Article Text

Abstract
In the UK, over 20% of patients leaving hospital after a stroke will be severely disabled. Despite this, limited clinical guidance is available to teams tasked with providing support for this complex population at home. Additionally, many areas across the UK are not commissioned to treat this patient cohort, leaving them with no specialist support on discharge.
Objectives To establish core components of home-based rehabilitation for survivors of stroke with severe disability, based on expert panel consensus.
Setting Virtual nominal group technique (vNGT) across the UK.
Participants Experts in the field of stroke rehabilitation (n=14) including researchers, clinicians and those with lived experience.
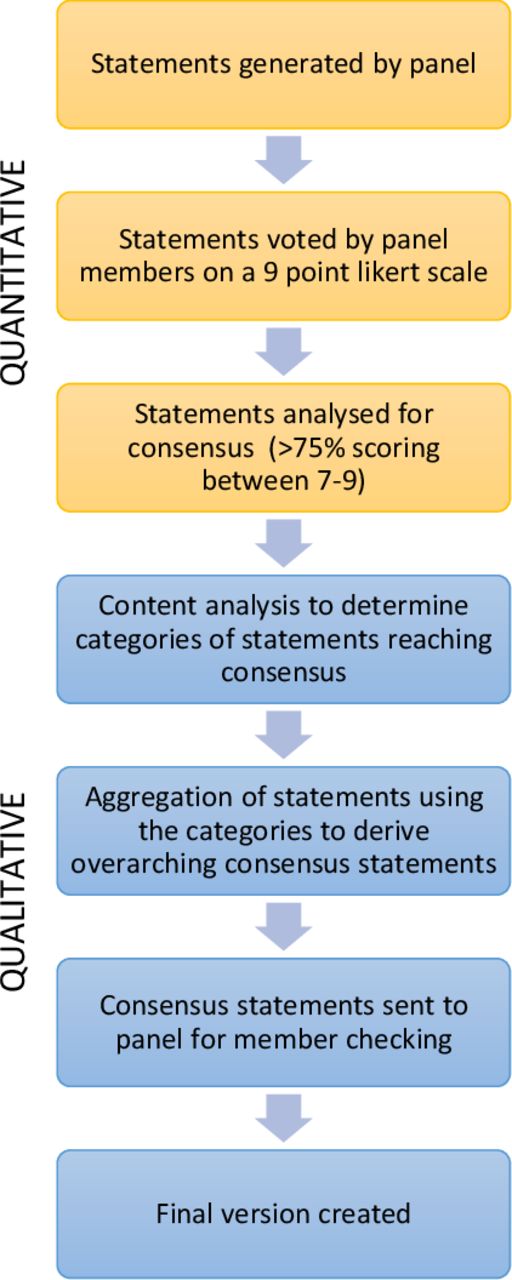
Methods Two vNGT were completed using a freely available online platform, Microsoft Teams. The technique’s five stages were completed virtually; introduction, silent idea generation, round robin, clarifications and scoring. Statements were analysed for consensus, those achieving consensus underwent content analysis to form rich overarching consensus statements.
Results A combined total of 421 statements achieved positive consensus (>75% in agreement), which formed 11 overarching consensus statements. These outline key components of home-based rehabilitation for survivors of stroke with severe disability including the structure and members of the team, as well as the skills and knowledge required.
Conclusion The consensus statements highlight the complexity of managing patients with severe stroke disability following discharge from hospital. This study has the potential to support the provision of services for this patient group, providing a benchmark for commissioners and clinicians as well as setting expectations for stroke survivors and their carers. What remains unknown is how many services currently offer this service to patients with severe disability.
- stroke
- rehabilitation medicine
- primary care
Data availability statement
Data are available on reasonable request. Full content analysis categories available on request to lead author, Rebecca.Fisher@nottingham.ac.uk.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to determine the key components of home-based rehabilitation for survivors of stroke with severe disability.
Participating panelists represented the multidisciplinary team with highly experienced experts, both clinically and academic.
Lay expert input in the round-robin stage, giving the opportunities for lived experience to be represented.
