Article Text

Abstract
Introduction Despite the increasing diversity of UK medical students, students from low-socioeconomic backgrounds, some minority groups and members of communities with protected identities remain under-represented in medicine. In trying to ascertain why this under-representation persists, literature focuses on the barriers and challenges faced by under-represented students as opposed to the institution’s responsibility to remove or mitigate these obstacles. One UK University created a reverse mentoring scheme enabling students to mentor senior members of the medical faculty to help them understand the perspectives and experiences of students from minority backgrounds. This paper explores whether changes in staff perceptions of under-represented students resulted from engaging with reverse mentoring.
Methods This qualitative study explored the impact of the reverse mentoring scheme. Staff mentees were required to write a narrative text about the Higher Education journey of an under-represented medical student before and after the reverse mentoring intervention. These texts were compared using discourse analysis to identify shifts in language use that demonstrated a change in perceptions.
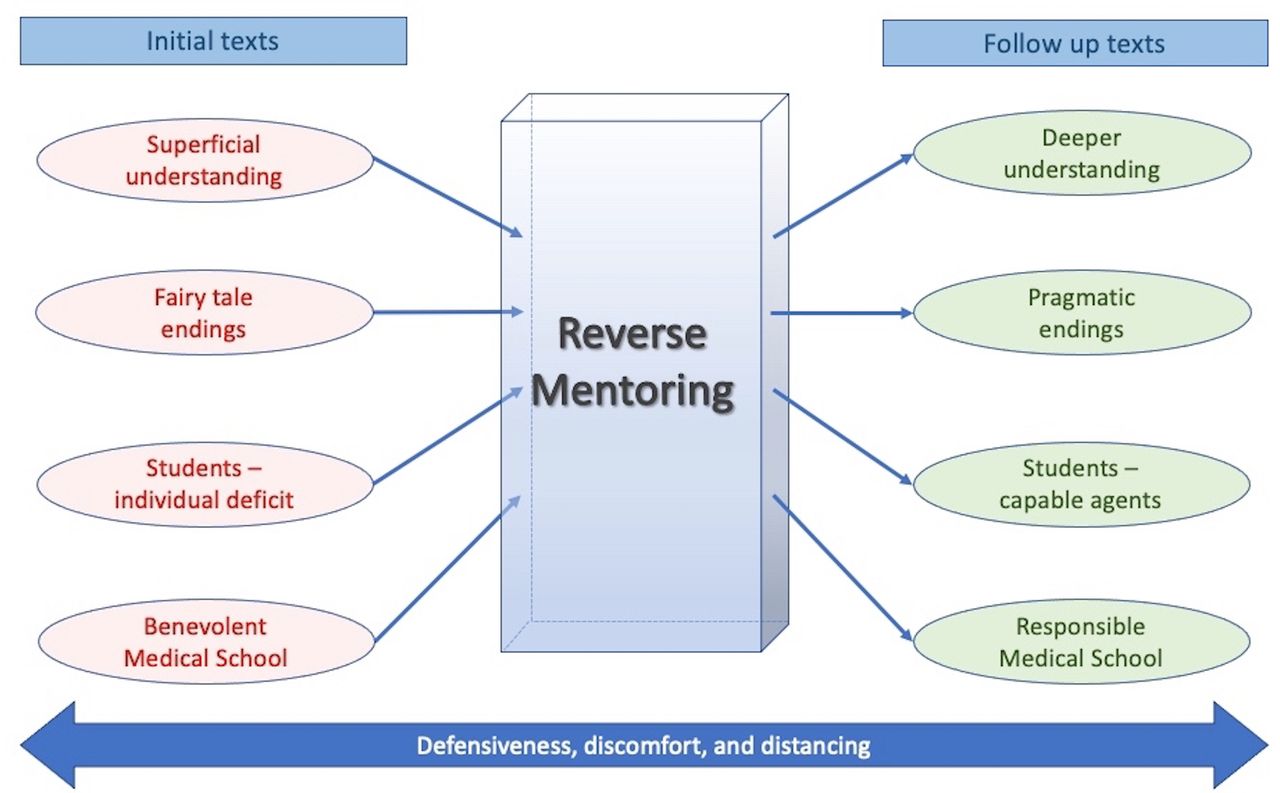
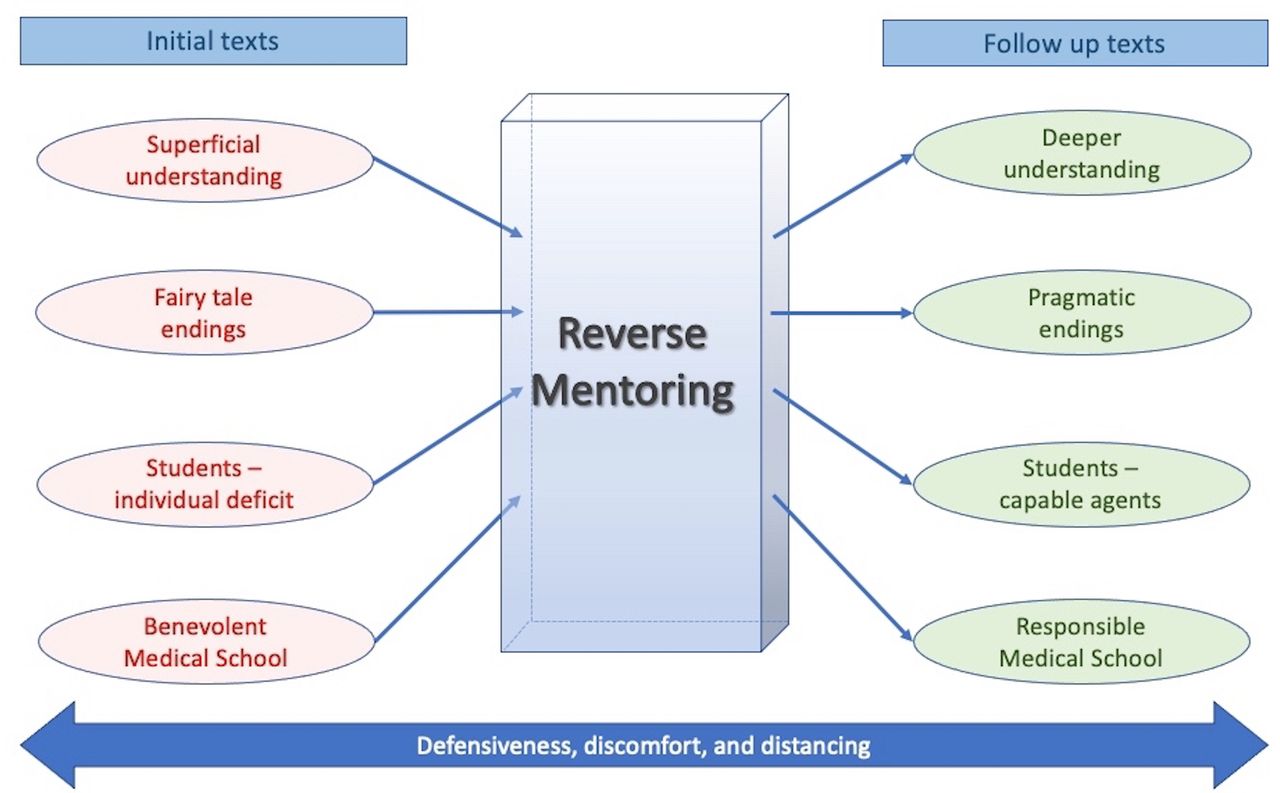
Results The key themes from five senior staff members indicate a positive change in staff characterisation of the students and an acceptance of institutional responsibility for challenges faced. Initial texts revealed a superficial understanding of the student journey that focused on individual deficit but had fairy tale endings depicting the medical school as benevolent. The follow-up texts revealed a deeper understanding reflected by the portrayal of students as capable agents and containing pragmatic endings acknowledging the responsibility of the medical school.
Conclusion These findings highlight how removed senior staff can be from the reality of the student experience and that engaging with reverse mentoring helps to raise awareness and challenges the students face. This suggests a route for constructive change in medical schools and endorses the benefits of facilitating open discussion around educational inequity.
