Article Text

Abstract
Purpose The Kyushu and Okinawa Population Study (KOPS) was established to investigate gene–environmental interactions in non-communicable diseases in Japan. Besides collecting blood samples and anthropometric measurements, we also obtained medical histories, psychological status and lifestyle habits, including physical activities and dietary patterns.
Participants KOPS is a community-based prospective cohort study and consists of participants from four southwestern areas in Japan. Baseline surveys were conducted between 2004 and 2007 (wave 1), and 2009 and 2012 (wave 2) at the sites of municipality-based health check-ups. A total of 17 077 participants were included, comprising 10 697 participants of wave 1 and 6380 participants of wave 2; the median age in both groups was 61 years. Among them, 3006 individuals participated in both wave 1 and wave 2 surveys.
Findings to date We have focused on either risk or confounding factors for non-communicable diseases. We have assessed the clinical utility of the newly developed biomarkers for impaired glucose tolerance, such as urinary myo-inositol and glycated albumin, and atherosclerosis, such as small dense low-density lipoprotein cholesterol. We have conducted an international collaborative study with Framingham Offspring Study to investigate ethnic differences in impaired glucose tolerance and cardiovascular diseases. We have found that insulin resistance and deficiency might account for the ethnic differences in impaired glucose tolerance and cardiovascular disease risks. As gene–environmental interaction analyses, we found a synergic effect of interleukin 28B single nucleotide polymorphisms (SNPs) and gender on the spontaneous elimination of hepatitis C, and a beneficial interaction of SNPs of high-density lipoprotein cholesterol and gender on the impact of physical activity. In addition, we reported eight novel loci contributing to the development and severity of coronary artery disease from a large genome-wide association study.
Future plans We plan to investigate further the clinical utility of the newly developed biomarkers and the gene–environmental interactions using prospective data.
- epidemiology
- lipid disorders
- cardiology
Data availability statement
No data are available. No additional data available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Kyushu and Okinawa Population Study is a large-scale, population-based prospective cohort and aims to investigate the gene–environmental interactions on non-communicable diseases in Japan.
We collected the extensive data on medical histories, lifestyle habits, psychological factors and genomic information as risk factors of non-communicable diseases.
The blood samples of all participants are stored at −80°C, allowing researchers to measure and assess biomarkers which are developed later.
The participants of this study are all Japanese, so the findings may not be applicable to other ethnic groups.
Due to the recruitment method that the participants were recruited at the sites of health check-up, there may be a selection bias and the study population may not be a truly random sample representation of the entire population in Japan.
Introduction
Cancer is the leading cause of death worldwide, accounting for nearly 10 million deaths in 2020.1 In Japan as well, cancer has been the leading cause of death since the 1980s. The number of cancer deaths in Japan has increased, with approximately 375 000 people who died of cancer in 2019, accounting for 27.3% of all deaths in Japan.2 The age-standardised mortality rate per 100 000 people for all cancer in Japan in 2019 was 96.5, similar to that of the USA (102.6) and the UK (113.2). That rate in China was 133.7, slightly more than in Japan3 (online supplemental table 1). In addition to cancer, atherosclerotic cardiovascular disease (ASCVD), including coronary heart disease (CHD) and stroke, also remains the leading cause of death and disability in the world. In 2019, both CHD and stroke were two of the world’s biggest killers, responsible for 16% and 11% of the world’s total deaths in 2019, respectively.4 As in the rest of the world, ASCVD remains a significant cause of death, still accounting for approximately 25% of deaths in Japan in 2019.2 The age-standardised mortality rates per 100 000 people for ischaemic heart disease and stroke in Japan in 2019 were 30.6 and 23.2, respectively, similar to the UK (43.1 and 20.2, respectively). Compared with Japan, the USA had a 2.5-fold rate of ischaemic heart disease (73.5) and a similar rate of 22.3 for stroke. China had three times the ischaemic heart disease mortality rate (97.6) and five times the stroke mortality rate (110.8) than Japan3 (online supplemental table 1). Since cancer and ASCVD develop based on non-communicable diseases, prevention of non-communicable diseases is essential to decrease the incidence of cancer and ASCVD. Recently, non-communicable diseases are considered multifactorial diseases and to be caused by interactions between genetic predispositions and hazardous environmental factors. With the recent development of genetic analysis technology, many epidemiological studies have started gene–environment interaction investigations in non-communicable diseases.5–7 To elucidate the gene–environment interactions, large prospective cohort studies with long-term follow-up are needed.