A limitation of nominal group technique is the reliance upon small numbers, however, there was substantial convergence between the two panels, suggesting replicability amongst differing panels.
Introduction
Stroke remains the leading cause of disability in the UK.1 2 Although the establishment of organised stroke units and recent medical interventions (eg, thrombolysis and thrombectomy) have reduced mortality rates, stroke survivors can be left with a number of impairments. These can affect motor, sensory, vision, language and cognition function, therefore, support for recovery to promote quality of life beyond survival also needs to be considered.3 4 Comprehensive guidance exists for the rehabilitation of the stroke population in the community, however, the studies on which recommendations were based involve more abled stroke survivors, who meet the criteria for early support discharge (ESD).5–7 There is a lack of evidence for more severely disabled stroke survivors, who are ineligible for these services, leading to substantial disparities in provision across the UK.5 8
Over 20% of patients were discharged from hospitals in the UK last year with severe disability, equating to approximately 20 000 lives irrevocably changed.8 9 These individuals are commonly unable to stand without assistance and may have additional cognitive and communicative impairments combined with any pre-existing comorbidities, leading to a significant loss of independence.10 While defining severity of stroke and disability can be complex, the modified Rankin scale (a score of 4 or 5) is an established measure used in research and practice and it was these criteria that were used to define the population of focus in the current study.11
Within the community setting this population often have a complex presentation with high rates of readmission and secondary complications leading to challenges with their management.12 Previous research within the severely disabled stroke population has suggested that within the first 12 months following discharge, as many as 73% of stroke survivors with severe disability will experience a fall, 60% contractures and 55% pain.13 Rigby et al14 also found a significant correlation between disability severity and carer burden, which is attributed to serious health consequences for both carer and stroke survivor.14 An eightfold increase in rates of institutionalisation following hospital admission compared with their less severe counterparts has also been reported.15
Rehabilitation in the community setting is a complex intervention, and as such, difficult to evaluate in order to generate robust recommendations. This is made more difficult due to the varied needs of such a heterogeneous population.16 A recent systematic review of rehabilitation interventions for severely disabled stroke survivors in the hospital setting concluded there to be a paucity of high-quality research. However, much less research exists for this population in the community setting with authors again citing challenges associated with the population’s heterogeneity.17 A large phase III randomised controlled study reported neutral results when investigating the effects of a 3-month occupational therapy (OT) intervention in care homes.18 The study alluded to challenges in engaging in therapy for individuals with such high levels of disability.
Guideline development is reliant on high-quality evidence on which to base recommendations.19 Where gaps or poor evidence exist, structured consensus techniques using a panel of ‘experts’ has been advocated by the National Institute for Health and Care Excellence with the two most common being the nominal group technique (NGT) and Delphi method.19 It is argued that the output of these methods has the potential to provide more in-depth and nuanced guidance which has greater utility in practice.19 Previous research has achieved consensus on the core components of ESD and community stroke rehabilitation services for less disabled stroke survivors.6 20 Improving stroke care in the community setting is a national priority, it is therefore paramount that guidance is available to inform provision of services for this so far neglected population group.21 22
This study is the first to determine expert consensus regarding key components of home-based rehabilitation for survivors of stroke with severe disability. The output of this consensus activity aims to support the provision of services for this population, informing commissioners and clinicians as well as setting expectations for patients and their carers. Therefore, the aim of this study was to establish the core components of community stroke rehabilitation delivered within the UK National Health Service (NHS) for survivors of stroke with severe disability, based on expert panel consensus.
Methods
Design
The virtual NGT (vNGT) was used. This technique was specifically chosen over the Delphi technique due to its superior ability to inform areas where there is a dearth of pre-existing research.23 Equally, NGT has been reported to create rich data owing to the face-to-face element creating a stimulating and elaborative environment.23 This technique has also be used successfully within a similar population group.24
Participants
Panel members are known leaders in the field of stroke rehabilitation and were purposefully sampled through established clinical and academic networks to gain multidisciplinary representation from clinical, research and lay member groups.25 Among the clinical and academic participants the following criteria were used to ensure sufficient specialism and skills, conforming to the notion of ‘expert’: over 10-years clinical or research experience within stroke rehabilitation with additional experience with the severe stroke population, understanding of the NHS, geographical representation of the UK and stroke multidisciplinary team (MDT) representation as documented in previous research.26 Potential participants were approached via email.
