Article Text

Abstract
Objective Opioids are increasingly prescribed and frequently involved in adverse drug events (ADEs). The underlying nature of opioid-related ADEs (ORADEs) is however understudied. This hampers our understanding of risks related to opioid use during hospitalisation and when designing interventions. Therefore, we provided a description of the nature of ORADEs.
Design A post-hoc analysis of data collected during three retrospective patient record review studies (in 2008, 2011/2012 and 2015/2016).
Setting The three record review studies were conducted in 32 Dutch hospitals.
Participants A total of 10 917 patient records were assessed by trained nurses and physicians.
Outcome measures Per identified ORADE, we described preventability, type of medication error, attributable factors and type of opioids involved. Moreover, the characteristics of preventable and non-preventable ORADEs were compared to identify risk factors.
Results Out of 10 917 patient records, 357 ADEs were identified, of which 28 (8%) involved opioids. Eleven ORADEs were assessed as preventable. Of these, 10 were caused by dosing errors and 4 probably contributed to patients’ death. Attributable factors identified were mainly on patient and organisational levels. Morphine and oxycodone were the most frequently involved opioids. The risk for ORADEs was higher in elderly patients.
Conclusions Only 8% of ADEs identified in our sample were related to opioids. Although the frequency is low, the risk of serious consequences is high. We recommend to use our findings to increase awareness among physicians and nurses. Future interventions should focus on safe dosing of opioids when prescribing and administering, especially in elderly patients.
- pain management
- adverse events
- health & safety
- quality in health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study was based on data gathered during three national retrospective patient record review studies conducted in 2008, 2011/2012 and 2015/2016 within 32 Dutch hospitals.
During all three studies, a broad and randomly selected sample of all hospital admissions of patients were reviewed to assess the nature and preventability of adverse drug events with opioids.
Our study population was stratified, resulting in an over-representation of in-hospital deceased patients.
The low frequency of opioid-related adverse drug events limited a comparison of events over time among the three study periods.
Introduction
Over the past decades, prescription of opioids has substantially increased worldwide.1 2 Moreover, the rise in addiction rates and deaths resulting from opioid overdoses has urged physicians to call out an opioid crisis.3 In the Netherlands, the prescription of oxycodone has increased almost fivefold over 10 years (from 96 000 users in 2008 to 485 000 users in 2018).4 This increase may however not only lead to more addiction but may also affect the number of opioid-related adverse drug events (ADEs) in hospitals.
Opioids are frequently involved in ADEs5–7 and approximately in 2%–14% of all patients.8–12 ADEs are unintended injuries from a medical intervention related to drugs.13 Opioid-related ADEs (ORADEs) occur frequently, specifically in paediatric,7 14 palliative15 and surgical patients.10 11 16 ORADEs are often caused by errors such as omissions or incorrect dosing.7 14 15 17 In addition, approximately 11% of ORADEs among hospitalised patients cause severe or even fatal patient harm,18 and also due to the fast therapeutic effects of opioids. Besides these severe consequences, ORADEs lead to significantly higher healthcare costs.9 10 16
Our current knowledge about the incidence of ORADEs and their underlying nature is mostly based on medication-related incident reports.7 14 15 17 However, a comprehensive patient chart review provides the most reliable information on ADEs in hospitals, while incident reports suffer from severe under-reporting.19 20 Furthermore, ORADE studies based on incident reports were usually conducted at one point in time or within one hospital or at a specific department.7 14 15 17 The few ORADE studies based on comprehensive patient chart review were mainly conducted within a surgical population.10 11 16
Therefore, and also motivated by the opioid crisis, we have conducted an indepth analysis of ORADEs using data gathered during three consecutive national adverse event (AE) studies in the Netherlands in which patient record review was applied. To our knowledge, no such longitudinal multicentre study on ORADEs in a diverse inpatient population and using a comprehensive ADE detection method has been published. The aim of this study was to provide a detailed description of the underlying nature of ORADEs. By doing so, we hope to increase awareness and provide recommendations on how to prevent ORADEs in future hospitalised patients.
