Article Text

Abstract
Introduction Despite the use of quantitative neuromuscular monitoring together with the administration of reversal drugs (neostigmine or sugammadex), the incidence of residual neuromuscular blockade defined as a train-of-four ratio (TOFr) <0.9 remains high. Even TOFr >0.9 cannot ensure adequate recovery of neuromuscular function when T1 height is not recovered completely. Thus, a mathematical correction of TOFr needs to be applied because the return of a normal TOFr can precede the return of a normal T1 twitch height. On the other hand, different muscles have different sensitivities to neuromuscular blockade agents; thus, complete recovery of one specific muscle group does not represent complete recovery of all other muscles. Therefore, our study aims to assess the muscle strength recovery of respiratory-related muscle groups by ultrasound and evaluate global strength using handgrip dynamometry in the early postoperative period when TOFr=0.9 and corrected TOFr (cTOFr)=0.9 with comparison of neostigmine versus sugammadex as reversal drugs.
Methods and analysis This study will be a prospective, single-blinded, randomised controlled trial involving 60 patients with American Society of Anesthesiologists physical status I–II and aged between 18 and 65 years, who will undergo microlaryngeal surgery. We will assess geniohyoid muscle, parasternal intercostal muscle, diaphragm, abdominal wall muscle and handgrip strength at four time points: before anaesthesia, TOFr=0.9, cTOFr=0.9 and 30 min after admission to the post anaesthesia care unit. Our primary objective will be to compare the effects of neostigmine and sugammadex on the recovery of muscle strength of different muscle groups in the early postoperative period when TOFr=0.9 and cTOFr=0.9. The secondary objective will be to observe the difference of muscle strength between the time points of TOFr=0.9 and cTOFr=0.9 to find out the clinical significance of cTOFr >0.9.
Ethics and dissemination The protocol was reviewed and approved by the Ethics Committee of The First Affiliated Hospital, Sun Yat-sen University. The findings will be disseminated to the public through peer-reviewed scientific journals.
Trial registration number ChiCTR2000033832.
- ultrasonography
- adult anaesthesia
- clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study is the first randomised controlled trial to assess the effect of such low level of residual paralysis (train-of-four ratio (TOFr) >0.9) on muscle strength other than diaphragm.
This is the first study to apply a corrected TOFr (defined as T4/T1 reference) to detect residual paralysis.
The limitation of the present study is that we only focus on exploring the effect of residual neuromuscular blockade on different groups of muscle strength, so we do not try to follow-up on the further clinically relevant outcomes.
Further research is needed to focus on patients with higher risk factors for the development of postoperative pulmonary complications including the elderly patients undergoing surgery longer than 3 hours in multiple centres.
Introduction
Background
Complete recovery of neuromuscular function, defined as the train-of-four ratio (TOFr) greater than or equal to 0.9, should be obtained in the early postoperative period to enhance patient safety and improve the quality of recovery. However, although the RECITE (Residual Curarisation and its Incidence at Tracheal Extubation) studies conducted by several countries had reported the similar unacceptably high incidence (57.8%–64.7%) of residual neuromuscular blockade (rNMB) at extubation, these studies failed to find out specific causality between rNMB and respiratory complications (including upper airway obstruction requiring intervention, and hypoxia) until discharge from the post anaesthesia care unit (PACU).1–3 What’s more, as the incidence of critical respiratory events related to the administration of neuromuscular blocking agents (NMBAs) is as low as 0.8%,4 the awareness of clinical consequences of rNMB remains limited. Emerging evidence suggests rNMB may impair clinical recovery beyond the recovery room. Recently, a large cohort study showed that higher doses of NMBAs given during abdominal surgery was associated with an increased risk of 30-day readmission.5 Another multicentre study funded by the European Society of Anaesthesiology showed that the use of NMBAs was associated with an increased risk of postoperative pulmonary complications (PPCs) from the end of surgery up to postoperative day 28.6 These studies provide evidence that the effects of rNMB may last beyond the time when the patient leaves the operating room and extend to clinically related downstream postoperative complications such as pneumonia and respiratory failure. Thus, it is essential to manage neuromuscular block rationally and have a sound strategy to prevent and detect rNMB.
