Article Text

Abstract
Objectives The objectives of this study were to describe the demographic profile and baseline disease characteristics of patients with psoriatic arthritis (PsA) treated with either infliximab (IFX), subcutaneous golimumab (GLM) or ustekinumab (UST) treatment in Canadian routine care setting along with assessing long-term effectiveness and safety.
Methods Patients with PsA were enrolled into the Biologic Treatment Registry Across Canada registry (ClinicalTrials.gov Identifier: NCT00741793) from 2005 to 2017. The study visits occurred at study enrolment (baseline) and every 6 months thereafter. Effectiveness was assessed by changes in disease parameters (joint counts, Psoriasis Area Severity Index (PASI), Health Assessment Questionnaire, patient/physician global, minimal disease activity, enthesitis, dactylitis, erythrocyte sedimentation rate, C reactive protein). Improvements from baseline were explored with the paired t-test and the McNemar’s test. Safety was evaluated by assessing the incidence of adverse events (AEs) and drug survival rates.
Results A total of 111 IFX-treated, 281 GLM-treated and 70 UST-treated patients were enrolled. Most baseline disease parameters remained similar over time in all three cohorts. UST-treated patients had lower mean baseline Disease Activity Score in 28 joints CRP, swollen joint based on 28 joints and higher PASI compared with patients treated with GLM. Treatment with IFX, GLM and UST was associated with significant improvements in all disease parameters over time (p<0.001) from baseline up to 84, 84 and 40 months, respectively.
AEs were reported for 74.8%, 69.8% and 52.9% (138, 114 and 115 events/100 patient-years (PYs)) covering 325, 567 and 87 years of exposure for IFX-treated, GLM-treated and UST-treated patients, respectively. Severe AEs were reported in 19.8%, 8.5% and 5.7% (8.8, 7.2 and 8.0 events/100 PYs) in IFX-treated, GLM-treated and UST-treated patients, respectively. The proportion of patients who discontinued treatment were 63.1%, 50.9% and 50.0%, respectively.
Conclusions IFX, GLM and UST treatment significantly reduced disease activity and improved functionality in patients with PsA followed by routine clinical practice and had a safety profile similar to that previously reported in the literature.
Trial registration number NCT00741793.
- immunology
- rheumatology
- clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
These are the primary results from Biologic Treatment Registry Across Canada, one of the largest and longest running rheumatology registry in Canada.
This study includes effectiveness and safety data from patients treated with golimumab, for which very little real-world data have been published so far.
The results presented reinforce the effectiveness and safety profile of anti-tumour necrosis factor therapy in a real-world population with psoriatic arthritis over a very long follow-up (in the cases of golimumab and infliximab).
Limitations of this study may include channelling bias, survival bias as well as performance bias, such as in cases where the level of care may have differed across enrolment periods.
Introduction
Psoriatic arthritis (PsA) is a chronic, systemic inflammatory disease impacting the joints, skin, entheses and other organs with a heterogenous presentation and variable progression. The overall prevalence of PsA in the general population is 0.3%–1.0%.1–3 In accordance with disease severity, various treatment options may be selected. Non-steroidal anti-inflammatory drugs (NSAIDs) are generally provided as first-line therapy for peripheral and axial disease. Intra-articular treatment may further be prescribed for local disease.4 Moderate-to-severe disease may require the concomitant administration of NSAIDs and conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), such as methotrexate (MTX).5 6 Anti-tumour necrosis factor (anti-TNF) agents, including infliximab (IFX), etanercept, adalimumab and golimumab (GLM) and interleukin (IL)-12/IL-23 inhibitors such as ustekinumab are part of the biologics class of therapies indicated for patients who have moderate-to-severe PsA who have an intolerance to NSAIDs or csDMARDs.7–10 Relatively recently, IL-17A antagonists and JAK inhibitors have been approved and are available for use in Canada.
