 1, n=28 Study 2). 5.3% of patients reported a safety incident over the preceding 12 months. Patient demographic characteristics are provided in table 1.
Patient demographic characteristics
Forty-one safety incidents were revealed by question 1: ‘Have you experienced something that you thought was a safety concern or issue in the last 12 months at this practice?’, and 28 incidents were described in ‘Other Comments’ section of the questionnaire.
The patient-reported safety incidents were classified across eight categories (table 2). Nearly one-third (n=27) of the reports related to administration incidents, of which the majority concerned delays in patients accessing a physician (n=21, 24.1%). The remaining six incidents (6.9%) concerned errors in communication of information. Availability of appointments and long delays to see preferred physician were commonly reported. In some cases, patients reported delays in accessing care by up to 3 weeks and often presented to the clinic without an appointment for urgent care:
Unable to get appointment after referral from hospital as a matter of urgency. Had to stand outside at 8 AM to make an appointment. (Study 1)
Frequency and proportion of safety incidents by category
The second most commonly reported incident type was diagnosis and assessment (n=16, 18.4%). Errors in the process of assessing a patient were often reported (n=6, 6.9%). Patients described incidents where they believed physicians had not taken their health concern seriously or had not taken the time to adequately assess their condition.
The contributory factors to the patient-reported safety incidents were classified across seven categories (table 3). Organisation of care accounted for 27.6% (n=29) of the contributory factors identified in the safety incidents. Continuity of care and staff behaviour were most commonly described in this category. Problems of continuity of care within primary care and between different settings were reported:
In [hospital] for major operation, on seeing my doctor [GP] when I came out no information was available to him. (The GP) was not aware which medication was prescribed. (Study 1)
Frequency and proportion of contributory factors to the safety incidents by category
Staff behaviour related to inappropriate conduct or performance, mainly concerning patient communication and interaction:
A lot of doctors tend to run late, yet if a patient is a couple of minutes late, we have had an instance when we were nearly turned away and told we could not be checked in to see the doctor as we were 2 minutes late. After some discussion and explaining why we were late they allowed us in (child needed to go to the toilet as we were walking out the door at home). (Study 2)
Moreover, staff factors was the second most commonly reported contributory factor to safety incidents. Inadequate skill set/knowledge was identified in n=9 (8.6%) of patient reports and was mainly associated with diagnosis and assessments of patients and junior/trainee physicians:
I came with a swollen leg because I had a DVT before. I considered that it could be another DVT. I was assured hundred percent it wasn't a DVT. A couple of days after I saw another doctor who sent me straight to hospital where confirmed it was a DVT. The doctor concerned was wrong in her diagnosis. Locum doctors should have more training with long-term patients and consider illnesses that might need treating at hospital. (Study 1)
There were three self-derived contributory factor categories developed during analysis: communication (definition: effectiveness of the exchange and sharing of information between primary-care staff and patients), external policy environment (definition: national primary care system, structures and policies that impact on the delivery of care and resources available) and physical environment (definition: features of the physical environment that help or hinder safe practice).35 Staff listening to the patient and showing empathy were key contributory factors within the communication category, and problems encountered with the UK’s NHS same day appointment policy for study 1 patients (n=11, 10.5%) was a prominent theme in the external policy environment category.
The types of outcomes from the patient-reported safety incidents were classified across four categories (table 4). There was no reported patient outcome, or it was difficult to determine a clear patient outcome, for the majority of the incidents (n=38, 45.2%). Inconvenience to patients was the second most common outcome (n=24, 28.6%). This predominantly concerned delays in management or time spent on attempting to access care. Patient clinical harm was the third most common outcome (n=21, 25%). Psychological and emotional distress (n=8, 9.5%), and unpleasant experiences (n=4, 4.8%) were frequently reported outcomes:
When I was in desperate need of help advice/support I rang distraught, and nobody helped me. I was just transferred between staff (not Drs). I should have been referred to [telephone counselling service] or a mental health option. My usual Dr was not available. The staff would not listen to my requests to see anybody. Instead shuffled me around listened but missed any opportunity to help me. This was not a normal issue/occurrence for me. I WAS DISTRAUGHT! I NEEDED HELP. My mental health was not addressed. My friend was worried for me/my husband was worried for me. But I had to wait a week to see my Dr who cared for me & referred me to a mental health specialist immediately. I have dealt with this clinic for 30 years. I could have hurt myself… They seriously let me down…. (Study 2)
Frequency and proportion of the safety incidents outcome by category
Preventability and seriousness of patient-reported safety incidents
Of those patients that reported a safety incident in question 1, n=27 patients believed their safety incident could have been prevented (71.1%) and half believed their safety incident to be extremely serious (n=20, 51.3%). There were 17 (42.5%) patients who believed their safety incident was both extremely serious and preventable.
