Article Text

Abstract
Objectives To explore patients’ and general practitioners’ (GPs’) perspectives on primary care management of patients with type 2 diabetes mellitus (T2DM) in Ningbo, China. We aimed to understand the current benefits and challenges and to identify development priorities.
Design Exploratory qualitative descriptive study using face-to-face interviews and analysed by thematic, inductive analysis.
Setting 11 primary care facilities spread across the city of Ningbo, China.
Participants 23 patients with T2DM and 20 GPs involved in caring for patients with T2DM.
Results GPs were considered the first point of contact and providers of information. However, the care varied, and many GPs lacked confidence and felt overworked. The medication was a particularly weak area. The diagnostic screening commenced late, leading to crisis presentations. Patients were variably informed about their condition, contributing to poor adherence.
Conclusions Future developments of primary care for T2DM in Ningbo should centre around improving GP confidence and workload and patient education and adherence.
- general diabetes
- primary care
- qualitative research
- public health
- international health services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study methodology used a large sample size and purposively selected interviewees spread across the city of Ningbo, ensuring representation of different demographic groups.
The bottom-up capabilities method employed by the study ensures that the findings are relevant to the front-line general practice.
The study methodology used interviewers from a range of professional backgrounds and interviewed both patient and general practitioner participants, thus, improving validity through triangulation of findings.
The recruitment process was unable to avoid selection bias since the patient pool represents only the care-seeking population, and so, it is possible that the views of hard to reach patients or those experiencing significant diabetic stigma maybe under-represented.
Introduction
Type 2 diabetes mellitus (T2DM) presents a global public health issue. Asia’s large population and rapid economic development have made it an epicentre of the epidemic.1 In China, the prevalence of T2DM is now 9.7%, above the global average.2 Ningbo is an economically developed Chinese city, in the northeast Zhejiang Province. In 2015, the prevalence of T2DM in people aged over 40 years in Ningbo was 21%.3 More than half of the patients with T2DM at the diabetes centre at Ningbo First hospital have poor glycaemic control,4 and many have potentially preventable vascular complications.
Primary care in Ningbo is delivered from community hospitals. At the end of 2019, Ningbo had 0.52 registered general practitioners (GPs) per 1000 permanent residents.5 There is a significant heterogeneity in the training pathways taken to practice as a GP, from a 2-year technical degree to a doctorate with research. The most common route is to attend 5 years of medical school followed by 3 years of postgraduate GP training.6 The majority of community hospitals have access to basic laboratory investigations, such as kidney function testing. This may be processed on-site or sent to a linked secondary care facility. In extremely rural areas, GPs that are based at a community hospital may travel to remote village outposts, run from a café or similar, with limited medical facilities. To access laboratory investigations in these settings, the GP makes a recommendation to the patient that they attend a centre with the appropriate facilities, however, there is no system of direct referral.
There are a few allied health professionals in primary care settings. Some centres have a nurse who may perform triage or health education, but physiotherapists and dieticians are found only in secondary care. GPs would usually undertake this work themselves but could refer to a dietician or physiotherapist in secondary care if required. Clinical guidelines are increasingly being developed in China to standardise practice, however, there is still substantial variation between regions7 and specialities, and few clinical guidelines have been developed for primary care.8
In many countries, T2DM is managed successfully by GPs in primary care.9 This benefits the patient with timely, local access to medical support and holistic care. At the health service level, the reduced burden on secondary care allows resource concentration on difficult to treat disease. In China, patients choose whether to present to primary care or see a hospital diabetologist directly as an outpatient. Many patients elect to go straight to the hospital, perceiving they will receive better treatment.10 Standards for T2DM care are broadly comparable between China and countries like the UK where primary care has a more prominent role in T2DM management.2 11 This suggests the potential for a larger role for GPs in China. China’s healthcare system is currently under reform, a central tenant of which is strengthening of primary care12; therefore, the time is right to study this in more detail.
The purpose of this study was to use qualitative research methods to explore patients’ and GPs’ perspectives on primary care management of patients with T2DM in Ningbo, China. We aimed to understand the current benefits and challenges and to identify development priorities, from a front-line perspective.