All these agents have been evaluated in randomised controlled studies with a randomised controlled period of no more than 6 months and a follow-up period extending from 2 to 5 years.11–13 Patients from these randomised controlled studies are not always representative of the general population due to many inclusion and exclusion criteria. Therefore, data from long-term observational studies are essential to confirm the efficacy and safety profile of new therapies, especially in diseases such as PsA that has a significant heterogenous presentation and comorbidities.14 15 There are only a few registries specifically focused on patients with PsA,16–19 although a number of psoriasis registries do include a subset of patients with PsA.20 21
The objectives of this study are to describe the demographic profile and baseline disease characteristics of patients with PsA over time who were selected for IFX, GLM or UST therapy in Canada as per routine care, and to describe the real-world survival, safety and effectiveness of these drugs.
Patients and methods
Study design
The Biologic Treatment Registry Across Canada (BioTRAC, ClinicalTrials.gov Identifier: NCT00741793) was a Canadian, prospective, multicentre, registry that collected real-world clinical, laboratory, safety and patient-reported data among patients with PsA, ankylosing spondylitis (AS) and rheumatoid arthritis (RA) treated with IFX, GLM or UST during routine care in Canada between 2002 and 2018. BioTRAC was initially established in 2002 to follow patients with RA treated with IFX.22 Patients with PsA treated with IFX were enrolled from 200523 and followed until 2017. The registry was subsequently expanded to include GLM-treated24 and UST-treated patients from 2010 to 2014, respectively and these patients were followed until 2018. Interim analyses of the IFX and GLM cohorts were published previously.23 24 The historical development of the registry has been described previously.22 23 Data from this study were presented at the 2019 Canadian Rheumatology Association,25 Panamerican League of Associations for Rheumatology 26 and European League Against Rheumatism27 conferences.
Patient population
For the purposes of this analysis, patients with PsA who initiated IFX, GLM or UST treatment as per their respective Canadian Product Monograph were included. Patients with PsA, either bio-naïve or with one prior biologic agent exposure were enrolled and followed for up to 12 years, with a study visit at baseline and every 6 months thereafter. Information on screened but not enrolled patients was not collected.
Patients treated with IFX were enrolled from 2005 until 2015 and followed until 2017 or until permanent treatment discontinuation, whichever occurred first. Enrolment for GLM-treated and UST-treated patients occurred between 2010 and 2014, and they were followed until 2018 or until permanent treatment discontinuation. All analyses were conducted in the full analysis set comprising patients receiving treatment without major eligibility violations.
Data collection
Study assessments took place per routine practice at each participating site with recommended visits at baseline and every 6 months thereafter. The following clinical, laboratory and patient-reported outcomes (PROs) were collected as per routine care: C reactive protein (CRP), erythrocyte sedimentation rate (ESR), tender joint count based on 28 joints (TJC28), swollen joint based on 28 joints (SJC28), Health Assessment Questionnaire (HAQ), patient global assessment (PtGA), physician global assessment (MDGA), Psoriasis Area Severity Index (PASI), morning (AM) stiffness, pain, enthesitis (16 locations including supraspinatus, medial epicondyle of the humerus, lateral epicondyle of the humerus, greater trochanter, quadriceps-to-patella, patellar-tibia, Achilles and plantar fascia), dactylitis and acute phase reactants (CRP, ESR).28 Safety was assessed with the incidence of treatment-emergent adverse events (AEs).
Statistical analysis
The current study includes data from two distinct statistical analysis plans. The first one covered the IFX cohort and was filed in May 2018. The second statistical analysis plan covered the remainder of cohort and included patients treated with either GLM or UST. Since the investigators had already been exposed and were aware of the IFX data, a decision was made not to do any statistical analysis comparing the IFX and GLM/UST cohorts. Nonetheless, comparative data are presented herein, as it provides an interesting vision of how patients with PsA evolved over the years and how each drug was used. To that effect, an analysis of patient baseline profile was conducted based on enrolment period, specifically, 2006–2008, 2009–2012, 2013–2015 and 2016–2017. These periods were chosen based on protocol amendments and/or major changes in market dynamics.