Methods
Design and setting
We conducted a post-hoc analysis of data that were collected during three national retrospective patient record review studies conducted in 2008, 2011/2012 and 2015/2016. The aim of these studies was to identify AEs and ADEs in Dutch hospitals. A detailed description of the methodology used in these studies was previously published and comparable with other international AE studies.21 22 In summary, for the 2008 and 2011/2012 studies, a random sample of 20 hospitals participated. In 2015/2016, a new random sample of 19 hospitals were selected, of which 7 had previously participated in two of the earlier studies. Both samples were stratified for hospital type and representation of urban and rural areas. In 2008 and 2011/2012, 200 patient records per hospital were randomly selected for review: 100 records of discharged patients and 100 records of in-hospital deceased patients. The 2015/2016 study was limited to 150 in-hospital deceased patients per hospital because the frequency of preventable AEs remained unchanged for in-hospital deceased patients in both the 2008 and the 2011/2012 measurements.23–25 Records of patients younger than 1 year and of patients admitted at the departments of psychiatry and obstetrics were excluded because other expertise is necessary to detect AEs in these patients. The random selection of patient records was conducted by the participating hospitals with clear instructions of the researchers.
Review procedure: AE studies
During all three AE studies, selected patient records were reviewed for the occurrence of AEs, including ADEs. In figure 1, a schematic overview of the review process in the national studies and this study is presented. In summary, the review process consisted of two phases. In phase 1, the records were screened for potential AEs by trained independent nurses. When predefined triggers were found, indicating an AE might have occurred, the record was labelled for an indepth review by a trained independent physician. Independent means that the physicians and nurses never had an employment contract in the participating hospitals. The physicians were highly experienced and specialised in surgery, internal medicine or neurology, and during the record review studies they had access to all information on the electronic patient records. Besides, 10% of all patient records were reviewed by two physicians to determine inter-rater reliability. Validity of this scoring system has not been tested, but it has been used widely in AE studies for over 20 years and the ratings of the system did not change in that time.21–23 26–29 Prior to the study, both nurses and physicians had training sessions in which cases were discussed to enhance the quality and standardisation of the review process.
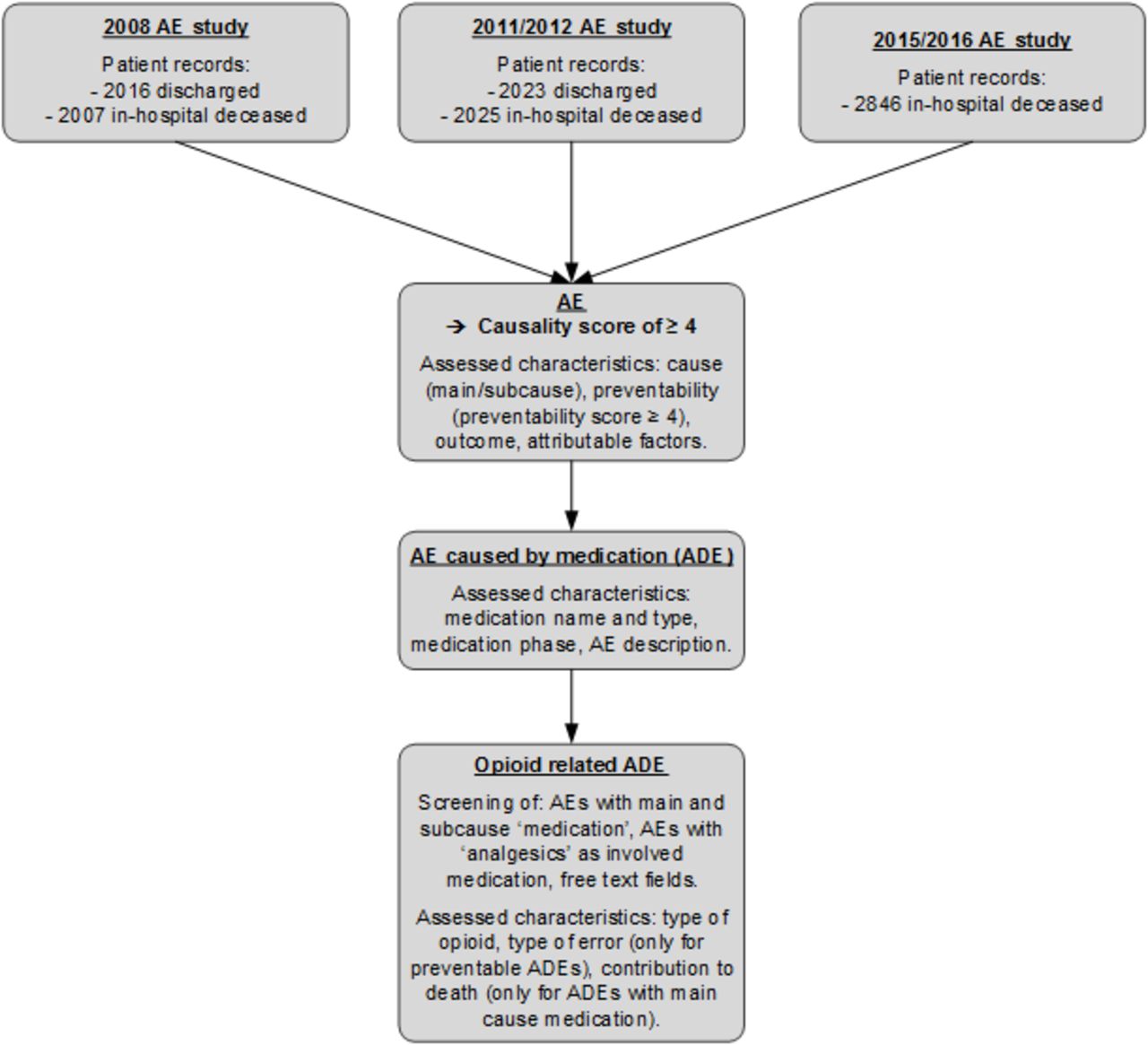
{kind=link}
Overview of the three Dutch adverse event studies and our study. ADE, adverse drug event; AE, adverse event.
