Article Text

Abstract
Introduction As people age, they are more likely to experience a decline in their response inhibition ability, which interferes with daily life. Previous studies have shown that exercise intervention can improve the cognitive ability of the elderly, but research on open-skill and closed-skill exercises to improve the response inhibition in this age group is still limited. This study will explore the advantages of long-term intervention of table tennis (open-skill exercise) compared with fit aerobics (closed-skill exercise) on the response inhibitory ability of the elderly.
Methods and analysis A single-blind randomised controlled trial will be conducted. A total of 90 elderly subjects will be recruited and allocated randomly to the following groups: table tennis, fit aerobics and control. The interventions for the table tennis group and the fit aerobics group will be implemented in three 60 min sessions per week for 6 months; the control group will receive no exercise intervention. The primary assessment will be behavioural indicators of response inhibitory ability in the elderly based on the stop signal task. The secondary outcomes will include cognitive ability, mental status and depression in the elderly. Assessments will be conducted at baseline, 3 months, 6 months and 12 months.
Ethics and dissemination This study was approved by the Shanghai University of Sport Research Ethics Committee (102772019RT012) and will provide reference for the advantages of table tennis compared with other types of sports in improving the response inhibitory ability of the elderly. The results of this study will provide a theoretical basis for choosing the best exercise programme to improve the response inhibitory ability of the elderly.
Trial registration number This study has been registered prospectively in the Chinese Clinical Trial Registry (ChiCTR2100043616, 23 February 2021).
- old age psychiatry
- mental health
- biophysics
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Because it is a sports intervention, the safety of the elderly during exercise is worth worrying about.
How to select and control participants in a longitudinal study is one of the difficulties of this project.
The patients will come from one geographic area, which limits the generalisability.
Introduction
Response inhibition ability is a type of cognitive control ability that can achieve behavioural goals by adjusting perception and motor function in the changing environment as well as be used to solve conflicts.1 As people age, they are likely to experience a decline in their response inhibition ability,2–5 which can interfere with daily life and even the ability to live independently. Although some studies have shown that exercise intervention can improve the cognitive ability of the elderly,6 there are few studies on the effect of exercise intervention on reactive inhibition ability. In particular, research on the different types of exercise to improve the response inhibition ability of the elderly is still limited.
Sports can be divided into closed skill activities and open skill activities.7 The operating environment of closed-skill exercises, such as fit aerobics, fitness running, is stable; and the operating state is determined by the operator. In contrast, the operating environment of open-skill exercises, including those involved in the sports of table tennis, basketball, is unstable; and the operation state is determined by external conditions, such as a ball and opponents. In open-skill exercises, the participant must continuously adjust their behaviour to unpredictable stimuli and must invest more cognitive resources in the decision-making process. Previous studies have shown that open-skill exercises require more regulating capacity than closed-skill exercises.8 First, a study comparing the cognitive control of sports involving open-skill exercises with that of closed-skill exercises has revealed that athletes engaging in open-skill exercises have an advantage in cognitive control. It has been demonstrated that intervention with long-term open-skill exercise can improve cognitive function better than closed-skill exercise,7 but whether it can improve response inhibitory ability better is not clear.
As one of the classical paradigms to test response inhibition, the stop signal task (SST) tests the complete suppression of an ongoing action. The SST instructs the participant to perform a response when the go signal appears, but after a few go signals appear, a stop signal will appear at a specific time interval, and the individual will be asked to stop the response as far as possible.9 The strengths of this test are that a stop signal to evoke controlling behaviour is administered after a go signal is used, and the interval between these two signals dynamically changes regularly.10 In addition, the SST is capable of quantising inhibitory control behaviour. However, no response occurs when the participant holds up successfully. The stop signal response time (SSRT) is a more sensitive indicator to evaluate the response inhibitory ability.11 In short, to calculate the SSRT, all go-reactions (ie, go-trials in which the response was missed) are rank-ordered and assigned the maximum response time in order to compensate for the lacking response. Afterwards, the most recent stop signal delay (SSD) is subtracted from the response time corresponding to the stop-signal response percentile. The resulting value is termed the SSRT.12 13 These results can be used as an important index to evaluate the response inhibitory ability.
