Article Text

Abstract
Objective As the cost-effectiveness evaluation of cinacalcet and conventional therapy in China has not been reported, the objective of this study was to make a pharmacoeconomic evaluation of cinacalcet specific to the Chinese healthcare setting in patients with moderate-to-severe secondary hyperparathyroidism (SHPT) undergoing dialysis.
Designs Data from Evaluation of Cinacalcet Therapy to Lower Cardiovascular Events trial were used for this analysis. A semi-Markov model was constructed to estimate quality-adjusted life years (QALYs) and lifetime costs in cinacalcet plus conventional therapy (cinacalcet strategy) compared with conventional therapy (standard strategy), in patients with moderate-to-severe SHPT undergoing dialysis. Treatment effect estimates from the unadjusted intent-to-treat (ITT) analysis and covariate-adjusted ITT analysis were used as the main analyses. Model sensitivity to variations in individual inputs and overall decision uncertainty were assessed through probabilistic sensitivity analyses.
Primary and secondary outcome measures Incremental cost-effectiveness ratio (ICER) as measured by cost per QALY gained.
Results The ICER for cinacalcet strategy was US$44 400 per QALY gained using the covariate-adjusted ITT analysis. Probabilistic sensitivity analysis suggested a 46.2% chance of the ICER being below a willingness-to-pay threshold of US$26 508. Treatment effects from unadjusted ITT analysis yielded an ICER of US$87 210 per QALY. The model was most sensitive to the treatment effect on mortality.
Conclusions Existing evidence does not support the cost-effectiveness of cinacalcet strategy in patients with moderate-to-severe SHPT undergoing dialysis when applying a willingness-to-pay threshold of US$26 508 per QALY, whether it is using the treatment effect from covariate-adjusted ITT analysis or unadjusted ITT analysis.
- cinacalcet
- cost-effectiveness
- haemodialysis
- secondary hyperparathyroidism
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A semi-Markov model was developed to estimate quality-adjusted life years and lifetime costs, comparison did between cinacalcet strategy and standard strategy in patients with moderate-to-severe secondary hyperparathyroidism undergoing dialysis.
The assessment based on the impact of cinacalcet on hard outcomes within the scope of Evaluation of Cinacalcet Therapy to Lower Cardiovascular Events trial rather than the surrogate markers.
The main limitation of this study is the heterogeneity of the patient population. Since the high adherence is difficult to achieve in the real world, the health benefits of drug therapy may be overestimated. The study only included direct medical costs, without considering indirect and direct non-medical costs, which may underestimate the total cost of patients.
Introduction
Chronic kidney disease (CKD) has become an important public health problem in China, there were 132.3 million cases of CKD in China in 2017.1 According to 2015 Annual Data Report of the China Kidney Disease Network, the number of patients with end-stage renal disease (ESRD) undergoing dialysis was estimated at approximately 608 000 in 2015, and the number was expected to reach more than 1 million by 2020.2 With the increasing trend of patients with ESRD, the demand for dialysis therapy becomes a heavy financial burden to healthcare payers. The number of haemodialysis (HD) and peritoneal dialysis patients comprised only 0.16% and 0.02% of insured patients in the China Health Insurance Research database, but they consumed 2.1% and 0.3% of the overall expenditures, respectively. The total medical expenditure for dialysis patients was 429 million Renminbi (RMB) in 2015, among which 76.6% was covered by basic health insurance.2
Secondary hyperparathyroidism (SHPT), characterised by persistently increased serum parathyroid hormone (PTH) concentration, is a common consequence of ESRD and associated with elevated mortality, cardiovascular (CV) morbidity and bone disease.3–5 The incidence of SHPT increased with the years of dialysis.6 The treatment of SHPT includes many drugs according to its complexity of pathogenesis. Active vitamin D and phosphate binder are the most widely used effective drugs for SHPT,7 but still many refractory patients could not be well controlled by these drugs, especially in those with severe disease. According to current guidelines, such as Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline and the Japan Dialysis Medical Association’s Guidelines, parathyroidectomy (PTx) is recommended as a treatment for SHPT when drug therapy is ineffective.8
Over the last decade, cinacalcet, a calcimimetic agent, has been added to conventional therapies for SHPT and becomes a promising treatment option for refractory patients with SHPT.9 10 Cost-effectiveness analyses of cinacalcet were published in the USA,11 12 Europe13–15 and Japan16 before the result of Evaluation of Cinacalcet Therapy to Lower Cardiovascular Events (EVOLVE) trial was announced. The conclusions of these reports were inconsistent which reflected heterogeneity of the modelling assumptions and costs across regions.
