Article Text

Abstract
Objectives The four SARS-CoV-2 variants of concern (VOC; Alpha, Beta, Gamma and Delta) identified by May 2021 are highly transmissible, yet little is known about their impact on public health measures. We aimed to synthesise evidence related to public health measures and VOC.
Design A rapid scoping review.
Data sources On 11 May 2021, seven databases (MEDLINE, Embase, the Cochrane Database of Systematic Reviews, Central Register of Controlled Trials, Epistemonikos’ L-OVE on COVID-19, medRxiv, bioRxiv) were searched for terms related to VOC, public health measures, transmission and health systems. No limit was placed on date of publication.
Eligibility criteria Studies were included if they reported on any of the four VOCs and public health measures, and were available in English. Only studies reporting on data collected after October 2020, when the first VOC was reported, were included.
Data extraction and synthesis Titles, abstracts and full-text articles were screened by two independent reviewers. Data extraction was completed by two independent reviewers using a standardised form. Data synthesis and reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews guidelines.
Results Of the 37 included studies, the majority assessed the impact of Alpha (n=32) and were conducted in Europe (n=12) or the UK (n=9). Most were modelling studies (n=28) and preprints (n=28). The majority of studies reported on infection control measures (n=17), followed by modifying approaches to vaccines (n=13), physical distancing (n=6) and either mask wearing, testing or hand washing (n=2). Findings suggest an accelerated vaccine rollout is needed to mitigate the spread of VOC.
Conclusions The increased severity of VOC requires proactive public health measures to control their spread. Further research is needed to strengthen the evidence for continued implementation of public health measures in conjunction with vaccine rollout. With no studies reporting on Delta, there is a need for further research on this and other emerging VOC on public health measures.
- health policy
- public health
- COVID-19
Data availability statement
Data are available upon reasonable request. The datasets may be made available by emailing the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To the authors’ knowledge, this rapid scoping review is the first to comprehensively synthesise the evidence related to variant of concern (VOC) and public health measures.
This review involved stakeholder engagement throughout the entire review process to ensure findings were accurately reported and relevant for end users.
The majority of studies were preprints and not yet peer reviewed, thus findings should be interpreted with caution
This rapid scoping review highlights the heterogeneity of the existing literature and provides recommendations for future research.
As of May 2021, most studies reported on Alpha and none reported on Delta, suggesting that ongoing research is needed on the impact of public health measures on newly emerging VOC.
Introduction
The SARS-CoV-2, responsible for COVID-19, was initially detected in December 2019, and in March 2020, the WHO declared COVID-19 a global pandemic.1 As of May 24 2021, over 166 million cases of COVID-19 had been detected worldwide, and 3.5 million deaths have been reported as a result of the virus.2 The growing number of COVID-19 cases presents significant challenges for health systems as they try to adapt and enforce public health measures to control the spread of the virus to prevent further death and disability.
An additional public health challenge of COVID-19 is related to the emergence of SARS-CoV-2 variants of concern (VOC).3 The WHO defines VOC as novel SARS-CoV-2 strains with increased potential for transmission, presence of genomic mutations and rapid spread across nations or regions with potential for decreased effectiveness of public health measures.4 As of 31 May 2021,5 the four circulating VOCs include Alpha (B.1.1.7) and Beta (B.1.351) which were both identified in December 2020, Gamma (P.1) which first originated in January 2021 and, most recently, Delta (B.1.617.2) which emerged in May 2021.6 While evidence continues to emerge about these four VOCs, there are clear indications that they are more transmissible than non-VOC strains.7–9 The increased transmissibility of VOC highlights the urgent need for countries to enforce measures to prevent further spread of COVID-19.
Initially, national governing bodies were directed to manage the spread of COVID-19 through a combination of public health measures and health system restructuring.10 While the WHO provided initial instruction for managing the spread of COVID-19,11 contextual differences between regions meant public health officials had to make decisions in the absence of evidence. The majority of public health measures initially introduced across jurisdictions focused on reducing virus transmission through general public health protocols such as hand washing, coughing etiquette, avoiding person-to-person contact and staying home if unwell.11 However, as more information about COVID-19 began to emerge, public health officials introduced additional measures such as mask wearing, testing, lockdowns and border restrictions.12–14 After the introduction of these public health measures in early 2020, many countries witnessed a downward trend in case numbers by mid-2020, signalling the stabilisation of wave 1.15 These epidemiological trends indicated the potential, positive impact of public health measures on mitigating COVID-19.