Supplemental material
The Kyushu and Okinawa Population Study (KOPS), launched in 2004, aimed to examine gene–environmental interactions in non-communicable diseases, including cancers. The participants of KOPS consist of healthy Japanese residents from four areas in the southwestern region of Japan. Kyushu is a region consisting of eight prefectures including Okinawa Prefecture in the southwestern part of Japan (figure 1). Fukuoka Prefecture, where Kasuya Town and Hoshino Village are located, and Nagasaki Prefecture, where Iki City is located, had slightly higher cancer, coronary artery disease (CAD), and stroke mortality rates in 2005 and 2010 than the whole of Japan. Okinawa Prefecture, where Ishigaki City is located, had slightly lower cancer, CHD, and stroke mortality rates in 2005 and 2010 than the whole of Japan8 9 (online supplemental table 2). Additionally, KOPS has provided epidemiological data to the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study, which started in 2005 and aimed to examine gene–environment interactions in non-communicable diseases, especially cancers.10 Both KOPS and the J-MICC Study are supported by a research grant for Scientific Research on Special Priority Areas of Cancer from the Japanese Ministry of Education, Culture, Sports, Science and Technology.11
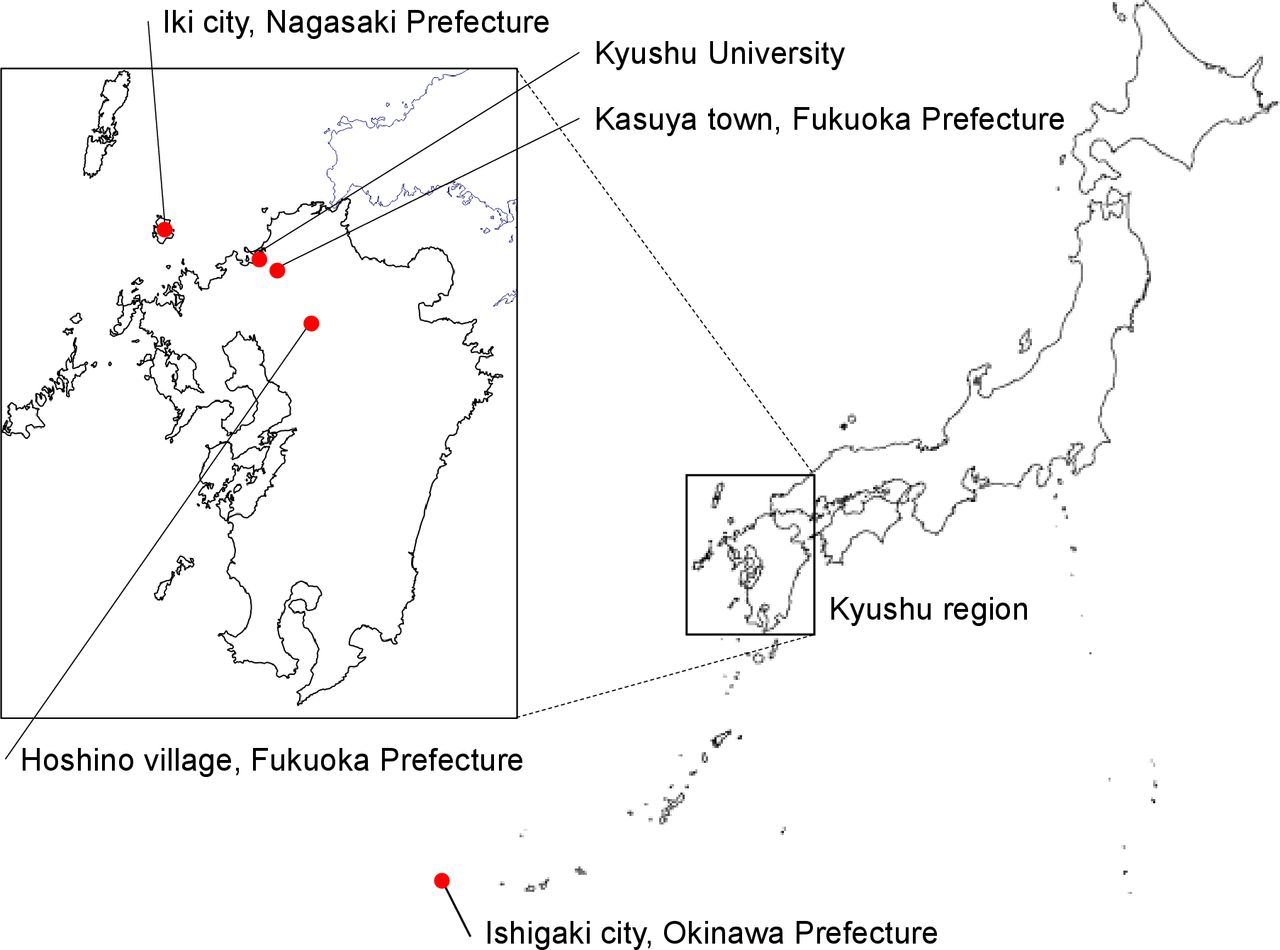
Location of the four study regions of the Kyushu and Okinawa Population Study.
While we have reported several cross-sectional studies,12–15 especially on atherosclerotic diseases, we have not reported details of study design and baseline characteristics of participants. Therefore, this report aims to describe the study design and the baseline profile of the participants.
Cohort description
Study design, inclusion criteria and exclusion criteria
KOPS is a community-based prospective cohort study that aims to investigate the gene–environment interactions in non-communicable diseases and consists of participants from four areas in the southwestern region of Japan. They are Ishigaki City of Okinawa Prefecture, Iki City of Nagasaki Prefecture, and Hoshino Village and Kasuya Town of Fukuoka Prefecture (figure 1). Inclusion criteria were persons aged 30 years old or over who were registered in the Basic Resident Register of the above four municipalities at the time of enrolment. We did not include persons aged 80 years and older or who did not consent to participate in this study.
