Article Text

Abstract
Introduction There is limited evidence regarding the effectiveness of timely integration of short-term specialised palliative care services for older people in primary care. Using a Theory of Change approach, we developed such an intervention, the Frailty+ intervention. We present the protocol of a pilot randomised controlled trial (RCT) with a process evaluation that aims to assess the feasibility and preliminary effectiveness of the Frailty+ intervention.
Methods and analysis We will conduct a pilot RCT in Flanders, Belgium. Frail older people who are discharged to home from hospital will be identified and recruited. Seventy-six will be randomly assigned either to the control group (standard care) or the intervention group (Frailty+ intervention alongside standard care). Data will be collected from patients and family carers. At the core of the Frailty+ intervention is the provision of timely short-term specialised palliative care facilitated by a nurse from the specialised palliative home care service over a period of 8 weeks. We will assess feasibility in terms of recruitment, randomisation, acceptability of the intervention, retention in the programme and data completion. The primary outcome for assessing preliminary effectiveness is a mean score across five key symptoms that are amenable to change (ie, breathlessness, pain, anxiety, constipation, fatigue), measured at baseline and 8 weeks post-baseline. The process evaluation will be conducted in the intervention group only, with measurements at 8–11 weeks post-baseline to evaluate implementation, mechanisms of change and contextual factors.
Ethics and dissemination The study has been approved by the ethics committee of University Hospital Ghent. Results will be used to inform the design of a full-scale RCT and will be published in a peer-reviewed, open access journal.
Trial registration number ISRCTN39282347; Pre-results.
- palliative care
- primary care
- adult palliative care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The timely short-term specialised palliative care service intervention was developed and modelled through synthesising evidence from a systematic literature review with qualitative research, including perspectives of older people, family carers and professional stakeholders (eg, formal care providers, researchers, policy-makers), integrated in a Theory of Change.
Thorough piloting of the intervention will ensure feasibility and acceptability of the intervention, the randomised controlled trial design and procedures and will facilitate determining the required sample sizes for future full-scale evaluations.
We will conduct an in-depth process evaluation that has a vital role in understanding the feasibility and acceptability of the intervention and in optimising its design and evaluation.
We will include a diverse population of frail older people, including patients without cognitive capacity who are often under-represented in clinical studies.
We translated measures for the primary and secondary outcomes that were not available in Dutch by using forward-backward procedures; however, a formal validation of these measures in Dutch does not exist.
Introduction
A growing number of people worldwide are living into old age, yet the added years of life are not always spent in good health1; many experience long periods of illness and multimorbidity (ie, the simultaneous presence of multiple chronic conditions) or frailty. Different conceptualisations and operational definitions are used to define frailty, although many focus on the physical/medical domain of frailty. Some also include other domains such as the psychological and social.2–4 In this study, we use the definition of the British Geriatrics Society, defining frailty as ‘a distinctive health state that is related to the ageing process in which multiple body systems gradually lose their inbuilt reserves’.2 Frailty is a common condition in old age, and an estimated 26% in those aged 80 and over are frail.5 The increased susceptibility of frail older people to adverse health outcomes paired with the cumulative effects of various chronic health problems results in prolonged, complex and fluctuating needs and symptoms in the last years of life.6 7 As populations are ageing, the number of frail older people with such complex needs and symptoms is expected to rise considerably in the near future. Although these problems are known, evidence is lacking regarding which interventions are effective in addressing the resulting needs. Hence, there is an urgent need to develop and evaluate interventions that can improve care for frail older people towards the end of life.