Methods
The research was conducted according to a predetermined protocol (online supplementary file 1). We followed the Consolidated Criteria for Reporting Qualitative Research guideline for conducting and reporting qualitative research.13
Supplemental material
Study design and participants
An exploratory qualitative descriptive study was conducted among T2DM patients and GPs in Ningbo, China. The study used immersion, thematic coding and inductive analysis to explore the perspectives of both patients and GPs in Ningbo, China, with regard to the management of T2DM in primary care. The inclusion criterion for patients was: diagnosed with T2DM and for GPs was: experience of treating patients with T2DM. Exclusion criteria for all were: cognitive impairment or other condition suggesting vulnerability or inability to give informed consent, acute illness, aged under 18.
Interview guide
Two semistructured interview guides (online supplementary file 2) were developed, one for GPs and another for patients, based on the Chinese Diabetes Society’s guidance on T2DM management.2 The English interview guide was translated into Mandarin Chinese, and the translation checked for accuracy by an independent local translator. A pilot interview was conducted with a local person to ensure clarity and cultural appropriateness of the questions. The interview guide was not formally revised during the study, however, in order to remain responsive to the findings and context, minor adjustments were made to the manner of questioning in later interviews after discussion and agreement with all the interviewers. Regular comparison of approaches between interviewers ensured consistency.
Supplemental material
Recruitment and sampling
Participants were recruited from 11 primary care facilities in Ningbo over a 3-week period in December 2017. Purposive sampling was used to select participants, distributed across 10 geographical districts, to provide a balanced view. One facility was selected (to interview two patients and two GPs) in each district. Yinzhou District is a recent amalgamation of two previous districts; therefore, one facility was visited from each of the former districts. GP participants were approached directly by the research team, via the phone or in person. Patient participants were approached by their GP by phone or during a visit to the health centre. No repeat interviews were conducted. No participants dropped out. Figure 1 depicts the recruitment process.
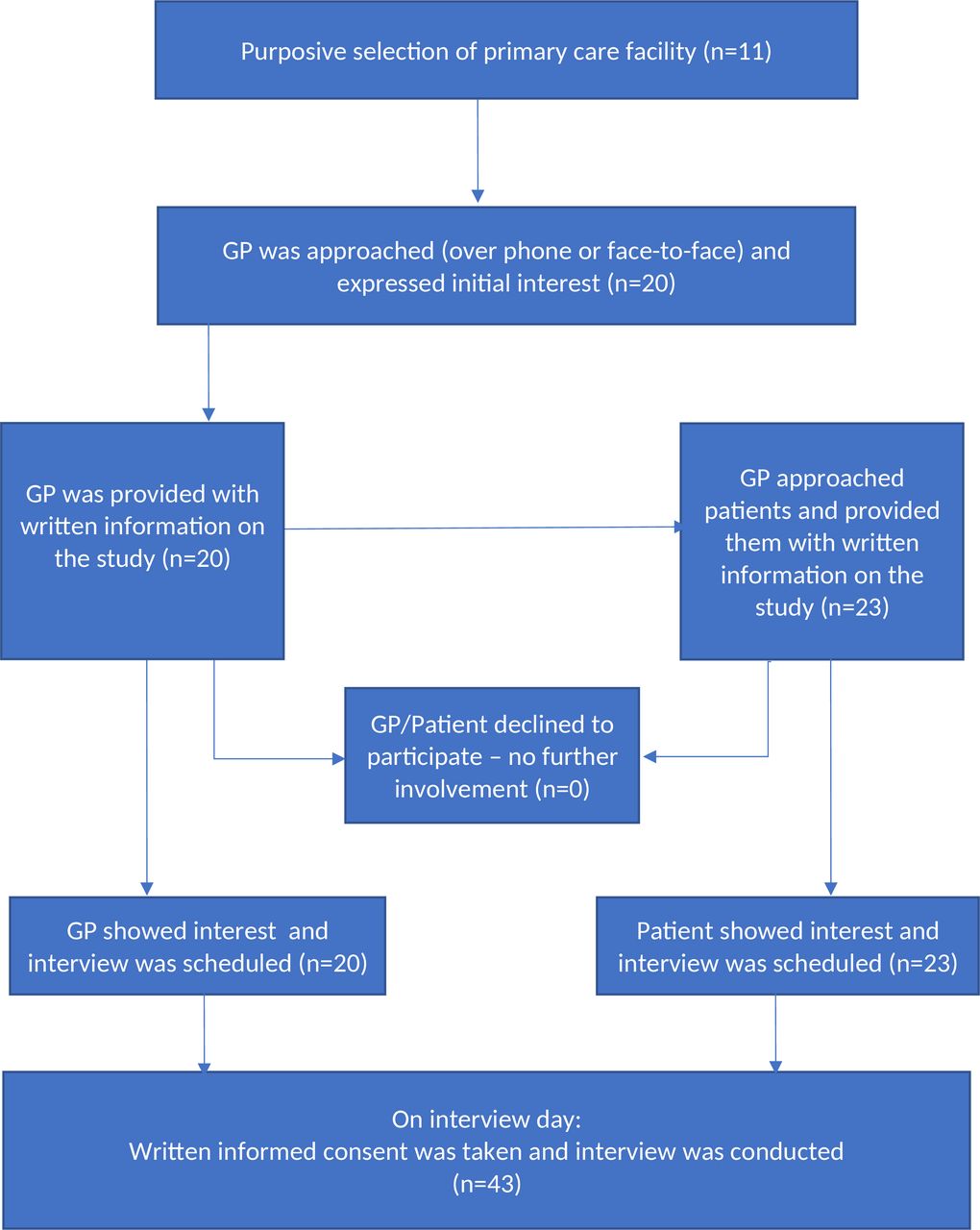
Recruitment strategy flow diagram. GP, general practitioner.
Interview procedure and transcription
Prior to commencing the interviews, the participant information sheet, including information about the study purpose and procedures, was re-explained and a consent form was signed. Interviewees had no prior relationship with the interviewers and knew only that they were healthcare professionals from the UK. Interviewers (AW/PritC/PunaC) were trained in qualitative research methods and the use of the interview guide. Face-to-face interviews lasting between 20 and 45 min took place in private rooms at the primary care facilities. Two interviewers and the interpreter were present at each interview. One interviewer led, the other made field notes. An additional member of the Chinese medical team was present to assist in the clarification of translated medical terminology. Interviewer characteristics are listed in table 1.
