Article Text

Abstract
Introduction Among US veterans, more than 78% have a body mass index (BMI) in the overweight (≥25 kg/m2) or obese range (≥30 kg/m2). Clinical guidelines recommend multicomponent lifestyle programmes to promote modest, clinically significant body mass (BM) loss. Primary care providers (PCPs) often lack time to counsel and refer patients to intensive programmes (≥6 sessions over 3 months). Using peer coaches to deliver obesity counselling in primary care may increase patient motivation, promote behavioural change and address the specific needs of veterans. We describe the rationale and design of a cluster-randomised controlled trial to test the efficacy of the Peer-Assisted Lifestyle (PAL) intervention compared with enhanced usual care (EUC) to improve BM loss, clinical and behavioural outcomes (aim 1); identify BM-loss predictors (aim 2); and increase PCP counselling (aim 3).
Methods and analysis We are recruiting 461 veterans aged 18–69 years with obesity or overweight with an obesity-associated condition under the care of a PCP at the Brooklyn campus of the Veterans Affairs NY Harbor Healthcare System. To deliver counselling, PAL uses in-person and telephone-based peer support, a tablet-delivered goal-setting tool and PCP training. Patients in the EUC arm receive non-tailored healthy living handouts. In-person data collection occurs at baseline, month 6 and month 12 for patients in both arms. Repeated measures modelling based on mixed models will compare mean BM loss (primary outcome) between study arms.
Ethics and dissemination The protocol has been approved by the Institutional Review Board and the Research and Development Committee at the VA NY Harbor Health Systems (#01607). We will disseminate the results via peer-reviewed publications, conference presentations and meetings with stakeholders.
Trial registration number NCT03163264; Pre-results.
- primary care
- nutrition & dietetics
- medical education & training
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Peer-Assisted Lifestyle (PAL) intervention was developed through rigorous formative work to provide evidence-based 5As (Assess, Advise, Agree, Assist, Arrange) counselling delivered by peer coaches in combination with brief counselling by primary care providers (PCPs).
PAL was designed to serve as an adjunct or stand-alone intervention, providing more moderate intensity systematic obesity counselling, appealing to patients who do not have the time, ability or motivation to attend an intensive programme.
The evidence gained from this study will inform a broader model for integrating peer-supported counselling within private and public healthcare settings.
Assessment accuracy could be reduced because some of the study measures rely on self-report, which can be affected by recall and social desirability biases.
Difficulties might arise regarding implementing a rigorous study protocol in a real-world setting due to factors such as PCP and peer coach turnover, which may affect counselling quality and frequency.
Introduction
The burden of obesity is substantial. In 2014, more than 78% of US veterans had a body mass index (BMI) in the overweight (≥25 kg/m2) or obese range (≥30 kg/m2)1–5 despite their access to care through the Veterans Health Administration (VHA), America’s largest integrated healthcare system. Primary care providers’ (PCP) obesity counselling can help promote behavioural changes and modest body mass (BM) loss.6–8 PCPs, however, often do not counsel patients9 10 due to competing demands11 and lack of training.11 12 The average number of PCP visits (3.6 visits/year) is too few to provide an intensive intervention as per clinical guidelines (≥6 sessions over 3 months13 or ≥12 sessions/year).14–16 Intensive lifestyle programmes such as the MOVE! programme offered through VHA can produce modest BM loss and decrease cardiovascular risk.17 Although the VHA provides access to obesity treatment through systematic screening and referral, in reality, fewer than 8% of eligible veterans attend MOVE!.18 19
Peer coaching has the potential to improve obesity treatment for veterans. In other populations and settings, including primary care, peer coaches effectively delivered obesity interventions to support health behaviour change.20–27 The peer coaching approach may be appropriate for veterans given the strong communal identity and the camaraderie felt by those with shared military experience.28–30 Because peer coaches share a similar background, they can understand and help address barriers specific to veterans such as the change from leaving the highly structured military environment.31 Among female veterans, support from military friends after separation from service has been associated with better health outcomes.28 Further, peer-led interventions among veterans with diabetes improved glucose control.32 33
We developed a novel technology-assisted peer coaching intervention, called the Peer-Assisted Lifestyle (PAL) intervention, that uses the 5As (Assess, Advise, Agree, Assist, Arrange) counselling framework34 and was adapted from our Goals for Eating and Moving (GEM) study.35 A pilot study of the GEM intervention (n=22) showed modest BM loss when compared with control (n=23) for 6 months (−1.5±3.1 kg vs 0.2± 3.6 kg, p = 0.08).36 The PAL intervention builds on our experience with GEM,35 with the added focus on peer coaches to address the specific needs of veterans. The PAL study’s aims are to (1) determine the impact of PAL on BM, clinical and behavioural outcomes; (2) identify predictors of BM loss related to PAL intervention components and goal-setting processes; and (3) evaluate PAL’s impact on PCP obesity-related counselling attitudes and practices.