Acceleromyography (AMG) is the quantitative monitoring technique that is most widely used in clinical practice. Murphy et al reported that AMG monitoring reduced the incidence of rNMB in the PACU.7 However, in this study, symptoms of muscle weakness still existed even when TOFr had been greater than 0.9. This may be explained by a different recovery pattern existing in some patients that the recovery of TOFr to 0.9 is faster than the recovery of first twitch (T1) height when the fourth twitch (T4) and T1 have similar but rather low amplitudes (figure 1). Typical spontaneous recovery from non-depolarising NMBAs is that the T1 normally recovers to baseline first, while at this point, TOFr may still be depressed (figure 2). As the TOFr reflects the effects of the NMBAs at the presynaptic membrane of the neuromuscular junction, the T1 reflects the events at the postjunctional membrane and is directly related to the force generated.8 Thus, the TOFr of 0.9, by itself, may not ensure adequate neuromuscular recovery if the T1 recovery is not back to baseline. This limitation of TOFr suggests that a mathematical correction needs to be applied. Moreover, a recent exploratory analysis of the POPULAR data by Blobner et al concluded that PPCs were reduced if tracheal extubation were performed with TOFr >0.95 compared with TOFr >0.9, which demonstrated the limitation of TOFr=0.90.9 Therefore, in this study, we raise the concept of ‘corrected’ TOFr (cTOFr=T4/T1 reference), defined as the ratio of the present T4 to last T1 during the calibration process (T1 reference).
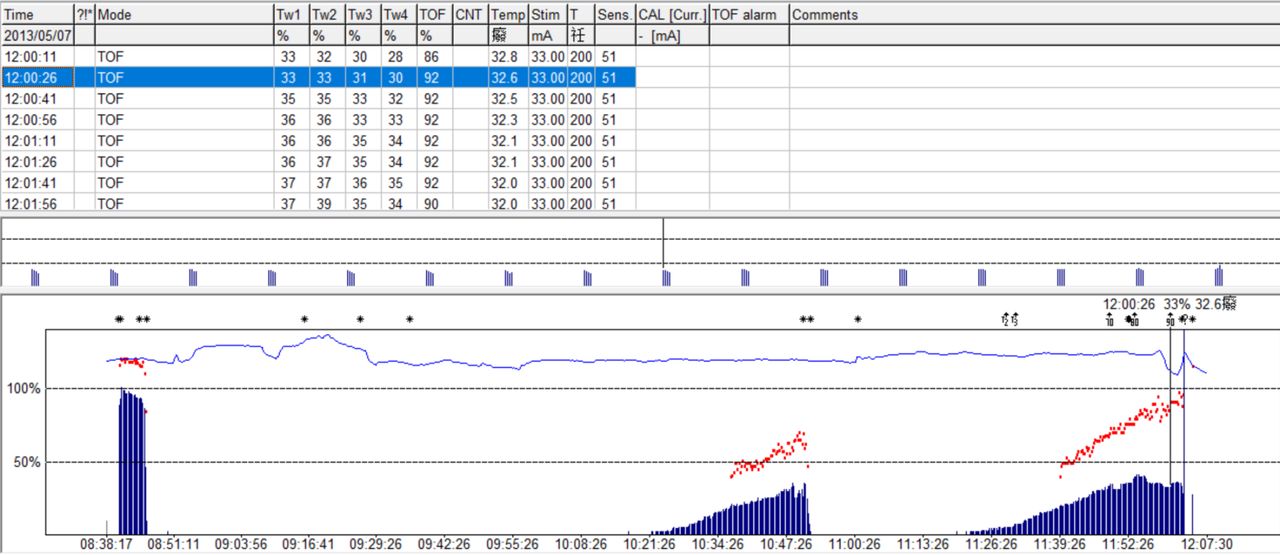
Reversal with neostigmine after cisatracurium-induced non-depolarising neuromuscular blockade. When the TOFr reaches a value of 92% (red dotted line), the T1 twitch height reaches only 33% and T4 twitch height reaches 30% of control. TOFr, train-of-four ratio.

Reversal with neostigmine after cisatracurium-induced non-depolarising neuromuscular blockade. When the T1 twitch height reaches 91% of control, the TOFr still be depressed as 73% (red dotted line). TOFr, train-of-four ratio.
Furthermore, after the absence of any twitch depression detectable by neuromuscular monitoring, approximately 75% of postsynaptic acetylcholine receptors are still occupied by non-depolarising NMBAs and the magnitude of NMBAs effects at the neuromuscular junction cannot be quantified by current methods of neuromuscular monitoring. Therefore, the impact of remaining low-level block at TOFr >0.9 or cTOFr >0.9 on muscle strength recovery is still unknown. The use of ultrasound to evaluate the respiratory muscle pump function is a relatively new and attractive method to assess multiple muscle groups.
The diaphragm is the principle inspiratory muscle that contributes to more than 60% of the total breathing effort in the supine position, making diaphragmatic dysfunction a major factor in the aetiology of PPCs.10 Therefore, studying diaphragmatic function in the perioperative context is of paramount importance.
