Article Text

Abstract
Objectives Computerised physician order entry (CPOE) systems facilitate the review of medication orders by pharmacists. Reports have emerged that show conception flaws or the misuse of CPOE systems generate prescribing errors. We aimed to characterise pharmacist interventions (PIs) triggered by prescribing errors identified as system-related errors (PISREs) in French hospitals.
Design This was a cross-sectional observational study based on PIs prospectively documented in the Act-IP observatory database from January 2014 to December 2018.
Setting PISREs from 319 French computerised healthcare facilities were analysed.
Participants Among the 319 French hospitals, 232 (72.7%) performed SRE interventions, involving 652 (51%) pharmacists.
Results Among the 331 678 PIs recorded, 27 058 were qualified as due to SREs (8.2%). The main drug-related problems associated with PISREs were supratherapeutic (27.5%) and subtherapeutic dosage (17.2%), non-conformity with guidelines/contraindications (22.4%) and improper administration (17.9%). The PI prescriber acceptation rate was 78.9% for SREs vs 67.6% for other types of errors. The PISRE ratio was estimated relative to the total number of PIs. Concerning the certification status of CPOE systems, the PISRE ratio was 9.4% for non-certified systems vs 5.5% for certified systems (p<0.001). The PISRE ratio for senior pharmacists was 9.2% and that for pharmacy residents 5.4% (p<0.001). Concerning prescriptions made by graduate prescribers and those made by residents, the PISRE ratio was 8.4% and 7.8%, respectively (p<0.001).
Conclusion Computer-related prescribing errors are common. The PI acceptance rate by prescribers was higher than that observed for PIs that were not CPOE related. This suggests that physicians consider the potential clinical consequences of SREs for patients to be more frequently serious than interventions unrelated to CPOE. CPOE medication review requires continual pharmacist diligence to catch these errors. The significantly lower PISRE ratio for certified software should prompt patient safety agencies to undertake studies to identify the safest software and discard software that is potentially dangerous.
- health & safety
- adverse events
- health informatics
Data availability statement
Data are available on reasonable request. Deidentified participant data are available upon reasonable request to Act-IP© Administrator (email address : actip@sfpc.eu).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study provides an overview of prescribing issues related to the use of computerised physician order entry (CPOE) systems at the national level.
Beyond this large register of prescribing problems related to CPOE use, this is the first study to evaluate pharmacist interventions in daily practice for such a large sample of interventions, pharmacists and hospitals.
This study focuses on declarative data based on interventions performed by hospital pharmacists.
These pharmacist interventions highlight prescription problems, but they are not exhaustive.
Introduction
Every day, numerous hospitalised patients are subject to drug-related problems (DRPs), resulting in suboptimal therapy, suffering and decreased quality of life, as well as high healthcare costs for society.1 2 Computerised physician order entry (CPOE) systems, along with clinical decision support systems (CDSS), improve the safety, quality and value of patient care.3 According to a meta-analysis, CPOE systems have reduced hospital medication errors by approximately 12.5% (95% CI 10.6% to 14.4%).4 However, CPOE systems also have the potential to introduce or contribute to errors. Indeed, new mechanisms that lead to prescription errors have been identified with CPOE: wrong patient selection, failure to report drug allergies, incorrect entry or wrong selection of medication, dose, route or time of administration and confusing free-text comments.5–10
In France, as in other countries, various incentives and requirements have been put in place to encourage computerised drug prescribing, such as France’s ‘Digital Hospital’ programme.11 Since the 2000s, prescribing errors associated with the use of CPOE have been slowly coming to light as healthcare has become increasingly computerised.9 Compared with handwritten prescriptions, the analysis of electronic prescriptions requires a particular effort on the part of pharmacists and other health professionals to detect errors.9 System-related errors (SREs) are defined as those in which the electronic prescribing system functionality or design contributed to the error, with little possibility that another cause, such as lack of knowledge, produced the error. For example, an order for an inappropriate drug located on a drop-down menu next to a likely drug selection is an SRE.12
A pharmacist intervention (PI) due to an SRE is defined as any PI resulting from the identification of a prescribing error by a pharmacist that would probably not have occurred in the context of a handwritten prescription and of which at least one cause is related to the use of a computer (software system configuration issue, software functionality issue or software misuse).13–16
Most studies concerning PIs triggered by system-related prescribing errors were conducted within a single hospital.17–19 As a result, it is not possible to assess the extent of prescribing errors related to electronic systems or draw conclusions about subsequent PIs at a national level.