Methods and analysis
Study design and overview
This cluster-randomised controlled study compares the PAL intervention to enhanced usual care (EUC). PAL includes an in-person peer coaching session, 12 peer coaching phone calls over 1 year and brief PCP obesity counselling during routine medical visits. In-person data collection occurs at baseline, month 6 and month 12 (figure 1).

The Peer-Assisted Lifestyle (PAL) study design. EUC, enhanced usual care; PCP, primary care provider.
Setting and participants
At the Brooklyn campus of the Veterans Affairs New York Harbor Healthcare System (Brooklyn VA), primary care teams have one to five PCP among other medical staff (eg, registered nurses). The Brooklyn VA has a diverse patient population. Patients enrolled in our study (n=251, as of 31 December 2019) were identified as African–American (59.5%), white (22.8%) and Hispanic/Latinx (79.3%).
PCP participants
We enrol PCP, including residents, with a panel of at least 250 primary care patients.
Veteran participants
Eligible patients are between the ages of 18 and 69 years (MOVE! eligibility criteria),18 under the care of a PCP with at least one prior visit in the past 2 years, have a BMI of ≥30 kg/m2 or a BMI of ≥25 kg/m2 with an obesity-associated condition (ie, hypertension, high cholesterol, sleep apnoea, osteoarthritis, metabolic syndrome or pre-diabetes),14 16 have access to a telephone and have the ability to travel to the Brooklyn VA. We exclude patients who are non-veterans, have a documented history of active psychosis or other cognitive issues via ICD-10 codes, have participated in more than four sessions of MOVE! in the past year, are pregnant, have a PCP stating that the patient should not participate, or have a self-reported inability to read at a fifth grade level due to literacy skills or vision problems.
Recruitment and screening
Potentially eligible patients are identified using the Veterans Health Information Systems and Technology Architecture (VistA). PCP review patient lists to identify other contraindications to participating. Patients receive an invitation letter about the study. Research staff then calls patients to recruit, screen for eligibility and schedule the baseline visit. Enrolment began in January 2018 and has been suspended since March 2020 due to the COVID-19 pandemic.
Randomisation and blinding
In 2017, PCPs (n=17), along with their eligible patients, were initially randomised to either PAL (n=8) or EUC (n=9) using a random number generator. In 2018, five PCP left the VA, and in 2019, two new PCP joined the VA and were randomised so that 14 PCPs are currently active in the study (PAL=6; EUC=8). Patients of PCP that left were assigned new PCP by VHA. Those patients remained in the same study arm assigned at the time of enrolment due to the intention-to-treat methodology. As in other behavioural interventions, patients, peer coaches and PCP cannot be blinded to group assignment. We anticipate that the majority of research assistants (RAs) will not be blinded. While we take care not to divulge study arm assignment during measurement visits, our pilot study revealed that patients frequently reported health coach interactions to the RAs conducting outcome assessments. Thus, to minimise assessment bias, we use rigorous training protocols for RAs to standardise the collection of anthropomorphic measures and survey administration. Lastly, the data analyst is blinded to group assignment.
PAL intervention description
Peer coach training
Peer coaches have at least a bachelor’s degree but no clinical degree or license and had to have served in one of five branches of the US military with honourable discharge. They receive a minimum of 20 hours of training delivered by the principal investigator (PI) and/or senior coaches based on a prior intervention.37 Peer coaches learn techniques based on motivational interviewing (MI)38 including brief action planning, review coaching manuals and use role-playing and audiotape review to practise counselling skills. MI materials are adapted from the Centre for Collaboration, Motivation, and Innovation (CCMI).39 Peer coaches learn to promote small lifestyle changes, provide empathic care to minimise perceived obesity stigma, identify red flags and barriers (eg, binge eating, hypoglycaemic, untreated depression or pain). To ensure ongoing training, peer coaches meet biweekly with other coaches, the study coordinator and/or PI to discuss cases and share best practices.
