Article Text

Abstract
Objectives Survival among children diagnosed with acute lymphoblastic leukaemia (ALL) has increased considerably. However, morbidity in survivors constitutes a potential increasing burden not limited to secondary health care. Our objectives were to compare health care utilisation, including both primary and secondary health care, between childhood ALL survivors and matched references up to 15 years after curative treatment. Moreover, to increase knowledge on survivors’ health service seeking behaviour as time from treatment elapsed.
Design and setting A Danish population-based matched cohort study linking multiple nationwide registries.
Participants 675 cases, diagnosed with childhood (1.0–17.9 years) ALL between 1994 and 2015, and 6750 matched references sampled randomly from the source population (matched on age, gender and geographical region).
Primary outcome measures Repeated consultations in general practice and hospital (outpatient and inpatient) estimated as yearly rates from 2.5 years after diagnosis and onwards. We compared cases and references with yearly incidence rate ratios (IRRs) from negative binomial regression models.
Results Survivors of childhood ALL had a mean number of yearly daytime contacts in general practice of 4.75 (95% CI 4.41 to 5.11) the first year, corresponding to an IRR of 1.85 (95% CI 1.71 to 2.00); decreasing to 1.16 (1.01 to 1.34) after 15 years, and without significant impact of gender (p=0.894) or age (p=0.399). For hospital contacts, ALL survivors had a mean number of yearly contacts of 14.21 (13.38–15.08) the first year, corresponding to an IRR of 31.50 (28.29–35.07); decreasing to 2.42 (1.59–3.68) after 15 years. No differences were found across calendar time.
Conclusions ALL survivors used significantly more health care services across sectors than the reference population. Decreasing use over 15 years illustrated the dynamics of health care needs; this knowledge may inform the future organisation of integrated follow-up programmes.
Trial registration number NCT03985826.
- leukaemia
- paediatric oncology
- primary care
- epidemiology
Data availability statement
No data are available. Data sharing statement: According to the data agreement with the data provider, we are not allowed to share our data. Data are stored and maintained electronically at Statistics Denmark.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to assess use of general practice in a population of childhood acute lymphoblastic leukaemia survivors, and not a broad spectrum of childhood cancer survivors.
The longitudinal data with measuring of repeated events provide valuable insight into long-term changes of health care utilisation as time from treatment elapsed.
Use of complete nationwide registries with nearly no loss to follow-up linked on an individual level ensures that the study was population-based and limits selection bias.
A large, matched population-based reference group provides a high statistical precision.
Information on all possible confounders was not available; however, due to a high number of matched references and the random identification, residual confounding is minimised.
Introduction
Acute lymphoblastic leukaemia (ALL) is the most frequent childhood cancer. In recent decades, advances in ALL treatment have increased the 5-year survival rate to above 90%.1 2 Recent studies have demonstrated that long-term survivors of childhood cancer, including ALL, have an increased risk of hospitalisations3–11 and have more chronic conditions than references.12–15
The majority of previous studies including non-hospital-based contacts with doctors found survivors of childhood cancer to have increased utilisation of general practice services,10 16–19 with one study presenting similar use of general practice in survivors of childhood cancer and references 11 years after diagnosis.20 Participants in these studies had a diverse spectrum of childhood cancers. In some studies, data were self-reported thus increasing the risk of recall bias, and some studies had a short follow-up time.10 16–21 Studies on health care utilisation in general practice as a function of time since diagnosis are inconsistent; however, the majority of existing studies did not investigate this association. An inverse association between time since diagnosis and number of yearly visits was observed for the first 5 years after diagnosis.16 17 McBride et al19 described no association between time since diagnosis and health care utilisation in later time periods. None of these studies reported results about changes in health care use in general practice across calendar time.
Thus, questions remain about the longitudinal excess health care utilisation including general practice as well as inpatient and outpatient hospital contacts, which may be used as proxy measures for health care needs and overall disease burden in this patient group. The aim of this study was to compare health care utilisation over time between ALL survivors and matched references, and to analyse if calendar time or treatment regime affected health care utilisation.
Methods
Study design and setting
We conducted a nationwide, population-based matched cohort study using information from several Danish registries. Data on health care utilisation were extracted retrospectively for the period 1 January 1997 to 31 December 2018. Since 1997, all Danish children have been registered with their own unique Civil Personal Registration (CPR) number, enabling complete follow-up of each individual child. Before 1997, children’s contacts to general practice were registered under their parents’ CPR number.22 In Denmark, health care is primarily tax financed and free of charge for all citizens (population 5.8 million). The CPR number follows all citizens from birth to death, and data retrieved from Danish public registries were linked at individual level using the CPR number.