EVOLVE was a multicentre, double-blind, prospective, randomised, placebo-controlled trial, evaluating the effects of cinacalcet versus placebo, both in addition to conventional therapy, including vitamin D sterols, phosphate binders or both, on death or major CV events in patients with moderate-to-severe SHPT undergoing dialysis.17 Based on EVOLVE trial, Belozeroff et al reported that in the USA, cinacalcet does not represent cost-effective when applying a willingness-to-pay threshold of US$100 000 per QALY in the unadjusted intent-to-treat (ITT) analysis, while it could be cost-effective when using the covariate-adjusted ITT treatment effect, which represents the least biased estimate.18
Cinacalcet has been listed in China since 2015. As it was a successful breakthrough for the management of SHPT in patients with CKD on dialysis by simultaneous reduction in intact PTH (iPTH) and control of serum calcium and phosphorus levels, cinacalcet has been widely accepted in clinical practice and included in the National Medical Insurance Catalogue of China in 2018. In China’s first CKD–mineral and bone disorder (MBD) diagnostic and therapeutic guidelines that published in 2019, the recommended levels of cinacalcet and conventional therapy were same as to the treatment of SHPT. However, the cost-effectiveness evaluation of cinacalcet and conventional therapy in China has not been reported. The purpose of this paper is to make a pharmacoeconomic evaluation of cinacalcet specific to the Chinese healthcare setting using the data from EVOLVE trial.
Methods
Study design and model structure
In the modelling of SHPT, periods of stable chronic disease alternate with periods of adverse events in which additional medical treatment is required and hence the corresponding treatment costs are increased. To realistically represent such process by means of a continuous-time Markov model, we need to divide the stable chronic disease state into a set of embedded states. Semi-Markov models allow for a parsimonious representation of complex medical processes in these situations. Therefore, we constructed a semi-Markov model to estimate quality-adjusted life years (QALYs) and lifetime costs associated with cinacalcet plus conventional therapy (cinacalcet strategy) compared with conventional therapy (standard strategy) in moderate-to-severe SHPT undergoing dialysis. The semi-Markov model diagram is shown in figure 1.18 The modelled population was consistent with the EVOLVE trial inclusion criteria, that is, adult patients with ESRD maintained HD three times a week for more than 3 months, who had a PTH level of 300 pg/mL or more, serum calcium level of 8.4 mg/dL or more and calcium–phosphorus product level of 45 mg2/dL2 or more. Standard strategy included calcium, vitamin D sterols and phosphate binders.

Model structure. PTx costs and utility decrements are calculated outside the Markov by applying the expected costs, disutility and probability of PTx to the number of patients alive. In the base-case analysis, PTx is treated as an outcome only (as in the EVOLVE trial) and is modelled outside of the Markov. This follows the statistical analysis of the EVOLVE trial in which PTx was not treated as a censoring event. The costs and utility decrements associated with the PTx surgery are applied to the per-cycle cost and QALY calculations. *PTx was included in the model as an outcome that could be experienced in the event-free, non-fatal CV event and non-fatal fracture event health states. †Patients may progress to the death health state from any other health state. CV, cardiovascular; CVD, CV disease; EVOLVE, Evaluation of Cinacalcet Therapy to Lower Cardiovascular Events; PTx, parathyroidectomy; QALY, quality-adjusted life year.
The patients enter the model in the health state of event-free and transit to the following state: non-fatal CV event, including myocardial infarction, hospitalised unstable angina, heart failure or peripheral vascular event and non-fatal fracture. The postevent state refers to the state within 1 year after the event, so that the increased cost and sustained impact of the event can be considered. After the postevent state, patients return to the event-free state. In the postevent state, patients can be reversed to non-fatal CV event, non-fatal fracture, maintained in postevent state or PTx. Patients may transit to the health state of death from any other health state in the model. To be consistent with the EVOLVE trial, PTx was modelled as an outcome. The model assumed a lifetime horizon and used a 3-month cycle.