The proposed randomised clinical trial will examine the effects of table tennis (open-skill exercise) and fit aerobics (closed-skill exercise) on the primary outcome (behavioural task) of response inhibitory ability as well as on the secondary outcomes of cognitive ability, mental status and depression in the elderly. We hypothesised that different types of exercise intervention can affect the response inhibitory ability to varying degrees and that the effect of open-skill exercises is better.
Methods
Study design
This study protocol of a study is designed as a prospective, single-blind randomised controlled trial (RCT). Eligible participants will be randomised into table tennis, fit aerobics, or control groups at a 1:1:1 ratio. The duration of exercise intervention will be 6 months. The cognitive function test (questionnaire and behavioural task) will be conducted before the intervention as well as at 3 months, 6 months and 12 months after the intervention. Participants who meet the criteria will undergo baseline assessments. All evaluations will be done at baseline and immediately after the exercise intervention (see figure 1). We will recruit healthy right-handed elderly participants with normal or corrected-to-normal vision and without a history of neurological diseases in the same way. The study is scheduled to begin in August 2021 and continue until August 2023.
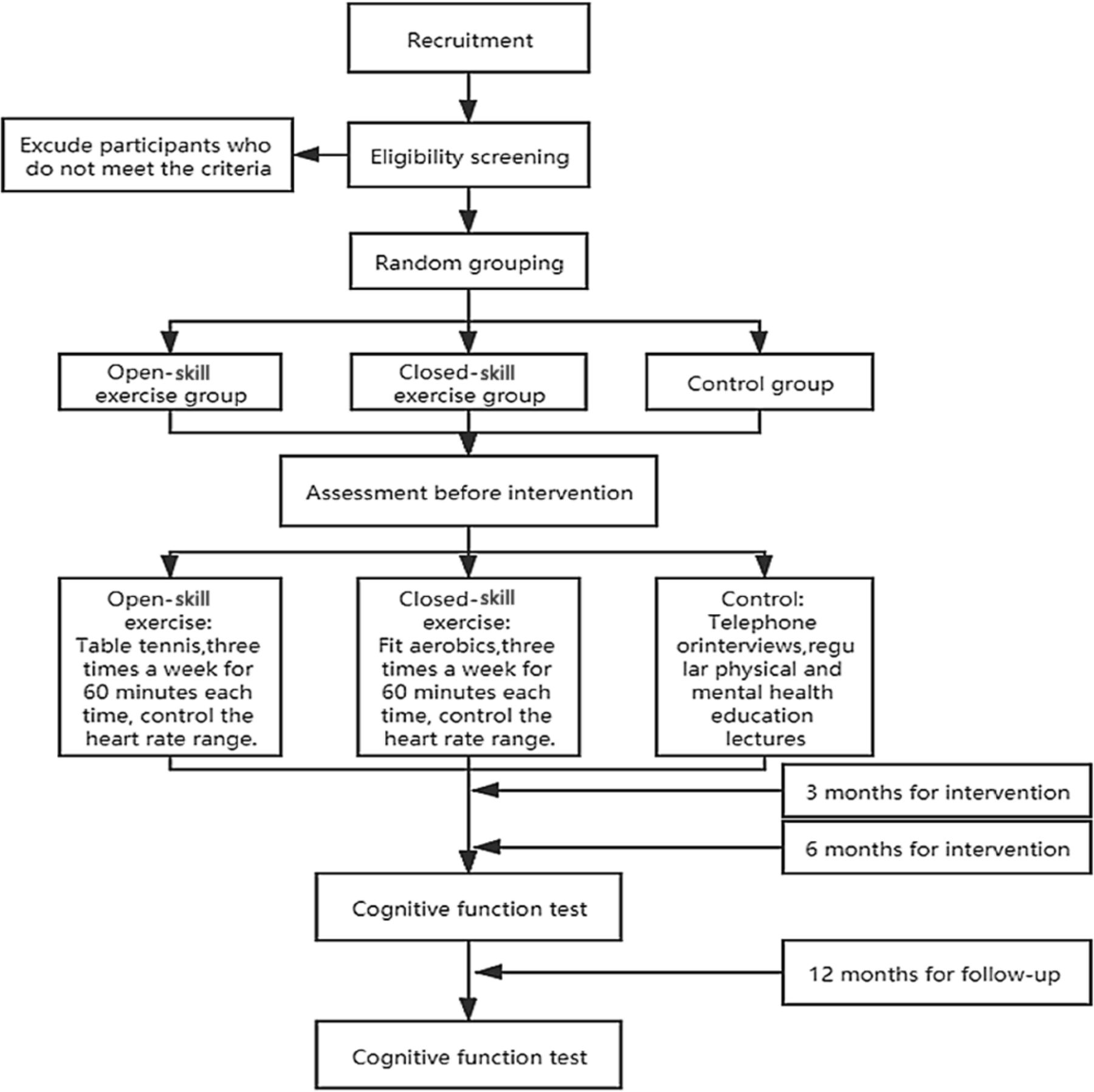
Flow diagram of the study design.