General practitioners act as gatekeepers in the Danish healthcare system except for emergencies and approximately 98% of the Danish population is registered with a specific general practice.23
We used the REporting of studies Conducted using Observational Routinely collected health Data statement checklist24 as a guide for reporting of this study (online supplemental table S1).
Supplemental material
Participants
Cases were defined as children (1.0–17.9 years) diagnosed with ALL between 1994 and 2015, and surviving at least 2.5 years after diagnosis (figure 1). Cases were identified in the Nordic Society of Paediatric Haematology and Oncology (NOPHO) ALL registry, which holds comprehensive data on all children aged 1.0–14.9 years in Denmark diagnosed with ALL since 1992. From 2008 and onwards, the ALL registry was extended to include children and adolescents aged 1.0–17.9 years.
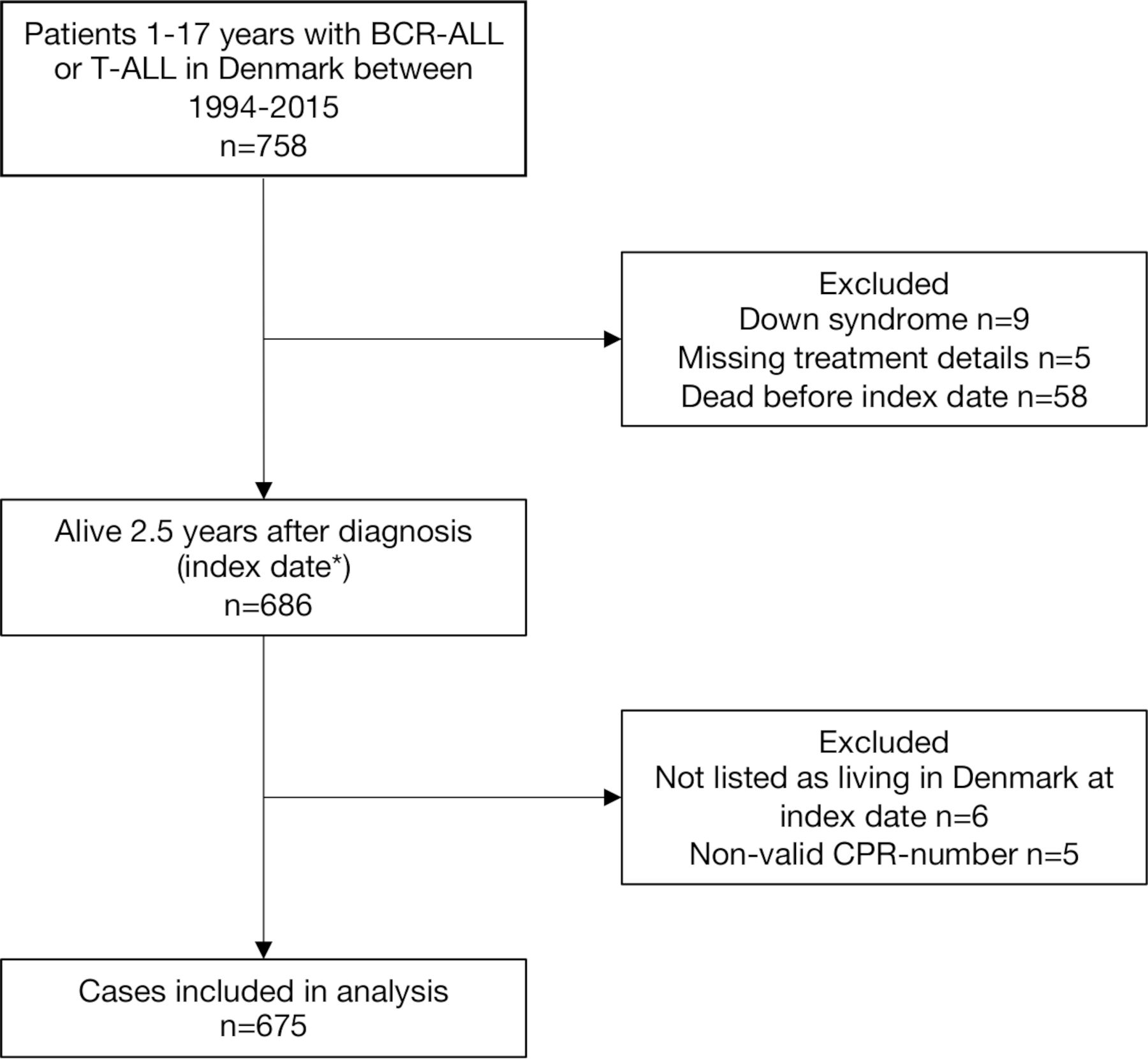
Flow diagram of the study population.*Index date: 2.5 years after diagnosis of acute lymphoblastic leukaemia. BCR-ALL, B-cell precursor acute lymphoblastic leukaemia; CPR-number, Civil Personal Registration number; T-ALL, T-lineage acute lymphoblastic leukaemia.