Interviewer characteristics.
Interviews were audio-recorded, with permission. The English translation was transcribed (verbatim) and checked for accuracy against the audio. Transcripts were not returned to the participants.
Data analysis
Data were anonymised, securely stored and managed using Microsoft Word and Excel. Transcripts were analysed using immersion, coding and thematic inductive analysis.14–16 All transcripts and field notes were read by one interviewer (AW) and a 10% subset were read and parallel coded by a second interviewer (PunaC) for consistency. After discussion, a coding framework was derived from the data, with broad themes and smaller subthemes. Transcripts were coded by AW with a second 10% subset checked for agreement by PunaC. During the analysis of later interviews, no new themes emerged, suggesting data saturation was reached. Participants did not provide feedback on the findings.
Patient and public involvement
The primary intention of this study was to capture patient views and opinions on primary care for T2DM. However, patients were not directly involved in the design of the research.
Results
A total of 23 patient and 20 GP interviews were conducted. The characteristics of the interviewees are summarised in table 2.
Demographic characteristics of interviewees.
Four overarching themes emerged, as described below. We have presented the patient and GP perspectives together for each theme. The coding tree, figure 2, summarises the overarching themes and subthemes and how they interact.

{kind=link}
{kind=link}
Coding tree describing the interplay between themes and subthemes. GP, general practitioner.
Theme 1: benefits of current GP practice
The first theme focused on the numerous benefits of primary care to patients with T2DM. Patients were overall very positive about the care they received, and the GPs enjoyed their holistic, long-term relationships with patients. The benefits could be further classified into four subthemes.
Improvement on old system
A third of patients talked about being diagnosed before the GP care existed and how the current system is a vast improvement. In the new system, many primary care facilities offered both traditional Chinese medicine (TCM) and Western medicine. GPs felt that TCM and Western medicine could work on shared treatment goals, and patients enjoyed the flexibility of this approach.
When my tablets ran out, I went to TCM instead for 2–3 months, this helped a bit but not enough, so then I recommenced tablets. Patient 11
Holistic care and relationship
Both groups considered holistic care as part of the GP role and an advantage over specialists.
<The main benefit is the> close relationship with patients, like friends or relatives. Specialist doctors cannot achieve such a relationship. GP 2
GPs tailored their advice to family circumstances and aimed to look after both psychological and physical health.