- medical education & training
- education & training (see medical education & training)
- qualitative research
Data availability statement
Data are available upon reasonable request. All available data can be obtained by contacting the corresponding author (SC).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- medical education & training
- education & training (see medical education & training)
- qualitative research
Strengths and limitations of this study
This study aims to add new perspectives to existing evidence challenging the student deficit discourse, by exploring how reverse mentoring conversations can change senior medical school staff’s perceptions of medical students from under-represented backgrounds.
Discourse analysis provides insights into underlying attitudes, using this before and after the reverse mentoring intervention can indicate changes to individuals’ perceptions and how they portray or frame their thoughts.
The longitudinal impact of whether staff’s changing attitudes persist over time or how this impacted on their practice is not within the scope of this paper.
Introduction
Despite the increasing diversity of students in UK medical schools,1 students from low-socioeconomic backgrounds, some minority groups and members of communities with protected identities1 2 remain under-represented in medicine. In trying to ascertain why this under-representation persists, literature focuses on the barriers and challenges faced by students from under-represented backgrounds as opposed to institutional responsibility to remove or mitigate these obstacles.3–8 This exclusive emphasis on the barriers students face contributes to the student deficit model.9 10 The discourse around this model denotes students as lacking aspiration5 11–13 and the essential knowledge, skills and support systems, such as adequate encouragement from teachers14 15 and having parents who attended university.16 17
Students portrayed by the deficit discourse ‘require fixing’ to achieve academic success, with support programmes designed to ‘remedy’ student inadequacies.4 9 This implicitly frames universities as generous champions of opportunity,18 with benefits flowing in one direction from the institution to the student,19 which suggests additional support is required for an under-represented student to become suitable for studying medicine.20 By only offering support in the form of student remediation, institutions effectively circumvent their obligation to critically examine practices that may inhibit equal participation4 9.
The attainment gap, a difference in academic outcomes seen between groups of students from different social backgrounds, has been associated with the deficit discourse.21 In medicine, as in Higher Education (HE), the attainment gap is seen between white students and students from black and minority ethnic backgrounds7 8 and recently this has been evidenced for medical students from low socioeconomic backgrounds.22 Studies also show a higher rate of attrition for students from the aforementioned backgrounds than for their peers.22–25 The belief that differential attainment is the sole responsibility of the individual student feeds into the student deficit discourse. However, studies have shown the difference in performance remains after controlling for a variety of factors including attainment,23 socioeconomic,23 24 first language26 and assessments25 which indicates wider institutional concerns regarding causes of differential attainment.
Discourses are widely recognised as shaping social practices in medical schools.19 26 27 An analysis of interviews with Admissions Deans at 24 UK medical schools revealed how language presented non-traditional medical students as ‘other’ and as less suitable for studying medicine than students from more traditional medical backgrounds.20 These perceptions have clear implications for medical student selection, yet the Admissions Deans did not acknowledge any responsibility for perpetuating institutional inequity. This study, among others, illustrates that language and discourse reflect the attitudes and behaviours of medical school staff who have the power to facilitate institutional change.20 28 These studies also show how the deficit framing of under-represented students may affect students’ ability to access and participate equally in medical school.
It is essential we address this deficit discourse and change the behaviours of our medical schools and universities towards students from under-represented backgrounds. One way to address this challenge and enhance staffs’ understanding of under-represented students’ experiences is through conversation.29
Reverse mentoring is an inversion of the traditional mentoring model. It encourages meaningful conversations between mentors who would normally be considered junior and less experienced in a particular field, and mentees, who are typically regarded as more experienced or senior.30 Many senior medical school staff do not regularly meet or have opportunity to spend time with students and frequently hold privilege and come from backgrounds far removed from those of under-represented students. Implementing reverse mentoring of senior staff by medical students from under-represented backgrounds creates the time and support for conversations. This can enlighten staff to the realities of the student experience, and through wider discussion and dissemination challenge established and misconceived discourses.
The reverse mentoring scheme presented in this study focused on the mentors’ life experiences including disadvantage and discrimination. The aim of the scheme was to raise awareness of their experiences through conversation and challenge beliefs around barriers, facilitating behaviour change of the staff and their institution. This study aims to explore changes in mentees’ perceptions following reverse mentoring through their use of language.
