Article Text

Abstract
Objectives The incidence of Neisseria gonorrhoeae and its antimicrobial resistance is increasing in many countries. Antibacterial mouthwash may reduce gonorrhoea transmission without using antibiotics. We modelled the effect that antiseptic mouthwash may have on the incidence of gonorrhoea.
Design We developed a mathematical model of the transmission of gonorrhoea between each anatomical site (oropharynx, urethra and anorectum) in men who have sex with men (MSM). We constructed four scenarios: (1) mouthwash had no effect; (2) mouthwash increased the susceptibility of the oropharynx; (3) mouthwash reduced the transmissibility from the oropharynx; (4) the combined effect of mouthwash from scenarios 2 and 3.
Setting We used data at three anatomical sites from 4873 MSM attending Melbourne Sexual Health Centre in 2018 and 2019 to calibrate our models and data from the USA, Netherlands and Thailand for sensitivity analyses.
Participants Published available data on MSM with multisite infections of gonorrhoea.
Primary and secondary outcome measures Incidence of gonorrhoea.
Results The overall incidence of gonorrhoea was 44 (95% CI 37 to 50)/100 person-years (PY) in scenario 1. Under scenario 2 (20%–80% mouthwash coverage), the total incidence increased (47–60/100 PY) and at all three anatomical sites by between 7.4% (5.9%–60.8%) and 136.6% (108.1%–177.5%). Under scenario 3, with the same coverage, the total incidence decreased (20–39/100 PY) and at all anatomical sites by between 11.6% (10.2%–13.5%) and 99.8% (99.2%–100%). Under scenario 4, changes in the incidence depended on the efficacy of mouthwash on the susceptibility or transmissibility. The effect on the total incidence varied (22–55/100 PY), and at all anatomical sites, there were increases of nearly 130% and large declines of almost 100%.
Conclusions The effect of mouthwash on gonorrhoea incidence is largely predictable depending on whether it increases susceptibility to or reduces the transmissibility of gonorrhoea.
- epidemiology
- infection control
- public health
- sexual medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data analysed during this study are included in this article and its additional file.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our model is the first to include infection occurring at multiple anatomical sites in the same person and include complex sequential sexual practices to evaluate the potential effect of antiseptic mouthwash on the incidence of gonorrhoea at a population level.
Our model is the first to assess the effect that antiseptic mouthwash would have on gonorrhoea incidence if it were to increase the susceptibility of the oropharynx to gonorrhoea or/and reduce transmission of gonorrhoea from the oropharynx at a population level.
There were limited data on the effect of mouthwash on susceptibility or transmissibility, so we had to make assumptions about the magnitude of these effects.
There were limited data on some variables in our model, including the duration of mouthwash’s potential ‘treatment’ effect, how men would use mouthwash (eg, oral rinse, oral gargle and oral spray) and when they used mouthwash in relation to sexual exposure.
Our model included the main sexual practices that involved the use of saliva when men have sex together but not all of the many possible combinations.