‘Rather as the heart does not comprise only a left ventricle, but also a right one, the respiratory muscle pump is much more than just the diaphragm’.11 The expiratory muscles are the ‘neglected component’ of the respiratory muscle pump, including those of the abdominal wall (transversus abdominis muscle, internal oblique muscle, external oblique muscle, and rectus abdominis muscle) and some of the rib cage ones (eg, the internal intercostal muscles and the triangularis sterni muscle). Activation of the abdominal wall muscles increases abdominal pressure in the expiratory phase, enhancing inspiratory muscle capacity via at least two mechanisms. First, increased abdominal pressure moves the diaphragm at end-expiration to a more cranial position, which results in a more optimal length for tension generation; second, when the end-expiratory lung volume falls below functional residual capacity, elastic energy is stored in the respiratory system. This stored energy facilitates the next inspiration (ie, allows more rapid and significant development of negative pleural pressure). Another fundamental role of the expiratory muscles is to develop effective cough pressure to facilitate airway clearance.11 Insufficient strength of the diaphragm and the abdominal wall muscles decreases a patient’s ability to cough and clear secretions, and increases alveolar collapse, possibly resulting in pneumonia.
Beyond the ability to cough, the swallowing function is also pivotal to avoid aspiration. The geniohyoid muscle (GM) is one of the suprahyoid muscles that move the hyoid bone anterosuperiorly during swallowing, contributing to the generation of negative pressure in the upper oesophageal sphincter which plays a role not only in suction that helps the downward movement of the food, but also in preventing aspiration.12 rNMB can evoke dysphagia and a decrease in maximum airflow during inspiration. These signs and symptoms can be observed even with a magnitude of muscle weakness insufficient to evoke respiratory symptoms, suggesting that upper airway muscles are more susceptible to neuromuscular blockade than the diaphragm.13 Evaluation of the strength of GM is thus useful for assessing the muscles of deglutition.
In addition to respiratory muscle function, peripheral muscle function also significantly impacts patients’ postoperative rehabilitation and may be critical for enhanced recovery after surgery.
A previous study showed that there was a strong correlation between handgrip strength and TOFr during recovery from general anaesthesia.14 However, currently, no clinical trials have systematically assessed the differences of the recovery of muscle strength measured by maximal voluntary contraction force with the comparison of neostigmine and sugammadex as reversal drugs.
Prevention of rNMB depends on judicious neuromuscular blockade management, monitoring, and the use of reversal agents. Neostigmine, the most common acetylcholinesterase inhibitor, currently remains the mainstay of the practice of reversal of non-depolarizing NMBAs but is ineffective in reversing deep block. Sugammadex is a new selective relaxant-binding agent that can reverse any depth of block from non-depolarizing aminosteroid relaxants. Sugammadex has been proven to be associated with a lower rate of rNMB at the time of extubation and PACU admission, and also be associated with a 40% reduction in r NMB compared with neostigmine.15 Recently, a multicentre observational matched cohort study showed that sugammadex administration was associated with improvement in pulmonary outcomes compared with neostigmine.16 We presume that the potential mechanism of sugammadex reducing the incidence of PPCs is that sugammadex may be quicker and more efficient to enhance the recovery of muscle strength in the early postoperative period than neostigmine.
In the present study, we aim to design a randomised clinical trial to exert serial measurements of global and respiratory muscle strength in the early postoperative period using ultrasonography, to compare the recovery of muscle strength of different muscle groups at the time of TOFr=0.9 and cTOFr=0.9 after reversal with neostigmine or sugammadex.
Methods and analysis
Study design
This study will be a prospective, single-blinded, randomised controlled trial conducted at The First Affiliated Hospital, Sun Yat-sen University. The design of this study protocol has referred to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 guideline.17
Study population
Inclusion criteria
Age between 18 and 65 years old.
Patients scheduled for microlaryngeal vocal surgery.
American Society of Anesthesiologists physical status I–II.
Able to give informed consent.
Exclusion criteria
Significant kidney disease (stage 4 kidney disease or higher).
Significant liver disease (Child-Pugh B or C class).
Allergic to neostigmine or sugammadex.
History of a neuromuscular disorder.
History of chronic obstructive pulmonary disease.
Pregnancy or nursing women.
Refuse to participate.
Difficult airway (history or suspected of difficult mask ventilation).
Arrhythmic disease or taking anti-arrhythmic drugs.
Randomisation
The study will be a single-blinded, randomised controlled parallel-group trial. Eligible patients will be randomised in a 1:1 fashion to either the sugammadex (SUG) group or the neostigmine (NEO) group. Randomisation will be performed by a randomisation list created on www.randomization.com. The allocation sequence will be created before study commencement by a member of the clinical research department not involved in recruitment, coordination or data collection. Allocation will be concealed in sequentially numbered opaque envelopes. The attending anaesthesiologists will be blinded until they are ready to prepare and administer reversal drugs, typically when the operation is nearly completed. Researchers involved in recruitment, consent and outcomes assessment will be blinded to group allocation until study completion. Assessors will not be involved in patients’ care and have no access to anaesthesia records.