Recruitment
In this study, we recruited potential participants at the sites of municipality-based health check-ups in Ishigaki City, Iki City, Hoshino Village and Kasuya Town, between 2004 and 2007 (wave 1), and between 2009 and 2012 (wave 2). Some of the participants in wave 2 are also participants in wave 1. Figure 2 shows a flow chart of recruitment and response rates in those four areas. Researchers explained the overview and study contents of KOPS to the participants at the sites of health check-ups. The briefing was performed by staff doctors of the Department of General Internal Medicine of Kyushu University Hospital, who had been trained regarding the study protocol and the medical procedures. Informed consent was obtained with individual face-to-face interviews by the researchers, and each participant checked all the items on the written form and signed it. A total of 17 077 participants were enrolled in this study, comprising 10 697 participants of wave 1 (median age was 61 years and total response rate was 66.4%) and 6380 participants of wave 2 (median age was 61 years and total response rate was 64.1%). Among them, 3006 individuals participated in both wave 1 and wave 2 surveys.

{kind=link}
{kind=link}
Flow chart showing details of recruitment and assessment. For wave 1, we recruited participants at the health check-up sites in Ishigaki City between 2004 and 2007, Iki City in 2005, Hoshino Village in 2006 and Kasuya Town in 2007. For wave 2, we recruited participants at the health check-up sites in Ishigaki City in 2009, Iki City in 2010, Hoshino Village in 2011 and Kasuya Town in 2012. Among 6380 participants of wave 2, 3006 participated in the wave 1 study (duplicate participants).
Patient and public involvement
Participants were not involved in setting the research question or the outcome measures. However, participants and their families played an important role in dissemination of the baseline information, which helped to motivate community involvement during and beyond the study.