Fidelity
We use a modified version of the VA ASPIRE health coach fidelity checklist40 to monitor skill acquisition and quality of counselling. A random subset (minimum 10%) of peer coach sessions are audiotaped and reviewed by research staff using the fidelity checklist. Refresher training will occur periodically as needed. We also document reasons for missed sessions.
PCP training
PCP receive training during year 1 of the study (approximately 45 min) with at least one follow-up training by the PI. Similar to the peer coach training, this session is based on previously developed MI training protocols,37 and other adapted MI materials through CCMI.39 We educate PCP about the various MOVE! programmes (eg, in-person MOVE! or TeleMOVE!) and receive contact information for referrals. We provide an overview of the 5As, the intervention components, and practice brief MI (through role-play) to support patients’ goals and address barriers to change. We scheduled either one-on-one or in small groups so as not to interfere with clinical or administrative duties.
Fidelity
We assess the quality of PCP counselling with patient surveys during in-person study visits (see the Aim 3: PCP counselling section and table 1 for timing). Also, we use a chart abstraction tool to monitor how often PCP see patients and document goal-setting discussions during visits after enrolment. We evaluate the percentage of clinical reminders completed in the EHR to document counselling or reasons for not counselling.
Study measures and assessment points
PAL intervention arm
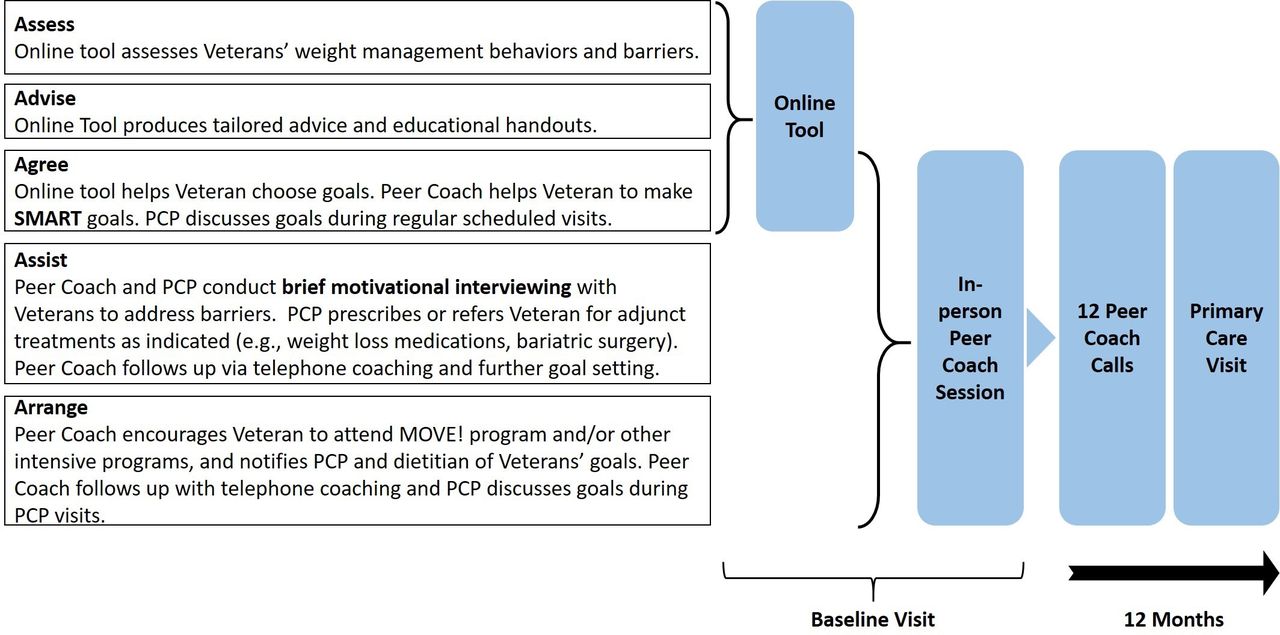
To deliver 5As-based obesity counselling, PAL uses in-person and telephone-based peer support, a tablet-delivered goal-setting tool and PCP training. Figure 2 describes how the PAL intervention elements fit into the 5As model. Patients in the PAL intervention complete the following items. The estimated time to complete each step stem from pilot testing.