While public health measures were effective in slowing the initial spread of COVID-19, the emergence of VOC presents a new challenge for public health officials and policy makers. With continuously changing and limited available evidence on the highly transmissible VOC, there is a need to explore how public health measures impact the spread of VOC, and whether changes to public health protocols are needed in relation to VOC characteristics. Therefore, the aim of this study was to synthesise the literature on the four circulating VOCs and their impact on public health measures. This study attempted to answer the following research questions, which were determined through consensus meetings with knowledge users and stakeholder groups:
What is known about the global implications of the four circulating VOCs for public health measures on:
Modifying approach to vaccination?
Modifying infection prevention measures in the community?
Modifying infection control procedures?
Methods
Study design
A rapid scoping review was conducted, following standard methodological guidelines for rapid16 and scoping reviews.17 This type of review can be beneficial to inform urgently needed practice or policy change, which is the case for the rapidly evolving COVID-19 pandemic.18 Ethics approval was not required for this study. The research team collaborated with knowledge users (public health and infectious disease experts, researchers and policy makers) through regular meetings to identify the research question, design the search strategy and synthesise the evidence. The research question was guided by the Population, Context and Concept framework proposed by scoping review guidelines.17 For the purpose of this review, population includes individuals/communities affected by VOC, concept includes public health measures and context includes any country or region.
Patient and public involvement
Patient partners, experienced in patient engagement but not the lived experience of being diagnosed with COVID-19, were invited to review the summary of findings table. Patient partners will assist in disseminating the key findings of the published paper for a public and lay audience.
Protocol
The study protocol was registered with Open Science Framework (https://osf.io/tkrbm/).19
Search strategy
A literature search was designed by an information specialist (LB), trained in scoping review methodology, to identify all sources related to VOC. Seven electronic databases were searched, including MEDLINE (Ovid MEDLINE All), Embase (Elsevier), the Cochrane Database of Systematic Reviews (CDSR), Central Register of Controlled Trials (CENTRAL) (Cochrane Library, Wiley), Epistemonikos’ L-OVE on COVID-19, medRxiv and bioRxiv. No limitation was placed on date of publication, but the search was restricted to English-only sources. Any non-English results returned by the search were translated where possible and considered for inclusion. The search was conducted on 11 May 2021. The full search strategy for all databases can be found in the online supplemental material 1.
Supplemental material
Eligibility criteria
Studies were eligible for inclusion in the review if they reported on any of the four VOCs which were identified by the WHO at the time of the search: Alpha, Beta, Gamma and Delta (also known as B.1.1.7, B.1.351, P.1 and B.1.617.2, respectively). Studies also had to report on public health measures, relating to three overarching subtopics: modifying approach to vaccines, infection prevention or infection control measures. This could include studies that reported on lockdown measures, quarantine, physical distancing, mask wearing, hand washing, outbreak management and/or vaccination scheduling. Any study setting, country and population were eligible for inclusion. Due to the first VOC, Alpha, being identified in October 2020, any studies that reported on data collected before October 2020 were excluded. Grey literature preprint articles were also eligible for inclusion in this review. Studies that reported on immune escape, vaccine efficacy, non-VOC-related impacts, novel testing approaches, transmission, health system measures, animal studies or case studies without data related to public health measures were excluded. While this review did not consider studies that reported on health system impacts, these data were extracted and synthesised in a separate review (Dol J et al Health systems impacts of SARS-CoV-2 variants of concern: A rapid review).
Screening
Screening occurred in two stages and was conducted by 11 authors (MS, JAC, JD, LB, AJG, HW, HDS, MM, RM-M, BR, DC). First, titles and abstracts of identified studies were uploaded to the online systematic review synthesis software, Covidence,20 and independently screened in duplicate. Then, full texts of articles were reviewed and independently screened in duplicate. Conflicts were resolved by an independent reviewer from the research team (MS, JD, JAC or LB). All screening tools were pilot tested prior to use.
Data extraction
A data extraction form was developed based on the research questions and in collaboration with the knowledge user partners. Study characteristics, including study design, population, sample size, country, date of publication and objective, were reported in the data extraction form. Details about the type and number of VOCs reported in the study were also extracted. Outcome data related to the specific public health measures employed in the study were extracted and reported in the standardised data extraction form.