Expertise from those with lived experience was sought from a stroke survivor and a spouse of a stroke survivor who were members of a Stroke Research Partnership group. On request, these participants met researchers prior to the panel meeting and generated a list of ideas associated with the nominal group questions. These were subsequently presented by the facilitator during the round robin phase (stage 3).
Research questions
The panels were asked to provide responses to the following questions:
Question 1: ‘From an organisational perspective, what should a rehabilitation service for survivors with severe stroke disability include in terms of structure, service delivery and outcome measures?’
Question 2: ‘From an intervention perspective, what treatments / techniques should be implemented in order to effectively rehabilitate this cohort of patients?’
Protocol
The NGT protocol used was Potter et al’s27 adaption of the original which included five stages: introduction, silent idea generation, ‘round robin’, clarifications and scoring.28 These were completed on a virtual basis using an online platform (Microsoft Teams) ensuring all methodological standards were maintained.25
As recommended in the literature, prior to the groups convening, preliminary information was sent to all panel members in the form of an e-booklet (online supplemental file 1). This comprised a scoping literature review, patient and carer experiences, a context statement, the vNGT questions and guidance on the process of the vNGT. The scoping literature review explored the evidence surrounding the rehabilitation interventions of severely disabled stroke survivors in the community following discharge from hospital. Papers were reviewed and synthesised by researchers LR and FR-B and presented into a summary table of evidence. Patient and carer experiences were presented as a word cloud which provides a visual representation of the experiences proffered from a Stroke Research Partnership patient and public involvement (PPI) group. The context statement, considered an important component within consensus generation, was produced by the research and collaborator teams, to set the scene from which participants were asked to base their ideas.25 This included a definition of the study population, survivors of stroke with severe disability, defined as a modified Rankin scale of 4 or 5, in the immediate period postdischarge from inpatient rehabilitation.11 The setting was defined as home-based rehabilitation (including nursing and residential settings) within the UK NHS.
Supplemental material
The same vNGT process proceeded as follows for the two panels:
Stage 1. Introduction: An online presentation was completed with panel members, detailing the vNGT process, and restating the context in which to base ideas and the vNGT questions for deliberation. This also provided the opportunity for any questions or clarifications.
Stage 2. Silent idea generation: Panel members were provided approximately 15 min per question (during which participant microphones and video functions were turned off), and facilitators were available via the platform’s chat function to answer any questions. To help organise the ideas generated, a list of domains (table 1) was displayed on screen alongside a 15 min timer. Domains were used to help organise responses during the round robin. These were informed by literature optimising patient follow-up following stroke.29 It was made clear that domains were to be used for organisation of ideas and not intended to restrict responses and panel members were encouraged to respond freely.
Domains used to help organise ideas
Stage 3. Round Robin: With video and microphones enabled, a member of the research team (FR-B) facilitated each panel member to offer a single idea, in turn, in response to question 1. This process continued until all the ideas were exhausted before progressing on to question 2. During this process within panel 1, the facilitator presented the ideas generated previously by the lay experts, in turn with other participants. All ideas were typed by a second researcher (LR) on to a live document, based on the domains shared previously, visible to all members in real-time, through screen sharing.30
Stage 4. Clarification stage: This was facilitated domain by domain and idea by idea and included each participant in turn. The meeting concluded when all panel members were satisfied that there were no outstanding queries.
Stage 5. Individual scoring: Prior to sharing with the panel members, the previously live document was formatted, converting ideas into single statements for participants to rate by FR-B. It was ensured that the manifest content of the participants’ ideas was maintained throughout through utilisation of their original words, these were subsequently checked by LR. An online questionnaire was sent to the participants within 72 hours following the online meeting.31 In line with previous research,25 a 9-point Likert scale was used from not important/do not agree (1) to important/strongly agree (9) for panel members to vote on generated statements.27
Analysis
This process is represented in figure 1, for further details refer to online supplemental file 2.