The reference cohort was sampled randomly from the source population using the Danish Civil Registration System25 and matched by age, sex and geographical region among the five Danish regions and with no history of childhood cancer 2.5 years after the case was diagnosed (incidence density sampling). To check for history of childhood cancer, the reference cohort was checked in the Danish Cancer Registry,26 which holds information on all new cases of cancer in Denmark.
Each patient with ALL was matched with 10 reference subjects. Because of the population-based design, the study size was determined by the number of cases in the area during the study period. No sample size calculation was made.
Data sources and variables
Data from national population-based health registries were linked and hosted by Statistics Denmark. Postlinkage data were pseudoanonymised before the authors obtained access to the data.
We collected data on the following variables from the NOPHO registry: ALL treatment protocol (1992, 2000 or 2008), immunophenotype, haematopoietic stem cell transplantation and relapse. From the NOPHO registry, we further collected data on risk groups (non-high risk or high risk); at diagnosis, patients were stratified as high risk or non-high risk based on a number of characteristics: age, white blood cell count, involvement of extramedullary sites, immunophenotype, cytogenetics and response to treatment. A detailed description of risk group stratification according to the different treatment protocols has previously been published.1 27 28 We had no patient level information on treatment with cranial irradiation; however, in the NOPHO ALL1992 and NOPHO ALL2000 eras, the very high-risk group was treated with cranial irradiation according to protocol.27 Data on very high-risk group were obtained as a proxy for cranial irradiation. Information about sex, age, vital status, immigration and emigration was obtained from the Danish Civil Registration System.25 Information about the development of a second malignant neoplasm (SMN) was obtained from the Danish Cancer Registry.26
Outcomes
The primary outcomes were repeated contacts to general practice and hospital for up to 15 years after the end of curative ALL treatment. Data from general practice were obtained from the National Health Insurance Service Register.22 General practice data included contacts (daytime face-to-face contacts, out-of-hours contacts, email consultations, telephone consultations and home visits) and diagnostic procedures (blood test, urine test, streptococcus throat test, pulmonary functions test and ECG). We chose to include diagnostic procedures to provide a picture of the diagnostic activity level. We did not include preventive health examinations of children, vaccinations, screening for cervical cancer and pregnancy care. For a complete list of codes, see online supplemental table S2. Data from secondary health care were obtained from the Danish National Patient Registry.29 Secondary health care data included inpatient hospital care and outpatient visits at both public and private hospitals. Contacts to the accident and emergency department were excluded from the analyses as we expected no difference in visits between ALL survivors and matched references.
Supplemental material
Statistical methods
Follow-up on health care contacts started 2.5 years after diagnosis for cases (the index date, which approximates the time of ending maintenance therapy) and on the corresponding day for the reference group. Study follow-up ended on the date of death, date of emigration or end of study (31 December 2018 for contacts related to general practice and 31 December 2017 for hospital contacts), whichever came first.
To estimate and compare yearly rates of health care contacts for cases and references, we used a negative binominal regression model. To account for differences in follow-up time, log-transformed risk time was included in the model with the regression parameter restricted to one. Cluster robust variance was applied to allow for intragroup correlation because repeated measurements (contacts) within individuals cannot be interpreted as independent events. Yearly rates for primary health care contacts (daytime contacts, out-of-hours contacts and diagnostic procedures) and secondary health care contacts (including inpatient hospitalisations and hospital outpatient contacts) were calculated from the index date and forward. Yearly contact rates were calculated as crude estimates.