Quality appraisal
Although quality appraisal is an optional step in scoping review methodology, based on discussions with knowledge users, it was decided to include this step in our review.The Newcastle-Ottawa Scale (NOS) was used to appraise observational studies in this review.21 As the NOS tool was originally developed for case–control and cohort studies, the adapted NOS tool22 was used to appraise studies of cross-sectional design. Modelling and laboratory-based studies were excluded from quality appraisal. Following a pilot test, two members of the research team (MS, BR) independently completed quality appraisal of the included studies. Researchers then met to discuss their final scores. When researchers disagreed on their scores, a third independent team member (JAC) joined the discussion until a consensus was reached about the final quality score of each study. Preprint studies are sometimes excluded from reviews; however, due to the rapidly emerging nature of COVID-19 research, preprint studies were included for synthesis. An additional layer of quality appraisal was applied to preprint studies by subtracting two points from preprint study scores. This deduction was based on advice from knowledge users and methodological experts (ACT, LS, SH, AD).
Data synthesis
Following data extraction, reported outcomes from each study were described and categorised based on public health topic. The findings were reported in a table alongside the quality appraisal score. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews23 checklist guided the reporting of this study (figure 1).
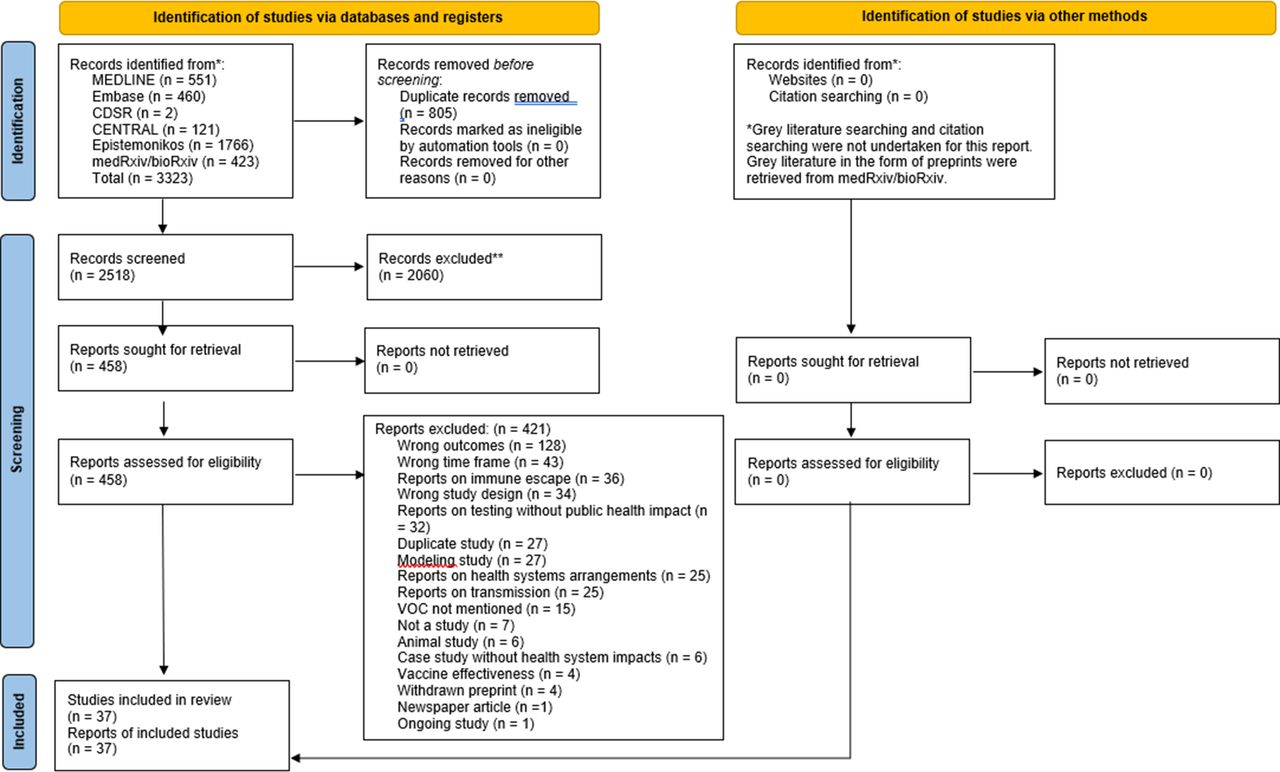
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. VOC, variant of concern. From: Page MJ et al66
Results
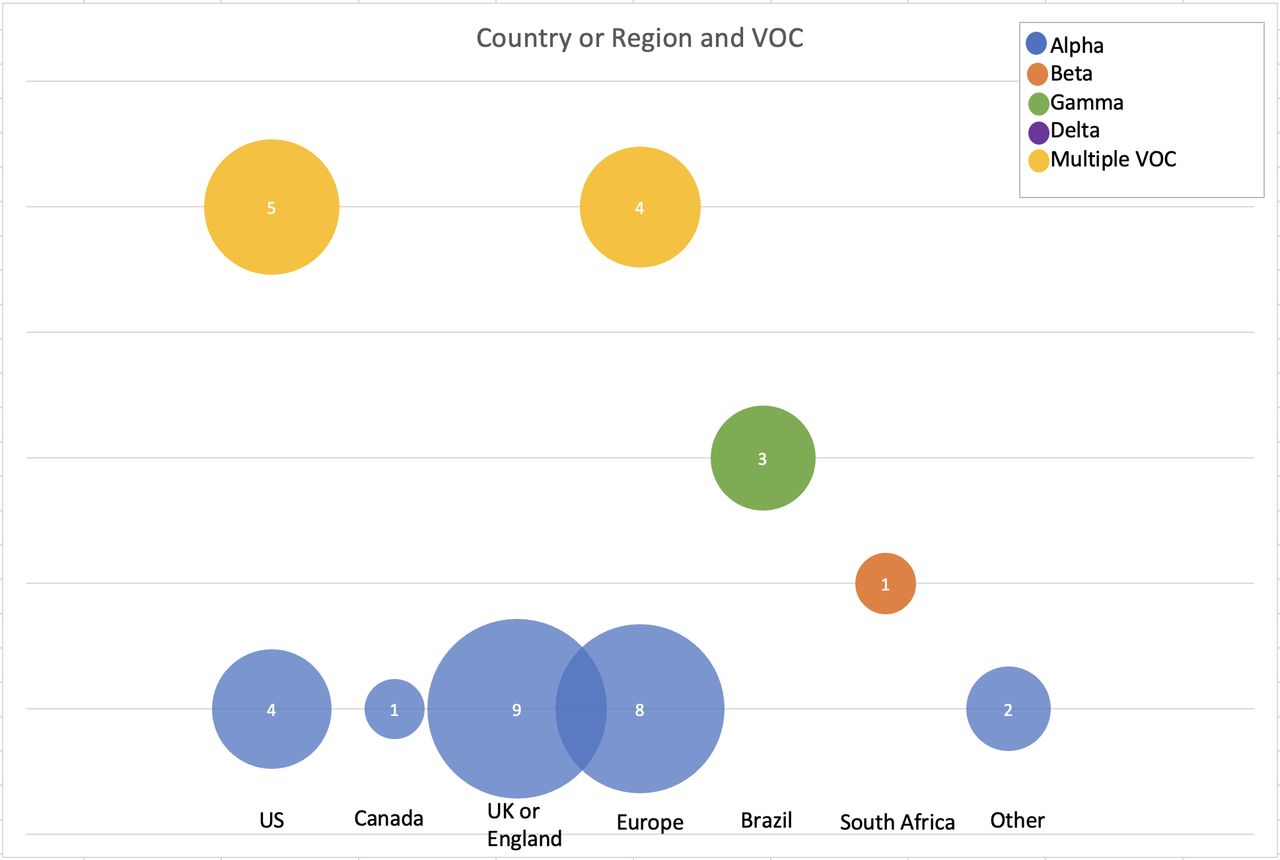
The electronic database search identified 3323 records. After removal of duplicates, 2518 studies were screened for eligibility. A total of 37 studies reporting on public health measures in relation to VOC were included after screening. The majority of included studies reported on the Alpha VOC (n=32).24–54 The majority of studies were conducted in Europe (n=12),24 29 30 34 35 39 40 44 47 51 53 55 followed by the UK (n=9),26 28 32 33 36 42 45 50 56 USA (n=9),25 37 38 41 43 48 49 54 57 Brazil (n=3),58–60 Canada (n=1),31 South Africa (n=1),27 Israel (n=1)46 and Japan (n=1)52 (figure 2). Additional details of each study can be found in the online supplemental material 2.
Supplemental material

Overview of country or region of data collection and variant of concern up until 11 May 2021.