Integration of the Peer-Assisted Lifestyle (PAL) intervention components and the 5As (Assess, Advise, Agree, Assist, Arrange) counselling framework. PCP, primary care provider; SMART, Specific, Measurable, Attainable, Relevant, Timely.
Online tool (20 min, baseline visit)
The development of the tool is described elsewhere.41 The tool is delivered via a tablet computer. It assesses healthy behaviours, barriers and facilitators related to BM loss (see online supplemental file A for questions), provides tailored advice and guides patients to set BM loss (5%–10%), diet and physical activity (PA) goals. It advises about intensive programmes and self-monitoring options. The tool generates an individualised patient report summary and tailored educational materials based on the patient’s answers that are assembled into a personalised binder.
Supplemental material
Computerised patient record system notes and clinical reminders
The online tool also creates a report that the peer coach enters into Computerised patient record system (CPRS, the VA’s Electronic Health Record (EHR). This clinical note summarises information about the peer coach session for the PCP and generates a clinical reminder. During the next visit, the reminder facilitates documentation about whether the PCP discussed goals and provided further counselling.
In-person peer coach visit (40 min, baseline visit)
After the patients complete the online tool, they meet with a non-clinician, peer coach. The peer coach works with patients to achieve health-related goals using MI38 and SMART (Specific, Measurable, Attainable, Relevant, Timely) goal setting.42 The peer coach performs the following tasks:
Use worksheets to turn goals into SMART goals42 and encourage participation in MOVE!, MOVE!TLC, or other programmes by providing brief MI with SMART Action Planning43 to address barriers (20 min).
Teach self-monitoring of BM, diet and PA behaviours via pedometer, food log and/or apps (eg, MOVE! Coach,44 My Fitness Pal)45 (10 min).
Enter a report for the PCP into CPRS summarising the encounter to communicate patients’ progress to the PCP (10 min).
Twelve telephone coaching calls (30–40 min each)
To achieve sufficient intensity according to clinical guidelines,15 PAL incorporates 12 telephone coaching calls by the peer coach over 1 year. Scheduled calls occur every 2 weeks (biweekly) for the first month and monthly for the remainder of the intervention. Patients receive a reminder call from the peer coach to self-monitor their BM, food intake and PA for at least 3 days before the coaching call. Studies suggest that episodes of short, consistent self-monitoring (for 3 days) lead to BM loss and may promote better adherence.46 Peer coaches use self-monitoring data to determine goal adherence, counsel patients and encourage small changes.47 They help patients create new goals when appropriate and use MI techniques to address barriers to behaviour change.
PCP counselling (3–5 min)
PCP in the PAL intervention arm are encouraged to provide brief MI to address barriers and discuss lifestyle goals, as needed, during regular medical visits. They document counselling with CPRS reminders (figure 3) and collaborate with peer coaches to discuss the patients’ progress.

{kind=link}
{kind=link}
{kind=link}
Logic model of the clinical reminder to facilitate weight management counselling.
EUC control arm
Veteran patients in the EUC arm receive non-tailored healthy living handouts by RAs as well as information about the MOVE! programme including contact information to enrol. Patients follow up with their PCP for usual care.
Retention
Follow-up visits are scheduled at the baseline visit. One month prior to study visits, patients receive a reminder flyer in the mail. Additionally, 1 week and 1 day before their visits patients receive reminder phone calls from the RA. We also ask patients to provide contact information of a friend or family member to facilitate retention. To compensate for travel and time spent completing study measurements, veteran patients receive $60 for the baseline visit, $45 for the 6-month visit and $50 for the 12-month visit.
Quality control
The study team meets weekly to monitor recruitment, data collection procedures and unanticipated adverse events. Any serious adverse events are reported to the Institutional Review Board. A data safety monitoring board (composed of VA leaders from ambulatory care, biostatistics and health services research) meets every 6 months to evaluate the data quality and timeliness, recruitment, accrual and retention, and participant risk versus benefit. The board has the authority to halt the trial if it perceives that harm is occurring due to the intervention.
