Article Text

Abstract
Objectives Occupational dust exposure may induce various lung diseases, including pneumoconiosis and chronic obstructive pulmonary disease (COPD). The features of combined COPD and pneumoconiosis have not been well described, and this may hamper the management. This study aimed to describe the prevalence and characteristics as well as the risk factors of the combined diseases.
Design A cross-sectional study.
Setting and participants 758 patients with pneumoconiosis were recruited at a single-medical centre. Of these, 675 patients with pneumoconiosis, including asbestosis, silicosis, coal workers’ pneumoconiosis and other pneumoconiosis, was eligible for analysis.
Primary outcome measures COPD was diagnosed based on clinical features and/or history of exposure to risk factors and post bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio <0.7. Clinical data were collected from predesigned medical reports. The patients underwent both chest radiograph and high-resolution CT scans. Risk factors for combined COPD and pneumoconiosis were analysed using regression analysis.
Results COPD prevalence overall was 32.7% (221/675) and was the highest in silicosis (84/221) and coal workers’ pneumoconiosis (100/221). COPD prevalence increased with smoking pack-years, dust exposure duration and pneumoconiosis stage. Patients with combined diseases had lower body mass index, higher smoking index and worse pulmonary function. Risk factors for combined diseases included heavy smoking, silica or coal exposure and advanced pneumoconiosis. The interaction between dust exposure and smoking in COPD was also identified. The risk of combined COPD significantly increased with heavy smoking and silica or coal exposure (OR 5.49, 95% CI 3.04 to 9.93, p<0.001).
Conclusions COPD is highly prevalent in patients with pneumoconiosis, especially patients with silicosis and coal workers’ pneumoconiosis. Occupational dust exposure as well as heavy smoking is associated with an increased risk of combined COPD and pneumoconiosis, which demands an effective preventive intervention.
- interstitial lung disease
- chronic airways disease
- occupational & industrial medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A cross-sectional study was carried out to describe the prevalence and clinical features of combined chronic obstructive pulmonary disease and pneumoconiosis.
The risk factors for the combined diseases were analysed using regression analysis in a cohort of patients with various subtypes of pneumoconiosis.
The present study was limited by recruitment of the patients with pneumoconiosis of a single medical centre and the failure to enrol dust-exposed workers without pneumoconiosis.
The cross-sectional design did not have the power to disclose the association between occupational exposure and disease progression or mortality.
Introduction
Pneumoconiosis is a group of heterogeneous fibrotic lung diseases that develops through the inhalation of the inorganic mineral dusts.1 Until now, pneumoconiosis is the most common occupational disease in China. In 2018, the prevalence was approximately 90% among the newly reported occupational patients, accounting for about 0.87 million Chinese people with pneumoconiosis.2 Moreover, pneumoconiosis is a potential cause of disability and thus induces a substantial socioeconomic burden, especially in developing countries.3 4 A cohort of 110 167 South African miners was found that emphysema remains the occupational lung disease with the highest prevalence.5 The occupational dust exposures induce lung inflammation cascades and structural damage that can lead dust-related lung disorders including pneumoconiosis as well as chronic obstructive pulmonary disease (COPD).6
COPD, characterised by chronic airflow obstruction and persistent respiratory symptoms usually associated with inflammatory response to noxious particles and gasses,7 is a serious public health problem worldwide.8–10 In China, the most recent national survey of COPD with 50 991 patients enrolled showed the prevalence of spirometry-defined COPD to be 8.6% (11.9% in men and 5.4% in women), representing an estimated 99.9 million population with COPD.11 Similarly, the 2015 Global Burden of Disease study of 384 million adults found that 174.5 million adults were affected by COPD.12 Cigarette smoking has been identified as the largest risk factor for COPD.11 13 14 However, numerous other risk factors have been identified, including several rare genetic syndromes (such as α1-antitrypsin deficiency), underweight, occupational exposures and environmental pollution.11 15 Specifically, the median population attributable fraction for occupational exposure contribution to COPD risk was 15% and was up to 31% among never-smokers.13 16 17 Previous research on COPD has mainly focussed on the general population or workers with history of exposure to vapour gas, dust and fumes,18 and few studies have investigated patients with combined COPD and pneumoconiosis, which may be a distinct clinical phenotype. Furthermore, a substantial proportion of pneumoconiosis patients have a history of smoking, and it is unclear whether occupational dust exposure contribution to COPD is equipotent to that of cigarette smoking in some circumstances.