Interventions
On the day before surgery, patients will be trained to be familiar with swallowing, deep breathing, sniff breathing, coughing using abdominal muscle and how to use an electronic hand dynamometer during preoperative visit. Patients will also be informed that they need to cooperate to do these exercises both before and after the operation.
Prior to induction of anaesthesia, the baseline GM, parasternal internal intercostal muscle, diaphragm and the abdominal muscle will be evaluated by one physician skilled in ultrasonography using an ultrasound machine (Mindray ME7, Mindray Bio-medical Electronics Co Ltd, Shenzhen, China) with a C5-1s convex transducer and a linear transducer. Patients will be assessed in a semirecumbent position (sitting at a 45° angle with a bed goniometer). A marker (on the skin) of each muscle group will be left to record the point of the preanaesthesia scans and the postoperative scans will be performed in the marked point. Besides, an adjustable handheld dynamometer will be used to measure the baseline maximum handgrip strength. Each evaluation will be performed three times and the respective highest values will be used in the analysis.
Ultrasonography
GM ultrasound
A C5-1s convex transducer will be applied in alignment with the midline of the floor of the mouth and perpendicular to the lower chin surface of the patient (see figure 3). The transducer will be positioned at a height that enabled delineation of the hyoid bone while avoiding contact between the face of the probe and the thyroid cartilage. The hyoid bone and the mandible accompanying the acoustic shadow together with the adhering GM at rest will be delineated in the midsagittal plane in a single screen and a static image will be saved. Once the researcher initiates the recording of the video loop, the participant will be prompted to swallow their saliva as they usually would. The evaluation will be performed three times, and sonograms will be obtained as individual video segments to record each swallow. There is a time lapse of no less than 30 s between swallows. The maximum hyoid bone displacement will be recorded.18

Submental ultrasonographic evaluation and hyoid bone displacement on a model. (A) A vertical line is drawn from superior thyroid notch to mandible for probe placement. (B) Probe is placed at midsagittal plane of submental area. The mandible and the hyoid bone (C) at rest and (D) during swallowing. White arrow represents shadow behind the mandible; green arrow represents shadow behind the hyoid bone; asterisk represents geniohyoid muscle.