Palliative care is suggested by the WHO as a way to address the problems associated with life-threatening illness by means of early identification, assessment and treatment of physical, psychosocial and spiritual problems.8 However, it has traditionally been limited to patients with cancer and is often started in the terminal phase. Over the past decade, the WHO, researchers and clinicians have made strong calls for it to be initiated early in the course of any serious or advanced illness, even alongside life-prolonging treatments, to improve quality of life.7–9 Nevertheless, research shows that access to palliative care is lower for older than for middle-aged and younger people10 and is often initiated only shortly before death (eg, the median number of days ranged from 15 in Belgium to 30 in Italy in a four-country comparison11). Frail older people may benefit from timely initiation of palliative care, especially in the community setting, as the majority of older people prefer to live at home as long as possible.12
Two complementary palliative care service models have been advocated across patient populations: generalist palliative care from healthcare professionals who provide basic management of symptoms, and specialised palliative care from a multidisciplinary service or a clinician whose core activity is to support primary care professionals in caring for patients and family carers.13 14 In particular at times when palliative care needs become too complex to be handled by generalist providers alone, the involvement of specialised palliative care services is recommended.13 14 The EAPC Atlas of Palliative Care showed that, although typology varies, similar services are established in most European countries.15
Building on an integration of generalist and specialised palliative care, a new model of short-term integrated palliative and supportive care for people with multiple sclerosis has demonstrated feasibility and beneficial outcomes.16 17 This model consisted of episodic involvement of a specialised palliative care service integrated with existing primary care providers.16 17 It has also been proposed for older people with frailty or other progressive conditions.18–21
This protocol concerns a pilot randomised controlled trial (RCT) with a process evaluation that aims to assess the feasibility, acceptability and preliminary effectiveness of a timely short-term specialised palliative care service intervention for frail older people and their family carers in primary care (henceforth named the Frailty+ intervention). We will conduct a pilot RCT as there is currently insufficient evidence on the feasibility and acceptability of such an intervention and RCT design.
Additionally, we will seek to answer the same research questions in the specific population of frail older people with a cancer diagnosis. This subanalysis is part of a research project (with LP as PI) linked to this pilot RCT. While previous studies have shown that palliative care, including early palliative care, can improve key symptoms in people affected by cancer,16 22 23 they have not tested whether this also applies to the specific health problems and disease trajectory experienced by older people with cancer. The cancer trajectory in older people is considerably different from that of younger patients. An estimated 80% of people aged over 85 experience multimorbidity24; 43% of cancer patients aged 70 or over are frail.25 Moreover, cancer and cancer treatment can worsen a number of geriatric syndromes (eg, bone loss, anaemia, depression, fatigue, insomnia).26 The cumulative effects of these conditions can lead to complex and unpredictably fluctuating symptoms over the course of several years.7 It is, therefore, important to test whether a timely short-term specialised palliative care service can be beneficial in this patient group as well.
The specific objectives of the pilot RCT are:
To pilot the Frailty+ intervention and evaluate its implementation, mechanisms of change and contextual factors potentially affecting implementation and outcomes.
To test the feasibility of the methods and procedures of the RCT.
To evaluate the preliminary effectiveness of the Frailty+ intervention in frail older people, with and without cancer, and their family carers.
Methods and analyses
In describing the study protocol, we followed the Standard Protocol Items of the Recommendations for Interventional Trials 2013 Checklist27 and the Consolidated Standards of Reporting Trials 2010 checklist.28
Study design
We will conduct a pilot RCT with two parallel groups (38:38 patients) and an embedded process evaluation. The intervention group will receive the Frailty+ intervention in addition to standard care. The control group will receive standard care. Patients who consent will be randomly assigned to one of the study arms after baseline assessment. The assessments will be conducted at baseline and 8 weeks after the baseline measurement. Data will be collected from patients and their family carers.
Study setting
In Belgium, multidisciplinary and trained teams of healthcare professionals are the main providers of specialised palliative care at home. Their main goal is to advise general practitioners (GPs), healthcare professionals, counsellors, informal carers and volunteers involved in the provision of palliative home care of a patient and to organise and coordinate the provision of palliative care at home between different care providers.29 The GP’s approval is required to initiate this service,29 usually consisting of nurses, a psychologist and a palliative care physician and covering a geographical region. The intervention in this study will be conducted in Flanders, the Dutch-speaking region of Belgium, in cooperation with two specialised palliative home care services. Recruitment of patients will be done via three hospitals in Flanders, one of which is a university hospital.
Eligibility criteria
Patients will be recruited on discharge from a hospital admission. The inclusion and exclusion criteria for patients are provided in table 1. For the specific recruitment of frail older people with cancer (as specified above), we will apply an additional criterion based on a previous study of early palliative care in oncology.30 Additionally, patients will be asked to indicate their most important family carer. The inclusion and exclusion criteria for family carers are provided in table 2.