In 2003, the French Society of Clinical Pharmacy (SFPC) developed and validated a tool for classifying and documenting clinical PIs.20 This tool allows the reporting of DRPs and PIs performed during the daily review of medication orders.21 In 2006, a website, Act-IP, was created with the objectives to (A) create a documentation system that is freely accessible to any pharmacist, through the SFPC Web site (http://www.actip.sfpc.eu/actip/index/ficheip/) and (B) pool the data recorded by all pharmacists to conduct epidemiological studies concerning DRPs detected by pharmacists.22 The data recording is on a voluntary basis. The pooling of PIs constitutes an observatory of clinical pharmacy practices, called the ‘Act-IP Observatory’.
The aim of this study was to characterise PIs triggered due to SREs in French hospitals between 2014 and 2018. Our secondary objective was to determine the physician acceptance rate and its frequency according to the certification status (certified vs non-certified) of the CPOE systems.
Methods
Study design
This was a cross-sectional observational study using PIs prospectively documented in the Act-IP observatory over a 5-year period from 1 January, 2014 to 31 December 2018. The main outcome was a PI due to an SRE (PISRE) reported by French hospital pharmacists on the Act-IP observatory.
Data sources
The data come from PIs registered in the Act-IP Observatory from January 2014 to December 2018. Based on the SFPC criteria, using the report form developed and validated for routine documentation of the PIs, Act-IP users completed the online report form notifying the date, type of DRP, PI, type of drug involved (according to the ATC (Anatomical Therapeutic Chemical) classification), acceptance of the intervention by the prescriber and free-text details of the context. Ten categories were determined for DRPs and seven for PIs (online supplemental appendix 1). A PI was considered to be ‘accepted’ if the physician took it into account and modified the prescription as suggested by the pharmacist or ‘refused’ if the prescription remained unchanged, including cases of expressed refusal by the prescriber. If acceptance of the intervention was impossible to ascertain (ie, discharged patients or those transferred to another ward before acceptance), the PI was noted as ‘not assessable’. The pharmacist’s academic background, hospital characteristics and software used were documented online by the pharmacist when he/she registered onto the Act-IP website. To be registered onto the Act-IP website, pharmacists had prior to accept terms and conditions and allowed the use of their data for analysis. Since July 2013, pharmacists have been able to indicate whether the DRP was ‘related to the electronic system’ or not for each registered PI. For the purpose of this study, PISREs were DRPs rated by each pharmacist as ‘related to the electronic system’ in the Act-IP website.
Supplemental material
The reliability of the classification of the type of drug therapy problem and intervention according to the SFPC classification was determined in a previous study by assessing the degree of agreement between 12 pharmacists using the kappa concordance coefficient (kappa=0.76 for drug problems and kappa=0.89 for drug interventions).20 Database quality controls were performed by an independent pharmacist to ensure that data coding and entry errors were minimal.22
French law made the certification of CPOE systems mandatory on 29 December 2011. However, two decrees abolished this obligation in 2017. Certification is now based on the sole initiative of the software developer. Forty-eight hospital CPOE software packages are currently certified by the agency for patient safety (Haute Autorité de Santé (HAS)).23 For our analysis, PISREs were classified according to the HAS status of the CPOE system (certified vs not certified).
Analysis
The PISRE ratio was estimated relative to the total number of PIs. Proportions were compared using the χ2 test. PISREs coded as ‘refused’ or ‘not assessable’ were combined and compared with the accepted PISREs. Values of p<0.001 were considered to be statistically significant. Statistical analyses were performed using Stata V.13 (Stata). Several qualitative examples are given to illustrate PISREs.
Study participants and public involvement
This research was done without study participant involvement. Patients and/or the public were not involved in the design, or conduct, or dissemination plans of this research.
Results
From January 2014 to December 2018, 331,678 PIs were entered into the Act-IP observatory. Among them, 27 058 (8.2%) were indicated to be system-related prescribing errors (figure 1).

Flow chart, PISRE selection in Act-IP observatory (extraction on 11 February 2019). PI, pharmacist intervention; PISRE, prescribing errors identified as system-related error; SRE, system-related error.