When comparing the yearly rates of health care contacts for cases and references, we calculated an incidence rate ratio (IRR). IRRs were adjusted for sex and age on the index date. To adjust for age, we used restricted cubic splines with six knots to allow for a non-linear relationship. We conducted stratified analyses on sex and age group (<10 years, ≥10 years at index date). Wald tests were performed to test for interaction between the effect of ALL treatment with age group and sex across all yearly periods of follow-up.
Finally, analyses of ALL cases only were conducted comparing the two risk groups (the non-high-risk group was set as reference), the three calendar times according to treatment protocols (the NOPHO ALL1992 protocol was set as reference) and haematopoietic stem cell transplantation in first complete remission (no transplantation was set as reference).
We performed a sensitivity analysis to investigate the robustness of our results by excluding all cases undergoing haematopoietic stem cell transplantation at any time point. Moreover, we conducted a sensitivity analysis censoring all cases developing a relapse or an SMN on the date of the relapse/SMN diagnosis.
All estimates are presented with 95% CIs. All tests were two sided and a p value<0.05 was considered statistically significant. Data were analysed using the statistical software package Stata V.16.1 (StataCorp LLC, Texas, USA).
Patient and public involvement
The study included no patient and public involvement.
Results
The study included 675 childhood ALL survivors and 6750 matched references with a total follow-up time of 81 611 person-years and a median follow-up time of 11 years. Table 1 shows characteristics of the population. The overall 5-year survival rate was 97.5% (95% CI 95.9 to 98.5) for the included 675 childhood ALL survivors (risk time starts at index date).
Characteristics of the study population
Health care utilisation
ALL survivors had a mean number of yearly daytime contacts in general practice of 4.75 (95% CI 4.41 to 5.11) the first year after the index date, corresponding to an IRR of 1.85 (95% CI 1.71 to 2.00); this declined to rates not statistically different from references during a 10-year period, IRR=1.11 (95% CI 0.99 to 1.25) 10 years after the index date; however, the IRRs remained above one throughout the follow-up (figure 2). For out-of-hours contacts and diagnostic procedures, the IRRs comparing cases and references the first year after the index date were 2.14 (95% CI 1.81 to 2.53) and 2.38 (95% CI 2.05 to 2.77), respectively, (figure 2).
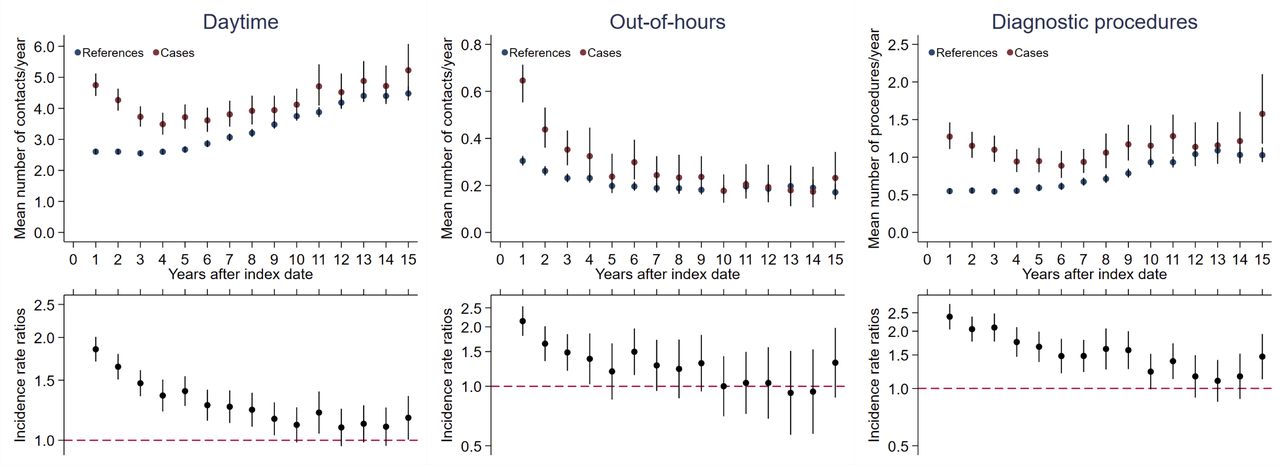
General practice health care utilisation during 15 years.A total of 675 cases compared with 6750 references. Health care utilisation after the index date is divided into daytime consultations, out-of-hours consultations and diagnostic procedures in general practice. Top panel: Mean yearly number of contacts/diagnostic procedures presented as crude rates. Bottom panel: Incidence rate ratios adjusted for age and sex. Vertical lines represent 95% CIs. Index date: 2.5 years after diagnosis of acute lymphoblastic leukaemia for cases and the corresponding date for references.