The effect of cinacalcet on patient-level outcomes was referred to the data from EVOLVE trial. The incremental cost-effectiveness ratio (ICER) was calculated using the following formula: ICER=(Costcinacalcet+std−Coststd)/(QALYcinacalcet+std−QALYstd), where std refers to standard strategy. An annual discount rate of 5% was applied to both costs and health benefits based on Chinese pharmacoeconomic guideline.19 All analyses were performed using TreeAge Pro 2011.
Patient and public involvement
No patient involved.
Clinical model inputs
The model clinical data were derived from the EVOLVE randomised controlled trial, which evaluated the effects of cinacalcet by including 3883 adults undergoing dialysis.17 The ITT analysis showed that cinacalcet did not significantly reduce the risk of death or major CV events although patients randomised to cinacalcet experienced numerically fewer composite events (relative hazard 0.93; 95% CI 0.85 to 1.02; p=0.11) due to the imbalance in the age distribution of EVOLVE trial. Analyses adjusted for baseline characteristics suggest that a relative hazard of 0.88 for the primary composite end point or a nominally statistically significant 12% risk reduction with cinacalcet than with placebo.17 Furthermore, the EVOLVE trial conducted prespecified companion analyses with lag censoring. This lag-censoring analysis used the full ITT cohort but censored the follow-up time at 6 months postdiscontinuation and was intended to take account of drug effects that may persist after discontinuation. The results showed that the effect of cinacalcet was consistent with ITT analysis, with a relative hazard risk of 0.85 for the primary composite end point (95% CI 0.76 to 0.95; p=0.003). The primary ITT analysis, as well as the prespecified covariate-adjusted and lag-censored analysis, is described in the EVOLVE primary manuscript.17 We analysed the cost-effectiveness of cinacalcet using the treatment effects of unadjusted and covariate-adjusted ITT and used lag-censoring treatment effects as a part of scenario analyses.
Transition probabilities
The rates of clinical events in standard strategy were estimated from EVOLVE trial, including all-cause death, non-fatal CV event, non-fatal fracture and PTx (table 1). The event of each type was calculated from the first occurrence of the event and censored at death or the end of follow-up in the trial for the ITT analysis, while it was censored at death or 6 months after discontinuation of the study drug for lag-censored analysis. The rate of subsequent events was estimated to be similar to that of initial events in patients with events of the same kind.18 Naturalistic rates of death in Chinese dialysis population with SHPT were collected from the literature,20 which was used as the mortality rate of postevents. Effect sizes were estimated from the EVOLVE data as measured by HR (table 1).
Event rates in standard strategy and treatment effect estimates of cinacalcet strategy
Utility inputs
Quality of life was incorporated into the model by using utility values. As literature on the utility of various events in patients with SHPT in China is lacking, we used the utility values from published literatures of Japanese.16 A number of meta-analysis of cinacalcet showed that the clinical efficacy of cinacalcet in the treatment of SHPT in HD patients was good, but it was prone to hypochondria, nausea, vomiting and other adverse reactions.17 We incorporated this effect into the model and reduced the utility value of cinacalcet strategy in the event-free state by 5% compared with the standard strategy.16 18 Two different effects, that is, acute effect and chronic effect of events should be considered.18 21 Acute effect refers to the disutility within 3 months after the event occurs, whereas chronic effect refers to the disutility in all subsequent months postevent. In the analysis of repeated events, there was no significant change in the effect of subsequent events, so the same effect estimates were used for the first event and the subsequent event. The utility inputs of the direct effects of cinacalcet and a series of clinical events are listed in table 2. A beta distribution was used to capture parameter uncertainty.