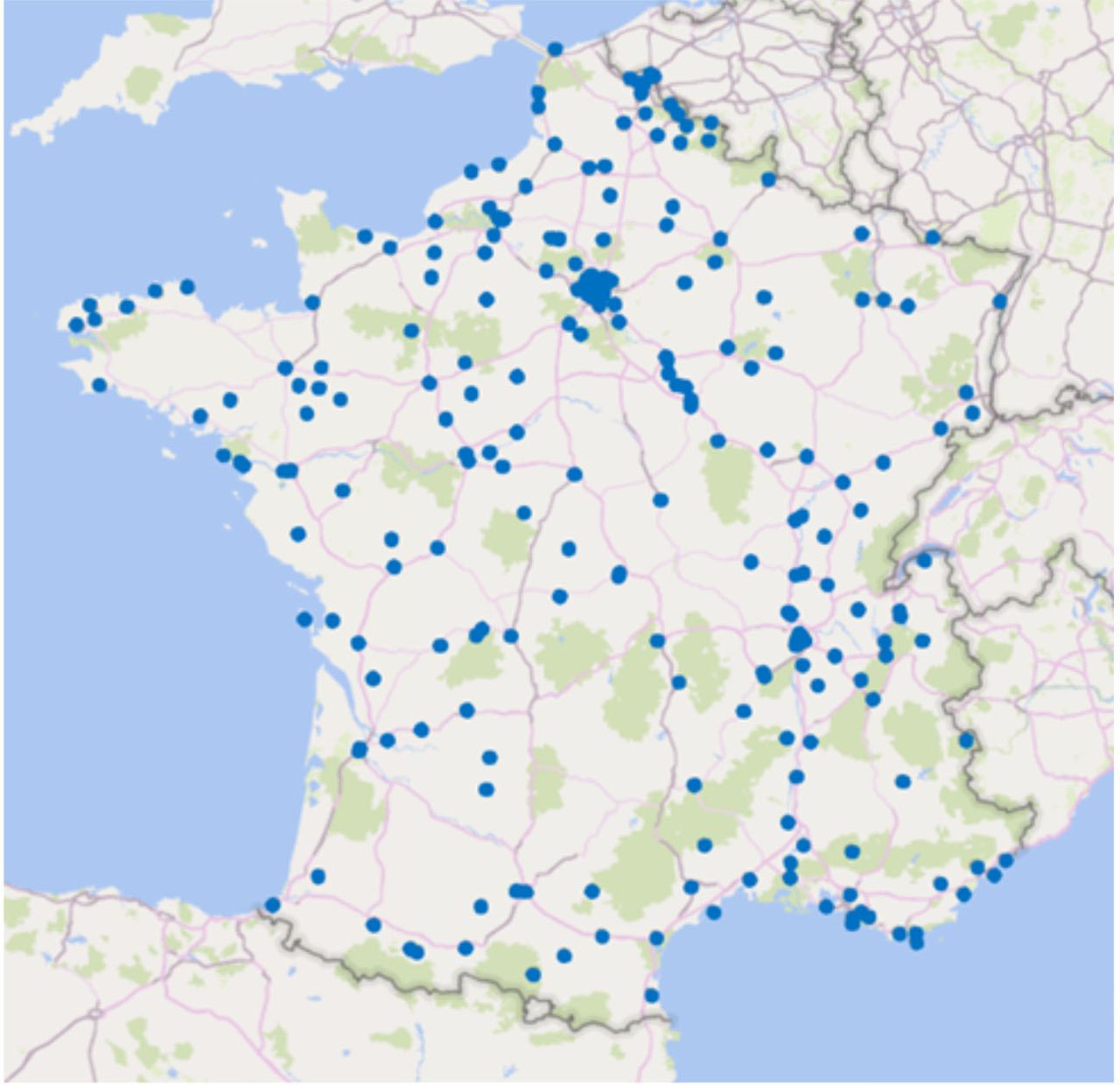
Over the study period, 1219 pharmacists from 319 hospitals recorded PIs in the Act-IP observatory database. The geographical location of the hospitals involved is shown in figure 2. Among them, 232 (72.7%), involving 652 (51%) pharmacists, performed SRE interventions. Among the 319 hospitals, 87 (27.3%) did not qualify any PIs as being due to an SRE. PIs come from 82 software involving 19 certified systems.

{kind=link}
{kind=link}
Geographical location of French hospitals that entered data into the Act-IP observatory between 2014 and 2018.