Introduction
The world is experiencing increasing trends in both the rates of gonorrhoea and its antimicrobial resistance that have prompted Neisseria gonorrhoeae to be deemed a significant global health threat, particularly among men who have sex with men (MSM).1–5 Unfortunately, effective interventions to reduce rates of gonorrhoea have been challenging to identify. Recently, researchers have suggested that oropharyngeal gonorrhoea may be critical to the persistence of infection at a population level6 and that infection may be transmitted by kissing and saliva exchange during sex.7–12 To address the potential transmission associated with the oropharynx, researchers have been investigating mouthwash as an intervention for gonorrhoea prevention without using antibiotics.13–17
Three randomised controlled trials (RCT) have explored the effect of antiseptic mouthwash on gonorrhoea infection.18–20 The first study of 58 MSM in Australia suggested that antiseptic mouthwash reduced the ability to culture gonorrhoea from the oropharynx and, therefore, may potentially reduce gonorrhoea transmission.18 Men in this study who used Listerine mouthwash were less likely to test positive for gonorrhoea at the tonsillar fossae (OR=0.14, 95% CI 0.03 to 0.77) compared with those who used saline. The second study of 530 MSM in Australia assessed whether mouthwash would prevent infection among men who used mouthwash for 3 months. This study reported no significant risk difference in gonorrhoea positivity between the Listerine mouthwash group and the control (Biotène) group of 2.5% (−1.8% to 6.8%) for oropharyngeal infection or at other sites of −4.4% (−7.4% to −1.3%) for urethral infection and 2.5% (−2.0% to 7.0%) for anorectal infection.19
The third RCT of 343 MSM in Belgium was stopped early because of the COVID-19 pandemic. It reported some similar findings to the larger RCT with a significant increase in gonorrhoea at the oropharyngeal and no significant changes at other anatomical sites in the adjusted analysis.20 This suggested that Listerine mouthwash increased the risk of oropharyngeal gonorrhoea and raised the possibility that it may increase the risk of oropharyngeal gonorrhoea rather than reduce it. Taken together, the results of the three clinical trials raise the possibility that antiseptic mouthwash may either increase the susceptibility of the oropharynx to N. gonorrhoeae or potentially decrease its transmissibility.
The WHO’s ‘Global Action Plan to Control the Spread and Impact of Antimicrobial-Resistance in Neisseria gonorrhoeae’ recommends the use of mathematical models to analyse new interventions.21 Zhang et al7 assumed that mouthwash could reduce the duration of gonorrhoea at the oropharynx and found that widespread use may significantly reduce the prevalence of gonorrhoea in the population. Based on the newly emerging evidence on mouthwash and gonorrhoea transmission and the mouthwash RCTs, we used a susceptible-infected-susceptible compartmental model to examine the potential effect of antiseptic mouthwash on gonorrhoea incidence in MSM.
Methods
Study design
We employed a population-level susceptible-infected-susceptible compartmental model to evaluate the potential effects of antiseptic mouthwash on the incidence of gonorrhoea in MSM. The model structure was based on our previously published multisite infection model7 22 (online supplemental figure 1). Differential equations are provided in the online supplemental information.
Supplemental material
Data resources
We used gonorrhoea diagnosis data of 4873 MSM attending Melbourne Sexual Health Centre using nucleic acid amplification test (NAAT) in 2018 and 2019 to calibrate our models.22 The percentage of positivity was ‘oropharynx infection only’ (2.96%), ‘urethra infection only’ (0.31%), ‘anorectum infection only’ (3.16%), ‘oropharynx and urethra co-infection’ (0.21%), ‘oropharynx and anorectum co-infection’ (2.46%), ‘urethra and anorectum co-infection’ (1.19%) and ‘oropharynx, urethra and anorectum co-infection’ (0.72%) (online supplemental information, Data source, online supplemental table 1).