Study measures
In-person study visits to collect data occur in a private research office or clinic room at the Brooklyn VA at baseline, 6 months and 12 months (table 1). During each in-person study visit, an RA administers a survey and collects anthropometric measures.
Aim 1: anthropometric measures
BMI
Participants remove their shoes, heavy clothing, empty their pockets and undo interfering hairstyles. Participants stand with heels, buttocks, shoulder blades and back of head positioned against the ruler. Stature is measured once, rounded up to the nearest 0.5 cm, using a SECA 213 Portable Stadiometer. BM is measured at least twice using a HealthOMeter 349KLX Digital Medical Scale and rounded to the nearest 0.1 pounds. If the first two measures differ by 0.5 pounds or more, RAs take a third measure, averaging the two closest values for data analysis.
Waist circumference
RAs measure at the high point of the iliac crest on bare skin at minimal respiration, rounding down to the nearest 0.25 inch. If the first two measures differ by 0.5 inches or more, RAs take a third measure, averaging the two closest values for data analysis.
Blood pressure
Using an automated sphygmomanometer (Omron HEM-907XL), RAs measure blood pressure at least 30 min into the survey administration. This delay ensures that the patient has not consumed any caffeine or participated in PA during this time. If the first two systolic or diastolic values differ by 5.0 mm Hg or more, RAs repeat the two measures, and take the average of the two closest values for data analysis.
Aim 1: behavioural outcomes
Intensive lifestyle programme attendance
To evaluate the attendance (number of sessions) to MOVE! programmes, we use electronic chart review. We also assess the self-reported use of intensive programmes via survey items.
Physical activity
The International Physical Activity Questionnaire–Short Form (IPAQ-SF)48 is used to measure the intensity, frequency and duration of PA and walking. Participants also wear Actigraph Link accelerometers (model GT9X-BT) on the non-dominant wrist for 7 days after all in-person visits (figure 1). The data from the ActiGraph monitor will be processed using ActiLife software. PA behaviour characterised will include total PA expressed as average daily vector magnitude units, time spent sedentary, and in light and moderate to vigorous intensity.
Dietary changes
We assess fruit and vegetable intake using a seven-item subscale of the validated Food Behaviour Checklist (FBC),49 sweet and salty snack consumption using two items adapted from the Rapid Eating Assessment–Shortened Version (REAP-S),50 51 and dietary changes including portion sizes for processed foods and sugar-sweetened beverages using six items from the Latino Dietary Behaviours Questionnaire (LDBQ).52
Self-monitoring and lifestyle behaviours
Patients report on how many days (scale: 0–7) during a typical week in the previous 6 months they have performed the following behaviours: weighing themselves, tracking their diet and PA, cooking a healthy meal at home and working out.53
Aim 2: BM-loss predictors
Motivational factors
We assess self-efficacy for exercise54 and for resisting overeating using the Weight Efficacy Lifestyle Questionnaire Short Form.55 We also assess the stage of change for healthy diet56 57 and exercise,58 and outcome expectations for changes due to participation in exercise.59 60 To assess intrinsic motivation for BM loss and self-monitoring, we use a subscale from the Treatment Self-Regulation Questionnaire61 62 (see online supplemental file B for questions).
Supplemental material
Use of PAL intervention
We record the number and duration (in minutes) of phone coaching calls. During each telephone coaching session, patients report the attainment of their SMART goals.42 To assess improvement in BM loss, PA and dietary behaviours, we ask the patients about their use of pedometers and food logs (paper or via smartphone apps), and collect their recorded data. During study visits, the patients answer questions about their experience with their peer coach (eg, ‘How willing would you be to go back to your peer coach for further support?’ or ‘My peer coach seems to know what he/she is doing.’).63 During exit interviews after the 12-month visit, the patients answer open-ended questions about any other health and lifestyle-related changes, and their experiences with PAL.
Aim 3: PCP counselling
Quality and frequency
To assess the use of 5As-based counselling, veteran patients report on their PCP use of 5As counselling practices (survey items that we have used previously).64 Adapted from previous research,63 the patients also report their satisfaction with their PCP treatment plan (eg, ‘My doctor is making good decisions about how to help me manage my weight problems’), their perception of fairness of decision-making and treatment (eg, ‘My doctor listens to my views’) and their willingness to follow their PCP recommendations (eg, ‘I am trying very hard to follow my doctor’s recommendations’). EHR reviews and chart abstraction provide information on the frequency of counselling (eg, completion of clinical reminders).