Therefore, the purpose of this study was (1) to describe the prevalence and clinical features of combined COPD and pneumoconiosis and (2) to identify the risk factors for combined disease among pneumoconiosis patients.
Methods
Study design
This descriptive study adopted a cross-sectional design and followed guidelines established by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist.19
Settings and participants
Patients with pneumoconiosis were consecutively recruited, from January 2016 to July 2019, on presentation at Beijing Chao-Yang Hospital, China, a regional medical centre specialising in occupational medicine. The pneumoconiosis was diagnosed according to the International Labour Organisation classification after multidisciplinary discussion.20 Patients of whom spirometry data were missing or with pulmonary malignant tumour, acute pulmonary infection, pulmonary tuberculosis, asthma, bronchiectasis or pneumothorax were excluded.
All investigations were conducted in accordance with the ethical standards of Beijing Chao-Yang Hospital and the World Medical Association Declaration of Helsinki. Written informed consent was obtained from all patients.
Sample size
The most influential parameters of sample size were the risk factors for combined COPD and pneumoconiosis. To identify the risk factors for combined diseases, with 95% confidence and 80% power, 5 to 10 observations per previously demonstrated risk factors for COPD in pneumoconiosis patients were needed.21 Based on the previous publication by Peng et al,21 the prevalence of COPD among pneumoconiosis was 18.65%, the calculated sample size was 214 to 428. Furthermore, this study demonstrated risk factors for COPD in never-smokers subgroup. Thus, the final sample sizes were 498 to 995 according to the proportion of non-smokers in patients with pneumoconiosis from Beijing Chao-Yang Hospital.
Study procedure
Data collection
Clinical data were collected from medical reports and included age, sex, height, weight, smoking status, occupational history (including type of exposure, and start and end dates of employment), current and past medical history and family history at the date of inclusion. Smoking status was categorised as: current smoker, former smoker (cessation ≥12 months previously) and never-smoker. Smoking intensity was measured in pack-years (years of smoking 20 cigarettes/day), categorised as: 0 pack-years, 1 to 9 pack-years, 10 to 19 pack-years and ≥20 pack-years, with ‘heavy smoking’ defined as having smoked ≥20 pack-years. Body mass index (BMI) was categorised as: underweight (<18.5 kg/m2), normal (18.5 to 24.9 kg/m2) and overweight/obese (≥25.0 kg/m2).11 Latency, defined as the time from initial occupational dust exposure to pneumoconiosis diagnosis, was also recorded.
Pulmonary function tests
Pulmonary function tests were carried out by certified technicians according to hospital guidelines, which met the quality control standards established jointly by the American Thoracic Society and European Respiratory Society.22 Pulmonary function parameters were measured using spirometry, whole body plethysmography and single-breath diffusing capacity for carbon monoxide measurements. In this study, the pulmonary function prediction formula is based on the normal lung function prediction formula of Chinese adults established in 2017.23 COPD was diagnosed based on clinical features and/or history of exposure to risk factors and post bronchodilator forced expiratory volume in 1 s (FEV1)/ forced vital capacity (FVC) ratio <0.70, according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guideline.24 Similarly, airflow limitation severity was categorised by the percentage of predicted FEV1, as: mild (≥80%), moderate (≥50% to<80%), severe (≥30% to<50%) and very severe (<30%).25 Positive bronchial dilation test was defined as an increase in FEV1 of ≥200 mL and ≥12% after bronchodilation (salbutamol 400 mg).24 Airway hyperresponsiveness (AHR) was defined by a methacholine provocation concentration of 4 mg/mL or less, which led to a 20% reduction in FEV1.26 Bronchial challenge test was performed in patients with FEV1 above 60%.
Chest radiographs
Chest radiographs were performed for each patient. These were independently assessed by two experienced clinicians according to the International Labour Organisation classification,20 with good interobserver correlation (0.81). Pneumoconiosis was classified as stage Ⅰ, II or Ⅲ based on the density and distribution of small nodules/large opacities disclosed on the chest X-ray. Further details about the classification criteria can be found in the online supplementary material (see Method).