The characteristics of the PISREs are summarised in table 1. The most commonly identified type of DRP was ‘supratherapeutic dosage’, followed by ‘non-conformity with guidelines/contraindications’ and ‘improper administration’. Among the 27 058 PISREs, 78.9% (n=21 356) were accepted. The PISRE ratio was 9.4% for non-certified systems vs 5.5% for certified systems (p<0.001). Online supplemental appendix 2 presents examples of DRPs classified as being triggered by prescribing errors due to the CPOE system. For example: Prescription errors can be the same whether they are handwritten prescriptions or computer-assisted prescriptions. Indeed, the combination of amiodarone and escitalopram can appear on handwritten prescription because of prescriber’s lack of knowledge. With CPOE, CDSS tool can alert on drug–drug interaction. However, high frequency of alerts and dozens of daily interruptions for clinicians are responsible of ‘alert fatigue’ and practitioners override alerts.24 We can also find duplicate orders, meaning the same drug is prescribed twice. With predefined order set, it is common to have 8 g of paracetamol per day prescribed. Duplication errors are partially explained by the fact that many screens are required to view patient medications, making intrinsically difficult to spot duplicates.25
Supplemental material
Characteristics of all Act-IP observatory PISREs and PIs between 2014 and 2018
Discussion
This study provides an overview of prescription problems related to CPOE systems used in French hospitals. It provides insights into the main situations and medications involved in computer-related prescribing problems detected by pharmacists by providing a broad description of PIs performed during the daily review of routine medication orders. Thus one strength of this study is that it is based on a large number of hospitals scattered throughout France, as no prior study of such extent evaluating PIs in daily practice has been published.
PISRE rate
Our PISRE rate (8.2%) is within the range reported by Korb-Savoldelli et al.19 They analysed peer-reviewed studies (n=14) that quantitatively reported medication-prescription errors related to CPOE. The prevalence of CPOE system-related medication errors relative to all prescription medication errors ranged from 6.1% to 77.7% (median = 26.1% (IQR: 17.6–42.1)) and was less than 6.3% relative to the number of prescriptions reviewed. Ours is the first large-scale descriptive study using an observatory hospital pharmacy practice database to study computer-related prescribing errors.
DRPs induced by CPOE
The main category of DRPs identified as PISREs were supratherapeutic (27.5%, 7436) and subtherapeutic dosage (17.2%, 4646), non-conformity to guidelines/hospitals’ drug formularies (22.4%, 6069) (ie, medication selection non-compliant with the hospital drug formulary) and improper administration (17.9%, 4838) (ie, incorrect or no formulation, wrong timing). According to Korb-Savoldelli et al all studies reported ‘wrong dose’ and ‘wrong drug’ errors,19 with the ‘wrong dose’ error being that most frequently reported (from 7% to 67.4%, median = 31.5% (IQR: 20.5–44.5)). Many of the prescription errors due to CPOE systems can have serious consequences for patients, depending on the clinical circumstances. Although some of are unlikely to occur (eg, IV ketoprofen 150 ampoules/day instead of 150 mg/day), they nevertheless illustrate flaws in certain CPOE systems.26 However, our data do not allow the discrimination between software errors, connection problems and human error.
CPOE systems
The proportion of PIs triggered by software-related prescription errors was higher for non-certified (9.4%) than certified software (5.5%). In France, certification tests produced by the HAS are intended to technically assess the functionality of the software in various situations, as the CPOE evaluation methodology simulates various clinical scenarios.27 French regulations do not require CPOE developers to carry out usability studies before the systems are marketed. Nevertheless, despite the limitations of this type of certification criteria, which have already been highlighted,28 our results show that prescribing with CPOE-certified systems results in fewer prescription errors than prescribing with non-certified software. These results are consistent with those of other studies, i.e. all software is not equal and some is safer than others.29–31
Prescribers
The PISRE ratio was higher for prescriptions made by graduate prescribers (8.4%) than medical residents (7.8%) (p<0.001). This finding is, at first glance, counterintuitive, as one would expect that a prescriber who has been practising for several years in the same health facility would make fewer CPOE-related prescription errors with the software than a resident who has only been using the software for a few months. Observational studies show that medical residents make most prescriptions and transcribe them to the software prescription instructions of senior prescribers during the medical examination.32 It is thus possible that, in some hospitals, senior physicians are only occasional users of the prescription software. According to Nerich et al the occasional use of software (<1 prescription per day) is a risk factor for prescription error (OR=3.85, 95% CI 2.08 to 7.14).33 Tolley described how a junior doctor remarked that there was no one he could ask for help with using the ePrescribing system, as he was ‘the most experienced person on this floor with regards to the ePrescribing system’. She also described how one consultant admitted she had not ‘learnt how to prescribe properly’ because she did not ‘use the system often enough and regularly enough to know the quirks and tweaks’. This consultant relied on her junior staff to prescribe on the system.34