Inclusion and exclusion criteria for patients
Inclusion and exclusion criteria for family carers
Treatment arms
Standard care (control) group
Patients in the control group will receive standard care from primary care providers (eg, GP, district nurses) and any specialists. If a patient is referred to a specialised palliative home care service as part of standard care within their follow-up period (8 weeks), we will exclude them from the study.
Intervention group
We have developed and modelled the Frailty+ intervention, using a theory-based development approach (Theory of Change) integrated with the UK Medical Research Council (MRC) framework for developing and evaluating complex interventions.31–34 As part of this, we integrated the evidence of a previously conducted systematic literature review of specialised palliative care services for older people in primary care20 with qualitative research, including qualitative interviews and group discussions with older people and family carers, Theory of Change workshops with professional stakeholders (ie, bringing together key professional stakeholders to develop a Theory of Change map and to encourage stakeholder buy-in31) and research group meetings.
The Frailty+ intervention will be provided alongside any standard care. The core component of the Frailty+ intervention consists of the provision of timely short-term specialised palliative care, facilitated by a nurse from the specialised palliative home care service over a period of 8 weeks; care should be holistic and based on needs as well as capacities; it should be person-centred and family focused as well as goal-oriented and proactive; collaboration and integration with other healthcare professionals is essential (see box 1 for more information on each component). Additional implementation components are added to this to ensure optimal implementation. They include informing, engaging and training of professionals involved in primary and secondary care in the intervention region and identification and referral of frail older people with complex unresolved symptoms who have been hospitalised and are referred home, and of their family carers.
Description of the core component of the Frailty+ intervention
Timely integration of short-term specialised palliative care service: 1–4 home visits with, if needed, additional phone follow-up, over a period of 8 weeks.
Holistic needs-based and capacity-based care: identifying and managing support needs in the four palliative care domains that is, physical, psychological, social and existential/spiritual and focusing on disabilities as well as functioning and capacities (strengths and deficits).
Person-centred and family focused: viewing family as both care recipients and care providers.