Participants
Any participants with heart disease, neurological disorder, musculoskeletal disorders, and other conditions not suitable for physical activity, contraindications to fMRI or transcranial magnetic stimulation (TMS) will be excluded. In addition, those with a regular exercise routine will be excluded. All participants will be between the ages of 60 and 70 years old and right-handed as assessed by the Edinburgh Handedness Inventory. Moreover, they must have their own residence.
Before and after the intervention, all groups will have their demographics statistically analysed for factors such as health status, physical fitness and cognitive function (table 1). Intergroup differences will be minimised before the intervention.
Demographic and clinical characteristics of the study participants
Sample size
From our previous studies on the modulation of SST performance,14 15 we expected an effect of r=0.4. Together with an α-value of 0.05 and a power of 1 – β=0.9, a sample of at least 72 participants (24/group) was planned to find a similar effect. Calculations were carried out using G*Power, V.3.1,16 with anticipation of a 20% attrition rate. Therefore, we plan to recruit 90 subjects (30/group).
Randomisation
Eligible participants will be randomised into table tennis, fit aerobics or control groups at a 1:1:1 ratio after consenting and baseline assessment. We will use the Excel software to code the subjects in 1–90 according to the recruitment time, and then use the formula '=RAND()' to generate the corresponding random sequence. By sorting the random sequence and then grouping it, 90 subjects will be randomly grouped. The above tasks will be completed by professional computer workers after the participants are recruited. They are double blind with recruitment and grouping.
Exercise intervention
The exercise intervention will last for 6 months. The participants will be divided into three groups: table tennis, fit aerobics and control. The table tennis (open-skill) and fit aerobics (closed-skill) groups will train for 60 min, three times a week. The exercise intensity will be monitored, ensuring that the heart rate remains in the range of 60%–70% of the maximum heart rate (HRMAX=220 – age). During the training period, the exercise intensity will be monitored by the experimenter through real-time heart rate monitoring and the subject’s subjective reaction. The exercise load and heart rate responses of the subjects will be recorded at each training session and adjusted accordingly with an increase of aerobic capacity. All the participants are not used to regular exercise before participating in the experiment. The control group just needs to maintain their old habits, and we will visit the control group regularly to evaluate their physical activity, so as to ensure that their physical activity does not meet the exercise standards. The entire intervention process will be monitored in real time by healthcare professionals. We will have coaches to monitor and record their attendance, and if they are absent, they will supplement the training at other times. Specific intervention methods are shown in table 2.
Exercise intervention TIDieR
SST protocol
The SST was programmed using E-prime V.2, in which the subjects will be asked to press a “←" button or a “→" button according to the left and right arrow directions. In 25% of the trials, the arrow will turn red and a grey triangle will appear; the participants will press the button to stop or give no response. The interval of stimulation will be dynamically adjusted according to the tracking procedure. The task will be divided into four groups of 120 trials each. The task flow is shown in figure 2. The execution go signal reaction time (GoRT), stop response reaction time (SRRT), SSD and SSRT will be investigated. GoRT is how long it takes for the participant to respond after the GO (black arrow) appears. SRRT is the time to respond to the stop signal (arrow turning red) task. SSD is the time between the task stimulus and the stop signal.

Stop signal task flow chart.