N. gonorrhoeae transmission routes
We simulated gonorrhoea transmission through (1) anal sex; (2) penile-oral sex; (3) rimming; (4) kissing; (5) oral sex followed by anal sex (or vice versa) (penis acts as a mediator and carries N. gonorrhoeae to the oropharynx or anorectum); (6) using saliva as a lubricant for anal sex (pass N. gonorrhoeae from his oropharynx to his urethra); and (7) oral sex followed by oral-anal sex (rimming) or vice versa (oropharynx acts as a mediator and carries N. gonorrhoeae to the urethra or anorectum).22
Model parametrisation and calibration
We collected behavioural and gonorrhoea progression data in the assumption for our models’ parameters/to inform parameter values for the models (online supplemental information, Data source, online supplemental table 2). We used MATLAB R2019a to conduct numerical simulations and perform the statistical analysis. We sampled the parameter space using Latin hypercube sampling23 24 within the parameter uncertainty bound ranges and generated a pool of 1000 parameter sets. Using each sampled set of parameters as the initial points, we simulated the transmission model. We used the ‘trust-region-reflective’ method (‘fmincon’ in MATLAB25) for the optimisation process to search for the parameter sets that are best fitted to the empirical prevalence of the infections. We then calibrated the model-simulated site-specific gonorrhoea prevalence at equilibrium to empirical gonorrhoea diagnosis data at each anatomical site (ie, oropharynx, urethra and anorectum) as well as multisite infection (oropharynx and urethra together, oropharynx and anorectum together, urethra and anorectum together, oropharynx and urethra and anorectum together). We define the goodness of fit as the sum square error between the prevalence levels based on model simulations and empirical data for each simulation. We then ranked the goodness of fit in ascending order (the best fitted simulations on the top) and selected the top 10% of 1000 simulations. We regarded the selected 10% simulations as the pool of parameter sets that were best calibrated to the empirical data and used these simulations to estimate the 95% CIs of the output indicators. The study methods and goodness of fit of the model have been reported previously.22
Scenarios for the modelled effect of mouthwash on gonorrhoea incidence
Following model calibration, we established four scenarios to evaluate antiseptic mouthwash’s effectiveness on the incidence of gonorrhoea. We estimated the number of new infections at any given time and calculated the incidence as the ratio between the number of new infections and the number of susceptible.7 22 26 The effect of antiseptic mouthwash on transmissibility and susceptibility between two men is shown in figure 1. We constructed the following four scenarios: (1) mouthwash had no effect on N. gonorrhoeae; (2) mouthwash increased the susceptibility of acquiring oropharyngeal