Goal-oriented and proactive care: focus on the patient’s individual health and care goals across several health, life and care domains; supporting the patient in defining and meeting realistic or attainable goals and determining how well these goals are being met. This also includes the initiation of advance care planning conversations and drafting an emergency response plan and out-of-hours plan.
Collaborative and integrative working: focus on multiprofessional and multidisciplinary collaboration, coordination and continuity of care from the perspective of the patient and family. This includes the organisation of at least one multidisciplinary face-to-face meeting with healthcare professionals involved in the patient’s care and appointing a key health professional for the patient and family within the primary care team who coordinates care within the multidisciplinary team.
Timing of intervention
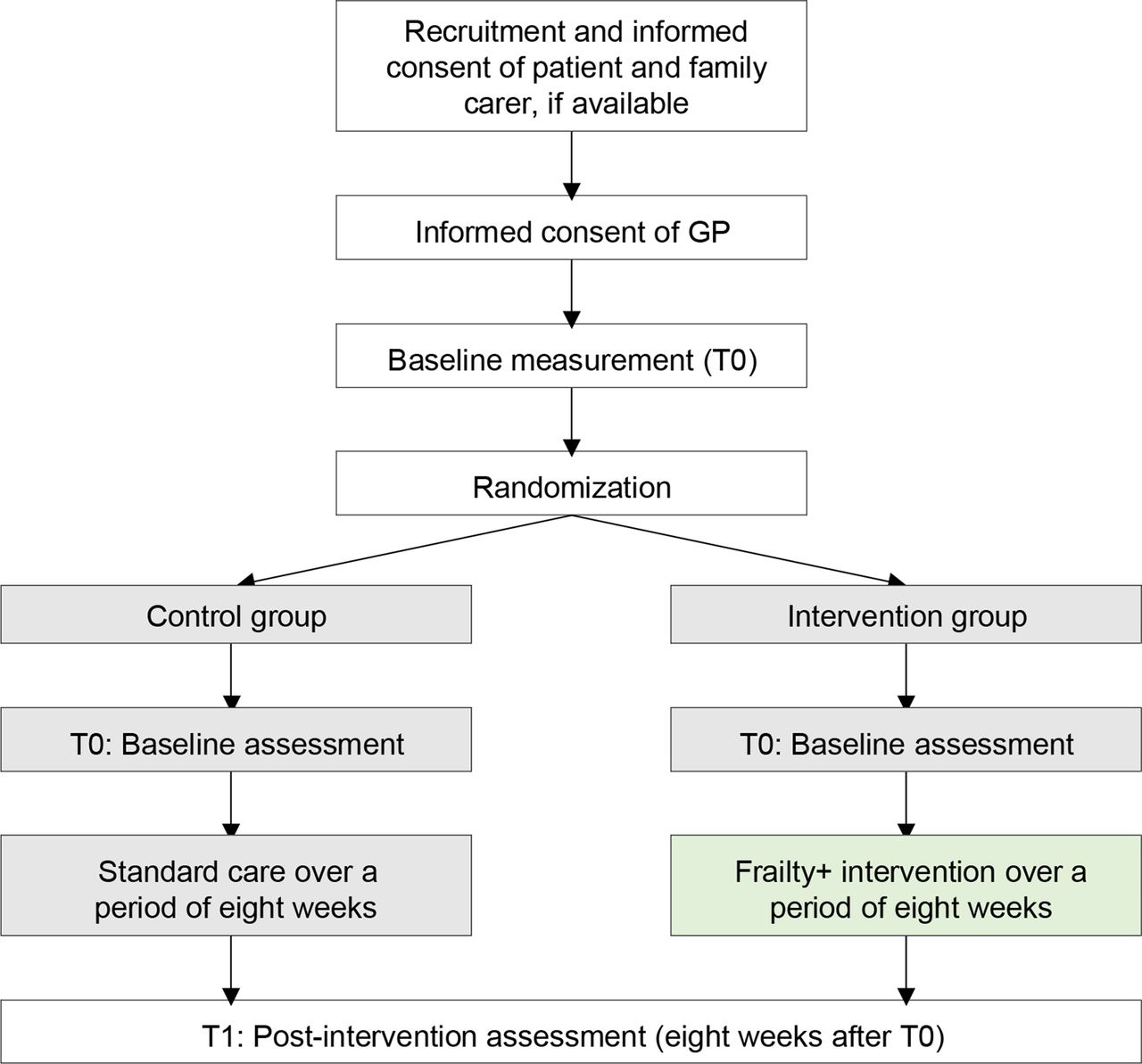
The first home visit will take place within five working days after discharge from the hospital. The additional visits and the multidisciplinary meetings will be planned by the nurses from the specialised palliative home care service with each patient and family individually. We foresee at least one and on average three to four home visits per patient and additional telephone calls, if needed, over a period of 8 weeks. An overview of the participant flow through the pilot RCT is displayed in figure 1.

{kind=link}
Flow chart of participant flow through pilot RCT. GP, general practitioner; RCT, randomised controlled trial.
Outcomes and data collection
Objective 1: pilot the Frailty+ intervention and evaluate its implementation, mechanisms of change and contextual factors affecting implementation and outcomes
To address objective 1, we will conduct a process evaluation, guided by the MRC process evaluation framework,35 to evaluate the following:
Components and activities that were delivered as part of the Frailty+ intervention, their ‘dose’ or ‘quantity’, and the adaptations that were made to the initial intervention description.
Views of and experiences with the timely short-term specialised palliative care service intervention, according to healthcare professionals (palliative home care services, GPs, geriatric liaison teams, geriatricians), patients and family carers.
Occurrence and type of unexpected or adverse effects, according to healthcare professionals (palliative home care services, GPs, geriatric liaison teams, geriatricians), patients and family carers.
Which external factors, if any, influenced the implementation and outcomes of the Frailty+ intervention according to healthcare professionals (palliative home care services, GPs, geriatric liaison teams, geriatricians), patients and family carers.