Supplemental material

{kind=link}
Representation of the analysis process.
Establishing consensus
The scoring responses from the online questionnaire, for participants included in each of the two panels, were exported to Microsoft Excel to analyse for consensus. The level of agreement was set as 75% of all participants within the set ranges, 1–3, 4–6 and 7–9 not important, equivocal and important, respectively.25 In the case of strong disagreement, defined as one panel member scoring 1 and another 9, outliers were removed, and the remainder reviewed for consensus.25 The median and interquartile range for each individual statement and all statements which reached consensus were calculated to highlight dispersion around the consensus.25
Qualitative content analysis
Content analysis was used to distill the key categories from each panel to review commonalities and discordance between ideas generated by the two panels and to determine the salient core categories32 (online supplemental file 3). This started with the familiarisation of the statements which reached consensus, followed by the primary coding (by researcher FR-B) and secondary coding (by researchers FR-B and LR) using tree nodes (parent and child) in NVivo V.12 pro.33 Both coders are clinical academic physiotherapists with a minimum of 8 years clinical experience working across the stroke pathway, including community rehabilitation. A combination of inductive and deductive coding was used, the deductive component resulting from the use of the domains (table 1). This initial secondary coding framework was presented to the wider research team for review. Following feedback, the initial secondary coding went through an iterative process of revision and reorganisation.34 The second-order category codes were used to create a framework for aggregating the single statements (from each of the two panels) into larger overarching consensus statements (generated across both panels).
Supplemental material
Individual statements associated with these categories were aggregated by a single researcher (LR) before iterative cycles of review by both researchers (LR and FR-B). Reorganisation of consensus statements occurred between the domains of question 1 and 2 to reduce repetition and aid clarity for the reader. No differential weighting was given to individual panel members.25 Decisions were made to exclude any statements that fell outside the scope of the original question and condensed where the level of detail was deemed too great to aggregate.
Once finalised, the overarching consensus statements were the final summary of the views of both panels and were returned to the panel members for member-checking. This ensured the statements reflected the raw data, this included minor phrasing and ordering, no additions were made to the manifest content.35
Patient and public involvement
The Nottingham Stroke Research Partnership PPI group were involved in the design and conduct of this research and have been instrumental in the agreement of adaptions as a result of the COVID-19 pandemic. This included contributing to the e-booklet for the panel members. The lay members participated in the idea generation stage of the nominal group, providing a rich lived-experience.
Findings
Participant characteristics
Twelve clinicians and academics confirmed they satisfied the inclusion criteria and consented to participate in a virtual nominal group. In total, two nominal groups were completed, each consisting of six synchronous expert panel members, with additional non-synchronous input from two lay members during panel 1. A range of disciplines were recruited, included physiotherapists (n=3), occupational therapists (n=3), speech and language therapist (n=1), nurses (n=2), physician (n=1), psychologist (n=1) and rehabilitation assistant (n=1).
Although efforts were made to balance the panels, ultimately there were differences based on individual availabilities (table 2).
Characteristics of members in each panel
Data were collected on two separate days, approximately 1 month apart, with each session lasting between 3 and 3.5 hours.
Consensus
A total of 492 statements were generated from ideas presented in the round robin stage (n=196 and n=296 panels 1 and 2, respectively), with 421 statements (n=183 and n=238) reaching consensus (>75% agreement). The overall score of those reaching consensus was median 9 and IRQ 1, for both panels. Ideas from panel 1 generated fewer statements (196 vs 296, panels 1 and 2, respectively), however, agreement was greater with fewer statements lost to non-consensus (7% vs 20%) as well as fewer instances of disagreement compared with the second group (2% vs 8%).
Qualitative content analysis
Two overarching categories were distilled from ideas and statements generated in both panels: organisation and intervention (table 3). These corresponded with the questions posed in the nominal group session, the former focusing on the components of the service and the latter with the content delivered. Under the first-order category of organisation 8 second-order categories were identified, 7 of which were the same across the two panels, with actively engaged in research only generated in panel 1. Similarly, under the first order category of intervention there were five common second order categories, with only evidence-based practice unique to the first panel group. While there was considerable overlap in content, differences between ideas and then statements generated between the two panels were also anticipated due to differences in group composition. The areas of convergence were summarised in the form of the consensus statements (table 4). While there were few areas of disagreement, there were areas of divergence of focus and these will now be discussed in further detail.