The instructions for the experiment will be follows: Welcome to the experiment. First, “+" will appear in the centre of the screen to alert the user to begin the keystroke reaction, and the right index finger should be placed on the “↓" to prepare for the experiment. When the black arrow appears in the centre of the screen, use your right index finger to press the button. When the left arrow appears, use your index finger to press the “←" key on the keyboard. When the right arrow appears, use your index finger to press the “→" key on the keyboard. After each key response, the right index finger should quickly return to the “↓" key to wait for the next response. When the black arrow in the centre of the screen turns red and a small grey triangle appears, please stop the keystroke reaction immediately. When the red arrow appears in the centre of the screen, please do not perform any keystroke reaction. Let’s move on to practice.
Outcomes
Primary outcome
Behavioral task
The task will include randomly interspersed no-go and stop-signal trials, which will enable us to examine both types of inhibition. A total of 480 trials will be performed, including 75% go trials and 25% stop trials. On go trials, the subjects will respond to a left/right black arrow (1000 ms) by pressing the buttons with their right hand. Responses will be made with the index finger (for the left or right arrow). In the stop-signal trials, a response will be initially cued by a left/right black arrow, but the arrow colour will change to red concurrent with a grey triangle after an SSD, and the subjects will be asked not to respond. The SSD will be varied from trial to trial by using a step-up/step-down algorithm with an initial estimate of 250 ms to maintain 50% successful inhibition. The task flow chart is shown in figure 3.

{kind=link}
{kind=link}
{kind=link}
Stop behavioural task.
The task will consist of randomly interspersed no-go and stop-signal trials. A total of 480 trials will be performed (75% go, 25% stop).
Secondary outcomes
Secondary outcome measures will include the following: (1) Montreal Cognitive Assessment (MoCA); (2) Beck Depression Inventory (2nd edition) (BDI-II); (3) Mini-Mental State Examination (MMSE); (4) Stroop task testing; (5) n-back task testing; and (6) task-switch task testing (table 3). The process of inhibitory control is the process of inhibition, refresh and switching of the response task through cognitive function, so we will test the abilities of inhibition, refresh and switching in the cognitive process of the elderly with different exercise types before and after the intervention by the Stroop task, the n-back task and the task-switch task to compare their response inhibitory ability. The details of each outcome and instrument will be compiled as in table 3.
The differences among the three groups of subjects at various stages
Montreal Cognitive Assessment
The MoCA is an assessment tool for the rapid screening of cognitive dysfunction. It includes 11 items in 8 cognitive domains: attention and concentration, executive function, memory, language, abstract thinking and computation.17 The highest possible total score is 30, and a score of 26 or more is normal. It has a high sensitivity and a short test time, so it is suitable for clinical application.
Beck Depression Inventory (2nd edition)
The BDI-II contains 21 topics, which are suitable for people older than 13 years old. The areas of focus include symptoms of depression, such as despair, sensitivity, ways of understanding things and physical characteristics, such as fatigue, weight loss and decreased sexual ability.18
Mini-Mental State Examination
The MMSE Scale includes the following seven aspects: time orientation, place orientation, immediate memory, attention and calculation, delayed memory, language, and visual space.19 There are a total of 30 questions asked in the exam, with 1 point awarded for each correct answer, and 0 points given for each wrong answer or unanswered question. The total score range of the scale is 0–30 points. The test scores are closely related to the educational level of the subject. The normal cut-off values are as follows: illiterate subjects, >17; primary school education only, >20; junior high school education and above, >24.
Stroop task
After a period of exercise intervention, comparison of the Stroop task response time between the open-skill, closed-skill, and control groups will be used to explore which types of exercise can improve cognitive inhibition ability.20
N-back task
By comparing the n-back task accuracy of the elderly in the three groups, the improvement of the cognitive refresh ability of each group will be compared under different cognitive loads.21
Task-switch task
By comparing the task-switch accuracy of the three groups under different stimulus conditions, we will determine which type of exercise can improve the cognitive transformation ability most significantly.22
Patient and public involvement
Participants have not been involved in the study recruitment. The authors conceived the initial research questions and outcome measures, and modified according to the telephone interviews with patients and their guardians by a research assistant. In order to assure the safety and feasibility of the intervention, we invited six elderly peoples to learn and practise the table tennis and fit aerobics exercise before designing the RCT. Table tennis and fit aerobics exercise were revised based on the exercise performance and feedback provided by the participants. The burden of the intervention will be assessed by patients and their advisors through face-to-face interviews before signing informed consent. The findings of the study will be disseminated to the participants and their guardians.