The process evaluation focuses on the intervention so will be carried out in the intervention group only. We will use a mixed-methods approach, integrating quantitative and qualitative data. The data will be collected by the researcher and the data manager prior to recruitment and eight to eleven weeks after baseline (ie, at T1). The quantitative data will be collected through registrations in standardised documents developed by the researchers and by the use of a structured data extraction form to scan electronic patient records. The qualitative data will be collected through semistructured qualitative interviews and focus groups. The interviews and focus groups will be audio recorded and transcribed verbatim by the researcher. An overview of the data that will be collected and the methods and timing of data collection is given in table 3.
Process evaluation: data collected, methods and timing
Evaluation of care delivered in control group
In order to evaluate and explore care in the control group, the researchers will conduct telephone interviews with the GP 8 weeks after the baseline measurement (after postintervention assessment) to obtain the following information: which care providers delivered care and where (eg, home, hospital); number of visits or consultations (by GP and other healthcare professionals), topics discussed, if any multidisciplinary meetings were organised (and if so, who attended and which topics were discussed).
Objective 2: to test the feasibility of the methods and procedures of the RCT
The feasibility of the RCT methods and procedures will be tested in the intervention and control group using a mixed-methods approach, integrating quantitative and qualitative data (see table 4 for detailed information). The data will be collected by the researcher, the data manager and the hospital staff involved in patient recruitment. The quantitative data will be collected through registrations in standardised forms developed by the researchers. The qualitative data will be collected through semistructured qualitative interviews and focus groups.
Feasibility of the methods and procedures: operationalisations and data collection methods
Objective 3: to evaluate the preliminary effectiveness of the Frailty+ intervention in frail older people
The evaluation of preliminary effectiveness will be carried out by comparing the intervention and control groups (see table 5 for details). We will measure the primary and secondary outcomes using structured questionnaires (administered in interview format). The data will be collected by the researcher and data manager at T0 and T1 from patients and family carers at a place and time of their preference. Respondents will be interviewed separately (or together, if they prefer). The primary outcome is the mean score across five key symptoms that are amenable to change (ie, breathlessness, pain, anxiety, constipation, fatigue) as measured using the integrated Palliative care Outcome Scale (iPOS). The iPOS is a validated questionnaire with good psychometric properties.36 37
Primary and secondary outcomes and respective measures to pilot the RCT and assess preliminary effectiveness
In addition, we will measure exploratory outcomes (ie, outcomes that are used to frame future research questions or explore new hypotheses38) using a mixed-methods approach, integrating quantitative and qualitative data (see table 5). These data will be collected by the researcher and the data manager at T1 only. The quantitative data will be collected through structured phone interviews and the qualitative data through semistructured qualitative interviews and focus groups. The qualitative interviews and focus groups will be audiorecorded and transcribed verbatim by the researcher.
For all participating patients, we will register basic sociodemographic data (ie, gender, age, educational attainment, current or previous professions) and aspects of their social situation (ie, living situation, marital status, number of children, geographical proximity and contact frequency with family and friends). Age at baseline, gender and medical diagnosis data will be taken from the patient medical file by hospital staff, other sociodemographic data at the T0 interview. We will also collect basic sociodemographic data of the family carer (ie, gender, age, relation to the patient) during the interview at T0.
Pretesting of questionnaires
The questionnaires to assess the primary and secondary outcomes from patients and family carers will be translated from English into Dutch, where necessary, using forward-backward procedures and pretested with five patients and five family carers (or until data saturation is reached). Participants for pretesting will be identified according to inclusion and exclusion criteria as described in tables 1 and 2 and will be recruited at one of the participating hospitals.
Capacity and proxy measurements
If a patient does not have the capacity to consent to participation (according to the clinical judgement of the treating physician, see recruitment section for evaluation of cognitive capacity) at T0 and/or at T1, a proxy respondent will be identified following stipulations of Belgian law concerning representatives of people lacking cognitive capacity.39 The first choice is the patient’s legal representative; if none has been assigned, this will be the person named in the will as executor.39 Only when there is no person named as executor, the representative is the spouse or any other beneficiary.39 For data collection with proxy respondents, a proxy version of the patient questionnaire will be used.