Competency and attitudes
We survey PCP before receiving training about obesity counselling and again after at least 12 months to measure 5As-related counselling competency and attitudes about obesity (including self-efficacy, outcome expectancy, discomfort and bias) using validated survey items65 (see online supplemental file C for the survey). PCP will participate in exit interviews to answer open-ended questions about their experiences with PAL.
Supplemental material
Data analysis
Main outcomes will be analysed using intention-to-treat methodology. All the variables will be summarised using mean (SD) and median (IQR) for continuous variables and frequency tables for categorical variables overall and by study arms, respectively. Although the randomisation should balance the treatment arms, we will use Mann-Whitney tests for continuous variables and Fisher’s exact tests for categorical variables to explore if both patients’ and PCP baseline characteristics may differ between the two arms.
Aim 1: anthropometric measures and behavioural outcomes
The primary outcome is mean BM loss at 12 months. To compare outcomes between the two arms, we will use Mann-Whitney tests for continuous outcomes (eg, BM loss) and Fisher’s exact tests for categorical outcomes (eg, number of patients achieving ≥5% BM loss). Unadjusted CIs will measure PAL’s effects on the outcomes compared with EUC. Also, repeated measures modelling based on mixed models will compare outcomes between study arms, using baseline and follow-up data to adjust for characteristics (eg, diabetes, gender), considering: (1) the correlation among patients within PCP and (2) the correlation among repeated measures within patients. Model-based adjusted CIs will be provided to demonstrate PAL’s effects on the outcome variables. These analyses combine the strength of both non-parametric tests, which are more powerful, and parametric tests, which are more robust, to justify our findings.
Aim 2: BM-loss predictors
Visualisation tools (eg, scatterplots) and descriptive analyses (eg, Spearman correlation coefficients) will display associations between BM change and potential BM-loss predictors (ie, motivational factors and use of PAL). Multivariate linear regression models for continuous variables and multiple logistic regression models for binary variables will further examine these predictors’ associations with BM loss. We will construct classification and regression trees (CARTs) to generate the variable importance for each intervention component.
Aim 3: PCP counselling
Mann-Whitney tests for continuous provider-level outcomes and Fisher’s exact tests for categorical provider-level outcomes will be used to compare the study arms at each survey. CIs of the effects will be computed as well.
Missing data analysis
Although the repeated measures modelling can address missing data automatically under the assumption of missing-at-random, we will further analyse the missing data due to loss of follow-up or non-response using an inverse-probability-weighting approach and a multiple-imputations approach. These approaches adjust for response bias based on baseline characteristics. To conduct sensitivity analyses under the practical assumption of missing not at random, multiple-imputations procedures with pattern-mixture models will examine the robustness of our findings when considering the least-favourable scenario where missing data from the PAL and EUC arms follow the same pattern.
Sample size and power analysis
We based our sample size on within-person BM change from baseline to 12 months in each arm. As similarities in BM change within clusters should only stem from PCP potentially treating their patients in their unique way, we assume a small but conservative interclass correlation coefficient of 0.0366 for patients of each PCP and a coefficient of variation of 0.25 for the cluster size, which was based on the data available at the Brooklyn VA. With eight physicians in the control group and six in the intervention group, we aim for 369 evaluable patients at 12 months to achieve 80% power and 5% type-I error for detecting a 2.4 kg (SD=6.0 kg) BM difference between the two arms. This amount of BM loss is consistent with findings from the ASPIRE VA study47 and a systematic review of technology-assisted BM-loss interventions in primary care.67 By incorporating a 20% dropout rate, PAL aims to recruit 461 patients.
Patient and public involvement
Feedback from patients and PCP enrolled in prior studies41 68 informed PAL’s framework and intervention design. We assess the burden of the intervention among PAL patient and PCP participants during exit interviews (see the Study measures section). A summary of the results will be made available to the public after the study’s conclusion and publication of the primary outcomes.