Patient characteristics associated with reporting a safety incident
There were no differences in terms of age or gender between patients who reported a safety incident and those who didn’t, but patients who did report a safety incident were more likely to have visited the general practice more often (12 vs 7 visits, p=0.006), and had a significantly lower mean PC PMOS scores (indicating poorer safety) (3.8 vs 4.2, p<0.001).
Discussion
This study contributes to the growing research characterising the nature of patient-reported safety incidents in primary care. 5.3% of patients reported a safety incident over the preceding 12 months. The most frequent type of incident was administration incidents, most of which concerned delays in patients accessing a physician. The most common contributory factor to the safety incidents was organisation of care, predominantly challenges with continuity of care. There was no reported patient outcome, or it was difficult to determine a clear patient outcome for over one third of incidents, with inconvenience to patient being the second most common outcome.
The frequency of patient-reported safety incidents is lower compared with other primary care patient-reported studies,27–34 but similar to studies using record review or staff reported safety incidents.54 The number of safety incidents may be an underestimate of the true prevalence of safety incidents in primary care for several reasons. First, patient-reported safety incidents are different or rarely overlap with incidents reported through other mechanisms (eg, staff reporting or record review).46 Consequently, using a combination of patient, staff and record review methods may more accurately determine the frequency of safety incidents.55 Second, the data collection methods, including questionnaire wording and mode of collection, may have limited the number of patient responses. The questionnaire relied on patient recall from the previous 12 months which may be challenging for some patients. Additionally, patients may have experienced a safety incident without knowing it. The open-ended question asking patients to report ‘safety concerns or issues’ without direct prompts such as ‘medication error’ or ‘misdiagnosis’, as used in other research studies,28–31 33 may have been too broad to elicit explicit safety incident experiences. Furthermore, 40% (n=28) of the safety incidents were reported in the ‘other comments’ section of the questionnaire. This may be attributed to patient’s different understanding and conceptualisation of patient safety in primary care when compared with secondary care.36 Third, although the questionnaire is anonymous, patients may still feel reluctant to judge or pass on negative comments about their healthcare providers. Lastly, the survey implemented in this study was self-completed without external facilitation from researchers or primary care staff. Survey facilitation has been shown to increase the frequency of incident reporting.46
The types of safety incidents that patients reported in this study were different to incidents that have been reported by staff or identified during record review studies.49 54–56 These large epidemiological studies and systematic reviews have classified communication, diagnosis and assessment, and medication errors as common incident types in primary care. Conversely, errors in administration, mainly access to care, was the most frequent patient-reported incident. While administration errors may be perceived as ‘soft issues’,57 these incidents are highly relevant to the patient care journey and may be considered as precursors to more serious safety incidents.
The types of contributory factors from the safety incidents were similar to what has been previously described in the literature.27 29 31 35–40 Additionally, there were several contributory factors reported by patients that did not correspond to any available codes in the PISA system. These findings indicate that patients have a unique perspective on patient safety which could be utilised to develop a patient inclusive taxonomy for use in primary care. Such a taxonomy may further facilitate the identification of important learning and preventative action across an extensive range of incidents in primary care.50
The data concerning the outcomes from the safety incidents in many patient reports was lacking or unclear. Many safety incidents to do not result in patient harm,13 which may explain the low frequency of outcomes reported. When there was an outcome reported the most common was inconvenience to the patient and psychological and emotional distress. Previous research has shown that patients emphasise emotional harm more so than physical harm when describing the outcome of a patient safety incident.37 58 Indeed being treated with dignity and respect is the foremost reported safety priority for patients in the literature,35 37 58 59 consequently, a high frequency of emotional harm was not unexpected. Until recently, only physical health outcomes were used to classify harm severity across many PISA systems.60 61 The newly developed Primary Care Harm Severity Classification System by Cooper et al encompasses mild, moderate and severe psychological harm categories as well as physical harm outcomes.50 This definition will assist professionals, organisations and policy-makers to understand the true nature of healthcare-associated harm.
The patient-reported preventability and seriousness of the safety incidents were generally higher than what is described in the literature. Most studies were conducted in hospital settings and employed clinician/academic reviewers rather than patient self-reported data.14 46 48 62 63 The patient perspective of the preventability and seriousness of safety incidents is an additional safety intelligence measure that can be used by researchers, health professionals and policy-makers to further understand and support patients who have experienced a safety incident in primary care.