Anthropometric measurements
Anthropometric measurements were performed wearing indoor clothing and without shoes. Body mass index was calculated as weight (kg) divided by height (m) squared. Waist circumference was measured at a level midway between the lowest rib and the iliac crest in a standing position. Systolic and diastolic blood pressures were measured on the right arm in the sitting position with an automated sphygmomanometer (HEM-780, Omron Healthcare, Kyoto, Japan) after a 5-minute rest.
Questionnaires
All participants were interviewed about their lifestyle, medical history, including medication, and dietary patterns, using a self-administered questionnaire. A detailed list of items included in the questionnaire is shown in table 1. Regarding dietary pattern, we used a Food Frequency Questionnaire (FFQ) consisted of 46 items for dietary studies of the middle-aged and elderly general Japanese population. The items included in the FFQ are shown in table 2. We also obtained food consumption frequencies classified into eight categories: never or seldom, 1–3 times per month, 1–2 times per week, 3–4 times per week, 5–6 times per week, once a day, twice a day, and three or more times a day. Detailed baseline information of participants of wave 1 and 2 is shown in tables 3 and 4.
Details of the self-administered questionnaire for KOPS
Items included in the Food Frequency Questionnaire for KOPS
Baseline characteristics of KOPS wave 1 participants*
Baseline characteristics of KOPS wave 2 participants*
Laboratory measurements
In this study, the blood collection amount was 15 mL, consisted of 7 mL in a blood tube for serum, 6 mL in an EDTA2Na blood tube for plasma and buffy coat, and 2 mL in an EDTA2Na blood tube for complete blood count, blood sugar, and glycated haemoglobin (HbA1c). All blood samples were collected at least 8 hours after overnight fasting, and aliquots of whole blood and fresh serum and plasma samples from each participant were immediately separated. Data of urine tests were obtained from each municipality. Details of common blood and urine tests in this study are provided in table 5.
Biological tests in KOPS
Follow-up survey
The endpoints of this study are death from any cause and incidence of cancer, cerebrovascular disease and CHD. Participants will be followed until 2025. To ascertain follow-up information, we perform the following ways: (1) interviews at the site of the municipality-based annual health check-up; (2) mail survey; (3) medical record review; (4) public statistics.
Interviews at the annual health check-up site have been performed every 5 years since the start of this survey in each area. Mail surveys have been conducted for participants who did not come to the health check-up site. The questionnaire used in the interview and mail surveys is the same. The questionnaire asks whether or not a participant has had cancer, CHD or cerebrovascular disease. If a participant suffered from those diseases, the information on onset and hospital will be asked. When information on the incidence of the endpoint is obtained, a medical record review is conducted, with permission from participants. The address of participants is confirmed using the Basic Resident Register of each municipality. When we obtain this information, we comply with the Basic Resident Registration Act. If a participant died, we confirm the death using the Basic Resident Register. The cause of death is confirmed by viewing the death certificates. When a participant moves out of the study area, the follow-up of the participant is censored.
Findings to date
As KOPS was established to investigate the gene–environmental interactions in non-communicable diseases, we have focused on either risk factors or confounding factors for those diseases. Recent publications of this cohort have reported the clinical utility of the newly developed biomarkers for non-communicable diseases such as impaired glucose tolerance, dyslipidaemia, atherosclerosis and the impact of lifestyle on medications. Details of the findings are shown as follows:
Newly developed markers for impaired glucose tolerance
Glycated albumin and urinary myo-inositol are newly developed markers for early detection of glucose intolerance. We have shown that elevated glycated albumin levels could predict diabetes based on both fasting plasma glucose and HbA1c levels,12 and the results of oral glucose tolerance test13 in cross-sectional studies. These studies demonstrated that the optimal threshold value of glycated albumin for the diagnosis of diabetes was approximately 15.5%.12 13
We have also shown the utility of urinary myo-inositol as a screening test of glucose intolerance.16 The urinary myo-inositol test is non-invasive to examinees because levels of urinary myo-inositol can be measured in urine. Receiver operating characteristic analysis showed that urinary myo-inositol levels 2 hours after glucose ingestion demonstrated a higher area under the curve than HbA1c (0.891 vs 0.785, respectively, p=0.06).16 It should be noted that these studies were cross-sectional designs. Further prospective studies will be necessary to prove whether these tests can predict the risk of diabetic complications.