Discussion
Developed through rigorous formative work, PAL provides comprehensive 5As counselling delivered by peer coaches in combination with brief counselling by PCP. Delivered by phone, PAL minimises patient travel and addresses logistical barriers like time and location, accommodating even hard-to-reach populations, such as those with lower income or who live in rural settings. PAL can serve as an adjunct or stand-alone intervention, providing more moderate intensity systematic counselling, appealing to patients who do not have the time, ability or motivation to attend an intensive programme. To promote PCP counselling, PAL includes brief PCP training, peer coaching notes and clinical reminders. PAL is designed to fit into the workflow without overburdening the healthcare team, addressing important PCP barriers to counselling: lack of time and training.11 12 It requires 3–5 min of PCP time for brief counselling and documentation, which is a workload that was acceptable to most healthcare staff.41 68
PAL may encounter challenges implementing a study protocol in a real-world setting. PCP and peer coach turnover may affect counselling quality and frequency. In anticipation of these challenges, patients are assigned a second back-up peer coach. The delivery of PAL may differ between patients as they may experience different barriers, prefer varying resources and set individualised nutrition and PA goals. To address these potential confounders, we assess these differences in implementation (eg, types of goals) as well as fidelity of counselling. These data will also help generate hypotheses about which components are most effective and fill a critical research gap; a systematic review on motivational interviewing in telehealth interventions finds that few trials (2 of 15) reported how engagement in different components and fidelity measures related to BM-loss outcomes.69
Assessment accuracy could be reduced because some of the measures rely on self-report (eg, PA), which can be affected by recall and social desirability biases. Although RAs receive comprehensive training and follow rigorous protocols, the lack of blinding to participants’ group assignment could result in measurement biases that inadvertently favour the intervention group. Lastly, while we aim to recruit a representative sample and have few exclusions for eligibility, patients who enrol in the study may feel more motivated than the average primary care patient, making the results less generalisable. Because PAL is investigated within a single VA site, future studies may test the implementation of PAL within different healthcare systems and populations.
This study emphasises the importance of incorporating obesity counselling in primary care and adds the innovation of using peer coaches, which addresses the specific needs of veteran patients and is cost-effective. The PAL intervention has the potential to improve obesity treatment within primary care and could serve as a model for integrating peer-supported evidence-based 5As obesity counselling within urban healthcare settings.
Ethics and dissemination
All study procedures have been reviewed and approved by the Institutional Review Board and the Research and Development Committee at the VA NY Harbor Health Systems (#01607). All participants are provided oral and written information on the study and asked to sign an informed consent form (see online supplemental file D) and a Health Insurance Portability and Accountability Act (HIPAA) authorisation (see online supplemental file E). Only authorised study staff will have access to the study data.
Supplemental material
Supplemental material
Acknowledgments
We thank our research staff and veteran peer coaches for their many contributions to the project: Vito Lattanzi, Terrell Fulton, Greg Mueller, Drury Duval and Andrea Aquines. We also extend our gratitude to our volunteer research assistants: Ruha Zahur, Erin Hall, Leon Ronoh, Shirley Chen, Xintong Gu, Izza Nawaz, Tammy Yang, Damiya Kaleem, Juliana Esposito, Tuhina Persaud and Britney Xu. We would also like to thank Dr Marina Fronshtein and the MOVE! team at the Brooklyn VA, New York Harbor Healthcare System, and Jeremy Pomeroy from ActiLife. Not least of all, we thank all of the patients and providers who participate in the PAL study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @WittlederPhD, @stephorstad
Contributors MJ initiated the collaboration, conceived of and obtained funding for the project. SES and CT contributed to the conception and design of the study. SS, SW, JMB, SLO and VS helped with developing the survey and data collection tools. YF and BW devised the statistical analysis plan and monitor data collection. AS advised on the development and implementation of the qualitative methods associated with the study and contributes to associated dissemination activities. MJ developed the conceptual model. SS and DG developed intervention materials and protocols. SS, LW and PD implement the study protocol. SS and LW manage the project day-to-day and supervise staff. All coauthors contributed to the conception of this work and critically reviewed and approved the final manuscript.
Funding This work was supported by the Department of Veterans Affairs, Health Services Research & Development Service, 810 Vermont Avenue, NW Washington DC 20420, Grant Number IIR 15-378. The funding source had no role in study design, data collection, data analysis and interpretation of data, in the writing of the report, and in the decision to submit the article for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.