All outcomes included in the ‘Data collection’ section were assessed descriptively using the median and/or mean and SD, 95% CIs of the mean for continuous variables, and frequency distributions for categorical variables. Data were expressed as observed and missing data were not extrapolated. Variations in patient demographics and baseline characteristics across enrolment periods were assessed using the Kruskal-Wallis test for continuous variables and the χ2 test for categorical variables. There was no imputation for missing data.
Kaplan-Meier survival analysis and Cox proportional hazards models were used to assess the time to discontinuation and survival rates. AEs were coded using the Medical Dictionary for Regulatory Activities (V.20.0), and the proportion of patients who experienced an AE along with incidence rates were summarised by preferred term (PT). Statistical analyses were conducted with SPSS V.24.0 (SPSS, Chicago, Illinois, USA) and SAS V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Of the 111 IFX-treated, 281 GLM-treated and 70 UST-treated patients, the proportion of males was 52.3%, 46.3% and 37.1%, the mean age was 48.4, 52.8 and 53.1 years and the mean disease duration was 5.8, 6.1 and 5.7 years, respectively. Most patients were bio-naïve (85.6%, 77.9% and 55.7% for IFX, GLM and UST, respectively (p<0.001 GLM vs UST)) (table 1).
Patientdemographics and baseline characteristics
Patients treated with IFX received a mean (SD) dose of 4.28 (1.35) mg/kg, over a median (min–max) of 14 (1–80) infusions representing a total exposure of 325 years. All GLM-treated patients started at the 50 mg dose monthly and received a median (min–max) of 14 (1–103) injections representing a total exposure of 281 years. Two patients (0.7 %) received 50 mg injections at shorter than every 28 days intervals while 33 patients (11.8 %) received 50 mg injections at every 28–32 days intervals throughout the study. UST-treated patients received a median (min–max) of 8 (1–18) injections representing a total exposure of 87 years. Twenty-six (37.1 %) patients started at the 90 mg dose while the remaining patients started at the 45 mg dose. Fifteen of those patients (34.9 %) were dose-optimised to 90 mg after a median (SD) of 2.3 (0.3) years.
Compared with GLM-treated patients, UST-treated patients had a significantly lower mean baseline Disease Activity Score (DAS) in 28 joints CRP (3.4 vs 3.9; p=0.0031), DAS ESR (3.3 vs 3.9, p=0.0035), SJC (3.8 vs 5.3; p=0.0046), lower incidence of previous and concomitant NSAIDs and csDMARDs (p<0.02), a higher baseline PASI score (4.8 vs 2.2; p=0.0061) and were more likely to have been treated with a previous biologic agent. In addition, UST-treated patients were less likely to receive concomitant NSAID or csDMARD treatment at baseline and more likely to receive concomitant corticosteroids.
As shown in figure 1, a reduction in mean baseline duration of morning stiffness was observed in the IFX cohort (from 69.8 to 42.6 to 23 min in 2006–2008 to 2009–2012 to 2013–2015; p=0.003). Previous use of NSAIDs and MTX was also significantly different across enrolment periods in IFX-treated patients, with a higher proportion of patients reporting previous NSAID use in earlier years (2006–2008 vs 2009–2012 vs 2013–2015: 69% vs 70% vs 39%; p=0.028) and more patients reported MTX use in the most recent enrolment period (73% vs 73% vs 87%; p=0.020). Most other baseline disease parameters remained similar over time in all three cohorts.