For hospital health care utilisation, ALL survivors had a mean number of yearly contacts of 14.21 (95% CI 13.38 to 15.08), corresponding to an IRR of 31.50 (95% CI 28.29 to 35.07) the first year after the index date, declining to an IRR of 2.42 (95% CI 1.59 to 3.68) 15 years after the index date (figure 3).

Hospital health care utilisation during 15 years.Hospital health care utilisation after the index date; 675 cases compared with 6750 references. Top panel: Mean yearly number of contacts presented as crude rates. Bottom panel: Incidence rate ratios adjusted for age and sex. Vertical lines represent 95% CIs.Hospital health care utilisation: Including hospital inpatient and hospital outpatient contacts. Index date: 2.5 years after diagnosis of acute lymphoblastic leukaemia for cases and the corresponding date for references.
Comparing the three protocols (corresponding three calendar times) for ALL cases only revealed similar contact rates (figure 4). Comparing the two risk groups showed statistically significantly more contacts in the high-risk group, year 1 after the index date in general practice (figure 5). Comparing patients with ALL treated with or without haematopoietic stem cell transplantation (no transplantation was set as reference) revealed more contacts in the transplantation group (online supplemental figure S1).
Supplemental material

Health care utilisation comparing three calendar times.cases only, health care utilisation by year after the index date comparing three calendar times (the NOPHO ALL treatment protocols from 1992 (n=231), 2000 (n=210) and 2008 (n=234)). Health care utilisation is stratified on health care setting (hospital and general practice). Top panel: Mean yearly number of contacts presented as crude rates. Bottom panel: Incidence rate ratios of ALL2000 and ALL2008 compared with ALL1992 (the ALL1992 protocol was set as reference) adjusted for age and sex. Vertical lines represent 95% CIs. Index date: 2.5 years after diagnosis of acute lymphoblastic leukaemia. NOPHO, the Nordic Society of Paediatric Haematology and Oncology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Health care utilisation comparing non-high-risk and high-risk groups.ALL cases only, health care utilisation by year after the index date comparing non-high-risk (n=515) and high-risk groups (n=160) (ie, therapy). Health care utilisation is stratified on health care setting (hospital and general practice). Top panel: Mean yearly number of contacts presented as crude rates. Bottom panel: Incidence rate ratios of high risk compared with non-high risk as reference adjusted for age and sex. Vertical lines represent 95% CIs. Index date: 2.5 years after diagnosis of acute lymphoblastic leukaemia.
Analyses stratified on age group and sex revealed no independent risk factors for use of health care after ALL treatment (online supplemental figures S2 and S3). This was supported by insignificant results from the tests for interaction between the effect of ALL treatment with sex (p=0.894 for general practice, p=0.067 for hospital) and age (p=0.399 for general practice, p=0.079 for hospital).
Supplemental material
Supplemental material
Sensitivity analyses
In the analysis excluding all cases undergoing haematopoietic stem cell transplantation at any time point before or after index date, the overall findings remained the same (online supplemental figure S4). In the analysis, censoring all cases developing a relapse or an SMN on the date of relapse/SMN diagnosis did not change the overall findings (online supplemental figure S5).
Supplemental material
Supplemental material
Discussion
The present population-based study was designed to investigate the longitudinal overall excess health care utilisation in survivors of childhood ALL from treatment cessation and onwards. Our results showed that ALL survivors had a higher utilisation of general practice and hospital health care services than their matched references, with a declining pattern over the 15-year period as time from treatment elapsed. For hospital health care utilisation, the number of yearly contacts showed a steep decline during the first 5 years. This finding is in agreement with survivors attending frequent but declining hospital-based follow-up during the first 5 years.30 It is noteworthy that the use of general practice services was high in the same time period as survivors attending frequent hospital-based follow-up.
No differences in health care utilisation emerged across calendar time (measured by treatment protocols). This has, to the best of our knowledge, not previously been analysed in a primary health care setting. As expected, we found increased health care use in patients following haematopoietic stem cell transplantation.31 32 Patients treated with cranial irradiation are included in the high-risk group, and we expected patients treated with cranial irradiation to have increased health care use.4 12 15 20 21 33–35 However, the increased utilisation in the high-risk group was only significant in year 1 in general practice. This could reflect that the number of patients exposed to cranial irradiation is low. Analyses stratified on age group and sex revealed no independent risk factors for use of health care after ALL treatment. As expected from previous research,36 we found an overall tendency towards increased use of general practice services in females compared with males. The differences found in ALL survivors corresponded to sex differences in the general population.