An AE was defined by three criteria: (1) an unintended physical or mental injury; (2) the injury resulted in prolongation of hospital stay, temporary or permanent disability, or death; and (3) the injury was caused by healthcare management rather than the patient’s underlying disease.23 27 28 An AE was scored as caused by the healthcare (causality) if the likelihood score was equal to or greater than 4 based on a 6-point Likert scale, with (virtually) no evidence (1), slight to modest evidence (2), not likely but borderline (3), more likely but borderline (4), moderate to strong evidence (5), or (virtually) certain evidence (6) of management causation. The scoring system was used in all three record review studies and the physicians made the judgements about causality and preventability based on all the available information of the patient’s condition and taking into account the guidelines.
If an AE was identified, the independent physicians (hereafter: experts) assessed each AE on cause (diagnostic, surgery, non-invasive procedure, medication, other clinical activities, admission and other), preventability, possible contribution to death and attributable factors. The attributable factors were based on the taxonomy of the Eindhoven Classification Model and consisted of the main categories: technical, care, organisational, patient-related, violation and other.30 An AE was considered to be preventable when the care given fell below the current level of expected performance of practitioners or systems. Before the physicians answered the question about preventability, they were required to respond to 13 questions to add more structure to the review process (see online supplemental table 1), for example, if there was a complex medical history, if the patient had comorbidity and whether another physician would repeat this treatment. Preventability was also assessed on a 6-point Likert scale, with almost no evidence (1), slight to modest evidence (2), modest evidence but borderline (3), modest to strong evidence (4), strong evidence (5), or almost certain evidence (6) of preventability. A score of 4–6 indicated that the reviewer assessed the AE as having a greater than 50% chance of being potentially preventable.
Supplemental material
Furthermore, for each patient the following characteristics were registered: gender, age, length of hospital stay, urgency of admission, whether patients were terminally ill prior to the admission, the number of involved medical specialists, department of admission, type of procedure and comorbidity. The latter was divided into no, minor, moderate and severe comorbidity, and was assessed by the experts after careful review of the information on the patient record. Also, one organisational characteristic (type of hospital: university, tertiary teaching or general) and one AE characteristic (weekend or holiday at the time of the AE) were registered.
When an AE was medication-related (ADE), the following additional characteristics were registered by the experts: name and type of medication involved, medication phase, a description of the ADE and whether the ADE possibly contributed to the patient’s death. The medication phases were classified into ordering, transcribing, dispensing, administering and monitoring.31 32 The possible contribution to the patient’s death was only registered for ORADEs, with ‘medication’ as a main cause of the event and not for ADEs with ‘medication’ as a subcause.
All data were entered into a national AE database specifically designed for these AE studies.
Review procedure: ORADEs
For our study, we used the national AE database to identify ORADEs (figure 1). One researcher (BCFMS) conducted the screening of the database and retrieved several preselected variables: (1) AEs with the main classification cause ‘medication’ as well as AEs with ‘medication’ as a subcause; and (2) AEs with ‘analgesics’ as involved medication. Furthermore, two free-text fields were selected: the summary of the AEs and the preventability assessment. A second researcher (MM) independently double-checked the selection procedure.