Parasternal intercostal muscle ultrasound
Parasternal intercostal muscle ultrasound will be performed with an L14-6Ns linear probe placed longitudinally in the second intercostal space approximately 2–3 cm lateral to the sternal edge. The thickness and inspiratory thickening fraction will be assessed when the patient is prompted to breathe deeply (figure 4). Video capture of at least three complete respiratory cycles will allow for maximal inspiratory and expiratory thickness measurements measured on the frozen image.19

Ultrasound of the right parasternal intercostal muscle on a model. (A) Probe is positioned in cranio-caudal direction at the second intercostal space approximately 2–3 cm lateral to the sternal edge. (B) Using B-mode the parasternal intercostal muscle is identified as a three-layered biconcave structure: two linear hyperechoic membranes, respectively, running from the anterior and posterior aspects of the adjoining ribs, and a medial portion with muscle echotexture. (C) Using M-mode, the thickness of the parasternal intercostal muscle will be measured on frozen images.
Diaphragm ultrasound
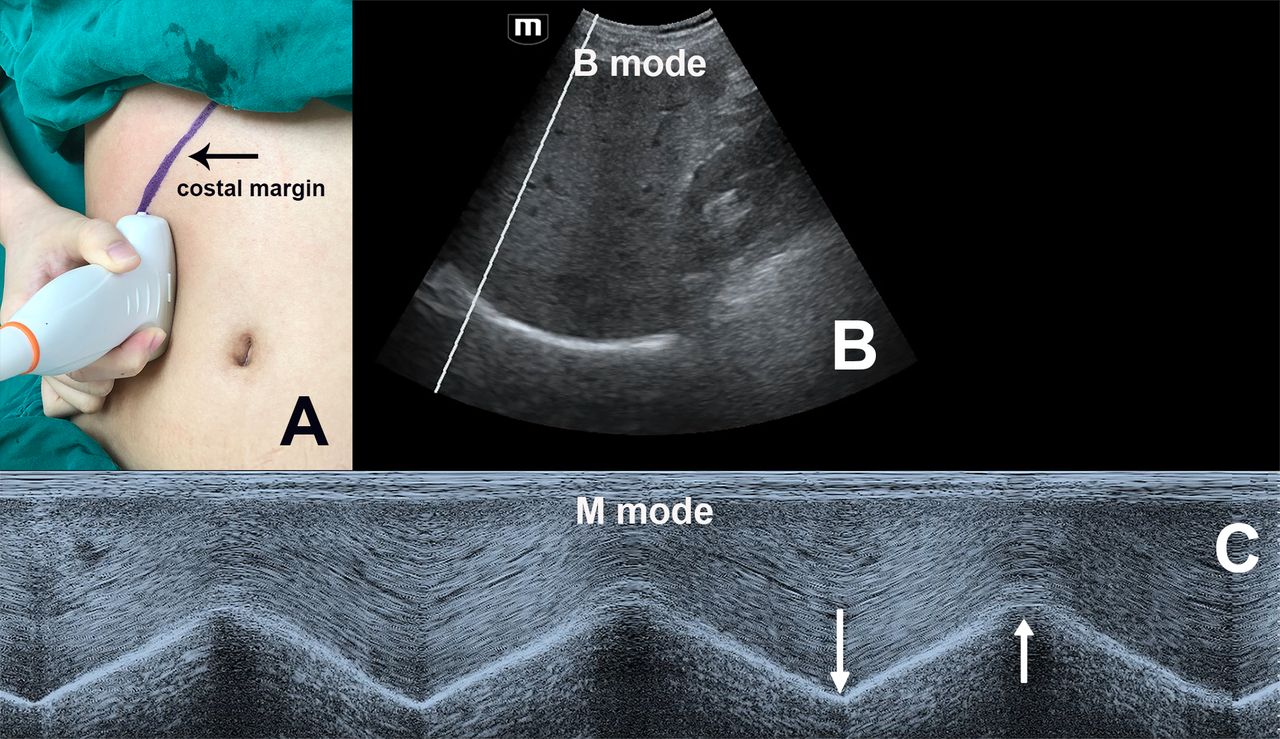
Diaphragmatic sonography is performed during maximum sniff breathing using a C5-1s convex transducer. The probe will be placed immediately below the right costal margin in the midclavicular line, directed medially, cephalad and dorsally so that the ultrasound beam reaches perpendicularly the posterior third of the corresponding hemidiaphragm. The B-mode will be initially used to identify the diaphragm as an echogenic line between the interface of the lung and liver.20 The amplitude of excursion of the hemidiaphragm will be measured on the vertical axis of the M-mode tracing from the baseline to the point of a maximum height of inspiration on the graph (figure 5). The sweep speed will be adjusted to 25 mm/s to obtain a minimum of three respiratory cycles within one image.21

Ultrasound of diaphragm on a model. (A) Probe position for diaphragmatic excursion measurements with C5-1s convex transducer. Black arrow indicates the costal margin. (B) B-mode diaphragm sonography. (C) M-mode diaphragm sonography. White arrows indicate the beginning (left) and the end (right) of the diaphragmatic contraction.
Abdominal muscle ultrasound