Supplemental material
High-resolution computed tomography
High-resolution computed tomography (HRCT) was acquired on a 64-slice single-source CT system with 0.625–mm sections, a 1–sec scan time and a 10–mm interval in the apex–base scans, with the inclusion of both lungs in the field of view. Large opacity was defined as an opacity having the largest diameter (at the mediastinal window setting) >1 cm. The central type of large opacities, which compress the bronchus causing airway obstruction, is located between the transverse section of the tracheal carina and a margin 50 mm below the carina. A detailed description of the size of the large opacities is found in the online supplementary material (see Method).
Statistical analysis
Statistical analyses were performed using SPSS Statistics V.23 (IBM Inc, Chicago, Illinois, USA). The distribution of the continuous variables was checked at first. Comparisons of normally distributed continuous variables were performed by a one-way analysis of variance across four groups. The comparisons of non-normally distributed variables were determined using the Mann-Whitney U test or Kruskal-Wallis test. Continuous variables were reported as mean±SD or median and IQR. Categorical variables were presented as number and percentage and were analysed using the χ2 test or Fisher’s exact test. Univariate and multivariable logistic regression analyses were used to investigate previously demonstrated risk factors for COPD in all pneumoconiosis patients and in never-smokers, respectively, and were reported with OR and CI. The possible interaction between occupational dust exposure and cigarette smoking was evaluated by logistic regression analyses. To eliminate the effect of mechanical compression on the bronchi, the patients with large opacities were excluded during logistic regression analyses. A p value <0.05 was considered statistically significant.
Patient and public involvement statement
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Results
Demographics
A total 758 patients were invited to participate between January 2016 and July 2019. Of these, 675 patients with pneumoconiosis (523 men) were included in the analysis. The detailed flow diagram is shown in figure 1. The sample included 130 patients with asbestosis, 210 with silicosis, 259 with coal workers’ pneumoconiosis and 76 with other subtypes of pneumoconiosis. The demographic characteristics of the groups are presented in table 1.
Demographics of the enrolled population

Flow chart of the enrolled population. COPD,chronic obstructive pulmonary disease.
Prevalence of combined COPD and pneumoconiosis
The overall prevalence of COPD was 32.7% (221/675) in the enrolled population (table 2). The prevalence of COPD was significantly different among the subgroups, and patients with silicosis and coal workers’ pneumoconiosis had relatively high prevalence (40.0% and 38.6%, respectively). The prevalence of COPD increased with smoking pack-years and was 24.3%, 36.2% and 43.9%, respectively, in the patients smoking 1 to 9 pack-years, 10 to 19 pack-years and ≥20 pack-years (p=0.002). Similarly, the prevalence increased with the duration of dust exposure and was 30.0% with 0 to 15 years, 36.9% with 16 to 30 years and 39.6% with 31 to 45 years of exposure (p=0.046). The prevalence of COPD also increased with the pneumoconiosis stage and was 20.2% in stage Ⅰ, 25.6% in stage Ⅱ and 62.6% in stage Ⅲ (p<0.001). The prevalence of COPD did not differ by sex, smoking history or BMI.
Prevalence of combined COPD and pneumoconiosis
Characteristics of the patient with combined COPD and pneumoconiosis
In comparison with pneumoconiosis alone, the patients with combined COPD and pneumoconiosis had higher cigarette pack-years (p<0.001), lower BMI (p=0.001), higher silica or coal dust exposure (p<0.001) as well as higher stage (p<0.001) (table 3). The patients with combined COPD and pneumoconiosis also differed from those with only pneumoconiosis in a range of lung function measures (online supplementary table S1); in particular, compared with those without COPD, patients with COPD had significantly more severe airflow limitation, increased small airway dysfunction and decreased membrane diffusing capacity.
A composition of pneumoconiosis combined with or without COPD
Among the 221 patients with COPD and pneumoconiosis, 31.7% had GOLD stage I COPD; 42.1% had stage II; 20.8% had stage III and 5.4% had stage IV (online supplementary table S2). Additionally, 29.4% (65/221) patients with combined diseases had a positive bronchodilation test, 57.1% (64/112) had AHR, and 43.9% (97/221) had blood eosinophil counts >100 cells/µL (online supplementary table S2).