Categories determined during content analysis of ideas and generated statements
The core components for the organisation of home-based rehabilitation for survivors of stroke with severe disability
Areas of divergence
The importance of a seamless transition between inpatient and community stroke services was highlighted by both panels. Panel 2 went a step further, raising the concept of prehospital discharge involvement, ensuring the team are not only operational prior to discharge but actively inputting into discharge communication and decision making.
There should be a discharge planning meeting with the community team, ward staff and family prior to discharge. Panel 2
Panel 1 raised the notion of ‘patient-centred rehabilitation’, suggesting that all aspects of the service and intervention should be related to the needs of that individual.
Therapist should think more ‘patient-need’ orientated, being creative in their response to what they need. Panel 1
Despite the focus on close working with patients, panel 1 did not specifically mention therapeutic relationships between the patient or carer and the rehabilitation team. In contrast, panel 2 emphasised ‘The service should create and provide a long-term relationship with family members.’ acknowledging the long-term nature of their involvement.
When discussing communication between teams and patients, Panel 1 placed a greater emphasis on cross organisational elements, including patient held records and the use of a coordinated electronic base system.
Interestingly, neither research nor evidence-based practice were mentioned by panel 2, which included more academics. These areas reached consensus within panel 1, highlighting the importance of research in practice and suggesting that professions should challenge those who do not follow evidence-based practice.
It is important to create and embed research into daily clinical practice Panel 1
Areas of discordance
The service structure was a dominant second order category within both panels, however, there was some discordance. Panel 2 suggested:
The team should form part of an integrated specialist stroke service delivered by the same team that deliver Early Supported Discharge. Panel 2
Conversely, panel 1 suggests there should not be a distinction between the two, instead opening up the Early Supported Discharge service to all stroke patients.
Early supported discharge teams should be available consistently across the country for all severe stroke, not limited to more able stroke survivors. Panel 1
The topic of inputting into national audits, in this case the Sentinel Stroke National Audit Programme (SSNAP) provoked strong responses from panel 1 reporting they felt ‘SSNAP currently doesn’t reflect community or [the] longer term aspect of stroke recovery’. In contrast, panel 2 emphasised the importance of contributing to the audit. Both panels made suggestions for the collection of additional metrics to demonstrate functional change in the population and service delivery, such as social care requirements (panel 1), unmet needs, hospital readmission, 90-day mortality, care home admission and return to home incidences (panel 2).
An additional point concerned 7-day working, with both panels agreeing that this should be in place, yet disagreement around who should be providing this.
Support workers should be used to provide personalised care and offer weekend input Panel 1
The team should have the ability to provide a seven day service if appropriate and acceptable to the stroke survivor and family. Panel 2
The panels adopted divergent approaches, with Panel 2 taking a more prescriptive approach than panel 1 who suggested a more needs-led approach.
The patient should have a post discharge visit within 1 week to assess needs Panel 2
Services should provide flexibility of input intensity and dose related to goal of task for example, time to settle once home, starting at specific point appropriate to their needs. Panel 1
Consensus statements
Eleven overarching consensus statements were formed using the second-order categories headings. Areas of divergence or discordance were resolved by the research team, referring to raw data where possible. These were then sent out to the panel for member-checking, with minor phrasing and ordering adaptations only, no changes were made to the manifest content. This resulted in the final version of consensus statements presented in table 4, a summarised infographic can be found in online supplemental file 4.
Supplemental material
Discussion
This study generated consensus statements defining the key components of home-based rehabilitation for survivors of stroke with severe disability. This is the first step in providing much needed guidance to support the provision of services, informing commissioners and clinicians as well as setting expectations for stroke survivors and their carers. A total of 421 statements derived from the vNGT process reached consensus identifying a breath of rehabilitation needs for this population, from restorative rehabilitation to end-of-life care and carer burden, with high levels of convergence between the two panels. These were distilled into 11 overarching consensus statements, a summarised, succinct format, which aims to optimise uptake and use in practice.