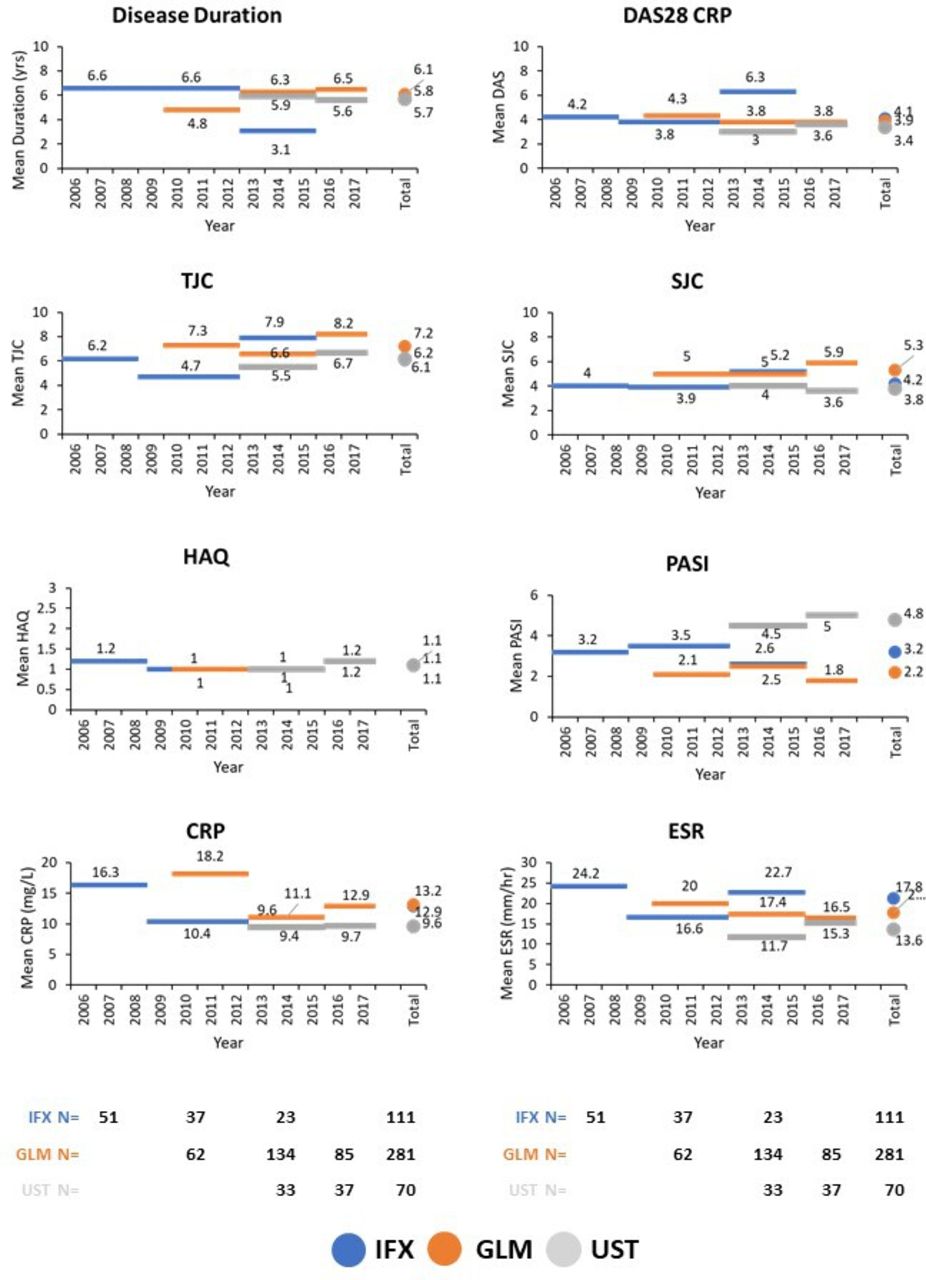
Evolution of baseline characteristics over time. CRP, C reactive protein; DAS28, Disease Activity Score in 28 joints; ESR, erythrocyte sedimentation rate; GLM, golimumab; HAQ, Health Assessment Questionnaire; IFX, infliximab; PASI, Psoriasis Area Severity Index; SJC, swollen joint count; TJC; tender joint count; UST, ustekinumab.
Treatment with IFX, GLM and UST was associated with significant improvements in most disease activity parameters over time (p<0.001) from baseline up to 84, 84 and 40 months, respectively, with similar effectiveness between agents (figure 2 and online supplementary figures S1, S2). The proportion of patients in minimal disease activity (MDA) at 12, 24 and 36 months reached 40.7%, 50.0% and 55% in IFX-treated patients; 64.7%, 68.8% and 78.9% in GLM-treated patients and 58.8%, 60.0% and 83.3% in UST-treated patients (p=0.004 and p<0.001 vs IFX). IFX, GLM and UST patients showed a significant improvement in dactylitis while only IFX-treated and GLM-treated patients showed significant improvement in enthesitis (online supplementary figure S1).