Sample size
The main objective of this pilot RCT is to assess feasibility and acceptability of the intervention, and of the RCT methods and procedures. As determining effectiveness is not the main objective, sample size calculations seem of less importance.40 41 Nevertheless, we have conducted a provisional sample size calculation to allow the reader to interpret our analysis of preliminary effectiveness of the Frailty+ intervention based on the only similar RCT available at time of development (follow-up periods and the patient population differ to some extent).42 The intervention will be evaluated in two groups: frail older people and frail older people specifically with a cancer diagnosis. We aim to include 50 eligible patients, 25 in each study arm; it is estimated that this will allow us to detect differences of >1.6 on the Palliative Outcome Scale (for individual items) at α=0.05 and power 1-β=0.80.42 After the target sample has been reached, we will sample an additional 25 frail older people who have a cancer diagnosis in order to achieve a sample of N=50 frail older people with cancer (based on the estimate that around half of those included will have a cancer diagnosis; clinical estimate based on patient numbers at the participating university hospital). The total sample will, therefore, be N=76 (rounded up to an even number). To allow for an expected attrition of 45%, we plan to recruit at least 139 patients.
Recruitment
Patients will be recruited at the acute geriatric department and through the geriatric liaison teams of several hospitals in Flanders. Each hospital will assign one staff member as contact person; the treating physician will judge if a patient meets the inclusion criteria and will ask them if they will agree to a researcher visiting them to introduce the study; if so, the treating physician or contact person will inform the research team. Once every 3 weeks, the researcher or data manager will attend the multidisciplinary meeting at the acute geriatric department in each hospital to ensure that all eligible patients are offered the opportunity to participate in the study.
On their initial visit, the researcher will inform the patient about the details of the study and what participation entails. They will explain the term ‘specialised palliative care service’ (ie, an additional service that is often provided at the end of life for people with advanced serious illnesses but may be beneficial also at earlier stages of illness), and that this study aims to test whether timely provision would be feasible and acceptable and beneficial for older people discharged from the hospital. If the patient agrees to participate, the researcher will ask them to provide written informed consent and indicate their most important family carer (if they have one and conforming to inclusion and exclusion criteria) and whether they can be contacted for participation in the study. They will then visit the family carer to inform them about the study and obtain written informed consent. They will also ask the patient for permission to contact their GP to introduce the study and obtain their written informed consent to participate in the study.
If the patient does not have cognitive capacity (according to the clinical judgement of the treating physician) a proxy respondent will be approached (for details on this procedure, see outcomes and data collection section). It is important to test the Frailty+ intervention in those without cognitive capacity too as they form a large proportion of the older population43 ensuring that the conclusions apply to this population as well.
Patients randomised to the intervention group will be referred to the specialised palliative home care service by the researcher which will then obtain a formal referral from the GP, as required in the Belgian healthcare system. In case the patient is randomised to the control group, the GP will be informed and will provide standard care.
Patient recruitment started in January 2020 and is expected to end in December 2020 (last patient follow-up ends in February 2021). Due to COVID-19, recruitment was suspended between 13 March and 9 June 2020. We will adapt the timing should the crisis cause further delays.
Randomisation and blinding
Patients will be randomised in a 1:1 ratio to receive either the Frailty+ intervention or standard care. We will use a block randomisation technique with a variety in blocks, in order to reduce potential bias (ie, the variety in blocks prevents the researcher being able to predict which group the patient will be referred to) and achieve balance in allocation of patients to the intervention and control arm which will be done randomly by an external researcher independent of the research team for this study. This is an unmasked trial. The researchers involved in data collection cannot be blinded in this pilot RCT as the process evaluation is conducted in the intervention group only.
Analysis
Process evaluation and feasibility
The data collected via the standardised documents and the structured data extraction form developed by the researcher will be described using descriptive summary statistics (mean, SD, percentages). All qualitative data will be analysed by using thematic content analysis (ie, inductive coding into themes).44 One researcher will read the transcripts carefully several times to have a sense of the data, with a sample checked by another researcher. Both researchers will independently conduct the preliminary analysis by generating initial codes and converting them into categories that represent the main themes and categories arising from the data. The identified themes and categories will be compared, and in case of disagreement, a third reviewer will reconcile any discrepancies. Subsequently, meetings with the research team will enable consensus to be reached on the themes and categories. The analysis will be conducted in the original Dutch language, and final themes and categories (as well as selected quotes) will be translated to English by one researcher in cooperation with a professional translator.