gonorrhoea during sexual practices including penile-oral sex (from the urethra to oropharynx), rimming (from the anorectum to oropharynx) and kissing (from the oropharynx to oropharynx); (3) mouthwash reduced the transmissibility from an infected oropharynx during sexual practices including penile-oral sex (from the oropharynx to urethra), rimming (from the oropharynx to anorectum), kissing (from the oropharynx to oropharynx), using saliva as a lubricant for anal sex (from own oropharynx to own urethra), oral sex followed by oral-anal sex (rimming) or vice versa (oropharynx acts as a mediator and carries N. gonorrhoeae from the oropharynx to the anorectum); (4) mouthwash reduced transmissibility from the oropharynx and increased susceptibility to acquiring oropharyngeal gonorrhoea, that is, a combined scenario of (2) and (3).
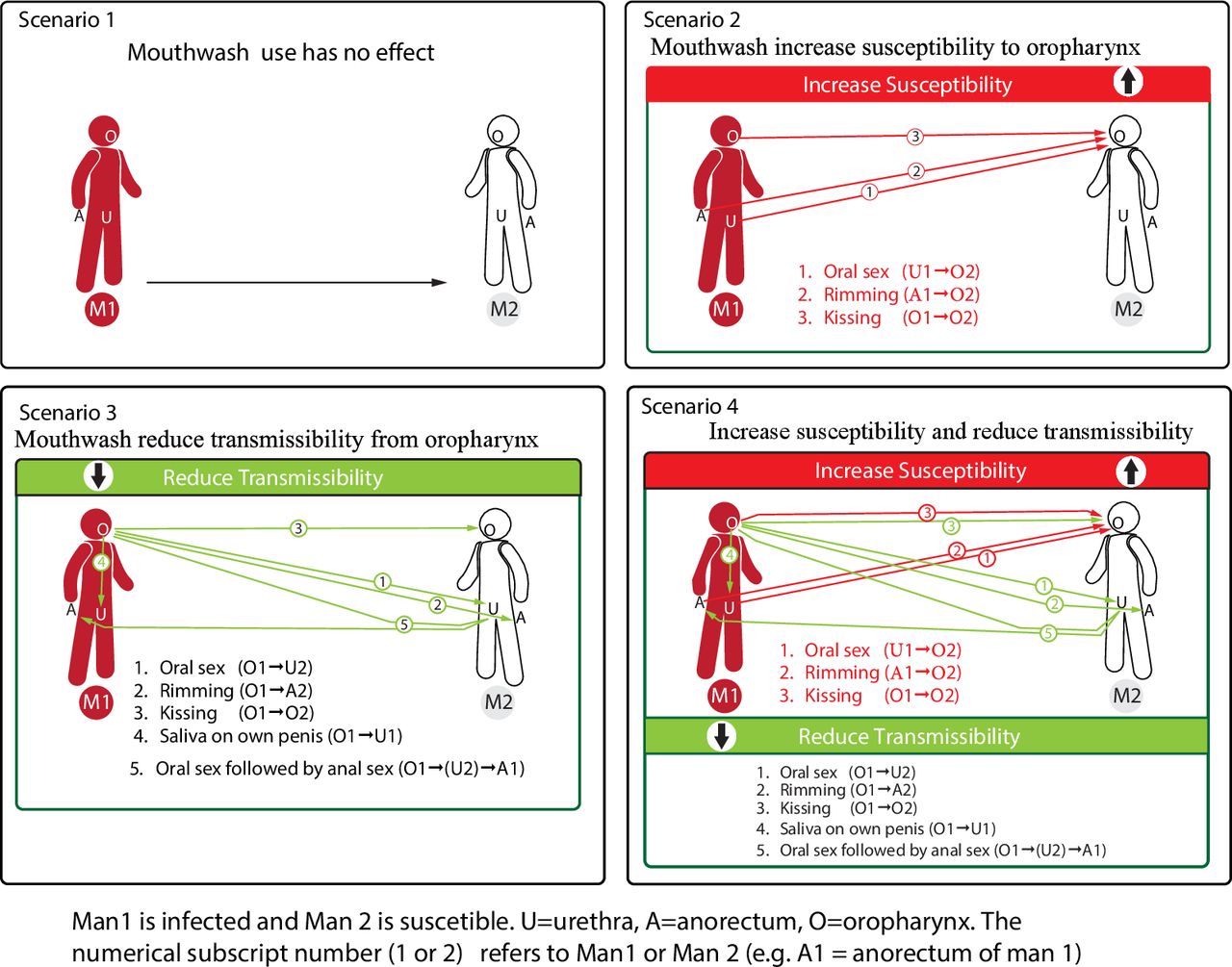
The effect of antiseptic mouthwash on transmissibility and susceptibility between man 1 and man 2 in the one sexual episode.
In our simulations, we examined the scenarios for the potential efficacy of mouthwash that would increase the susceptibility and reduce the transmissibility by 5%, 10%, 15%, 20% and 25% for using mouthwash shortly before or immediately after each sexual act. Like previous studies,19 20 we defined the population coverage of mouthwash as the proportion of MSM who used mouthwash daily.
Sensitivity analysis
We identified five similar studies that reported multisite infections of gonorrhoea using NAAT, including (1) 3049 MSM, attending a health centre in Boston, Massachusetts, during 2012–20169; (2) 393 MSM attending sexually transmitted disease and HIV care clinics in the USA during 2018–201927; (3) 179 MSM living with HIV in Birmingham, Alabama, during 2014–201628; (4) MSM surveillance data (271 242 consultations) from nationwide Dutch sexually transmitted infection clinics during 2008–201729; and (5) 1610 MSM attending a community-led test and treat cohort in Thailand during 2015–201630 (online supplemental information, Data source, online supplemental table 1). We also modelled the potential effects of antiseptic mouthwash on the gonorrhoea incidence using the above five additional data sets.
Patient and public involvement
Our study was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes or to interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
Figure 1 shows the potential effects of mouthwash on the incidence of gonorrhoea at any anatomical site and also the effect at individual anatomical sites: oropharynx, anorectum and urethra. In the absence of any effect of mouthwash (scenario 1), the incidence of gonorrhoea at all three anatomical sites was 44 (95% CI 37 to 50)/100 person-years (PY): 26 (95% CI 22 to 31)/100 PY at the oropharynx, 9 (95% CI 8 to 11)/100 PY at the anorectum and 8 (95% CI 5 to 12)/100 PY at the urethra (online supplemental information, Supplementary results, online supplemental tables 3–8).