Strengths and limitations
The population-based design using nationwide registries linked on an individual level is a strength. The use of complete nationwide registries with nearly no loss to follow-up limits selection bias. Use of registry data on health care contacts covering a long period provides a picture of the temporal development in health care utilisation as time from treatment elapsed. Furthermore, a large matched population-based reference group is an advantage as it provides a high statistical precision. Data on exposure are robust to misclassification because cancer registration is mandatory in Denmark.26
Health care data are collected routinely and uniformly in the Danish healthcare system. They are collected for all individuals and not for the purpose of the present study. We have no reason to believe that ALL cases had more or less complete registration of health care data, thereby minimising potential misclassification.37
The study period began 2.5 years after diagnosis to ensure that curative treatment had ended, which ensures a fairly homogeneous study group. However, we expect some cases to have extended treatment, explaining some of the increased rates of hospital contacts in the first year after the index date.
We reduced confounding by age, gender and geographical region by matching cases with references. Still, residual confounding will exist due to ethnicity and socioeconomic factors, including rural/urban status. However, due to the high number of matched references and the random identification, residual confounding may have been further minimised. We believe that our findings can be generalised to other countries with comparable healthcare systems.
Comparison with other studies
Previous studies on primary health care utilisation in childhood cancer survivors have been based on participants with a broad spectrum of childhood cancers and have investigated shorter periods either right after diagnosis or later in life. Two studies16 17 investigated health care utilisation in the 5-year period from diagnosis. Both studies found increased use of general practice services among childhood cancer survivors, which is in agreement with our results. Shaw et al20 found similar use of general practice services among childhood cancer survivors and general population controls. This is not in agreement with our results; however, results are based on self-reported outcomes. Three studies10 18 19 found an increased use of general practice in the survivor group compared with a comparison group later in life, including patients analysed up to 62 years after a cancer diagnosis. Data in these studies are not presented with contact rate ratios as a function of time since diagnosis and they are thus difficult to compare with our results. In none of the mentioned studies, it was possible to compare different calendar times.
We studied both inpatient and outpatient hospital contacts, and calculated the contact rate ratio for each year following the end of ALL treatment. Two studies3 5 based on hospital admissions found that the hospitalisation rate ratio for leukaemia survivors was approximately two times higher than their references. This was in agreement with our results, at 15 years from index date. These studies presented no information about treatment regimen.
Conclusions
Our findings demonstrate that ALL survivors use health care in general practice, out-of-hours services and hospitals considerably more often than their peers. This indicates a continuing need for medical care across sectors for 10 or more years after treatment has ended. Thus, ALL survivors seem to have a high need for integrated and coordinated follow-up in general practice and hospitals; this knowledge may inform the organisation of future follow-up programmes for this group.
Data availability statement
No data are available. Data sharing statement: According to the data agreement with the data provider, we are not allowed to share our data. Data are stored and maintained electronically at Statistics Denmark.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Danish Data Protection Agency (ID 277). Medical ethical approval was not required according to Danish law.
Acknowledgments
The authors wish to thank Kaare Rud Flarup for his assistance with data management.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KSJ designed the study, analysed and interpreted data and wrote the manuscript. BKA interpreted data and edited the manuscript. HS designed the study and edited the manuscript. AZF analysed and interpreted data and edited the manuscript. KS interpreted data and edited the manuscript. SR interpreted data and edited the manuscript. MTC interpreted data and edited the manuscript. PV designed the study, interpreted data, edited the manuscript and acted as guarantor. All authors approved the final manuscript.
Funding This work was supported by a grant from the Danish Cancer Society (Kræftens Bekæmpelse). Grant number R124-A7831-15-S2. The funders had no role in the design and conduct of the study.
Competing interests BKA declares the following: sponsor for the investigator initiated NOR-GRASPALL 2016 study. KS declares the following: Speaker and/or Advisory Board Honoraria from Jazz Pharmaceuticals (2020) and Servier (2020); speaker fee from Amgen (2020) and Medscape (2020); Educational grant from Servier (2020).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.