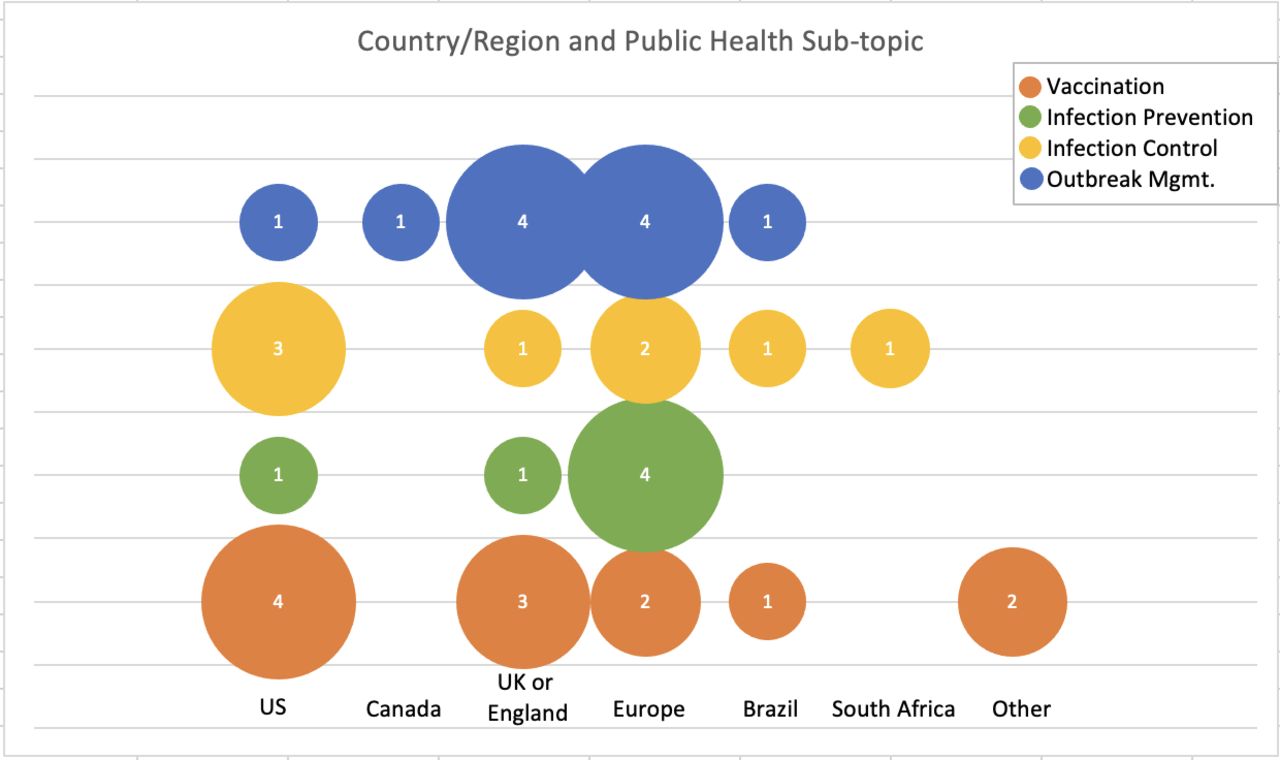
The majority of studies were modelling studies (n=28) and 28 were preprints. Nineteen studies reported on infection prevention measures, of which 11 were specifically related to outbreak management. Twelve studies reported on modifying approach to vaccinations and seven studies reported on infection prevention measures (figure 3).
{kind=link}
{kind=link}
{kind=link}
Overview of country or region of data collection and public health subtopic up until 11 May 2021. VOC, variant of concern.
Quality appraisal
Of the 37 studies included in this review, three were cohort studies and four were cross-sectional studies, and therefore underwent quality appraisal. Cohort study scores ranged from 44% to 89% while cross-sectional studies ranged from 10% to 80%. Of these seven cohort/cross-sectional studies, two were categorised as low quality,28 42 three were of medium quality26 31 58 and two were considered high quality32 36 (table 1).
Quality appraisal scores based on NOS tool for observational study designs
Question 1A: modifying approach to vaccination considering VOC
Of the 12 studies that reported on modifying approaches to vaccination in consideration of VOC, seven were modelling studies,35 38 43 46–48 52 three were observational studies28 42 58 and two were laboratory-based studies.33 57 Of the three observational studies, one was appraised as medium quality58 and two were appraised as low quality.28 42 Therefore, the findings should be interpreted with caution. The modelling and laboratory-based studies were not appraised. Ten studies reported on different vaccine schedules and VOC.33–35 38 43 46 47 52 57 58 One study reported on attitudes towards vaccines related to VOC prevalence28 and one study compared natural protection versus vaccine protection against VOC.42 A summary of studies can be found in table 2.