Specialised lipid markers and atherosclerosis
Analyses of lipoprotein subclasses are clinically essential to manage cardiovascular disease risk, and small dense low-density lipoprotein cholesterol (small dense LDL-C) is considered the most atherogenic lipoprotein.17 18 We have assessed specialised lipoproteins, including small dense LDL-C, regarding carotid intima-media thickness (cIMT) progression over 5 years.15 Our results demonstrated that elevated small dense LDL-C had a significant positive association with cIMT progression even in subjects with LDL-C<100 mg/dL, who were considered at low cardiovascular disease risk.15 Moreover, other studies have shown that elevated small dense LDL-C is a strong risk factor for cardiovascular disease events.19 20 Further studies are necessary to determine which lipoproteins are most atherogenic.
Ethnic differences in impaired glucose tolerance and cardiovascular diseases
To investigate ethnic differences in impaired glucose tolerance and cardiovascular diseases, we have conducted an international collaborative study with Framingham Offspring Study.21 22 Fasting insulin levels in Japanese men (4.6 μIU/mL) and women (4.3 μIU/mL) were about 50% lower (both p<0.001) than those in Framingham men (10.8 μIU/mL) and women (9.9 μIU/mL). Although fasting insulin and homeostasis model assessment of insulin resistance (HOMA-IR) values significantly increased as glucose intolerance worsened among the Framingham population, there were no differences in those values between the impaired fasting glucose and the diabetic groups among the Japanese population. Our results indicated that insulin deficiency might play a significant role in causing impaired glucose tolerance in Japanese, while a significant factor for Caucasians may be insulin resistance.21
We have also compared the prevalence of cardiovascular diseases and risk factors between Japanese and Framingham populations. The cardiovascular disease prevalence rates were more than sixfold higher in Framingham men (13.2%) and women (8.6%) than Japanese men (2.1%) and women (1.0%) (all p<0.001); however, standard cardiovascular disease risk factors could not account for the ethnic difference.22 An approximately 2.5-fold greater level of insulin resistance (HOMA-IR) in the Framingham population could have been a significant factor accounting for the ethnic difference in cardiovascular disease risk.22 It should be noted that these studies were cross-sectional, and other factors such as dietary patterns were not included; thus, further prospective studies are necessary to elucidate the ethnic difference in non-communicable diseases.
Helicobacter pylori eradication therapy and dietary pattern
Helicobacter pylori (H. pylori) infection is a known risk factor for gastric cancer, and the eradication of H. pylori could prevent the development of gastric cancer.23 We investigated the influence of food and nutrient intake on H. pylori eradication therapy among 352 Japanese subjects.14 The success rate of H. pylori eradication therapy was 60.2% (212 of 352), and we found that a higher intake of cholesterol, n-3 highly unsaturated fatty acids and vitamin D were associated with a greater failure rate of H. pylori eradication therapy (all p for trend <0.05). When the subjects divided were into three groups according to egg consumption frequency, the group with the highest egg consumption (more than 0.9/day) showed a significantly lower success rate than the group with the lowest egg consumption (less than 0.2/day) (40.5% vs 70.1%, respectively).14 Our results indicated that dietary pattern change could improve the success rate of H. pylori eradication therapy. Further intervention trials are necessary to find dietary patterns or nutrients which could improve the success rate of H. pylori eradication therapy.