If mouthwash increased the oropharynx’s susceptibility to N. gonorrhoeae (scenario 2), then the incidence would increase at all three sites. The magnitude of the increase would depend on the coverage of mouthwash in the MSM population. With a mouthwash coverage of 20% the incidence at the oropharynx, percentage changed between 7.5% (95% CI 5.9% to 61.6%) and 37.3% (95% CI 29.3% to 85.4%), at the anorectum percentage changed between 7.3% (95% CI 5.7% to 59.2%) and 36.0% (95% CI 28.0% to 81.6%) and at the urethra it increased by between 7.4% (95% CI 5.8% to 60.3%) and 36.5% (95% CI 28.6% to 83.4%) when the susceptibility increased from between 5% and 25%. When the population coverage of mouthwash uses increased, the magnitude of the incidence also increased (figures 2 and 3).

Estimated effect of antiseptic mouthwash on gonorrhoea incidence rate per 100 person-years that occur at the oropharynx, anorectum or urethra in men who have sex with men (MSM). (1) Baseline (scenario 1). (2) Increasing susceptibility of oropharyngeal gonorrhoea only (scenario 2). (3) Reducing transmissibility of gonorrhoea only (scenario 3). (4) Reducing transmissibility from the oropharynx and increasing susceptibility to the oropharynx (scenario 4).

{kind=link}
{kind=link}
{kind=link}
Contour plots for the effect of antiseptic mouthwash on the percentage change (%) of incidence at the oropharynx, anorectum or urethra by increasing susceptibility of oropharyngeal gonorrhoea and reducing transmissibility of gonorrhoea from the oropharynx. The black solid isoclines indicate the threshold that the percentage change of incidence is zero.
If mouthwash were to reduce the transmissibility of N. gonorrhoeae from the oropharynx (scenario 3), then the incidence of gonorrhoea would reduce at all three sites. As for scenario 3, the magnitude of the decrease would depend on the coverage of mouthwash in the MSM population. With a mouthwash coverage of 20% the percentage changed in incidence at the oropharynx from −11.5% (95% CI −13.5% to −10.1%) to −54.1% (95% CI −62.0% to −48.6%), at the anorectum from −11.9% (95% CI −13.9% to −10.5%) to −54.5% (95% CI −62.3% to −48.9%) and at the urethra from −11.6% (95% CI −13.6% to −10.2%) to −55.4% (95% CI −62.9% to −49.8%) when the susceptibility increased from between 5% and 25%. When the population coverage of mouthwash uses increased, the magnitude of the fall in incidence also increased (figures 2 and 3) (online supplemental information, Supplementary results, online supplemental tables 2–7).
If mouthwash increased the susceptibility of the oropharynx to N. gonorrhoeae and reduce the transmissibility of N. gonorrhoeae from the oropharynx (scenario 4), the combined effect of mouthwash on incidence depends on the varying efficacy of both transmissibility and susceptibility and the coverage of mouthwash in the MSM population. With a mouthwash coverage of 20%, mouthwash could result in negative percentage change in incidence of −0.8% (95% CI −10.7% to 42.5%) to −48.4% (95% CI −56.8% to −12.2%) at the oropharynx, −1.8% (95% CI −12.0% to 38.8%) to −48.8% (95% CI −57.2% to −13.8%) at the anorectum and −2.8% (95% CI −12.7% to 38.5%) to −49.8% (95% CI −57.9% to −15.1%) at the urethra, in areas below the zero-threshold curve (figure 3). Mouthwash also could result in positive percentage change in incidence of 2.7% (95% CI −1.1% to 53.1%) to 11.6% (95% CI 2.8% to 56.1%) at the oropharynx, 2.3% (95% CI −1.6% to 50.5%) to 23.2% (95% CI 14.8% to 67.1%) at the anorectum and 2.0% (95% CI −1.8% to 51.0%) to 23.2% (95% CI 14.8% to 68.0%) at theurethra, in areas above the zero-threshold curve (figure 1). When the coverage increased, so did the magnitude of the percentage increase. If the incremental reduction in the transmissibility is the same as the incremental increase in susceptibility (scenario 4), the combined effect of mouthwash was projected to reduce gonorrhoea incidence (figures 2 and 3).