Methods
Institutional context
The Faculty of Medicine at the University of Southampton delivers a range of undergraduate medical degree programmes for students from a variety of backgrounds; these include the 5-year standard entry programme which has an intake of approximately 170 students, and the 4-year graduate entry programme that has an intake of approximately 48 students. The 6-year Widening Participation programme delivers an additional year at the start to support students from backgrounds of social and economic disadvantage transition to University and has an intake of approximately 32 students. Southampton was one of the first medical schools to deliver a bespoke widening participation programme, which started in 2002, and is recognised as a leader in widening participation to medicine in the UK.
These programmes are designed with early patient contact from the first few weeks and are mainly academic for the earlier years and clinically based for the later years.
Study context
At the Faculty of Medicine, University of Southampton, a reverse mentoring scheme was designed to facilitate conversations between under-represented students and senior staff in a supportive and safe environment; this ran between March and June 2020. Medical student volunteers from low-socioeconomic backgrounds, minority groups and members of communities with protected identities were recruited via advertisements on social media and through the students’ regular email communication bulletin. Staff from the faculty board and those with senior education roles were recruited via email. All participants gave informed consent to take part in the study.
All staff and student volunteers were required to attend a training session to prepare them for their roles as mentors and mentees. The first section of the training was specifically designed to help prepare and support all participants for the reversal of the power dynamic seen in reverse mentoring. For the second part of the training session, the mentees and mentors were grouped separately; training for the mentees focused on preparing them for challenging conversations, to be more aware of their own biases and how they may contribute to microaggressions. For the mentors, the training focused on empowering them within the relationship and helping them to navigate the meetings. At the end of the session, the mentees and mentors regrouped, the mentor/mentee pairings were made and the date of the first meeting was established. Each pair was asked to hold minimum of four mentoring meetings outside of their timetabled activities over the next 2–3 months.
Data
Prior to the training, mentees were asked to write and submit a short piece of narrative writing entitled ‘The Higher Education journey of a student from a minority background’. They were given no further instructions on the style or approach to this task. The prompt was left intentionally open, so participants would interpret the task in their own way. From this point, the written accounts will be referred to as ‘texts’ for simplicity. Following completion of the training and mentoring sessions, staff were asked to provide a second, follow-up text of the same title. Due to the nature of the analysis, which required a direct comparison of the individuals’ texts, only mentees who provided both initial and follow-up texts were included in this study. From this point, these mentees will be referred to as participants.
Each participant was randomly assigned a letter to maintain anonymity. The initial texts were labelled number 1 (eg, A1), while follow-up texts were indicated by a number 2 (eg, A2). Labelling each text this way enabled a comparative analysis to be undertaken between each participant’s initial and follow-up texts, to identify any shifts or changes between them.
Discourse analysis
This qualitative, interpretivist study uses discourse analysis (DA) to explore change in language use before and after undertaking reverse mentoring. Language is a social practice, and the words we use contain values and convey our attitudes towards the things we describe.31 It can therefore be considered a form of social behaviour;32 one way of assessing behaviour change is through DA, which can aid the understanding of the relationship between language and beliefs by ‘exploring the way in which theories of reality and relations of power are encoded in such aspects as the syntax, style and rhetorical devices used in texts’ (p.145).33
This data-driven study is guided by Fairclough’s approach to DA,34 which has been used previously to analyse positions of power in the ways in which staff describe medical students from widening participation backgrounds,20 but is a relatively unusual approach in medical education research. Our analytical process began with word-level analysis, using this to interpret participants’ perceptions about students from minority backgrounds. We then considered how these perceptions may influence wider institutional practices and perpetuate inequality.31
We compared language use in each participant’s initial and follow-up texts, allowing us to consider how discursive features such as structure and vocabulary create meaning. These sorts of devices can provide an insight into more subconscious elements of an individual’s attitudes;35 while people may consciously adapt their language to accommodate perceived expectations, a more reliable indicator of their underlying attitudes may be how they portray or frame their thoughts.36
The research group read and discussed the initial texts before the follow-ups were submitted, identifying themes and ideas about how the students were presented. Once the follow-up texts were submitted, an initial DA of the text pairs was undertaken by CL and HM where they:
Began by refamiliarising themselves with the initial text for each participant.