All identified ORADEs were then classified by BCFMS on the type of opioids involved using the WHO Anatomical Therapeutic Chemical (WHO ATC) classification.33 For the preventable ORADEs, the type of medication error was classified according to a data-driven analysis of the free-text summaries of the ADEs. The classification of ORADEs was double-checked by two senior researchers (JEK and IJ) and any discrepancies were resolved by consensus.
Outcomes
To provide insight into the nature of the ORADEs, each ORADE case was summarised by gender, age of the patient (categorised in steps of 10 years for privacy reasons), type of opioid involved, attributable factors and preventability. When the ORADE was preventable, then the type of medication error and medication phase were also described. Furthermore, in order to identify risk factors, we compared the outcome variables between preventable and non-preventable ORADEs.
Data analysis
Only descriptive statistics were used in this study. Descriptives are presented as median (age and length of hospital stay) or frequency (gender, comorbidity, type of opioids and attributable factors and so on). Patient and hospital characteristics are presented on the patient level and ORADE characteristics are presented on the AE level. Inter-rater reliability among nurses and physicians was addressed in terms of positive and negative agreement frequencies.34 All analyses were conducted using STATA V.14.1 and double-checked by a second researcher (MM) and a statistician (PS).
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
In total, 10 917 records were screened during the three AE studies. The patient records of discharged and deceased patients were equally distributed among male and female patients. Most patients were hospitalised for a non-elective procedure (table 1). In 1150 patient records, at least one AE was detected, with a total of 1240 AEs. When detecting the predefined triggers, positive agreement between nurses varied between 76.0% and 91.5%. When detecting AEs, positive agreement between physicians varied between 53.4% and 63.3%. For assessing preventability, positive agreement between physicians varied between 71.4% and 73.3%. Overall, agreement frequencies were moderate. More detailed information about the inter-rater reliability is presented in online supplemental table 2.
Supplemental material
Patient and hospital characteristics of all reviewed patient records, including adverse events per study period and discharge status
Opioid-related ADEs
Of 1240 AEs, 357 (29%) were medication-related (ADEs). In 28 (8%) ADEs, opioids were involved. These ADEs are summarised in detail in table 2, and included 24 ADEs with ‘medication’ as a main cause and four ADEs with ‘medication’ as a subcause. The ORADEs occurred in 27 patients; one patient experienced two ORADEs. Most patients with ORADEs involved female patients (59%). The median age of the patients was 76 years (IQR: 66–83), and the median length of hospital stay was 7 days (IQR: 4–16). Most patients had moderate to significant comorbidity (70%) and had three medical specialists during the admission (78%) (table 3).
Descriptions of the 28 opioid-related adverse drug events divided into preventable and non-preventable
Characteristics of patients (n=27) with ORADEs (n=28)*
Nature of ORADEs: preventability
According to the experts, 11 (39%) out of the 28 ORADEs were considered as potentially preventable (table 4). Non-preventable (31%) ORADEs occurred slightly more during weekends and holidays than preventable ADEs (18%). Moreover, most preventable and non-preventable ORADEs occurred during day shifts (08:00–17:00).
Clinical context of ORADEs (n=28)*
Nature of ORADEs: medication errors and phase
Of the 11 potentially preventable ORADEs, 10 (91%) were caused by dosing errors, of which 6 were during the prescribing phase (cases 1, 3, 7, 8, 9 and 10) and 4 during the administration phase (cases 2, 4, 5 and 6) (table 2). Of the 10 dosing errors, 6 occurred in elderly patients (≥70 years) (cases 1, 3, 4, 5, 8 and 9) and 2 around patients’ discharge (cases 2 and 7). The remaining one preventable ORADE (case 11) was related to incorrect decision making. Finally, the experts assessed the consequences of the ORADEs (multiple options possible). In eight ORADEs, an intervention or extra treatment was needed, in two ORADEs the patients had a prolonged hospital stay, and four preventable ORADEs possibly contributed to the death of the patient (cases 5, 6, 8 and 9).
Nature of ORADEs: attributable factors
The attributable factors involved in ORADEs were care-related (knowledge, skills, monitoring, verification and coordination of care) and patient-related (comorbidity, age, a demanding patient or a patient with an intellectual disability) (table 4). Of preventable ORADEs, eight were care-related and six were patient-related. For non-preventable ORADEs, 3 were care-related and 10 were patient-related. However, in three of the cases of non-preventable ORADEs, the attributable factors could not be assessed by the experts due to insufficient information on the patient records.