Convenient access and regular contact
Patients highlighted the convenience of the GP as another advantage. GPs held clinic outposts in remote villages, reaching out to patients that might otherwise not be seen. Some patients received all care from the GP as this was more convenient for them.
I haven’t seen a specialist for 2 years. They are far away <in comparison to the GP>. Patient 21
There was regular contact between GPs and patients, sometimes twice a week, although often only for a small task, such as blood glucose monitoring. The frequency was tailored to the individual.
GP knowledge
Patients were confident in their GP’s knowledge, and some considered the GP better than the specialist. Both groups mentioned the GP role in knowledge sharing.
The GP gives me more detailed care and information than the specialist. Patient 5
Although the current care offered many benefits, as described above, we also identified significant variability in the provision of these benefits in practice, reported within theme 2.
Theme 2: variability in current practice
The positive reports of GP care in theme 1 were unfortunately contrasted by wide variability in the practice of GPs and the experiences and behaviour of patients. This theme was subdivided into four subthemes and classified into variability at the GP level (ie, variability in care provision) and the patient level (ie, variability in behaviour and outcomes).
GP level
Inconsistency in primary/secondary care division
Across many care aspects, confusion existed over whether any given task, including diagnosis, medication prescribing or complication screening, should be done in primary or secondary care.
GPs considered themselves the first point of contact in the illness.
We have a very important role in T2DM. We are the first line in prevention and treatment. GP 18
However, after raising the suspicion of T2DM, GPs varied between referring to a specialist for diagnostic confirmation or making the diagnosis themselves. Reasons included low confidence, lacking equipment or perceived patient expectation.
For medication, there was a distinction between first initiating medication and later dose titration. GPs were more comfortable in titrating than initiating. Drug type also mattered, and GPs were more likely to manage tablets than insulin. However, practice ranged from delegating all prescribing to specialists, to initiating both insulin and tablets in primary care. Reasons included safety concerns about hypoglycaemia, patient preference or lack of experience.
If the blood glucose is just a little high, then we will advise on lifestyle change or sometimes start oral medication… insulin is only started by the specialist. GP 8
Reported practice around complication screening was highly variable in the content and frequency, and mostly due to the lack of knowledge or equipment. Many GPs only checked for complications if the patient developed symptoms. Comments such as:
I check for complications including feet, urine and review by an eye doctor—I do this at regular intervals. GP 18
Contrasted with:
There is no regular monitoring. I might feel pedal pulses. GP2
Variable execution of patient education
Although lectures and one-to-one advice was offered widely, there was a significant variation in the quality and content. Some GPs dined with patients in their homes to give practical suggestions of diet alterations or involved the family in lifestyle change, others offered only group education.
If the patient does not listen to my advice, I can tell their families and ask them to help me…together we persuade them to make changes. GP 20
Education by phone or instant messaging was mentioned favourably, but not unanimously offered. Education content also varied, and most discussed exercise and diet, but fewer included important topics, such as self-monitoring and complications.
Patient level
Patient engagement and adherence
Just as GP care provisions were variable and so was patient adherence to clinic attendance, lifestyle change and taking medication. Most patients agreed with the GP as a ‘first contact’, although some felt that it depended on the problem.
For little things like fevers, I will see my GP. If it is more serious, such as stomach ache, I will go directly to a specialist. Patient 3
Many patients admitted poor medication adherence, particularly with insulin. Only half of the patients reported eating healthily or exercising. Reasons included self-reported ‘laziness’, lack of awareness, time pressure, hunger or believing tablets were more important.
My blood glucose is controlled by tablets, so diet change is not necessary. Patient 12
Only a few patients measured their own blood glucose. GPs promoted self-monitoring in patients for whom they felt it was appropriate.
Nearly half of the patients had not attended the screening for complications; usually, because they felt well, and therefore, did not see a need. Patients did not view the lack of adherence as a problem, but it concerned GPs greatly.
Crisis presentation and complication development
This outcome was often the result of the described care provision and adherence issues. Many patients had been diagnosed suboptimally, ‘in crisis’, after presenting with disease manifestations.
I was losing weight, tired and dizzy, so I went to the hospital. Patient 2
In Ningbo, GP screening for T2DM starts at the age of 65, but the condition often develops much earlier; therefore, younger patients might go undiagnosed and present in crisis. Some reported screening younger people with risk factors but did not mention a specific guideline. Half of the patients already had complications. Some were waiting for symptoms before attending the screening for complications.