Risk factors for combined COPD and pneumoconiosis
In the full study sample, 9.5% (20/210) of the patients with silicosis and 1.5% (4/259) of the patients with coal workers’ pneumoconiosis showed central of large opacities on HRCT, who were excluded during the logistic regression analyses. In the univariate logistic regression analysis, the risk factors associated with COPD included age ≥40 years, heavy smoking, silica or coal exposure and pneumoconiosis stage Ⅲ (table 4). In the multivariable-adjusted analyses, the risk of COPD was increased among patients with exposure to silica (OR 2.42, 95% CI 1.28 to 4.59, p=0.007) and coal (OR 3.19, 95% CI 1.57 to 6.49, p=0.001) dust, compared with patients with exposure to asbestos; there was a significantly increased risk of COPD in pneumoconiosis stage Ⅲ compared with stages Ⅰ/Ⅱ (OR 4.85, 95% CI 3.18 to 7.42, p<0.001).
Logistic regression model for 651 patients with combined COPD and pneumoconiosis*
Among the never-smokers, multivariable-adjusted analyses showed that the risk of COPD was increased with silica exposure (OR 3.88, 95% CI 1.49 to 10.12, p=0.006), and coal (OR 3.85, 95% CI 1.12 to 13.18, p=0.032) compared with asbestos exposure, consistent with the results for the full sample (online supplementary table S3).
Interaction between occupational dust exposure and cigarette smoking
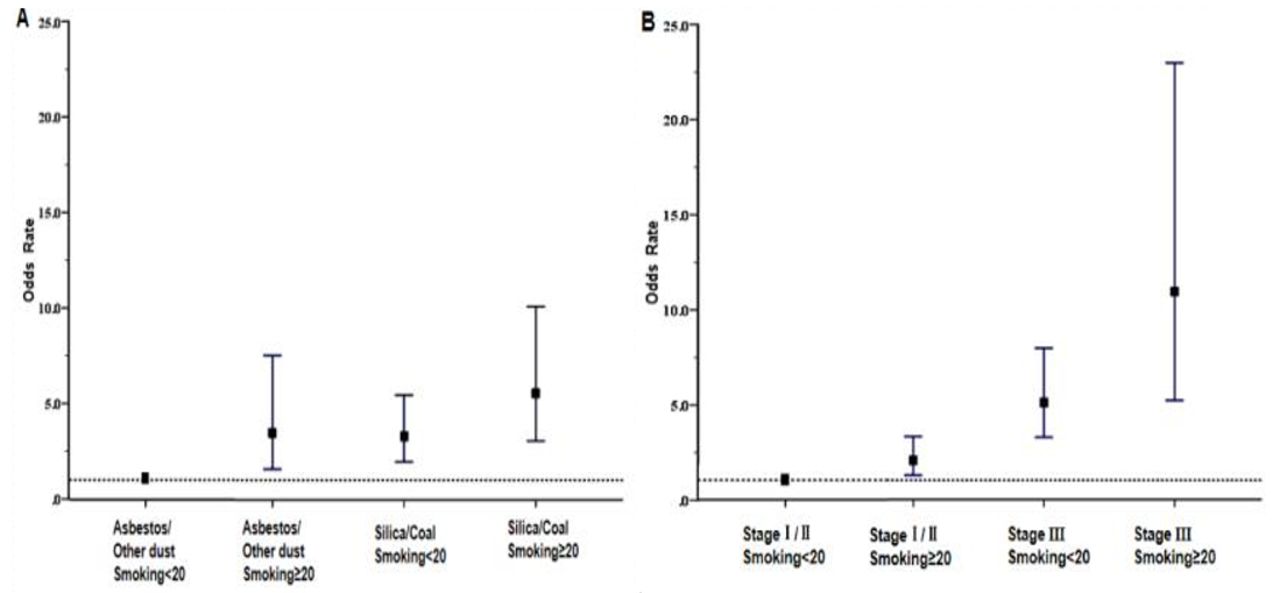
A significant interaction was found between occupational exposure and cigarette smoking (online supplementary table S4 and figure 2). The risk of COPD increased with heavy smoking and silica or coal exposure (OR 5.49, 95% CI 3.04 to 9.93, p<0.001). Similarly, a significant interaction was noted between smoking intensity and pneumoconiosis stage.

{kind=link}
{kind=link}
Interactions between risk factors for combined chronic obstructive pulmonary disease and pneumoconiosis: (A) occupational dust exposure and cigarette smoking and (B) pneumoconiosis stage and cigarette smoking.