Identified phrases and patterns of language used to construct both the under-represented students and the institution.
Asked questions as they read about what assumptions might underpin the ways that students were presented (discourses).37
Examined linguistic, structural and rhetorical features for the possible effects and functions of these features.
Grouped the statements into categories (such as ‘structural features’ and ‘construction of student’).
Repeated this process for the participants’ follow-up narratives.
Compared and critically discussed the initial findings for each pair of texts. Similarities and differences were teased out across the text pairs to develop overall categories.
Interpretations were explored and refined by the wider research group, and an additional category entailing ‘limitations to change’ was developed. The group then discussed the findings in relation to discourses about under-represented students. The process was iterative, with members of the research group referring to the data, wider social context and theory throughout the analysis.38
The core research group consisted of Medical Education staff from the University of Southampton and University of Bristol, and postgraduate researchers from the University of Southampton. All members of the core research group have work or research interests in the area of diversity and inclusion. To mitigate bias in the analytical process, we invited current and former members of the institution, not working in medical education, to read the data and contribute to the analysis. Our additional contributors widened the diversity of ethnic, sex and socioeconomic background of the research group. This helped to develop our interpretations, ensuring that a range of perspectives were incorporated, enhancing the robustness and credibility of the findings.39 40
Ethical approval was granted by the University of Southampton, Faculty of Medicine Ethical Review Board number 54470
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research
Results and analysis
Five of the eight staff members who took part in the reverse mentoring scheme provided both initial and follow-up texts following completion of the scheme and were included in the analysis (participants A–E).
The key changes between the initial and follow-up texts were identified through the structure and tone of the stories and how students were positioned within them. In addition, defensiveness, discomfort and distancing were identified in the initial text and continued in the follow-up texts. The key themes representing these changes are presented in figure 1.
{kind=link}
presents the key themes of the changes in language use seen between the initial and follow-up texts . Defensiveness, discomfort and distancing was a theme present in both initial and follow-up texts.
Structure: initial texts
All initial texts began by describing barriers faced by under-represented students, with two discussing general barriers like finance and preuniversity education, while the others attributed barriers to the individual: ‘I will be the first person in my family to go to University and, as a girl, my parents are not supportive of it’ (E1).
All concluded with a primary focus on the student: ‘I feel my confidence is beginning to grow and that this has been the right decision for me, even if it has been hard at times…’ (E1). They had somewhat idyllic, fairy-tale endings, in which the students achieved academic success or positive identity development in medical school: ‘progresses well through the programme, passing finals well’ (D1). Such endings offer a superficial interpretation of the students’ journeys and the obstacles they face, and perhaps reveal a lack of awareness of differences in attainment and other outcomes experienced by under-represented students.8 22
This style and structure presented unrealistic and idealised views of the student journey minimising, and at times overlooking, the challenges under-represented students face in entering and progressing through medical school. As the student characters moved from struggle to success by attending the institution, participants implicitly framed the university as the ‘hero’ of the story,18 and the student and their background as the ‘problem’, indicating a limitation to the participants’ understanding of the students’ challenges.
Structural changes: follow-up texts
Two follow-up texts began by describing students’ backgrounds that presented a more positive context than seen in the initial texts. One began by acknowledging that under-represented students have valuable knowledge to share with staff: ‘It has truly been a privilege getting to know my mentor. I have learned a lot’ (C2).
All follow-up texts had much more pragmatic endings which tended to focus on systemic elements of the student journey, such as ‘The education system needs to deliver a joined up consistent message that inequality should not adversely affect a person’s ability to learn’ (A2).
As opposed to the ‘fairy-tale’ style endings adopted in the initial texts, these follow-up texts ended with a clear indication of where the challenges lie in the institution and how they can be addressed, rather than assuming problems are solved simply by the student progressing through medical school.
Changing tone of the texts
A distinct stylistic shift was seen between some of the texts, with the informal tone of the initial narrative account being replaced by a more serious style in the follow-up. E1 used a ‘Dear Diary’ trope to narrate the piece; while effective at delivering points, this was a somewhat juvenile method of communicating poignant thoughts. This could indicate discomfort on behalf of the participant as it allows deflection of the serious issues being discussed. Similarly, a frequent use of exclamation marks in this narrative could be indicative of enthusiasm,41 relaying a superficial perception of the WP journey.