Statistical analysis
The outcome assessor will be completed by the designated medical institution (Shanghai Punan Hospital of Pudong New District, Shanghai, China), when the participants go for the assessment, there will be no labels, so the outcome assessors will be blind in the group allocation. In order to ensure no intergroup differences in all test indicators after random grouping, Independent sample t-test will be performed on each pretest data after random grouping. Repeated measures analysis of variance will be used to determine the effects of different types of exercise (open, closed or control) on the primary outcomes (GoRT, SRRT, SSD and SSRT) as well as on the secondary outcomes (MoCA Score, BDI-II Score, MMSE Score, Stroop response time, n-back accuracy, task-switch accuracy), with group and time-serving as factors. Data will be analysed by Ph.D. students who are blind to group allocation.
Discussion
Studies have found that elderly people who participate in ball and racket projects have higher health and physical awareness.23 Pilates exercises decreased depression and improved the balance related to falling in elderly,24 and also experienced significant improvement in physical, social spiritual and emotional wellness.25 Korean scholars found the cognitive/exercise dual-task programme was an effective intervention for improving cognitive function, health status and life satisfaction, and for decreasing depression of the elderly living in the community.24
Then some researchers found that athletes participating in open-skill exercises have a faster switching speed, fewer cognitive resources and a higher efficiency in the inhibition process.26 At the same time, another study has demonstrated that athletes who engage in open-skill exercises have a stronger reaction switching capability.27 Based on previous research, participating in sports involving open-skill exercises can improve the ability of inhibition, refresh and conversion in the inhibitory control process. In the Stoop task, when two different dimensions of a stimulus interfere with each other, it is necessary for participants to inhibit the interfering stimulus, it looked at the participants’ ability to suppress interference. In the n-back task, participants’ attention capacity and memory capacity could be examined during the process of stimulus updating. In task-switch task, participants need to keep their attention focused when switching between different tasks, so it can investigate the transformation ability of participants in the cognitive process. Therefore, in this study, the Stroop task, n-back task, and task-switch task were selected as secondary outcomes to investigate the inhibition, refresh and transformation abilities, respectively, of the participants. Determining the effect of long-term intervention of different types of sports on the response inhibitory ability of the elderly will improve our understanding of inhibitory control degradation and support the development of diversified training programmes.
This study will use the SST to explore how different types of exercise experience affect the response inhibition ability in the elderly. Because of the interactions of the cognitive level, depressive state and mental state with the response inhibitory ability, we will perform multiple MoCA, BDI-II, MMSE measurements before and after each intervention. We will also explore whether sports involving open-skill exercises can improve the cognitive level, depression state and mental state of the elderly while improving their inhibition and control ability. Through multidimensional measurements of the participants, we hope to provide a more sufficient theoretical basis for the mechanism of improving the inhibition and control ability of the elderly through exercise.
This study will have several limitations. In this research, the screening principles of the subjects will be determined in the longitudinal study, and the inclusion criteria and exclusion criteria will be strictly defined, especially the experimental groups and the control group in terms of age, physical level, intervention time and intensity. In addition, because the exercise that will serve as an intervention will be widely known to the participants, the single-blind design may expose the study to risks of bias stemming from performance and evaluation, which may potentially lead to overestimation of the effects of exercise.
Ethics and dissemination
All participants who meet the inclusion and exclusion criteria will be required to sign an informed consent form prior to enrolling in the study. This study was approved by the Shanghai University of Sport Research Ethics Committee (102772019RT012). Study findings will be disseminated via publications in peer-reviewed journals and presentations at international conferences.
Ethics statements
Patient consent for publication
References
Footnotes
LK and ZL are joint first authors.
Contributors LK: Conceptualisation, methodology and software. ZL: Writing—reviewing and editing. ZJ: Visualisation and investigation. WJ: Data curation and writing—original draft preparation.
Funding This study was supported by grants from the outstanding clinical discipline project of Shanghai Pudong (PWYGy 2018-04) and National Natural Science Foundation of China (3197070657).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Outcomes section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.