Supplemental material
Effect of treatment with IFX, GLM and UST on enthesitis, dactylitis, CRP and ESR over time. Observed data. P valuevs baseline.
{kind=link}
{kind=link}
Effect of treatment with IFX, GLM and UST on disease parameters over time. Observed data. P value versus baseline. GLM, golimumab; HAQ, Health Assessment Questionnaire; IFX, infliximab; PASI, Psoriasis Area Severity Index; PtGA, patient global assessment; SJC, swollen joint count; TJC; tender joint count; UST, ustekinumab.
The proportion of patients who discontinued treatment were 63.1%, 50.9% and 50.0% over a mean exposure of 2.9, 1.9 and 1.2 years and a median time to discontinuation of 45.9, 38.2 and 27.2 months for IFX, GLM and UST, respectively (online supplementary figure S2). The reasons for discontinuations are shown in table 2.
Discontinuations and reasons for discontinuations
AEs were reported for 74.8%, 69.8% and 52.9% (138, 114 and 115 events/100 patient-years (PYs)) and severe AEs (SAEs) for 19.8%, 8.5% and 5.7% (8.8, 7.23 and 8.02 events/100 PYs) covering 325, 567 and 87 years of exposure for IFX-treated, GLM-treated and UST-treated patients, respectively (tables 3 and 4). For IFX-treated patients, the most commonly reported AEs were nasopharyngitis, headaches and arthralgia. Drug ineffective and nasopharyngitis were most often reported for GLM-treated and UST-treated patients. Only one GLM-treated patient experienced a uveitis AE and only one IFX-treated patient experienced a Crohn’s disease AE. The incidence of serious infections was found to be 0.95, 1.24 and 1.17/100 PY in IFX-treated, GLM-treated and UST-treated patients, respectively. No more than one type of serious infection occurred in any given cohort. Five patients experienced an opportunistic infection: two onychomycosis in IFX-treated patients and three candidiasis in two GLM-treated and one UST-treated patients. The incidence of malignancies was found to be 1.26, 3.18 and 5.73/100 PY in IFX-treated, GLM-treated and UST-treated patients, respectively. The only types of malignancies that occurred more than once in any of the cohorts were basal cell carcinoma (two IFX and two GLM), seborrhoeic keratosis (one IFX and two GLM) and skin papilloma (three GLM). There were two pregnancies, both in GLM-treated patients, one of which concluded with a spontaneous abortion. There were two deaths: thalamus haemorrhage in an IFX-treated patient and a squamous cell carcinoma in a GLM-treated patient.
Adverse events (SOC with PT terms occurring in ≥2% of patients with at least one agent)
Serious adverse events (SOC term) occurring in ≥0.5% of patients per agent
Discussion
The aim of this real-world study was to describe the patient profile of patients with PsA treated with IFX, GLM and UST in Canada between 2006 and IFX, 2018 and IFX, and to evaluate the effectiveness and safety of those agents during routine care. Limited information exists concerning the use of biologic agents in patients with PsA and, to our knowledge, this registry represents one of the earliest prospective, multicentre observational study of biologic therapy in patients with PsA.
Comparison between enrolment periods demonstrated temporal differences in a few baseline patient and disease characteristics, including treatment history and disease parameters. These results suggest a change in patient management over time, whereby there may have been a shift away from NSAID as a first-line therapy towards more frequent MTX use in more recent years. This shift could be due to better understanding of long-term risks associated with NSAIDs, and its intended short-term use,29 while MTX is known to be relatively tolerable in patients with PsA and can be used as a long-term therapy with dose escalations, suggesting it could be a more appealing option for first-line therapy.30 However, there did not appear to be any changes in disease duration and overall disease activity over time when starting a biologic agent, whereas a substantial reduction in disease duration and disease activity was observed in patients with RA and AS initiating treatment with IFX, from its initial approval until 2012.22 31 This lack of change in disease duration and disease activity over time could be driven by a lower sense of urgency when patients do not have erosions at baseline and possibly less pain. Additionally, a large majority of patients with PsA initially present with skin symptoms and, therefore, could spend many years under the care of a dermatologist before being transferred to rheumatology care on the appearance of joint symptoms and pain.