An L14-6Ns linear probe will be positioned on the anterior axillary line, midway between the inferior border of the rib cage and the iliac crest, perpendicular to the abdominal wall. The different expiratory muscles will be relatively easy to visualise as hypoechogenic layers enclosed by fascial sheaths (figure 6). Ultrasound measurements of abdominal muscle maximal thickening fraction during coughing correlated to expiratory force generation. The thickness of the abdominal muscle will be measured at rest and the maximum contraction when the patient is told to cough with maximum strength. Thickening fraction of the internal oblique muscle (TFIO) will be calculated by using the formula (TFIO = (end-coughing thickness − end-inspiratory thickness)/end-inspiratory thickness) ×100%).22
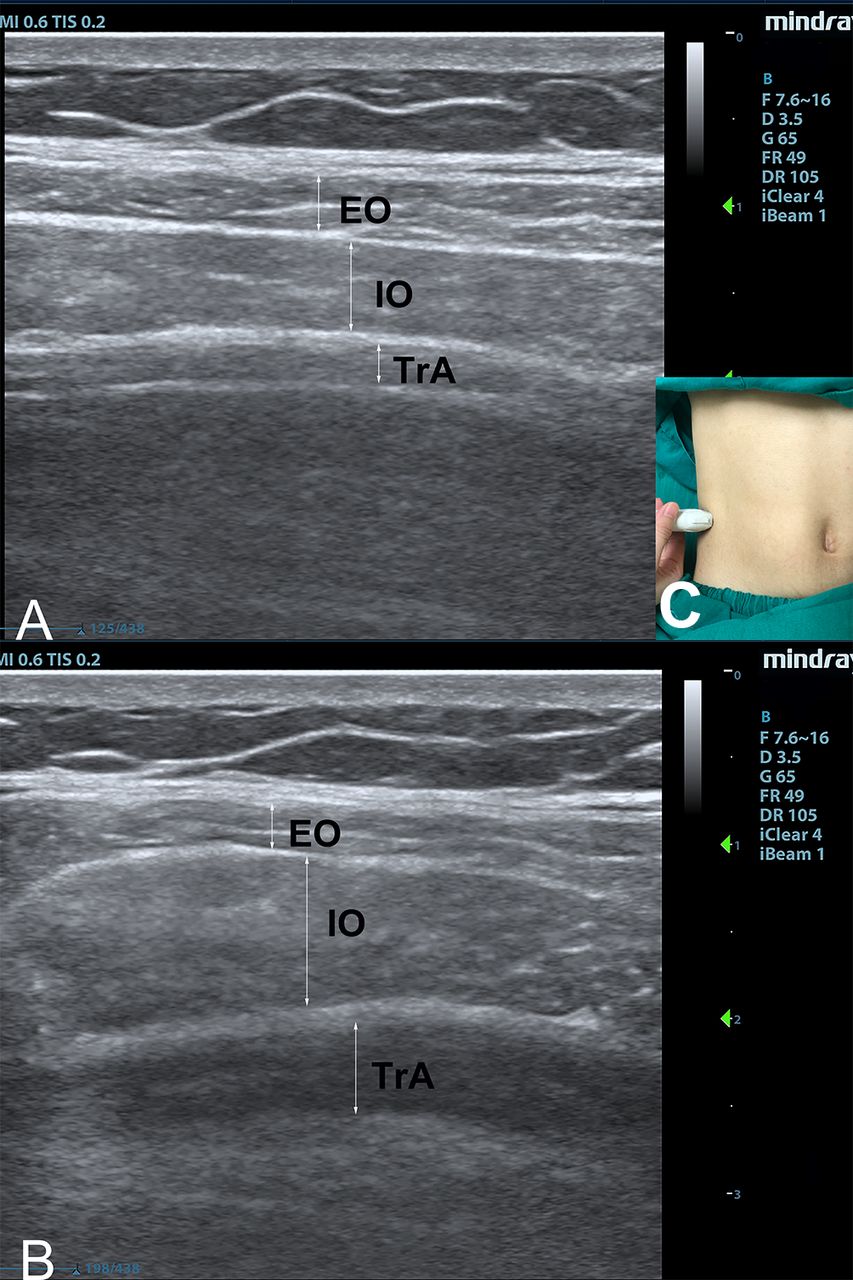
Ultrasound imaging of the lateral abdominal wall muscles on a model (A) taken during resting state, (B) taken during cough. (C) Probe is positioned perpendicular to the abdominal wall. Probe position for abdominal muscle sonography with L14-6Ns liner transducer. EO, external oblique; IO, internal oblique; TrA, transversus abdominis.
Handgrip measurements
The handgrip strength of the right hand will be measured using an electronic device (Electronic Hand Dynamometer EH101; Camry, China) three times. The patients will be instructed to squeeze the handle as hard as possible for 3 s, and the maximum contractile force will be recorded in kilograms.23
Anaesthetic management and neuromuscular monitoring
To standardise the anaesthetic technique, no premedication will be administered.
All patients will undergo neuromuscular monitoring using continuous AMG at the adductor pollicis muscle with TOF-Watch SX (Organon, Dublin, Ireland) throughout the entire study period. After skin cleansing, two surface electrodes will be positioned over the ulnar nerve at the wrist. A hand adapter that applied a constant preload to the thumb will be secured to the hand with tape. An acceleration transducer will be attached to the distal phalanx of the thumb via the hand adapter. The hand will be positioned on the transport cart to prevent movement of fingers except for the thumb during each assessment. Anaesthesia will be induced by propofol and remifentanil. After induction of anaesthesia but before NMBAs administration, TOF-Watch SX will be calibrated with the built-in calibration modus (CAL 2) after 5 s 50 Hz tetanic stimulation preceded by a repetitive TOF stimulation for 1 min. After calibration, a 3 min repetitive TOF stimulation will be required to ensure a stable response before the administration of the NMBAs.3 24 TOF stimulation will be applied at 15 s intervals until the patient is discharged from the PACU. Neuromuscular monitoring data will be collected using the TOF-Watch SX Monitoring Program, V.2.5.