I know that there are complications, but I do not do any tests for them because at the moment I feel good. Patient 13
As described, the observed variability affected different aspects of care. Theme 3 explored factors found to contribute to the variability.
Theme 3: factors in the variability of care and engagement
There were five main subthemes that contributed to the observed variability, which were also subdivided into the patient and GP level. In addition to contributing to care variability, many of these factors were further propagated by the inconsistency, in a self-reinforcing cycle.
GP level
Low GP morale and confidence
This was both a cause and an effect of the variable care. Underconfident GPs felt unable to perform all T2DM-related tasks, reinforcing their low morale. Inadequate diagnostic equipment in some cases made hospital referral inevitable. In contrast to patients, whose confidence in the GPs knowledge has been highlighted, most GPs mentioned limits to their capabilities and felt, incorrectly, that patients lacked confidence in them.
I am a GP, not a specialist, and so, I am less experienced in treating diabetes. GP 17
GP overwork
High patient-GP ratios left GPs overworked. Short consultations, sometimes only for 2 min, prevented them from fully addressing the patient’s agenda or their own. Overwork also reduced the time for continuing professional development, and thus, compounded the morale problems described.
Our work is very busy, but we do need more training. GP 20
Patient level
Variable patient knowledge
Patients' understanding of their condition and treatment was very variable. GPs reported that low population health literacy exacerbated poor adherence. Patients' misconceptions, such as the condition being infectious, caused diabetic stigma. Patients then avoided health education lectures since attending meant acknowledging the illness publicly. Thus, the cycle was perpetuated.
I like to keep my diabetes a secret—I am afraid of other people’s opinions. Patient 17
Patient time factors
These influenced patients’ care-seeking behaviour. Patients avoided the screening for complications at hospitals due to the long queues or attended the GP less frequently than recommended.
I avoid coming to the GP… I have to work and look after my child; so, it would not be convenient to come more often. Patient 11
Cost of care
Patients lamented the expense of medication and doctors’ appointments for their chronic condition. GPs mentioned that patients sometimes refused treatment or monitoring on cost grounds.
The price of the medicine puts some patients off. GP 17
And so, given the benefits of current practice, but also the variability and factors in that variability, what are the ways forward towards improvement? Some suggestions were made by interviewees and others have emerged during analysis.
Theme 4: suggestions for improvement
There were three broad strategies that emerged from the study that could improve primary care for T2DM. In most cases, these addressed one or more of the factors found to introduce variability of practice.
Improvements in GP training
Much of the observed lack of confidence and morale was rooted in GP perceptions that they lacked knowledge. Improved training might address this. Three specific areas were suggested. During GP interviews, researchers noted in field notes that guidelines were rarely mentioned. Their use could improve treatment consistency and provide clarity over the primary/secondary care division. Second, GPs requested practical training in T2DM-specific competencies during their training and time to keep updated thereafter. They felt that improved GP knowledge would translate to improved patient care and reduced need for specialist input. Finally, GPs also desired training in consultation skills to successfully motivate patients to improve their lifestyle and adherence.
I would like training in how to carry out effective patient education. GP 20
Improved care efficiency
Several possible methods to improve care efficiency emerged. These were intended to reduce the described GP workload and make better use of patients’ time. Suggestions included the use of allied health professionals, peer teaching by experienced T2DM patients and a nominated ‘community GP’ dedicated to visiting rural villages, to spare health centre-based GPs from travelling.
I hope that we will have a nurse with training in T2DM, so that we can organise more activities for the patients. GP 11
I think that it would be helpful for newly diagnosed diabetics to learn from those with more experience. Patient 10
Improved provision of medication and equipment
Lacking equipment was a common reason for GPs failing to perform complication screening or diagnosis, and this should be addressed. Medication cost contributed to the lack of adherence, and so, the reduced cost to the patient could improve T2DM outcomes.
Discussion
Main findings of this study
The present study highlighted many benefits, but also identified a current central variability, which formed the basis of a self-propagating cycle with negative consequences for patients and GPs. The significant variation in practice and experience observed across the GP pool supports the need for a standardised set of T2DM competencies for GPs. Barriers currently facing GP care for T2DM in Ningbo include GP morale and overwork and patient education and adherence. There is a need to improve health literacy and lifestyle at the population level. The diagnostic T2DM screening programmes currently operating in Ningbo should be extended to include younger people with risk factors, and major improvements in the screening for complications are required to promote patient awareness and reduce late presentation. Skilled allied health professionals could support GPs to reduce overwork.