This study complements previous research in which consensus statements guiding the delivery of stroke ESD and community stroke rehabilitation, using modified Delphi approaches were generated.6 20 The current consensus activity focused on provision of care to stroke survivors with severe disability, and choice of the NGT was based on the lack of evidence for this patient population. NGT has been widely used within healthcare for the generation of priorities and guidelines due to its highly structured processes, especially when there is a dearth of evidence within the field.25
The findings from this study are aligned to, and build on, recommendations made in previous consensus activities.6 20 24 These include an emphasis on the need for a comprehensive MDT as well as predischarge involvement, weekly meetings6 and the need for an integrated stroke care pathway, highlighting principles which are applicable for stroke services for any survivor of stroke. Both panels agreed on the need for rehabilitation delivery alongside ESD, however, with slight differences in opinion. One panel suggested expansion of current ESD criteria whereas the other panel suggested integration (offering ESD alongside community stroke rehabilitation) so that the service ‘offers stroke rehabilitation at a range of intensities.’ This aligns with the recommendation by the National Integrated Community Stroke Service model detailed in the current National Stroke Service Model.22
Sackley and Pound24 previously used NGT within care homes for a similar stroke patient population and with a focus on transfer of care on hospital discharge. In the current community focused study, some similar themes were evident such as: the importance of cross team communication, equipment provision, written information and education of staff.24 Community stroke teams have the potential to support the transfer of care between acute hospitals and care homes, as reflected by the consensus statements generated in this study regarding both in-reaching into acute hospitals and working collaboratively with care home staff as well as supporting family and carers within their homes.
Severely disabled stroke survivors are more likely to be discharged to care homes compared with less disabled survivors. Dutta et al9 showed that 37.3% and 55.8% of stroke patients in the categories of modified Rankin scales of 4 and 5, respectively, were discharged to care homes compared with only 7.9% of patients with a modified Rankin scale of 3.9 Only in recent years have clinical guidelines recommended that those resident in nursing homes should have access to specialist stroke services, however, these guidelines fall short of detailing the content of these services.7 The lack of specialist stroke rehabilitation provided to survivors of stroke within these facilities has been highlighted; being classified as a ‘resident’ of long-term care facilities was associated with reduced access to rehabilitation.36 A randomised controlled trial by Sackley et al18 investigating the impact of a 3-month OT intervention on care home residents following stroke reported neutral results. However, their intervention, while individually customised, ‘aimed to augment or maintain functional capacity in personal activities of daily living’ with the primary outcome being the functional independence measure, the Barthel Index. The current consensus statements highlight that, for survivors of stroke with severe disability, interventions should be tailored to a variety of aims such as the reduction of secondary complications or access to leisure activities, interventions focusing on these may have seen a different outcome, however, to the authors knowledge no interventional research has been completed in these areas.
This study also emphasises that location should not be an exclusion criterion for rehabilitation in this population. The consensus statements provide important guidance for care provided to stroke patients in nursing or residential care homes (as well as those in their own home), focusing on the training needs of the staff to ensure safety yet equally not neglecting their quality of life, with the enablement of leisure activities.
Outside of the care home environment there is also a dearth of evidence. McGlinchey et al37 recently reported a survey to describe the current practice of therapists with survivors of stroke with severe disability. The most frequently reported interventions, for both physiotherapists and OT’s, were stroke survivor positioning and training of carers.37 The authors highlighted the lack of trials researching these areas, arguing that existing research trials do not reflect actual clinical practice. Their findings closely reflects the findings from this study which indicates the need for carer training and education, prevention of secondary complications and posture and seating interventions.