Discussion
The present study disclosed that COPD was highly prevalent in the patients with certain types of pneumoconiosis. The results also showed the characteristics and risks for combined COPD and pneumoconiosis. The prevalence of COPD differed according to the type of pneumoconiosis and was the highest in silicosis, followed by coal workers’ pneumoconiosis. Patients with both COPD and pneumoconiosis had higher cigarette pack-years, lower BMI, higher composition of silica or coal dust exposure as well as higher percent of stage Ⅲ, more severe airflow limitation and increased small airway dysfunction, compared with patients with pneumoconiosis alone. Heavy smoking, silica or coal dust exposure and advanced pneumoconiosis were identified as the preventable risk factors for COPD in patients with pneumoconiosis. A positive interaction was found between occupational dust exposure and cigarette smoking among patients with combined COPD and pneumoconiosis.
Previous population-based studies have reported different prevalence of COPD in various countries and on populations with a variety of occupations.11 27 28 Data from 418 378 adult respondents to the 2017 Behavioural Risk Factor Surveillance System survey showed that the overall age-adjusted prevalence of COPD was 6.2% in the USA.29 Similarly, the most recent population-based study from China reported an overall COPD prevalence of 8.6%.11 Our data showed a particularly high prevalence of COPD among patients with pneumoconiosis, especially in silicosis and coal workers’ pneumoconiosis. A cross-sectional study of patients with silicosis or coal workers’ pneumoconiosis from South China reported a COPD prevalence of 18.65% (119/638), which is lower than our finding.21 One reason may be that our study had a higher percentage of smokers. It is also possible that the differences in COPD prevalence are a result of other differences in study participants and working conditions. The present study also found that over half (57.0%) of the patients were smokers and that the prevalence of COPD did not differ between smokers and non-smokers—these findings are in line with the data previously reported.21 While these earlier studies are not directly comparable, the data indicate that combined COPD and pneumoconiosis occurs often in patients with certain types of pneumoconiosis.
Silica, coal, asbestos and mixed dusts are common occupational respiratory toxins. One study found the prevalence of emphysema to be higher in the patients with silica exposure (55%) than in those with asbestos exposure (29%) (p=0.04).30 Another study from South Africa also showed that the rate (per 1000 autopsies) of emphysema was higher with coal exposure (404/1000) than with asbestos exposure (345/1000).31 Similarly, in the present study, the prevalence of COPD was twice as high in patients with silicosis and patients with coal workers’ pneumoconiosis than in those with asbestosis. Of note, our previous study found that even in the presence of both emphysema and pulmonary fibrosis, spirometry and lung volumes may still be in normal range or show mild abnormalities, such as the small airway dysfunction.32 Thus, it is possible that COPD was underestimated in patients with pneumoconiosis, especially asbestosis.32 Additionally, we found that pneumoconiosis severity was associated with COPD prevalence. This finding is consistent with previous data showing that the prevalence of emphysema increases with pneumoconiosis stage—as high as 60.76% (144/237) in pneumoconiosis stage Ⅲ.33 These results suggest that airflow obstruction is associated with the severity of pneumoconiosis.34 35
The high prevalence of COPD in our sample of patients with pneumoconiosis underscores the importance of identifying the risk factors for combined COPD and pneumoconiosis. Cigarette smoking has been well recognised as one of the main risk factors for development of COPD.11 36 37 In the present study, smoking pack-years was associated with increased risk of COPD. However, in previous research, no significant correlation was found between smoking and COPD in patients with pneumoconiosis.21 A possible explanation of the inconsistency is the lack of stratification by smoking pack-years in the earlier work. Previous studies of COPD have examined occupational risk factors in addition to smoking. An earlier meta-analysis showed that occupational exposure to irritant dusts, gases and fumes was an independent risk factor for COPD.38 Several studies have found that compared with asbestos dust, silica and coal dust exposure is more strongly associated with emphysema.30 39 40 Similarly, the present study provides confirmation that exposure to silica or coal dust results in a higher risk for COPD than asbestos exposure does, both in smokers and never-smokers. These findings support the hypothesis that patients with silica and coal dust exposure suffer from higher dust concentrations or more damaging components (compared with asbestos), resulting in elevated risk for COPD. Inhaled silica and coal dust are predominantly deposited in the bronchioles, where they are engulfed by alveolar macrophages,41–43 whereas inhaled asbestos fibres accumulate in the peribronchiolar and adjacent alveolar spaces.44 Thus, different types of dust inflict varying damage to the lungs, but chronic inflammation, remodelling of the small airways and destruction of lung parenchyma ultimately lead to COPD.45 46 Moreover, the higher OR for COPD among never-smokers compared with the full sample suggests that silica and coal dust exposures contribute more substantially to the burden of COPD in non-smokers. Additionally, a longitudinal cohort study of 3202 patients with silicosis in Hong Kong demonstrated interactive effects of cigarette smoking and silicosis on COPD.47 Our study also indicates that smoking potentiates the effect of silica and coal dust exposure on COPD, consistent with the findings from other previous studies.48–50 Thus, smoking cessation, in addition to prevention of occupational exposure, is critical to reducing COPD-related morbidity.