Nature of ORADEs: medications involved
Out of the 11 preventable ADEs, 8 occurred with opioids with ATC code N02AA, which are morphine and oxycodone (table 4). Non-preventable ORADEs occurred with opioids mainly with ATC code N02AA (morphine and oxycodone, 53%).
Discussion
In three national patient record studies with 4-year intervals, we found 28 ADEs caused by opioids. These ADEs correspond with 8% of all identified ADEs and 0.3% of all studied patient records. Of the 28 ORADEs, 11 (39%) were assessed as potentially preventable, involving mostly morphine and oxycodone. Dosing errors during the prescription and administration phase were the most common cause of preventable ORADEs and occurred most often in elderly patients. Four preventable ORADEs probably contributed to patients’ death. Finally, attributable factors for ADEs were mostly care-related and patient-related.
In this study, the percentage of ORADEs of all patient records (0.3%) was low, also in comparison with previously conducted ORADE studies that focused on large populations (11%–14%).10 11 16 However, two of these studies were based on large databases and all involved surgical patients who often receive opioids postoperatively. We focused on a broad hospitalised patient population, both surgical and non-surgical. Furthermore, the difference in ORADE occurrence might be explained by differences in the used ADE definition. For example, instead of using all ORADEs, that is, including side effects of opioids, in our study only ADEs that resulted in severe patient harm were included. This means that ADEs resulted in prolongation of hospital stay, temporary or permanent disability, or death. Furthermore, only ADEs with a causality likelihood score of equal or greater than 4 were included, which means that the experts indicated an ADE as having a greater than 50% chance of being caused by healthcare. Should we have selected the cases with causality likelihood scores of 1–3 as well, then we could determine at least 2500 additional cases on whether medication and opioids were related. However, we did not determine these 2500 cases, since we wanted to stay true to the definition of an AE (at least 4 on the 6-point Likert scale), and we did not consider it ethical to change the method of the study afterwards.
In line with previous studies,7 14 15 17 we found that dosing errors during prescribing and administering were the main cause of preventable ORADEs. Furthermore, 60% of the dosing errors in our study occurred in elderly patients (≥70 years). In general, prescribing medication for elderly patients is challenging since polypharmacy, multimorbidity, and altered pharmacokinetics and pharmacodynamics of drugs are often present. Besides, this population will rapidly increase in the upcoming years. Specifically related to opioids, physicians also need to be aware of the higher sensitivity of elderly patients to the effects of opioids,35 and balancing between minimising the risk of addiction and side effects while effectively relieving pain.36 37 Taking into account all these factors while prescribing demands a lot from physicians during their busy daily hospital practice. A clinical decision support system (CDSS) can help physicians in this complex task by showing warnings and advice during prescribing, for example showing the most appropriate choice of medication for a given condition and/or by providing dosing recommendations. CDSS has shown to effectively reduce prescribing errors among hospitalised elderly patients38 39 and errors with medications of which the therapeutic effects are fast, such as opioids.40 Furthermore, a CDSS can also be effective in predicting which patients are at risk for ORADEs. Using retrospective data from gastrointestinal surgical patients, Minkowitz et al 41 developed a risk-scoring model to identify patients with a high risk for experiencing an ORADE based on their clinical and demographic profiles. If developed specifically for elderly inpatients, such a prediction model could help physicians in determining the most appropriate and safe pain management strategy for these vulnerable patients. Finally, a CDSS could also be used to identify patients who might be suitable for pre-emptive genotyping, which involves metabolic testing prior to prescribing.42 Patients with high levels of pain despite using high doses of pain medication or patients who experience severe side effects while using common dosing schedules may especially benefit from such an intervention.43
Administering opioids is a task usually conducted by nurses. The dosing errors in our study were mostly related to injectable opioids. Error-prone activities, such as calculating the concentration and administration rate,14 17 require that nurses have sufficient arithmetic knowledge and follow the protocol for safe preparation and administration of injectable medication. However, in daily practice, some nurses have math anxiety, and on average arithmetic knowledge of nursing students seems moderate.44 45 Besides, nurse compliance with protocols for safe administration of injectable medication is considered low (around 20%)46 47 and needs further attention. An intervention which might help to reduce dosing errors during opioid administration is the use of smart infusion pumps. These pumps have integrated medication libraries which allow nurses to set the pump automatically to the right administration rate during administration. By doing so, the administration rate of smart pumps can be seen as a double-check of the nurses’ own calculation. Smart pumps seem also effective in reducing programming errors.48 Furthermore, educational programmes for nurses about brand and generic names and pharmacology of opioids or side effects might increase their knowledge and awareness of risks related to dosing during the administration of opioids.49–51
Overall, we think the ORADE frequency of 8% of all ADEs and 0.3% of all studied patient records found in our study is low and acceptable. However, although the frequency is low, the risk of serious consequences is high. Thus, new contributions to prevent ORADEs in future hospitalised patients need to be identified. Using the Safety-2 perspective may offer new opportunities to do so.52 In order to understand what happened when an adverse (drug) event occurred, it is also necessary to understand how work is done when the process goes well.53 Since healthcare processes have become more complex nowadays, it may be helpful to visualise the current variable practice of prescribing and administering opioids from a multistakeholder perspective.54
Strengths and limitations
Opioids are in the top 10 of drug types that cause fatal medication errors.8 Hence, focusing on the detailed description of the nature of ORADEs was important and necessary. Another strength of this study is that it was based on a comprehensive ADE detection method and conducted in a broad sample of all hospital admissions. Most previous studies, which described the nature of ORADEs, are based on medication-related incident reports. Furthermore, data were gathered over an extended period of time within a randomly selected sample of one-third of all Dutch hospitals.