In E2’s follow-up text, the style is more serious and the points being made show greater poignancy ‘The GP clinic was in an area with a real ethnic diversity, and for the first time I could see that my background gave me an insight that could help patients’. This movement away from the trivialisation seen in E1 implies a far more thoughtful understanding of the student journey.
Student positioning: initial narrative accounts
The initial texts often attributed the challenges faced by students to deficient academic abilities, personal qualities and cultural and religious identities.
In most initial texts, participants referred to vague, undefined constructs relating to non-normative identities, such as religion and culture, as challenges for under-represented students: ‘I understand that culture is a potentially major barrier, this may interestingly be getting less of a barrier’ (C1). This statement implies that some cultures, those which are not ‘the norm’ in medical schools, are problematic (although how culture may function as a ‘barrier’ is not explained). This discourse positions students’ cultural identities as a problem, rather than a lack of inclusivity within the system. Any potential benefits of cultural identity, such as belonging to a supportive community or having greater awareness of patient backgrounds, are absent. By using vague terms (‘may’, ‘potentially’), C1 avoided making a strong commitment to this perception, which suggests a limited understanding of ‘culture’ or a discomfort in engaging with the topic. Furthermore, the adverb ‘interestingly’ connotes a more academic interest than an empathic concern for under-represented students.
Several of the initial texts presented under-represented students as passive actors, who simply reacted to external experiences. For example, B1 portrayed the under-represented students in their narrative as lacking aspiration, ‘My parents (…) encouraged me to study hard for a proper career like Law or Medicine’, and their poorer academic grades as a result of laziness rather than of any systemic factors, ‘My grades (…) depended on how much work I put in before an exam (…) My final grades were a disappointment but I was glad to get onto BM6 (WP) programme)’. B1 positioned the student as academically deficient and lacking drive, qualities which would not be expected in a description of a ‘typical’ medical student but are attributed here to an under-represented student. Nearly all barriers described by participants in the initial texts invoke discourses of deficit: ‘I would highlight language, finance, cultural and social barriers as some of the obstacles they have to overcome’ (A1). The use of listing implies that there are many problems, creating the sense that the volume of issues is seen as being beyond the scope for support. The pronoun ‘they’ places responsibility on the student to ‘fix’ their problems, negating any institutional obligation.
Student positioning: follow-up texts
All follow-up texts showed a shift in responsibility from individual deficit, more frequently portraying the under-represented student characters as capable and active agents within a challenging system.
In the three follow-up texts written from the perspective of student characters, under-represented students were portrayed as academic and ambitious; for example, ‘I had my heart set on studying medicine at Uni. My predicted grades were ABB, but I got 3A’s and spent the day on the phone to two medical schools who had places in clearing. It was really hard work’ (B2). The shift in focus from ‘my parent’s’ encouragement to study to go into medicine to ‘I had my heart set on studying medicine’ emphasises the student’s agency in working hard and taking responsibility for the effort they exert. The metaphor ‘had my heart set on’ constructs a passionate and committed student, contrasting the depiction of a student who passively falls into the BM6 (WP) programme after achieving disappointing grades (B1). The student in B2 was described as excelling academically, positioning them as belonging within the meritocratic model of medicine.
The follow-up texts offered more specific and detailed descriptions of some challenges faced by under-represented students. C2 shifted to third person, creating a more objective and authoritative tone: ‘A very practical issue was raised at that first meeting which was the embarrassment of not having a relative with enough (reliable) income to act as guarantor signatory on a letting agreement’. The inclusion of the adjective ‘reliable’ adds a level of detail, nuance and clarification to the description, while including the emotional experience of ‘embarrassment’ indicates an increase in empathy and a more personal interest in the minority student experience. The tone and level of detail in C2 suggests a deeper understanding of challenges faced by some under-represented students, and greater ease in discussing them.