Study summary on findings related to modifying approach to vaccination, categorised by study topic
Vaccine schedules that offer greater protection
The 11 studies that reported on modifying approaches to vaccine schedules and VOC were further categorised into two subsections: (1) exploring vaccine protection using a correlate of laboratory neutralisation in consideration of variants; and (2) exploring different vaccination schedules. Further details on each of these studies can be found in table 2.
Exploring vaccine protection using a correlate of laboratory neutralisation in consideration of variants
Three studies contributed data on mRNA vaccines,33 43 57 which together showed vaccine protection after a second dose (also referred to as booster dose) against the Alpha,33 43 Beta43 57 and Gamma43 57 VOCs. Additional protective effects were noted for older adults in one study.33
Exploring different vaccination schedules
Seven modelling studies and one observational study examined the impact of changes in vaccine scheduling on VOC. Findings from these eight studies highlight the importance of an accelerated vaccine rollout either in isolation38 48 58 or in conjunction with non-pharmaceutical interventions (NPIs)35 46 47 51 52 to prevent VOC-related transmission, hospitalisations and deaths. Vaccine rollout scenarios varied across studies in terms of length and intensity, and included campaigns ranging from 6 to 24 months47 and vaccination rates of 9/1000 doses per person per day48 to 1/250 doses per person per day.52 The NPIs studied included physical distancing, testing strategies and lockdowns of varying intensity, with one modelling study of 20 unique scenarios reporting NPIs to be more important than vaccine rollout.35
Attitudes towards vaccination related to VOC
One cross-sectional study assessed changes in COVID-19 vaccine hesitancy related to VOC in the UK in late 2020 when Alpha began circulating.28 Following the emergence of Alpha, intention to receive the vaccine increased among participants, with changes in attitudes associated with certain demographic characteristics.
Comparing immune protection after COVID-19 infection and vaccination
One prospective cohort study of healthcare workers (HCW) in the UK assessed the protection following infection from Alpha and one or two doses of Pfizer or AstraZeneca vaccines.42 Alpha did not significantly alter the extent of protection following natural immunity or first dose of vaccine, which means natural infection and/or vaccination may effectively protect against Alpha.
Question 1B: modifying infection prevention measures in the community
The second subquestion addressed by this review related to the impact of infection prevention measures, such as hand washing, mask wearing and physical distancing, in the presence of VOC. Of the seven studies which reported on this subtopic, five were modelling studies,34 37 40 41 53 one was a laboratory-based study44 and one was observational.26 The observational study was appraised as medium quality. A summary of studies can be found in table 3.
Summary of studies reporting on public health infection prevention measures in the community up to 11 May 2021
Hand washing
One study compared the stability of the wild type, Alpha and Beta, on different surfaces and their sensitivity to heat, soap and ethanol.44 Both wild type and VOC were efficiently inactivated on treatment with at least 30% ethanol for 30 s and hand soap for 1–5 min, confirming that current measures of hand hygiene would be effective against Alpha and Beta.
Mask wearing
Gurbaxani et al modelled face mask efficacy parameters for a variety of mask types and fit.37 They found masks have potential for significant reduction in both VOC and non-VOC transmissions, even with moderately effective masks, when they are consistently worn correctly by a large portion of the population.
Physical distancing
Five studies assessed the impact of physical distancing on transmission of Alpha26 34 40 41 53 and/or Beta.41 Together, these studies found that due to the increased transmissibility between contacts, additional NPIs should be in place alongside physical distancing measures to contain VOC spread.26 34 40 41 53 These studies considered various settings, including community,34 workplaces,53 schools26 40 and universities.41
Question 1C: modifying infection control procedures
The third subquestion addressed by this review related to adjusting infection control procedures in the presence of VOC, such as duration of quarantine, testing strategies, contact tracing and outbreak management. Of the 17 studies reporting on infection control procedures and VOC, 12 were modelling studies,25 29 30 39 45 49 50 54–56 59 60 3 were observational31 32 36 and 2 were laboratory-based studies.24 27 Two of the observational studies were appraised as high quality32 36 while one was considered medium quality.31 A summary of studies can be found in tables 4 and 5.
Summary of studies presenting findings on testing and duration of quarantine related to VOC up to 11 May 2021
Summary of studies presenting findings on outbreak management related to VOC up to 11 May 2021
Duration of quarantine and/or isolation
Two modelling studies explored the impact of quarantine on cases and deaths related to Beta54 59 and/or Alpha.54 Both studies highlighted the increased transmissibility of VOC would require lengthier quarantines to control their spread both within and between countries.