Preliminary effectiveness
We will calculate summative scale scores for the primary and secondary outcomes. The resulting scale score for an individual is the sum of the individual item scores. If more than 25% of the items per scale were not answered (ie, missing), no sum score will be calculated for that scale and will be defined as missing. The pilot RCT data will be analysed on ‘intention-to-treat’ principle. This means that all patients who were enrolled and randomised will be accounted for in the main analysis, regardless whether they completed the Frailty+ intervention or not. The characteristics of patients in the intervention and control group will be described using descriptive summary statistics. We will test for differences in the primary and secondary outcomes between the groups at baseline and 8 weeks later (ie, T1). Linear mixed-model analyses will be used with treatment, time and treatment-by-time interaction as independent variables and with two random factors, one for clustering of patients within hospitals and one for clustering of the two measures within patients. Linear mixed models handle missing data through maximum likelihood estimation, so no missing data imputation method will be applied. All significance tests will be two tailed and assessed at the 5% significance level. The quantitative exploratory data will be described using descriptive summary statistics and the qualitative data using thematic content analysis. All analyses will be conducted in IBM SPSS v25 and R.
Patient and public involvement
Patients and family carers were involved in the design of the study.
Ethics and dissemination
Ethics approval and consent to participate
The study has been approved by the ethics committee of the University Hospital Ghent. In line with the General Data Protection Regulation (GDPR) guidelines of May 2018, an internal register will provide all required information on for example, the purposes of all processing operations; a description of the categories of data subjects and the recipients or categories of recipients to whom the data are disclosed; the legal basis of the processing operation for which the data are intended (the detailed internal register of all procession operations will also be sent to the Data Protection Officer of the University Hospital Ghent). In order to protect participants’ rights, information materials and informed consent forms are carefully formulated and structured to ensure that participants know exactly what participation in the study entails.
Distress protocol
The contact details of the researchers are mentioned on all information letters, consent forms and questionnaires. This allows the participants to contact the research team in case they feel the need to do so. In case a specific concern arises, the researcher will examine, together with the patient and family carer, which of their regular healthcare professionals is available to provide professional help and/or support. In addition, a psychologist from our research group (external to this project) will be available to provide support during the study period.
Confidentiality
The collected and transferred data will be pseudonymised to ensure that participants’ privacy and personal information are protected (eg, all personal information that can lead to identification of the patient or the family carers is changed into a code by those that perform the data entry, eg, the researchers). We will use sufficient safety measures to protect the data, for example, virtual server firewall and back-up systems and sufficient access controls (ie, ID and ultrahigh password regulator and frequent password changes).
Availability of data and material
The final data set will be available to all researchers involved in this study. After reporting of the results, the data will be stored safely for 25 years, with Prof. Dr. Lieve Van den Block being responsible for their storage. The audio files will be deleted immediately after transcription. Following the publication of the main results of the pilot RCT, the respective data will be made available for non-commercial research purposes upon a reasonable request made to the researchers.
Dissemination
The results of this study (feasibility of the methods and evaluation of the intervention) will be submitted for publication in peer-reviewed journals and will be presented at national and international conferences. Participants and health care professionals involved in the study will be informed about the results in a leaflet. The results of this study will be used to adapt the theoretical model of the intervention and inform the design of a subsequent full-scale effectiveness trial.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Jane Ruthven for linguistic help.
References
Footnotes
KdN and LP are joint first authors.
Twitter @KimNooijer
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors Conception and design of the work: KDN, LP, NVDN, PP and LVdB. Ethics committee application: KDN, LP, NVDN, PP and LVdB. Study registration: KDN, LP and LVdB; Drafting of the article: KDN, LP and LVdB. Critical revision for important intellectual content: NVDN, PP and LVdB. All authors read and approved the final manuscript.
Funding This work was supported by the Research Foundation – Flanders (under grant agreement G.0303.16) and by a Postdoctoral Fellowship of the Research Foundation – Flanders to Lara Pivodic.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.