Genome-wide association study
We have reported the results of several gene–environmental interaction analyses. We analysed the correlation between single nucleotide polymorphisms (SNPs) and other factors contributing to the spontaneous elimination of the hepatitis C virus in residents of a community with a high prevalence of hepatitis C infection.24 Women showed a higher spontaneous elimination rate of the hepatitis C virus than men (30.7% vs 17.3%, respectively, p=0.06). In the favourable interleukin 28B (IL28B) SNPs (TT) group, women showed a statistically significantly higher spontaneous elimination rate than men (39.0% vs 20.9%, respectively, p=0.02). On the other hand, in the unfavourable IL28B SNPs (non-TT) group, there was no sex difference in spontaneous elimination rate (4.2% vs 5.6%, respectively, p=0.5). Our results provide an example of the synergistic effect of SNPs and other factors.24
As a genome-wide association study (GWAS), we conducted a GWAS analysis to investigate the interactions between high-density lipoprotein cholesterol (HDL-C)-related SNPs and physical activity on HDL-C. In this sex-stratified GWAS analysis, we found a significant interaction of ABCA1 rs1883025 with physical activity only in men.7 However, this beneficial interaction was reduced in men with lower physical activity levels. Our results may contribute to developing individualised physical exercise programmes based on the individual genotypes of HDL-C-related SNPs. We also conducted another GWAS analysis for CAD in the Japanese population, a large-scale GWAS of 168 228 individuals of Japanese ancestry (25 892 cases and 142 336 controls) with BioBank Japan.25 We detected eight new susceptibility loci and Japanese-specific rare variants contributing to disease severity and increased cardiovascular mortality. Moreover, a trans-ancestry meta-analysis discovered 35 additional new loci. Based on our results, we derived a polygenic risk score for CAD, superior to previous ones.
Strengths and limitations
The main strengths of this study are its large-scale, population-based prospective cohort design and the extensive data collected on lifestyle habits such as eating and exercise habits, psychological factors and genomic information as risk factors of non-communicable diseases including cancer. Such information will allow adjustment of various confounders when elucidating the complex relationships of factors and identifying modifiable risk factors of non-communicable diseases. In addition, including relatively young subjects in this study population allows investigators to identify critical modifiable risk factors. Our central clinical laboratory conducted all laboratory analyses, and thereby interlaboratory variation could be eliminated. Another strength of this study is the high follow-up rate using the Basic Resident Register of each municipality and viewing the death certificates. Moreover, the stored biological samples are an asset of this study, allowing the measurement of biomarkers developed later in this population.
Several limitations should be noted. First, virtually all of the participants are ethnically Japanese. Thus, our findings may not apply to other ethnic groups. Second, the participants were recruited at sites of health check-up, suggesting there are a healthy volunteer effect and a selection bias in this cohort. For example, the current smoking rate of 15.1% was slightly lower than 19.5% in Japan’s 2010 National Health and Nutrition Survey. Therefore, caution should be exercised when generalising the findings of this study.
Collaboration
Collaboration with researchers is highly welcome. Please contact the corresponding author (HI) with any inquiries. An access committee will be set up to review data access and collaboration requests. Details will be made available on the study website once the access procedures have been decided.
Data availability statement
No data are available. No additional data available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Kyushu University Hospital Ethics Committee (the latest approval no: 590-02) and carried out in accordance with the principles of the Declaration of Helsinki as revised in 2008. All participants provided written informed consent after thorough explanation of the outline and objectives of this study.
Acknowledgments
The authors thank Drs Mosaburo Kainuma, Hiroaki Taniai, Hachiro Onishi, Kunimitsu Eiraku, Tsunehisa Koga, Takeshi Ihara, Takeo Hayashi, Fujiko Kaseida-Mitsumoto, Kazuya Ura and Ayaka Komori for their efforts in collecting data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The conception and design of the study were carried out by HI, NF and JH. The acquisition of data was done by all authors, mainly by HI, RN and MU. The measurement was done by HI, NF, KY, YM, AO, SY, SH, KTa, EO, KTo, MM and JH. The data were analysed by HI and RN, and interpreted by all coauthors. All authors, especially NS, contributed to the drafting of the paper and its revision. All authors are responsible for the intellectual content and the final approval of the version to be published. HI is the guarantor of this study.
Funding This study was supported by Grants-in-Aid for Scientific Research for Priority Areas of Cancer (No. 17015018) and Innovative Areas (No. 221S0001) and by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant (No. 16H06277 (CoBiA)) from the Japanese Ministry of Education, Culture, Sports, Science and Technology.
Map disclaimer The depiction of boundaries on the map(s) in this article does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.