After the TOF-Watch SX is set up, rocuronium 0.6 mg/kg will be administered within 5 s as a fast-running infusion. Tracheal intubation will be performed after the response signals to TOF are absent with a 6.0 mm cuffed endotracheal tube. End-tidal carbon dioxide concentration will be maintained at 35 to 45 mm Hg via controlled ventilation. To maintain neuromuscular block, rocuronium 0.15 mg/kg will be readministered when post-tetanic count (PTC) elicits more than three twitches. Maintenance of anaesthesia will be obtained with total intravenous anaesthesia. The plasma-targeted concentration of propofol will be titrated to keep the spectral edge frequency within 8–12 Hz from a Narcotrend device, and the infusion rate of remifentanil will be adjusted in response to systemic blood pressure or heart rate during anaesthesia maintenance. Dexamethasone 10 mg and palonosetron 0.25 mg will be applied to prevent postoperative nausea and vomiting. At the end of the surgery propofol will be stopped and remifentanil will be continued at the rate of 0.1 mcg/kg/min until extubation. As soon as the patient regains consciousness, the reversal drug will be administered according to the group they have been randomised. The doses will be determined according to the doses recommended in a review article: when PTC is more than or equal to 1, 4 mg/kg sugammadex will be administered; when TOF count is 1–3, or TOF count is 4 with fade present, or TOFr is between 0.1 and 0.4, 50 mcg/kg neostigmine or 2 mg/kg sugammadex will be administered; if TOF count is 4 without fade, or TOFr is between 0.4 and 0.9, 20 mcg/kg neostigmine or 2 mg/kg sugammadex will be administered25; if TOFr is more than 0.9, no reversal drug will be given and the patient will be excluded from the study. Extubation will be performed in the operation room when all the following criteria are met: (1) the patient is awake; (2) the patient can execute simple commands such as breath and open the mouth. Handgrip strength and the different muscle groups assessed by the ultrasound will be performed when TOFr reaches 0.9, the cTOFr reaches 0.9 and 30 min after PACU arrival. If TOFr and cTOFr recover simultaneously or recover one after another within 5 min, we consider them the same timepoint. We will also follow-up the adverse events in the PACU, such as nausea and vomiting, stomachache and respiratory complications. A flow chart of the inclusion process is shown in figure 7. Please see online supplemental material 1 and 2 for the study timeline and SPIRIT checklist, respectively.
Supplemental material
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Study flow diagram. PACU, post anaesthesia care unit; TOFr, train-of-four ratio.
Outcome measurements
Our primary outcome will be the ratio of TFIO at TOFr=0.9 to the TFIO at baseline. The secondary outcomes will include: (1) the ratio of the handgrip strength, hyoid bone displacement, parasternal intercostal muscle, diaphragm excursion at the time of TOFr=0.9, cTOFr=0.9 and 30 min after PACU admission to baseline, respectively; (2) the recovery time from TOFr=0.9 to TOFr=0.95 and to unity, respectively.
Database locking
Data will be collected by paper case report form (CRF). All the complete CRFs will be archived in a locker to which only clinicians involved in the study have access. After data recording, checks will be performed to search for internal inconsistencies, range errors or missing data. For each atypical, out-of-range or missing datum, a query will be sent to the researchers. After all the queries are solved, the principal researchers, data collectors, statistical analysts will complete the final definition of the analysis population. Then the database will be locked and used for statistical analysis.
Statistical analyses and sample size calculation
The sample size will be calculated according to the primary outcome, the ratio of TFIO at TOFr=0.9 to the TFIO at baseline. Based on our pilot study of neostigmine, the mean of the ratio of TFIO at TOFr=0.9 to the baseline was 46% and the SD was 33%. This trial is designed to achieve 90% power to detect 30% differences with a SD of 0.33 in the ratio of TFIO at TOFr=0.9 to baseline between the two groups with a two-sided α level of 0.05. A sample size of 27 participants will be needed for each group. Assuming that 10% of patients may be excluded from the analysis, a calculated sample size of 30 will be set per group.
Statistical analyses will be performed using IBM SPSS Statistics V.25. Normal distribution of data will be tested by the Shapiro-Wilk Normality Test. Data will be reported as mean±SD or median (IQR), as appropriate. Unpaired Student’s t-tests or Mann-Whitney U tests will be used to test the differences between the two groups for data with normal or not normal distribution, respectively. Pearson’s χ2 test or the Fisher’s exact test will be used to compare categorical data. The ratio of different muscle strength to the baseline between two groups will be analysed by Mann-Whitney rank-sum test. For all comparisons, a two-sided p value of <0.05 will be considered statistically significant.
Discussion
Impacts of rNMB may last beyond the time the patient leaves the operating room such as muscle weakness, upper airway obstruction and oxygen desaturation but may extend to clinically related downstream PPCs including pneumonia and respiratory failure.16 The residual effects of intraoperatively administered NMBAs may result in PPCs through different mechanisms: impaired contraction of ventilatory muscles with atelectasis formation, inability to cough and impaired swallowing, with the accumulation of airway secretions and aspiration of gastric contents.26 Thus detecting those impaired muscle function in the early postoperative period when TOFr has been more than 0.9 by bedside tools and minimising this vulnerable period is an important clinical issue.