Strengths and limitations of this study
We demonstrated the use of a ‘bottom-up’ capabilities approach17 to evaluate the care of patients with T2DM in China, ensuring findings are relevant to front-line general practice. Such approaches have previously been recommended to guide China’s current reform.12 Collecting both patient and GP viewpoints for comparison and employing researchers from a range of professional backgrounds for interview conduct and analysis increases the validity of our findings. The qualitative, thematic analysis methodology employed generated rich data, giving a more in-depth understanding of the issues. The study had a large number of participants and explored and compared the perspectives of both patients and GPs. Findings were triangulated across researchers of different backgrounds and with the wider body of literature. These factors strengthen the credibility and quality of a study.18 However, a qualitative approach also brings inherent limitations, such as the lack of repeatability. Furthermore, the selection and recruitment of patients relied on GP assistance; therefore, the pool reflects the ‘care-seeking’ population and might have excluded those with barriers to attendance. Those with the strongest views might have volunteered for the interview. Patients who felt most diabetic stigma might have avoided the interview (and thus, under-represented). Due to the subject matter, translators were sometimes assisted by another healthcare professional, which could have influenced the patient responses.
Our findings in the context
We have described the divergent views of patients and GPs about the quality of primary care for T2DM in Ningbo. Patients generally reported satisfaction whereas GPs were aware of many deficiencies. The lack of confidence about meeting patient expectations was observed to reduce job satisfaction among Chinese doctors in a previous study,19 in keeping with our observations. In an earlier work, the patient confidence was also low,10 which was not the case in our sample. GP perceptions might have lagged as patients have gained confidence. In Swedish primary care, the use of clinical guidelines was found to be an important confidence source for GPs.20 This could be a potentially useful strategy in China to improve GP confidence and consistency of care. Clinical guidelines were noted in our study, as in the wider literature,7 to be underutilised in China.
The current heterogeneity of GP training in China is considered to have a negative effect on the quality and consistency of primary care in China,6 and our findings were consistent with this. Our suggestion to improve GP training is in agreement with the existing recommendations in the wider literature as China proceeds with its current healthcare reform and the goal of providing universal care.21
Time pressure on GPs in China and the resultant detriment to care were in keeping with a previous study.19 We highlighted a need to improve the consistency of patient education, which is a crucial component of T2DM management. Education increases treatment adherence22 and self-monitoring of blood glucose,23 both of which were lacking in our findings. A previous study in China showed that improved patient knowledge was successful in improving health outcomes in T2DM,24 and this is corroborated by literature worldwide.25–27 Family education, as proposed by some interviewees in this study, has proven efficacy in improving T2DM control.28
Implications of the results
China’s primary care system is currently in a phase of redevelopment,12 and this study provides many important insights. The current system has many advantages, but several areas for improvement. These may be addressed through GP training and workforce changes. Future interventions should focus on GP morale and facilitate the learning of competencies, such as insulin prescription, supported by the routine use of clinical guidelines. Patient interventions to consider include peer education and family interventions.
Unanswered questions and future work
Future work should focus on the development, implementation and evaluation of the suggested interventions. In order to further triangulate the findings, views of secondary care doctors and patients and allied health professionals could be explored through additional interviews.
References
Footnotes
AW and LL are joint first authors.
Contributors AW and LL are co-first authors. Conception and design: AW, KC, JS, JL, PritC. Acquisition of data: AW, JL, KH, PunaC, PriyC, GT, PritC, LL. Analysis and interpretation of data: AW, KC, JS, PunaC. Drafting of the manuscript: AW, KC, JS, LL. Critical revision of the manuscript for important intellectual content: all. Statistical analysis: not applicable. Obtaining funding: PritC, KC. Administrative, technical or material support: JL, KH, PriyC, GT, LL. Supervision: KC, JS, PritC, LL.
Funding This work was supported by the University of Nottingham, Health Education England and Ningbo First Hospital.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Faculty of Medicine and Health Sciences Research Ethics Committee, University of Nottingham (ethics reference no: 132-1710) and Ningbo First Hospital Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available since all the interview transcripts are confidential, as per the protocol.