Frequency or change of testing for VOC
Two studies reported on implications for potentially modifying existing public health testing measures. One study evaluated the use of a primer that could be used in a rapid, low-cost screening protocol to detect VOC.24 A second study evaluated the PanBio SARS-CoV-2 Rapid Antigen Test in a sample of patients in South Africa, which was found to be effective at detecting both wild type and Beta.27 Together, these studies highlight potential, novel testing strategies for detecting VOC when access to laboratories for genome sequencing is limited.
Contact tracing
No studies were identified related to the impact of VOC on contact tracing.
Changing approach to outbreak management
Thirteen studies reported on different approaches to outbreak management across a range of settings and outcomes. Four studies discussed managing outbreaks through stricter lockdowns,25 36 39 49 four studies reported on the impact of physical distancing on outbreak management29 31 32 60 and five studies reported on outbreak management through various public health measures across community settings.30 45 50 55 56
Managing outbreaks through lockdown measures
The four studies reporting on managing outbreaks through lockdown measures evaluated the impact of Alpha on transmission36 39 and/or the economy25 49 through lockdowns of varying length and intensity. Together, these studies found that strict lockdowns effectively reduced transmission of Alpha while less strict lockdowns would see the reproductive number exceed one36 39 49 and contribute additional financial costs to society.25 49 One study suggested the most effective approach to mitigate the impact of Alpha would be a combination of frequent, systematic testing along with quick, strict lockdowns.39
Managing outbreaks through physical distancing
Four studies explored managing outbreaks through physical distancing measures on the spread of Alpha29 31 32 and Gamma.60 Of the four studies, one assessed community spread29 and three assessed household spread.31 32 60 All four studies found that physical distancing measures were associated with a decrease in transmission.29 31 32 60 However, in one of these studies, Gamma transmission was higher when individuals remained close to home, and where space was potentially limited.60 This study highlights the need to tailor public health measures to specific populations and that vigilance regarding household transmission is warranted.
Managing outbreaks through other public health measures
Five studies explored managing outbreaks through other public health measures, not previously discussed. Three studies modelled vaccination schedules and NPIs against outbreaks of Alpha.30 45 55 Together, these studies found that due to increased hospitalisation, intensive care unit (ICU) admission and death related to Alpha, subsequent waves will only be prevented if two doses of vaccine are administered quickly along with strict NPI measures.30 45 55 One study calculated that due to the increased transmissibility of Alpha, public health measures should be strengthened by 33.7% to mitigate the spread.56 The fifth study which explored the impact of temperature on VOC found that although warmer temperatures were associated with lower VOC transmission, this was only secondary to the impact of public health measures.50
Discussion
This rapid scoping review synthesised the evidence from 37 studies which reported on VOC and public health measures. While the types of public health measures varied in nature, the majority of studies were related to infection control measures, and in particular, outbreak management. Evidence overwhelmingly supports the implementation of NPI measures (eg, lockdowns, physical distancing, mask wearing and hand washing) alongside accelerated vaccine campaigns to mitigate the impact of the highly transmissible VOC.
Most studies contributing data on vaccinations reported on mRNA vaccines. This is not surprising as the first vaccines to be approved for use were two mRNA vaccines, commonly known as Pfizer-BioNTech and Moderna.61 62 While our review did not report on vaccine efficacy, more research is needed to understand the impact of modifying vaccine rollout for non-mRNA vaccines, such as AstraZeneca, on VOC transmission. In addition, the three studies reporting on vaccine protection using a correlate of laboratory neutralisation included small samples of 34–51 individuals. There are limitations in generalising these findings to a wider population. The findings of our review clearly suggest vaccination campaigns be accelerated in response to the more transmissible VOC. Some models suggest a vaccination rate of 60–90 doses per day per 10 000 population is required to mitigate VOC risk.48 52 Additionally, certain age groups, such as older adults, should be targeted to optimise immune response and prevention efforts. This is in line with many countries’ vaccine rollout plan where vaccine eligibility was largely based on age and HCW status.63 64 Clearly, there is an urgent need for public health officials to adjust their pandemic response measures to include accelerated vaccine campaigns to mitigate the spread of VOC.