A similar shift was identified in A2, which demanded action by institutions, rather than individual students, to address barriers to equality within education: ‘it is incumbent upon all organisations to actively review their current student journey from the view of someone from a minority background and make the system fairer’ (A2). A2 employed a more authoritative tone than A1, indicating greater knowledge, confidence and comfort in discussing minority student experiences. Throughout A2’s narrative, the university rather than the student was framed as responsible and accountable for their role in creating and perpetuating disadvantage. This was echoed by D2, who stated ‘…the university and medical school is not set up to acknowledge needs or wishes of all cultures or beliefs’.
Defensiveness, discomfort and distancing
The structural and linguistic changes between the initial and follow-up texts previously described indicate a positive impact of the reverse mentoring programme in challenging the deficit discourse. However, a number of statements in the follow-up texts suggest that some defensiveness, discomfort and distancing persisted around the issue of discrimination.
Participant D presented some more nuanced understandings of challenges faced by minority medical students in their follow-up text (D2), however, this was a near exact copy of D1. Participant D added to D1 ‘All of the above, plus:’ before including four new insights. This could represent an unwillingness to reflect on previous patterns of thinking, or to dedicate time and care to crafting a new narrative as all other participants did. It could also communicate defensiveness, an assumption they had been right before, so their views had not changed, suggesting issues of race and inequality in the medical school remain an uncomfortable topic for participant D.
Defensiveness and discomfort were also evident in E2: ‘Most of our lecturers are white. This does not reflect at all on the quality of their teaching or their attitudes towards students from black and minority ethnic backgrounds’. Although E2 presents a novel understanding of some systemic issues faced by under-represented students (by considering staff diversity and role models), the defensive posturing indicates fragility, represented by a need to protect themselves from real scrutiny of unconscious biases and thus minimises the significance of this issue. Participant E appears protective over the ‘quality of teaching’, demonstrating a desire to protect the current system, and perhaps their own identity as a teacher.
Participant C indicated a willingness to act to ‘make the system fairer’, presenting an offer to develop a guarantor system for under-represented students struggling to secure student accommodation: ‘If the group (of senior faculty staff) agree, I will take it away and work out the details of such a scheme’ (C2). The use of first-person pronouns and the verb ‘will’ communicate a determination and commitment to act on what they have learnt from the mentoring programme. However, it is caveated by hedging language (‘if the group agree’), possibly demonstrating some hesitance or lack of confidence in taking that action and belief that it is not their individual role to make systemic change.
Discussion
This study presents changes in discourse resulting from reverse mentoring of senior medical school staff by under-represented students. There is a clear shift from an idealistic and generalised to a realistic and more nuanced framing of the student position. This highlights how removed staff can be from the reality of the student experience and how this can change after engaging meaningfully with students. Senior faculty staff assumed greater knowledge and understanding of the systemic barriers faced by under-represented students, which led to increased awareness of institutional responsibility for the student experience. This was clearly demonstrated by the shift in the perceived position of the University from being the benevolent hero to being a source of barriers for under-represented students. However, the findings also reflected continued defensiveness, discomfort and distancing from issues of discrimination and disadvantage with respect to the staff members’ position and that of the institution. This indicates the development of awareness and consequent institutional change is a gradual process and further conversations or consolidation of altered understanding and behaviour are needed.
In accordance with the findings of Cleland et al’s study,20 the staff initially framed the medical school as fair and open and either ignored or minimised the role of the institution in both perpetuating and addressing the inequalities experienced by the characters they depicted. Under-represented students were initially characterised as lacking some of the academic and cultural resources required for studying medicine, which aligns with the student deficit model.9 20 27 The focus of the narratives was often on the students’ deficiencies and, as other researchers of the deficit discourse have identified, the onus was usually placed on the students to address their problems.42 43
The fairy-tale endings of the initial texts evoke the social mobility discourse, which reflects that a university education breaks ‘the transmission of disadvantage from one generation to the next’ (p.231),44 and is commonly promoted as the main purpose and benefit of widening participation in medicine in the UK.19 45 46 While HE does enable social mobility for many students,45 47 when presented alongside a deficit discourse, the social mobility narrative can reinforce perceptions that by attending university, under-represented students move from being ‘not good enough’ to being ‘more like the advantaged’ (p.11)46 and in alignment with middle class values.18 48 The university is cast as the gracious patron who grants these students a golden opportunity to achieve ‘better jobs’ and to ‘better myself’ (p.564).47 Moreover, universities are presented as powerful gatekeepers of this prospective and necessary transformation, as seen in our participants’ initial texts.