We conducted the sensitivity analyses using five different studies with multisite infection data, and the conclusions were similar (details in the online supplemental information, Supplementary results, online supplemental figures 2–6).
Discussion
To our knowledge, this is the first study to model the effect that mouthwash may have on gonorrhoea incidence at a population level if mouthwash were to increase the susceptibility or decrease the transmissibility of gonorrhoea infection. We found substantial changes in the incidence of gonorrhoea occurred in all scenarios but that reductions in the transmissibility of gonorrhoea were more potent than increases in the susceptibility if the incremental reduction in the transmissibility is the same as the incremental increase in susceptibility. To date, only one other study has modelled the effect of mouthwash on gonorrhoea incidence,7 but this study only looked at the effect on duration. There have been very little empirical data at present on the effect of mouthwash both on the transmissibility of gonorrhoea in infected men or susceptibility in uninfected men. We hope this work encourages more researchers to explore the effect of mouthwash on the susceptibility and transmissibility of N. gonorrhoeae to potentially design an intervention if further studies were to show it was beneficial.
Our study shows that if mouthwash increases the oropharynx’s susceptibility in uninfected individuals, it will increase the incidence in the MSM population. Van Dijck et al20 reported that mouthwash significantly increased oropharyngeal gonorrhoea incidence in their randomised trial. Van Dijck et al’s20 study was stopped early, and they suggested that the non-significant increase could possibly be explained if Listerine damaged the oropharyngeal mucosa or microbiome. Van Dijck et al20 also proposed that Listerine mouthwash may eliminate the beneficial effects on the carriage of pathogenic Neisseria, and that this effect was potentially mediated through inhibition of some commensal Neisseria spp that normally act to limit the growth or carriage of N. gonorrhoeae or N. meningitidis.31 32 More research will be needed to investigate the benefits and harms of using mouthwash as an intervention for gonorrhoea prevention. Further study is required to explore how mouthwash changes the oral microbiome and resistome and inhibits the growth of commensal Neisseria sp.
Our study shows that if mouthwash reduced the transmissibility from the oropharynx in the infected individuals, then widespread use of mouthwash would reduce the incidence of gonorrhoea at all sites in MSM at a population level. Mouthwash may reduce transmissibility by reducing the load of viable N. gonorrhoeae bacteria at the oropharynx. Indeed, the first randomised trial undertaken by Chow et al found that substantial and significant reductions in culture-positive gonorrhoea following a minute use of mouthwash.19 Chow et al 33 further examined the effectiveness of antiseptic mouthwash compared with standard of care antibiotics for the treatment of oropharyngeal gonorrhoea and found that mouthwash was not effective although in a small RCT among 12 men. The authors concluded from this study and their first randomised study that mouthwash might have a temporary effect on the load of viable organisms but may not have a prolonged effect. The Oral Mouthwash use to Eradicate GonorrhoeA (OMEGA) trial examined the effect of mouthwash on the incidence of gonorrhoea by comparing an intervention mouthwash (Listerine) versus a control mouthwash (Biotène) among 530 men using daily mouthwash for 3 months. Findings from the OMEGA trial found that men who use the intervention mouthwash (Listerine) had a 4.4% lower positivity of urethral gonorrhoea compared with the control mouthwash group and one possible explanation for this is that mouthwash reduced transmission from the oropharynx to their own penis.19
Understanding the effect of mouthwash on the incidence of gonorrhoea could provide additional potential interventions for controlling the increasing gonorrhoea incidence,34 if it were to be widely used.10 13 There are several issues that need to be clarified in relation to mouthwash. First, the duration of any potential effect of antiseptic mouthwash on the transmissibility of N. gonorrhoeae at the oropharynx should be quantified because it determines when mouthwash should be used in relation to sexual activities. Second, although two RCTs did not demonstrate a decline in the incidence of overall gonorrhoea,19 20 one study showed a decline in the incidence of urethral gonorrhoea.20 However, it does not mean mouthwash did not reduce the bacterial load in infected individuals. Third, the incidence measured by the RCT has its limitations. Although it measures the protective effects of mouthwash in these selected individuals, the RCT did not measure the transmissibility of infected individuals in the next generation of gonorrhoea transmission in the whole MSM population since sexual partners were not tested for gonorrhoea.