Act-IP pharmacist’ users
The PISRE ratio for senior pharmacists (9.2%) was higher than that of pharmacy residents (5.4%). This is consistent with the results of a study performed in a UK teaching hospital showing that the likelihood of senior pharmacists identifying errors was greater than that of junior pharmacists35 and in accordance with our expectations. A study concerning French pharmacy students showed that they trust the contribution of computerisation to healthcare without critical analysis. This results in overconfidence in the computer tool, perceived to be reliable, and makes users less willing to search for the errors produced by this tool.36 They are therefore not aware that the review of computerised prescription orders requires additional effort to identify prescription errors. This is the consequence of the lack of teaching/training about this subject in French pharmacy schools. This situation contrasts strikingly with the content of the curricula taught in the UK and USA, for example.37 38
Prescriber acceptance rate
The rate of acceptance of PISREs by prescribers was 78.9% vs 67.6% for other PIs. This suggests that prescribers recognise the relevance of such interventions due to the potential clinical consequences of such prescription errors. This rate varies from 65.9% to 92% in studies of drug errors induced by computerised prescription,10 14 suggesting that physicians consider the potential clinical consequences of SRE to patients to be more frequently serious than interventions unrelated to CPOE. In light of our findings, a CPOE-related prescription error is a factor that favours acceptance of the PI. These points warrant further studies.
Limits
Our study had several limitations. First, our work is based on declarative data. These interventions are performed by hospital pharmacist and entered on Act-IP website on a voluntary basis. Therefore, these PIs highlight prescription problems, but are not exhaustive. Moreover, our team annually analyses the quantitative and qualitative evolution of the data recorded on the Act-IP website (unpublished data). We observed that data entry can be irregular or performed with a delay. Indeed, data can be conditioned by pharmacist workload. For example, many pharmacists record prospectively their data on paper on a daily basis and thereafter register them by series on Act-IP. Data entry can also be total on a given period and can stop during a change of assignment. We consider that these elements have consequences on the quantity of recorded data but not on their quality. However, as illustrated by publications related to other databases on information technology incidents, despite their limitations, studies based on voluntary reports remain relevant to examine the nature of technology safety problems.39 40 Moreover, the large sample size probably provides a relatively precise vision of the problem at the national level. Second, several pharmacists analysing the same drug prescriptions may not all track down the same problems. One of major determinant of a PI is the knowledge of the pharmacist who analyses the prescription. It is this knowledge that enables him to detect a problem. Thus, a PI that is considered as necessary and is not performed means that it is not recorded and will be absent from the database. This happens when a doctor routinely makes a certain type of prescribing error and the pharmacist fails to detect it.41 It has been shown that, if several pharmacists analyse the same drug prescriptions, they do not all track down the same problems. In a study involving 57 hospital pharmacies, the mean percentage of detected prescribing errors was 59%, with a broad range of 7%–88% between pharmacies.42 In the absence of specific studies to determine the performance of pharmacists in detecting prescription errors induced by CPOE-system flaws and misuse, we are reduced to simply assuming that such variation may be observed. In addition, there are various definitions of PISREs in the literature.13–16 This suggests that there is a certain level of subjectivity when a pharmacist characterises a PI as being related to a computer-generated prescription. Among hospitals that entered the PIs on Act-IP, 87 never qualified a PI as being an SRE. There are two possible explanations for this observation. The first, and relatively unlikely, is that the software is near perfect and that there was no misuse by prescribers. For example, the absence of PISREs for these hospitals could result from the absence of computer-related errors due to the use of high-performance software and/or appropriately trained prescribers. The second possibility is that pharmacists do not establish a link between certain prescription errors and misuse of the prescription software and/or its design flaws. Conversely, a high rate of PISREs for a given hospital may result from software conception flaws and/or misuse of the software by prescribers and pharmacists who are very aware of the role of CPOE-systems in generating prescription errors. Regardless of the considered scenario, it is important to remember that differences in PISRE rates may also be due to the quality of the training provided. Studies have shown that insufficient training on an ePrescribing system can contribute to errors.43 44 Tolley illustrated how pharmacists did not receive any formal training about the system after starting at a hospital trust and observed that no formal training was offered when pharmacists changed roles. It has been shown that training plays a role in the users’ experience but there is a lack of published research in this area.34 Thus, further research is warranted to lift the veil on these unknowns.