Frequent attenders and those with lower overall scores of safety on the PC PMOS (indicating poor safety experiences) were significantly more likely to report a safety incident. These findings should be interpreted with caution due to the small sample size. Nonetheless the results are corroborated by studies which have identified a range of patient characteristics associated with experiencing safety incidents in primary care.64 65 Conversely, patient gender and age were not associated with experience of a safety incident. This finding is unable to be explained when compared with research showing that gender and age have been associated with increased likelihood of experiencing a safety incident.30 64–69 Identifying patients at risk of safety incidents is important for monitoring, assessing and error prevention efforts.13
It is worth noting that the survey used to collect the patient-reported safety incident data was not part of a formal incident reporting system. The survey was employed as a part of a suite of tools that are essential for primary care systems to learn from unsafe care and implement safety improvements. The impact of the patient-reported safety incidents from this study has been demonstrated through implementation of an innovative patient feedback on safety intervention. Primary care teams reviewed the patient-reported safety data and developed specific safety interventions which resulted in significantly improved patient safety scores.15
The cross-sectional study design may have been a limitation in this study. Longitudinal studies which track patients over time or qualitative studies may have elicited more in depth and rich data to accurately classify the incident type, contributory factor, level of harm and harm type for each safety incident. Due to the lack of data or detail in some of the patient reports we were not able to determine the level of harm associated with each outcome.50 Likewise, due to the small number of incidents further analysis investigating the association between type of incident and outcome was unable to be undertaken. As the PC PMOS was an anonymous survey, patients may have been able to report more than one safety incident if they visited their practice more than once during the recruitment period. However, the safety incidents reported by patients were perceived by the reviewer panel as separate and unique incidents. Furthermore, demographic information about patients who completed the PC PMOS compared with those who declined to participate was only available for study 2,15 and limited information was collected in study 1.41 As a result of this incomplete data, it is it is difficult to determine any differences between patients who chose to participate in the study compared with those who declined in terms of likelihood of experiencing and reporting a safety incident. Small differences between the two study settings (England and Australia) were observed for some contributory factors relating to the external policy context such as cost of appointment and same day appointment policies. Given that these contributory factors only made up 15% of the total factors reported, the authors believe that the majority of incident types and subsequent contributory factors were more generic and reflected a universal experience of patient safety in primary care across the two settings. These findings contribute to the growing evidence base examining the nature of patient-reported incidents in primary care.
Conclusion
The patient perspective can complement existing sources of information and provides another dimension to the patient safety in primary care research field. Simple patient surveys, like the one employed in this study, can generate useful feedback for practice teams to engage in error prevention and learning activities. Changes to questionnaire wording and provision of patient safety incident type examples may increase the quantity and quality of patient reports and should be assessed in future research.
Data availability statement
Data are available on reasonable request to the authors.
Ethics statements
Ethics approval
Ethical approval for study 1 was granted from NHS Health Research Authority (HRA) approval (project no. 16/SS/0096). Ethics approval for study 2 was granted from Deakin University Human Ethics Advisory Group, Faculty of Health (HEAG-H 175_2017).
Acknowledgments
The authors acknowledge the practice staff and patients who participated in this study. The authors would also like to acknowledge the administrative support from Gillian Beard and Liz Jackway at Deakin Rural Health, Rahul Alam at the National Institute for Health Research (NIHR) Greater Manchester Primary Care Patient Safety Translational Research Centre and Stuart Hellard at Cardiff University. The authors would also like to thank the two patient representatives who assisted with coding the patient safety incident reports.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @andreahernan11
Correction notice This article has been corrected since it was published. The word ‘primary care’ has been removed from the name of the institution mentioned in affiliation 2 and the funding statement.
Contributors ALH conceived and designed the study. SJG contributed to the study design. AC-S, MM, PL and JH were members of the expert panel that helped form consensus on the coding. ALH and SJG were responsible for the data analysis and manuscript preparation. ALH created the first draft of the manuscript and was responsible for its revisions. VV conducted the statistical analysis. AC-S, MM, PL, JH and VV contributed to specific sections of the manuscript. All authors read and approved the final version of the manuscript.
Funding Study 1 was supported by the Western Alliance (Grant number: WA-733721). Study 2 was funded by the National Institute for Health Research (NIHR) Greater Manchester Patient Safety Translational Research Centre (Grant number: gmpstrc-2012-1).
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.