Among the full sample of patients with pneumoconiosis in the present study, nearly three-quarters of the cases of COPD were mild-to-moderate in severity (by GOLD staging). The decline in lung function appears to result primarily from obstructive rather than restrictive air trapping. One-half of the patients with combined COPD and pneumoconiosis had AHR, but this was not significantly different from the finding of AHR in patients with pneumoconiosis alone. An earlier study reported that 24% to 60% of patients with COPD had AHR.51–53 However, little is known about the clinical features of combined COPD and pneumoconiosis. A post hoc analysis of three randomised trials that included 4528 patients with COPD treated by inhaled corticosteroids (ICS) found a reduction in exacerbation at blood eosinophil levels >100 cells/µL (relative risk=0.75).54 Elsewhere, it was suggested that a threshold of ≥300 cells/µL can identify patients with the greatest likelihood of beneficial response to ICS.54 55 Based on these studies, the 43.9% (97/221) of the patients with combined disease with blood eosinophil counts ≥100 cells/µL (or the 7.5% with counts>300 cells/µL) in the present study are likely to benefit from ICS. Nevertheless, it is uncertain whether blood eosinophil count is a reliable biomarker for response to ICS treatment for the prevention of exacerbations of combined COPD and pneumoconiosis. Clinical trials are warranted to evaluate the effectiveness of ICS therapy in this regard.
This study had several limitations. First, this study recruited patients from a single medical centre and did not investigate dust-exposed workers without pneumoconiosis. Second, the cross-sectional design did not disclose the association between occupational exposure and disease progression or mortality—longitudinal, population-based studies are warranted to identify the role of occupational dust exposure in the development and prevention of COPD. Third, since the patients in the study were employed by different industries, it was difficult to estimate occupational exposure levels and therefore the exposure-response relationship in COPD prevalence. Finally, the effect of passive smoke was not taken into account in our study. The effects of smoking on COPD might be underestimated.
Conclusion
The present study showed that COPD was highly prevalent in the patients with certain types of pneumoconiosis. More than 70% of patients with combined COPD and pneumoconiosis had mild-to-moderate airflow limitation. Nearly half of them had peripheral eosinophil count >100/μL. Heavy smoking, silica or coal dust exposure and advanced pneumoconiosis are all associated with increased COPD risk, although differences in the onset of COPD before or after the onset of pneumoconiosis cannot be distinguished. In addition, occupational dust exposure interacts with smoking to further increase the risk of COPD. Our study indicates that the prevention measures are critical to decrease the occupational exposure and improve the disease controlling among dust exposure workers. Meanwhile, tobacco education and smoking cessation are needed to recognise and control smoking hazards.
Acknowledgments
We thank all patients who were involved in this study. We express our thanks to Miss Moyang Xu of University of Michigan, Ann Arbor, for polishing language and grammar of the manuscript.
References
Footnotes
Contributors YF performed all data collection, analysed and wrote the manuscript. WX and YW were responsible for acquisition of data and data analysis. YW and SY were responsible for recruiting the patients and acquisition of data. QY contributed as primary investigator and was involved in the conception, design and planning the study, the acquisition of data and revision of the paper. All authors contributed to data interpretation, read and approved the final manuscript.
Funding The work was supported by National Natural Science Foundation of China (81970061) and Consulting Research Project of Chinese Academy of Engineering (2019-XZ-70).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Obtained.
Ethics approval The study was approved by the Institutional Review Board of Beijing Chao-Yang Hospital (2018-KE-289).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.