Studies in our review suggest strong NPI measures be implemented in parallel with enhanced vaccine scheduling. The increased transmissibility of VOC signals the need for more pre-emptive restrictions (close phase first and then open with low case numbers) versus reactive (open first, then close to prevent ICU saturation) strategies. Studies relevant to this question focused broadly on social distancing as a strategy, with no specific recommendation regarding objective metrics such as proximity time, distance or type of social distancing strategy. Included studies identified the need for attention to managing contacts in specific environments such as households, educational and early care centres, and workplace settings, yet few recommendations were provided to address these needs. Without clear recommendations, public health officials are left to make decisions based on rapidly changing epidemiology and limited empirical evidence. It is important to highlight that all included studies reporting on NPIs were effective against VOC to some degree. Clearly, further research is needed to guide public health recommendations in response to VOC.
We identified limited evidence focused on modification to hand washing or masking related to the emergence of variant strains. This is surprising as public health messages from national governing bodies encourage mask wearing and hand washing as key infection prevention measures.12 Although this may be considered a gap in evidence, it is possible that these recommendations were based on non-VOC data and have remained unchanged with the emergence of VOC. With significant COVID-19 research efforts focused on developing and distributing vaccines, it is possible that some public health measures were implemented ahead of evidence. Certain measures, such as hand washing, are common recommendations for other viruses like influenza, and although there is mixed evidence on the effectiveness of hand washing in the community,65 hand washing recommendations for COVID-19 are likely based on implicit evidence. Despite the possible reasons for limited evidence associated with public health measures and VOC, this highlights a need for further research in this area.
Limitations
The rapid review study design allowed for a robust and timely synthesis of current evidence related to VOC and public health measures, highlighting a strength of this study. However, due to the rapid production of the literature, the majority of papers in this review were preprints and have thus not yet undergone peer review. This must be considered when interpreting study findings. Additionally, our search strategy was limited to articles that specified reporting on one of the recognised VOCs (Alpha, Beta, Gamma or Delta). Given the growing trend that VOCs are replacing the wild type as the dominant strain and the continued emergence of other variants of interest, future consideration of expanding the search strategy may be warranted. Additionally, as the search was conducted during a time when the Delta VOC was just beginning to emerge (May 2021), no studies in this review reported on Delta. New evidence related to this VOC may have emerged since running the search. Another limitation of restricting to studies that reported specifically on VOC, it is difficult to interpret some of the findings without taking into consideration the wider literature on SARS-CoV-2. For example, we report on attitudes towards vaccines only in context of VOC, without wider acknowledgement of the extensive body of literature on vaccine hesitancy for non-VOC. Despite some of these limitations, our study provides a novel overview of VOC research, which has direct and immediate impact on population health. To our knowledge, no other reviews have provided a synthesis of research on this topic to date.
Conclusion
The findings from this review highlight the urgent need for further research employing rigorous study designs on the implications of public health measures and VOC. Apart from outbreak management and vaccine rollout models, we found limited evidence on other public health measures such as mask wearing and quarantine procedures. Further studies are also needed on the range of existing VOCs. Our findings highlight the need for further research to strengthen the evidence related to vaccine campaigns and public health measures to limit the spread of VOC.
Data availability statement
Data are available upon reasonable request. The datasets may be made available by emailing the corresponding author.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MariSomerville, @justinedol, @MisenerRuth
Contributors MS, JAC, JD and LB led the project and contributed to all aspects of the study including conceptualisation, screening, extraction, data synthesis, quality appraisal and manuscript writing. MS and JAC are the guarantors and accept full responsibility for the conduct of the study. LS, AD and SH developed the research questions and provided continuous expert opinion throughout the research process, including manuscript writing. BR contributed to quality appraisal, screening, extraction and manuscript editing. AJG, HDS, DC, HW, MM and RM-M contributed to screening, extraction and manuscript editing. HM contributed to manuscript editing and formatting. ACT provided methodological guidance and manuscript editing. JC provided content expertise and contributed to manuscript editing. All authors reviewed and provided feedback on the manuscript. Patient partners reviewed the key findings and will support the dissemination of findings.
MS and JAC are the guarantors.
Funding The SPOR Evidence Alliance (SPOR EA) is supported by the Canadian Institutes of Health Research (CIHR) under the Strategy for Patient-Oriented Research (SPOR) initiative. COVID-19 Evidence Network to support Decision-making (COVID-END) is supported by the CIHR through the Canadian 2019 Novel Coronavirus (COVID-19) Rapid Research Funding opportunity (grant number CKS-174105). ACT is funded by a Tier 2 CRC in knowledge synthesis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.