The training of carers by community stroke teams has been proposed previously.20 However, these consensus statements emphasise the importance of carers and go as far as to suggest that a goal of intervention, and eligibility for the service, could be to reduce carer burden. This reflects previous literature suggesting severity of functional disability significantly correlates with carer burden.14 A Cochrane review conducted in 2011 concluded there was insufficient evidence of the impact of training interventions for carers.38 However, none of the included papers involved a face-to-face intervention in the home setting, led by therapists. Kalra et al39 demonstrated positive results with an inpatient training package for carers, however when replicated in a multicentre study no differences between the control and intervention were found. The authors concluded the intervention may be best delivered by the community team, in a patient’s own home, which echo the findings of this study.
The present consensus statements are in agreement with the wider available literature, however, they succinctly offer guidance for healthcare professionals, commissioners and patients regarding the specialist needs of this under-represented patient group.
Strengths and limitations
The use of the adapted vNGT within this study, provided many benefits while ensuring methodological rigour.40 41 These benefits included being able to include panel members from geographically distant locations, ensuring a breath of experience without the burden of travel or additional cost implications.42 Equally, Kulczycki and Shewchuk41 demonstrated high levels of acceptability among their panel members.
The strengths of this study include the use of a highly specialist panel, with collaborative working between different MDT members as well as input from those with lived experience.43 Highly experienced experts within stroke rehabilitation, from across the country were involved in this study, both nationally and internationally renowned. It is suggested that this can influence the implementation by maximising the credibility and the validity of the results.25 While we regard the inclusion of expert input from lay members as a strength of this study, involved with the idea generation, they did not participate in the scoring stage, at their request.
A long-standing debate in the use of the NGT is a reliance on the views of limited panel members.44 While the selected panel has been highlighted as one of the strengths of the study, there is a potential that different panel members (representing different disciplines) may have yielded different conclusions. The use of two separate panels within this study has provided an insight into the replicability of these views, with high levels of replication and few incidences of disagreement among n=421 statements. This was achieved despite the significant difference in casemix between the two panels. While this does not confirm the reliability of the results, this helps to strengthen the outputs. Similar to the previous uses of vNGT, the approach was deemed successful.40 41 An evaluation was completed seeking feedback from the panel members; however, results are to be published separately. In summary, the video conferencing platform enabled the face-to-face discussion synonymous with NGT. Using previous recommendations from virtual focus group literature and optimal nominal group panel sizes, this study purposely limited the groups (n=6) in order to support real-time discussion and generate sufficiently rich data.25 45 This meant the need for two separate panels with the subsequent triangulation of their data, however, it was felt that this positively aided scheduling.
Conclusion
This study is the first to determine expert consensus regarding key components of home-based rehabilitation for survivors of stroke with severe disability. Globally, an increasing and ageing population coupled with a trend in reducing mortality rates, has led to increasing numbers with long-term disability following stroke.46 The overarching consensus statements highlight the complexity of effectively managing patients with severe stroke disability following discharge from hospital. This study can be used to support the provision of services for this patient group, providing a benchmark for commissioners and clinicians as well as setting expectations for stroke survivors and their carers.
Data availability statement
Data are available on reasonable request. Full content analysis categories available on request to lead author, Rebecca.Fisher@nottingham.ac.uk.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was granted by the University of Nottingham Faculty of Medicine and Health Sciences Research Ethics Committee, reference 27-0520.
Acknowledgments
The authors wish to thank all the panel members for their time Professor Audrey Bowen, Professor Anne Forster, Jayne Greenwood, Gemma Hayden, Thérèse Lebedis OBE, Dr Angie Logan, Dr Deborah Lowe, Dr Mark McGlinchey, Rachel Sibson, Tracy Walker, Professor Dame Caroline Watkins and Nicola Wyatt. We would also like to thank the Nottingham Stroke Research Partnership Group for their time and guidance, especially CM and PJ.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RJF and LR conceived the presented idea and secured funding. The design was informed collectively by all authors (RJF, LR, FR-B, CL, CS, RS and MW). FR-B and LR completed the data collection and primary analysis. Further analysis was completed in collaboration with CL, CS, RS, MW and RJF with all authors involved in the interpretation of the data. FR-B and LR led in the writing of the manuscript with all authors involved in critical revision of the manuscript and approved the final draft. RJF is guarantor for this work.
Funding This work was supported by NIHR ARC-East Midlands, grant number NIHR200171.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.