This study also has some limitations. First, in all three AE studies, the population consisted of relatively many older and deceased patients. Therefore, it is not possible to generalise the results to all Dutch hospital population. To make the study sample more representative for the Dutch hospital population, weighting the results (ie, correcting for type of hospital, study period and discharge status) would be a solution which has been used in previous studies of our research group. However, since the total amount of ORADEs was low, we chose not to weight our results as this had little effect and makes interpretation difficult. Second, overall agreement frequencies between physicians were moderate. This could have led to different assessments or different scores if other experts were involved. This should be taken into account when interpreting our results. However, a previous review of studies focusing on assessing AEs showed also moderate to substantial inter-rater reliability.55 For this reason, patient records in all Dutch AE studies have been assessed by the same experts as much as possible, and over the years these experts have not become stricter or lenient in their judgement of AEs and their preventability.56 Third, due to this low number of ORADEs, it was not possible to compare the events over the three study periods. Therefore, we cannot conclude whether the low number is a positive finding and if the occurrence of ORADEs increased or decreased over time. Fourth, our post-hoc analysis was based on the information previously recorded by the experts in an AE database and on the assessment conducted by these physicians. Therefore, some information could be missing, and interpreting the assessment of preventability was difficult for us in one case, resulting in a non-preventable ORADE. Furthermore, this was also the reason that the harm could not be further categorised according to the National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP) Index for Categorizing Medication Errors.57 Besides, the retrospective interpretation can also be biased by temporal views. The current opinion is that prescribing opioids should be minimised due to the harm of opioids, which is supported by updated guidelines.58 This view changed throughout the years and may not have been recognised 15 years ago, when the focus was mainly on alleviating suffering of pain. This change in opinion may have increased alertness when prescribing or administering opioids, which could have led to less ORADEs. However, our study showed that ORADEs still occur and publishing about them could serve as a method of increasing awareness.
Conclusion
Only 8% of ADEs identified in our sample were related to opioids, 0.3% of all studied patient records. Although the frequency is low, the risk of serious consequences is high. We recommend to use our findings to increase awareness among physicians and nurses. Future interventions should focus on safe dosing of opioids when prescribing and administering, especially in elderly patients.
Acknowledgments
We would like to thank all participating hospitals and independent nurses and physicians for their cooperation during the data collection on the three Dutch adverse event studies. We also thank Peter Spreeuwenberg, MSc, for double-checking the statistical analyses, and Catherine Combee-Duffy, MANP, for improving the readability of this article.
References
Footnotes
Contributors BCFMS, MM, JEK, ML, MdB and CW designed the study and developed the study protocol. BCFMS and MM organised the selection and classification of ORADEs. JEK and IJ double-checked this classification. BCFMS and MM performed statistical analyses and interpreted the analytical results. BCFMS, JEK and IJ wrote the manuscript. MdB and CW supervised the study. All authors made critical revisions and approved the final version of the manuscript.
Funding This study was funded by the Dutch Ministry of Health, Welfare and Sport, with project title Monitor Zorggerelateerde Schade 2015–2018.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The medical ethical committee of the Amsterdam UMC, Vrije Universiteit Amsterdam waived the requirement of informed consent (protocol numbers: 2005.146, 2009.130, 2016.282) as they found the scope of the study outside the Dutch Medical Research (Human Subjects) Act.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. All data relevant to the study are included in the article or uploaded as supplementary information.