A reconceptualisation of the discourse around under-represented students, from deficit and problematic to valuable and enriching is critical to ensuring all students can participate equally in university.9 10 43 The follow-up texts in this study revealed a significant, positive shift in the ways that the students and institutions were characterised. Under-represented students were portrayed as possessing desirable aptitudes including academic ability and ambition; diversity and difference were no longer represented as a ‘problem’ to be fixed or accommodated within current systems.49 Instead, institutions were largely acknowledged as underprepared for meeting the needs of a changing student body, a key catalyst for improving equity in universities.9 Disadvantage was represented as a product of institutional inequities that could be tackled with systemic changes. This suggests that reverse mentoring is a way to improve understanding of the student experience and institutional inequities, which could help address the attainment gap.
The outcomes of this reverse mentoring scheme feed into the wider national discourse around fairness and equity in medical schools and the profession. The staff involved are both medical educators, but clinicians, researchers, medical administrators and hospital board members. Therefore, their changing attitudes will have benefits extending beyond the scope of the medical school, ultimately having the potential to influence clinical care and policy for the wider medical profession. It is interesting to note that despite national recognition as a leader in widening participation for nearly two decades, the student deficit discourse was still present in the faculty. This reflects the amount of time it can take for culture change to take place and to permeate belief systems.
Addressing barriers through system-level changes is unlikely to have a lasting or genuine impact without accompanying culture change.50 To be truly effective, this change needs to extend beyond medical schools to staff working in the profession itself, creating an inclusive run through of studying, training and working environments. This will take time and be challenging, for example, it will take many years for accessible and relatable widening participation role models to be available at all levels in all specialties. It will also take a significant and unified effort to address such changes across institutional and professional philosophy, policies and practice. Without authentic change in beliefs around the student deficit model, initiatives and policies to increase diversity, such as the use of contextual admissions, will have limited long-term impact. Effecting a cultural change in any large organisation such as universities and hospitals, requires open and honest conversations between all members,29 51 especially between those making and implementing policy with staff or students from under-represented backgrounds, to ensure equity.
These findings are the result of a small study with five participants from the same institution; in signing up for the scheme, participants have already demonstrated a willingness to change. Despite this, they provide fascinating insights and evidence of how meaningful individual conversations can prompt evolution of discourses about under-represented students. However, it should be noted the findings may not be entirely due to the conversations and could also result from the initial training. Measurements of the long-term impact cannot easily be made. While a longitudinal data collection methodology could confirm whether staff’s changing attitudes persist over time, there would be no way of ensuring this was a result of the scheme or how this impacted on their practice. It is also possible that the narratives are not fully reflective of the participants’ views and that discussions with their mentors provided them with knowledge about what they should say, rather than truly influencing their views. It is hoped the depth of analysis at a linguistic level accounts for this and has provided insights into participants’ views beyond their surface level accounts.
Conclusion
Through reverse mentoring and engaging in conversation with under-represented students, senior faculty staff embraced the opportunity for change and began to realise their own roles and responsibilities as a part of that change. Supporting institutional behavioural change by facilitating a shift in culture away from the student deficit narrative is vital in addressing inequities evidenced in medical schools and the profession.
Data availability statement
Data are available upon reasonable request. All available data can be obtained by contacting the corresponding author (SC).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethical approval was granted by the University of Southampton, Faculty of Medicine Ethical Review Board - Number 54470 Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are extremely grateful to Dr Nisreen Alwan (NA), Gino Graziano (GG) and Dr Jahangir Alom (JA) for their valuable insights into the analysis and presentation of the results. We would also like to thank all our participants and the student mentors that made this study possible. No patients or any members of the public were involved in this study.
References
Footnotes
Twitter @JacquieAKelly
Contributors SC obtained funding for the project and is acting as guarantor. SC, JK and JH developed the RM scheme and research study. SC prepared the ethics application. HM and CL undertook the initial data analysis with input from SC, JK and JH. SC, HM and CL drafted the paper. All authors contributed to the final paper.
Funding We would like to thank the Student Experience Directorate, University of Southampton, for funding the development of the project and for funding the open-access fee for this paper.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.