Baumüller and colleagues reported that antagonising rocuronium at TOFr ≥0.9 with sugammadex 1.0 mg/kg did not improve patients motor function, and they, therefore, concluded the decrease in fine motor skills and maximal grip strength in the early postoperative period after spontaneous recovery to TOFr ≥0.9 was more likely to be related to the anaesthetic agents.27 In contrast, Pung-Fei’s volunteer study showed that grip strength did not decrease but slightly increased at the predicted effect site propofol concentration of 1.2 mcg/mL or less.28 In our pilot study, the effect-site propofol concentration when patients woke up was 1.0 mcg/mL or less, which could rule out the possible weakening effect of propofol on muscle strength. Even so, in the present study, we choose short-acting sedative (propofol) and analgesic agents (remifentanil) to minimise their suppression effects on muscle strength. We will not administer reversal drugs until patients regain their consciousness for the purpose of minimising the weakening of muscle strength caused by propofol. Besides, the effect site concentration of propofol will be recorded at the beginning of the measurement of ultrasound when TOFr=0.9 in order to analyse if it is comparable between the two groups. As for remifentanil, we will not stop infusion at the same rate of 0.1 mcg/kg/min until the patient is extubated to avoid bucking and coughing. Thus, we think the residual effect of remifentanil between the two groups is comparable as well.
Ultrasound evaluation of diaphragm function has been utilised in many clinical scenarios for many years.21 29–31 Except for the diaphragm, the recovery of other muscles (expiratory muscles, upper airway muscles, limb muscles) is also vital for patients’ outcomes. As for parasternal intercostal muscle, recent studies confirmed that parasternal intercostal muscle thickness could be measured by ultrasound with good interobserver reproducibility.32 33 Moreover, ultrasonographic evaluation of GM movement was suggested to be a novel but useful method in the assessment of swallowing dysfunction for different diseases without significant discomfort for patients.12 34 35 All these studies showed the feasibility of assessing muscle function and excluding rNMB using non-invasive ultrasound tool in the postoperative period.
We choose microlaryngeal surgeries for the following reasons. First of all, microlaryngeal surgery is a short procedure but requires a deep neuromuscular blockade to provide optimum surgical conditions.36 Second, unlike the abdominal surgery chosen by most studies where the incision may damage the abdominal muscle fibres and obvious postoperative pain may limit the patient’s deep breathing, the postoperative pain of microlaryngeal surgery is negligible so the effect of pain on respiratory muscle strength can be eliminated. Last, analgesia regimens with rapidly metabolised opioids such as remifentanil appear to be the most widely accepted in microlaryngeal surgery,37 and sparing of long-acting opioids minimise the suppression on respiratory muscle strength. Therefore, the microlaryngeal surgery represents an ideal setting where it is necessary to include NMBA administration, but at the same time, fast and complete recovery of muscle function is needed.
In conclusion, the present study will be the first clinical trial designed to detect the effect of low-level residual paralysis after reversal with neostigmine or sugammadex on global and respiratory-related muscle strength in the early postoperative period by dynamometer and ultrasound.
Ethics and dissemination
The protocol was viewed and approved by the Ethics Committee of the First Affiliated Hospital, Sun Yat-sen University on 2 June 2020. The ethical approval number is [2020]180. All documents communicating with the ethics committee will be kept in the researcher’s folder. If it is necessary to modify this protocol during clinical research, it will be reviewed by the hospital ethics committee and implemented after approval. Written informed consent will be obtained from each subject. The objectives and methods, benefits, possible risks and solutions will be clarified clearly for all subjects by the authors. Data monitoring will be performed by a researcher who is not involved in the study. All personal information will be registered with absolute confidentiality. All subjects have the right to cease participation in this trial at any time for any reason. In the case of perioperative unexpected events, including a change in drug dose or serious complications such as massive haemorrhage and anaphylactic shock and patients with failure to cooperate during evaluation, the subjects will be withdrawn from the study, and the events will be recorded on the CRF. If patients need medical care that interferes with the correct conduct of the study, they will be treated according to clinical routine and will be excluded from the study. With regard to dissemination, the results of this study will be published in an academic journal. The Standard Protocol Items: Recommendations for Interventional Trials guidelines were adhered to in the production of the protocol for this trial (see uploaded material for details).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
XW and YL are joint first authors.
XW and YL contributed equally.
Contributors XW and YL contributed to the work equally. YX and XW designed the study. YX, XW, YL and CH conducted the pilot study. CH contributed to the sample size calculation. YX, XW and YL drafted the manuscript. CH, WX, QZ and LN provided further inputs and edited extensively before finalisation. All authors reviewed and approved the final submitted version of the manuscript.
Funding This trial will be supported by a grant from the Wu Jieping Medical Foundation. Grant number is not applicable. The funding body will provide funds for engagement of statistical support from Clinical Trial Center of the First Affiliated Hospital, Sun Yat-sen University and will pay for all study-related expenses including manuscripts processing fees. It is not involved in the design of the study, and collection, analysis and interpretation of data, and in writing of the manuscript.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.