Our results highlight that prescribing problems related to computer software are common in France. This is a concern that affects most (if not all) CPOE systems currently being used and therefore all hospitals, to varying degrees. Identifying the most dangerous software appears to be a priority to improve the quality and safety of patient care.
Conclusion
Computer-related prescribing errors are common, with wrong dose being the most frequent type of error. Such errors concern all drug classes and have potentially serious adverse clinical consequences if they are not intercepted by pharmacists when performing their daily medication review. The message appears to be well received by prescribers who agree to change their prescription more frequently than for PIs not related to CPOE use. CPOE medication review requires additional pharmacist diligence to catch such errors. As the PISRE ratio is significantly lower for certified software, patient safety agencies should undertake studies to identify the safest software so as to discard software that is potentially dangerous.
Data availability statement
Data are available on reasonable request. Deidentified participant data are available upon reasonable request to Act-IP© Administrator (email address : actip@sfpc.eu).
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval for the study was obtained on 19 February 2020 (CECIC Rhône-Alpes-Auvergne, Clermont-Ferrand, IRB 5891).
Acknowledgments
The authors would like to thank the team of THEMAS and VIP working group for assistance in this project. We thank the clinical pharmacists of the SFPC Act-IP group who participated in the data collection. Members of the working group ‘Valorization of Pharmaceutical Interventions/ Valorisation des Interventions Pharmaceutiques – Act-IP’ of the French Society for Clinical Pharmacy: Pierrick Bedouch (Grenoble), Magalie Bourdelin (Villefranche-sur-Saone), Bruno Charpiat (Lyon), Ornella Conort (Paris), Julien Gravoulet (Leyr), Audrey Janoly-Dumenil (Lyon), Michel Juste (Epernay), and Céline Mongaret (Reims). We thank Kévin Mastrorillo, technical consultant of the Act-IP observatory, for his contribution to the data extraction and data management.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Clinical pharmacists of the SFPC Act-IP group who participated in the data collection: S. Abkhtaoui-Couriat (Corbie), B. Allard-Latour (Saint-Genis-Laval), C. Andrieu (Saint-Etienne), X. Armoiry (Lyon), E. Armoiry (Villeurbanne), D. Attivi (Neufchâteau), L. Audibert (Alix), A. Barbet (Amiens), M. Bascoulergue (Aulnay sous bois), C. Basselin (Saint-Genis-Laval), F. Baud (Paris), P. Bedouch (Grenoble), M. Belhout (Amiens), S. Benhaoua (Saint Denis), J. Beny (Alix), S. Berthet (Lyon), J. Berthou (Besancon), D. Bichard (Besancon), A.C. Blandin (Besancon), E. Blondel (Aix les Bains), S. Bonn Loue (Luneville), A. Bonvin (Lyon), F. Bouchand (Garches), P. Bouniot (Francheville), M. Bourdelin (Besancon), C. Bouret (Lyon), L. Bourguignon (Lyon), C. Bourne (Saint-Egrève), M. Bouteille (Lyon), J. Burdin (Lyon), C. Bureau (Alix), C. Bureau (Villeurbanne), M. Burgin (Luneville), M. Buyse (Paris), E. Cabaret (Hyeres), D. Cabelguenne (Pierre Benite),C.Capele (Saint André lez Lille), D. Carli (Vienne), I. Carpentier (Saint-Genis-Laval), E. Chambrey (Rang-du-Fliers), S. Chantel (Pierre Benite), N. Charhon (Vienne), B. Charpiat (Lyon), M. Chaumont (Le Chesnay), K. Civiletti (Martigues), B. Clerc (Besancon), M. Cleve (Vienne), R. Colomb (Saint-Etienne), C. Combe (Saint-Etienne), O. Conort (Paris), R. Contreras (Besancon), S. Crepin (Limoges), M. Creusat-Aube (Illkirch-Graffenstaden), A. Cuoq (Lyon), C. Decourcelle (Lomme), T. Delanoy (Vienne), C. Derharoutunian (Vienne), A. Deronze (Lyon); M. Desseignet (Lyon), S. Diallo (Le Chesnay), L. Dietrich (Strasbourg), A. Dory (Strasbourg), J. Dos-Reis (Paris), N. Duarte (Draveil),M.O. Duzanski (Strasbourg), L. Escofier (Mayenne), F. Fabre (Clermont-Ferrand), S. Fare (Paris), J. Fillon (Paris),A. Fonteneau (Amiens), A. Fouquet (Vienne); A. Gadot (Lyon), H. Galtier (Vienne); I. Garreau (Epernay), C. Gerard (Francheville),R. Gervais (Saint Denis), O. Gloulou (Saint Denis), I. GraguebChatti (Vienne), A. Grass (Lyon), I. Gremeau (Clermont-Ferrand), P.Y. Grosse (Grasse), C. Guenaire (Rennes), F. Guerin (Aix les Bains), A. Guillermet (Lyon), S. Hannou (Illkirch-Graffenstaden), A. Henry (Lyon), G. Herbin (Bayeaux),N. Herment (Epernay), A. JanolyDumenil (Pierre Benite), C. Jarre (Vienne), L. Jovenaux (Martigues), M. Juste (Epernay), A.S. Kaczmarek (Clermont-Ferrand), W. KiniMatondo (Saint Denis), H. Labrosse (Lyon), C. Laillier (Strasbourg), E. Lamarre (Saint-Etienne), J. Lamoureux (Lyon), M. Laurent (Lyon), A. Le Bris (Le Chesnay), M. Le Duff (Rennes), R. Lecointre (Saint-Etienne), J. Lecompte (Grasse), M. Lefebvre (Lyon), A.L. Lepetit (Epernay), H. Lepont-Gilardi (Rennes), A. Lescoat (Villeurbanne), J.P. Levillain (Migennes), G. Liguori (Clermont-Ferrand), C. Lohier (Villeurbanne), C. Lupo (Lyon), J. Machon (Lyon), K. Maes (Vienne), G. Magerand (Villeurbanne), K. Mangerel (Epernay), S. Martelet (Saint-Etienne), D. Matanza (Francheville), V. Mermet (Saint-Genis-Laval), C. Mouchoux (Villeurbanne), Y. Nivoix (Strasbourg), A. Orly (Paris), E. Orng (Lyon), A. Oufella (Aulnay Sous Bois), I. Paillole (Toulouse), D. Pallot (Saint Denis), A. Papon (Lyon), L. Parnet (Paris), M. Paysant (Saint-Genis-Laval), E. Perrier-Cornet (Illkirch-Graffenstaden), S. Perrin (Besancon), D. Peynaud (Lyon), B.N. Pham (Vienne), D. Piney (Luneville), A. Pohyer (Montpellier), C. Porot (Besancon), J. Pouzoulet (Créteil), L. Poy (Lyon), E. Prevost (Epernay), E. Prunier (Besancon), F. Ranchon (Lyon), M. Rave (Besancon), C. Remonnay (Besancon), M. Remy (Ho-Chi-Minh Ville), M. Rhalimi (Chaumont-en-Vexin), C. Rioufol (Pierre Benite), A. Robelet (Paris), S. Roche (Epernay), F.X. Rose (Saint-Avé), R. Roubille (Vienne), A. Sambarino (Bourgoin Jallieu), D. Sankhare (Saint Denis), R. Santucci (Strasbourg), J. Scholler (Strasbourg), R. Selmi (Saint Denis), C. Stamm (Pierre Benite), C. Tanguy (Brest), D. Tessier (Saint Denis), H. Thery (Rang-du-Fliers), N. Thiriat (Paris), C. Turci (Saint-Genis-Laval), N. Vantard (Lyon), N. Vauvarin (Joigny),S.Vernardet (Annonay), D. Viard (Besancon), C. Vignand (Lyon), C. Villa (Vienne), P. Vonna (Epernay), S. Wacker (Strasbourg), N. Wereszczynski (Grasse), and L. Zerhouni (Paris).
Contributors MV and BC designed the study, performed the statistical analyses, interpreted the results and wrote the first version of the manuscript. CV contributed to the design of the study, performed the statistical analyses and revised the manuscript. J-LB contributed to the design of the study and revised the manuscript. OC contributed substantially to the interpretation of the data and contributed to the revision of the manuscript. PB designed the study, performed the statistical analyses, interpreted the results and revised the manuscript.
Funding This study was supported by The French Society of Clinical Pharmacy, a nonprofit and independent foundation for clinical pharmacy research and development.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.