Both anti-TNFs and UST demonstrated similar effectiveness to decrease disease activity and improve function. One difference among the three agents was MDA status where the proportion of patients achieving that state was greater in GLM-treated and UST-treated patients. For UST this may be partially explained by lower joint disease burden at baseline. Also, since the data presented are from ‘observed’ patients, it could also be reflective of the disease state at which a therapy is deemed to be effective. Indeed, the proportion of patients achieving very low disease activity (VLDA) status was quite similar between the three cohorts. One peculiar observation was that UST-treated patients did not appear to show improvements in enthesitis, CRP or ESR scores in this cohort, although there are multiple reports that UST can decrease enthesitis and acute phase reactants in clinical studies.32–34 We did observe differences in baseline disease activities between GLM-treated and UST-treated patients, whereby patients treated with the anti-IL-12/IL-23 tended to have more skin symptoms over joint involvement. Also, public access to UST for the treatment of PsA is limited to only two provinces across Canada (Saskatchewan and Quebec) and this is reflected in the low number of overall and bio-naïve patients in the registry. Patients that have failed previous biologic therapies are usually more challenging to treat,10 which may be reflected in the number of patients that were started at the 90 mg dose, the higher of the two doses for UST and patients who were optimised.
IFX-treated patients with PsA had better retention and a longer median time to discontinuation compared with GLM-treated or UST-treated patients. Also, a larger proportion of GLM-treated and UST-treated patients discontinued treatment due to lack of response while a larger proportion of IFX-treated patients discontinued due to an AE. Although such differences could be explained by variations in their relative benefit/risk profiles, they are more likely driven by a lower availability of alternative biologic therapies in earlier time periods. Indeed, most IFX-treated patients were enrolled between 2006 and 2012 while most GLM-treated and UST-treated patients were enrolled after 2013 (figure 1). IFX-treated patients who enrolled in earlier years, specifically between 2006–2008 and 2009–2012, were significantly less likely to discontinue treatment compared with those enrolled between 2013 and 2015. It is plausible that a patient on IFX without alternative treatment in case of treatment failure would be more likely to remain on therapy, despite a suboptimal response, until another reason such as an AE results in a discontinuation. This hypothesis is supported by the observed proportion of patients achieving MDA status, which reached almost 70% of GLM-treated and UST-treated patients over 4 years, while the proportion of IFX-treated patients never went above 50% during that same period. Another compounding factor is a 2014 protocol amendment that led to changes in the ‘End of Participation’ questionnaire and the addition of lack/loss of response as an AE of special interest. This would disproportionately impact the GLM and UST cohort as most of these patients were enrolled from 2013 onwards, and a higher incidence of ‘drug effect decreased/ineffective’ AEs were reported. A German registry (GO NICE) of GLM-treated patients reported a retention rate of 42% at 2 years,35 which is >50% rate found in BioTRAC and the 48% rate from another cohort in Northern Italy.36 However, this could be explained by the lower proportion of bio-naïve patients in GO-NICE.35
The incidence of AEs and SAEs was found to be quite similar between IFX-treated, GLM-treated and UST-treated patients, although some differences were noted. Patients treated with IFX had a greater incidence of headaches, arthralgia and back pain compared with GLM-treated patients, all of which could be the result of acute or delayed infusion reactions.37 Although the overall incidence of infections and serious infections were similar between the three cohorts, both IFX-treated GLM-treated patients reported a similar incidence of pneumonia (about 2/100 PY) while none was reported in any UST-treated patients. Overall, the incidence of AEs, SAEs and discontinuations due to AEs were comparable with or lower than those reported in other long-term studies with anti-TNF agents.38–42