This modelling study has some limitations. First, we assumed the effect of mouthwash on susceptibility or transmissibility, and we choose equal estimates with only moderate effect sizes of 0%–25% effects. If mouthwash had a more potent effect on either susceptibility or transmissibility, the effect on the incidence would be considerably greater. We did, however, show a moderate effect on the incidence of infection with the estimates we chose. Second, we have made several assumptions about mouthwash use in our study because no data were available for these estimates. These assumptions included the duration of the potential ‘treatment’ effect of mouthwash, how mouthwash would be used by men (eg, oral rinse, oral gargle and oral spray), when they used mouthwash (we assumed it was used before sex) and the effect of different ways of using it.35 Third, the diagnosed gonorrhoea data in our model were at a single time point, and we could not calibrate our model to a temporal trend of the epidemic. Fourth, the transmission of gonorrhoea may be largely biased towards high-risk MSM, and we did not separate the transmission by risk groups in our model. Finally, we acknowledge that sexual practices involving saliva may be more complex, and our model may not capture all sexual practices involving saliva. However, our gonorrhoea model does provide a good fit single-site and multisite infections at the oropharynx, urethra and anorectum.22 The good fit indicated an accurate reflection of the actual transmission of gonorrhoea among MSM.
Conclusions
In conclusion, our finding suggests that mouthwash could either increase or decrease the incidence of gonorrhoea at a population level depending on whether it increases susceptibility or decreases transmissibility. Our study highlights the need for more empirical data about the potential effect of mouthwash and the magnitude of this effect.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data analysed during this study are included in this article and its additional file.
Ethics statements
Patient consent for publication
Ethics approval
This study used secondary data analysis of data sets obtained from previous publications and therefore ethical approval was not required.
Acknowledgments
We thank Mark Chung at the MSHC for his assistance in preparing the figures.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors XX, CKF and LZ conceived and designed the study. EPFC contributed to the study design. XX and LZ established the model and did the analysis. MS contributed to modelling and gave overall feedback to the analysis. XX wrote the first draft. EPFC, ZZ, CW, JJO, CKF and LZ participated in the interpretation of results. All authors reviewed the manuscript and approved the final version.
Funding EPFC is supported by an Australian National Health and Medical Research Council Emerging Leadership Investigator Grant (GNT1172873). JJO is supported by an Australian National Health and Medical Research Council Early Career Fellowship (GNT1104781). MS is supported by the National Natural Science Foundation of China (grant number: 11801435), the China Postdoctoral Science Foundation (grant number: 2018M631134), the Fundamental Research Funds for the Central Universities (grant numbers: xjh012019055, xzy032020026) and the Natural Science Basic Research Program of Shaanxi Province (grant number: 2019JQ-187). CKF is supported by an Australian National Health and Medical Research Council Leadership Investigator Grant (GNT1172900). LZ is supported by the National Natural Science Foundation of China (grant number: 81950410639); the Outstanding Young Scholars Support Program (grant number: 3111500001); the Xi’an Jiaotong University Basic Research and Profession Grant (grant numbers: xtr022019003, xzy032020032); the Epidemiology Modeling and Risk Assessment (grant number: 20200344); and the Xi’an Jiaotong University Young Scholar Support Grant (grant number: YX6J004).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.