Limitations of this study may include channelling bias, survival bias as well as performance bias, such as in cases where the level of care may have differed across enrolment periods. These biases should be considered when contrasting the findings with other registries. Data quality, including missing data, also varied over enrolment period due to protocol amendments, changes in standard operating procedures between the three study sponsors and improvements in AE reporting. In addition, patient comorbidities were not systematically recorded by the treating physicians. As such, a comprehensive analysis of factors associated with improved efficacy and/or increased AEs was not possible. Another limitation is that joint assessments were only done in 28 joints, although a full 66/68 joints assessment would be required to assess MDA and VLDA. When PsA was included in BioTRAC in 2005, a complete joint assessment was not considered as standard of care in the majority of Canadian community centres compared with academic institutions. Despite this limitation, studies have reported that the 28 and 66/68 assessments are highly correlated and that differences between the two are rather small in terms of sensitivity and specificity. The incidence of AEs may also have been underestimated given that patients were seen under routine care, resulting in long interval lengths between visits which may lead to recall bias. The strength of the study pertains to the generalisability of real-world data as disease characteristics are similar to those described in another Canadian registry, as well as the larger population size and longer study duration, allowing the assessment of long-term effectiveness and safety of biologic agents in patients with PsA followed as part of routine clinical care.
In conclusion, although the number of patients in the UST cohort were small, differences in baseline characteristics between patients treated with an anti-TNF over an anti-IL-12/IL-23 agent suggest that the level of joint to skin involvement could be driving physician choice when the time comes to choose a biologic agent. IFX, GLM and UST treatment significantly reduced disease activity and improved functionality in a similar fashion and were well tolerated in patients with PsA.
Acknowledgments
This study is dedicated to the memory of William G. Bensen MD, who was BioTRAC’s primary investigator from its inception in 2002 until his premature passing on 15 March 2017. The authors are indebted to the BioTRAC investigators, nurses, study coordinators and to the individuals who were involved in its design, management, data generation and dissemination: Vincent Letourneau, John Leombruno, Hayssam Khalil, Chad Mitchell, Sophie-Elise Michaud, Frank Hack, Nader Khabboul, Heidi Imhoff, Susan Otawa, May Shawi, Kathy Tkaczyk, Karina Maslova, Brendan Osborne, Odalis Asin-Milan, Meagan Rachich, John S. Sampalis, Eliofotisti Psaradellis, Nadia Longo, James Vaillancourt, Angela Karellis, Saliha Boumaza, Patricia Bandeira, Karen Landers, Clara Fehrmann, Julie Dinniwell, Debra Mitchell and Sandra Sitar. The authors would like to thank all the people living with psoriatic arthritis that shared their time in the study to help better understand the impact of their disease.
References
Footnotes
Contributors PR, RA, MK, DS and MS were involved in recruitment. ER was involved in biostatistical analysis. ER, AJL and FN were involved in the study design and FN wrote the manuscript. All authors were involved in data analysis, reviewed and edited the manuscript and approved the final version.
Funding This study was financed by Schering-Plough (2002–2010), Merck (2010–2012) and Janssen Inc. (2012–present).
Competing interests PR has received consulting fees for Abbott, AbbVie, Amgen, BMS, Celgene, Janssen, Novartis, Pfizer and Roche; and received research grant from Janssen. RA, DS and MS received grant/research support from Janssen. MK received grant/research support from Novartis and consultant fees from Amgen, Celgene, Gebro, Janssen, Novartis, Pfizer, Lilly and Merck. AJL and FN are employees of Janssen Inc. and are JNJ stockholders.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Prior to enrolment, patients were required to provide written informed consent to participate. Ethics approval was obtained from a central Research Ethics Board (IRB Service, Ontario, Canada) for private practices, and from respective Research Ethics Boards for institutional sites. The study was conducted in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Janssen has an agreement with the Yale Open Data Access (YODA) Project to serve as the independent review panel for evaluation of requests for CSRs and participant level data from investigators and physicians for scientific research that will advance medical knowledge and public health. For more information on this process or to make a request, please go to https://yoda.yale.edu/