Utility and cost values
Cost inputs
This analysis was conducted from the perspective of Chinese healthcare system. It only includes patients’ direct medical costs, without considering indirect costs and direct non-medical costs. Drug prices were obtained from Zhejiang Pharmaceutical Equipment Purchasing Center. The cost of cinacalcet was calculated based on the dosage used by patients with iPTH levels above 500 pg/mL. The costs of standard strategy were calculated referred to the market share of various drugs in 2018. Drug cost was modelled using a gamma distribution constrained to be between the minimum dose and the maximum dose studied: 25–100 mg/day for cinacalcet, 0.5–7.5 g/day for calcium, 0.25–1.0 µg/day for calcitriol, 0.8–14.0 g/day for sevelamer and 0.25–4.5 g/day for lanthanum carbonate. The hospitalisation expenses and proportion of fracture events (mainly skull and facial fractures, femoral fractures, multisite fractures, etc) and CV events (mainly acute myocardial infarction, angina pectoris, heart failure, arrhythmia, etc) were obtained by inquiring China Health Statistics Yearbook in 2018. Due to the lack of national statistics, the costs of PTx were estimated as the average costs of ‘bilateral PTx+forearm transplantation’, which was derived from our hospital in the first half of 2019. To avoid repeated computation, the costs of fracture events and CV events are calculated separately in the model for the specified events and are associated with hospitalisation after the events occur. Postevent costs capture costs associated with outpatient and follow-up treatment after hospital discharge, which were estimated for 9 months after the acute event. According to China’s national conditions, after discharging from hospital, less nursing costs will be incurred,22 and the proportion of fracture patients undergoing rehabilitation treatment after discharging from hospital is low.23 Therefore, these two items are not included in our cost estimates for postevent. A gamma distribution was used for hospitalisation, outpatient and follow-up treatment costs with the SD set to equal the mean. All costs were calculated in RMB and converted into US$ using the average exchange rate in 2018 (US$1=¥6.61) according to statistical bulletin of the People’s Republic of China on national economic and social development in 2018 (table 2).
Sensitivity analyses
We conduct a one-way sensitivity analysis to evaluate whether the fluctuation of input parameters of the model has an impact on the results of the base-case analysis. Among them, each parameter has a reasonable upper and lower bounds, for example, 20% price fluctuation of cinacalcet and 95% confidence limit of the estimated parameter. A probabilistic sensitivity analysis was performed using Monte-Carlo simulations to further explore the uncertainty of parameters. We constructed a cost-effectiveness acceptability curve assuming willingness-to-pay thresholds of US$26 508 per additional QALY, which was three times China’s Gross Domestic Product (GDP) in 2018.24
Results
Base-case analysis
Table 3 lists the base-case results for incremental cost-effectiveness of cinacalcet strategy, including unadjusted ITT analysis and covariate-adjusted ITT analysis. In each treatment outcome assessment, cinacalcet strategy resulted in a slight increase in quality-adjusted life expectancy (0.1 QALYs and 0.2 QALYs), and corresponding increase in costs of US$8721 and US$8008, resulting in ICER of US$87 210 per QALY and US$44 400 per QALY, respectively.
Cost-effectiveness results for ITT analyses and scenario analyses
Scenario analysis
We conducted a series of scenario analysis using the effect estimates of covariate-adjusted ITT analysis (table 3). As the choice of PTx will be affected by the tolerance to symptoms in patients with severe SHPT, more patients may choose PTx directly instead of receiving medication. We therefore performed a scenario analysis in which the annual event rate of patients undergoing PTx increased from 0.05 to 0.075 or 0.1 in standard strategy. The results showed that the ICER decreased to US$28 546 per QALY and US$26 750 per QALY, respectively, with the increase of PTx population. The inclusion of dialysis costs in the analysis substantially increased the ICER to US$49 815. With the estimates of therapeutic effects of lag-censoring analysis, the ICER reduced to US$30 123 per QALY.
Sensitivity analysis
The results of one-way sensitivity analysis are presented as Tornado Map (figure 2), which showed that, among the parameters, the two most influential variables on ICER were the survival rate estimates of cinacalcet and event-free-related utility of standard strategy, while the least influential variable was the postfracture-related cost of cinacalcet and standard strategy. One-way sensitivity analysis was conducted for the two most influential variables separately. When death rate of cinacalcet strategy was lower than 0.97 (value ranges from 0.78 to 0.97), cinacalcet strategy was the dominated regimen; when the utility of standard strategy was higher than 0.74 (value ranges from 0.54 to 0.82) in the event-free state, standard strategy became the dominated regimen. Therefore, it can be concluded that the changes of the two variables have no significant impact on the evaluation results.
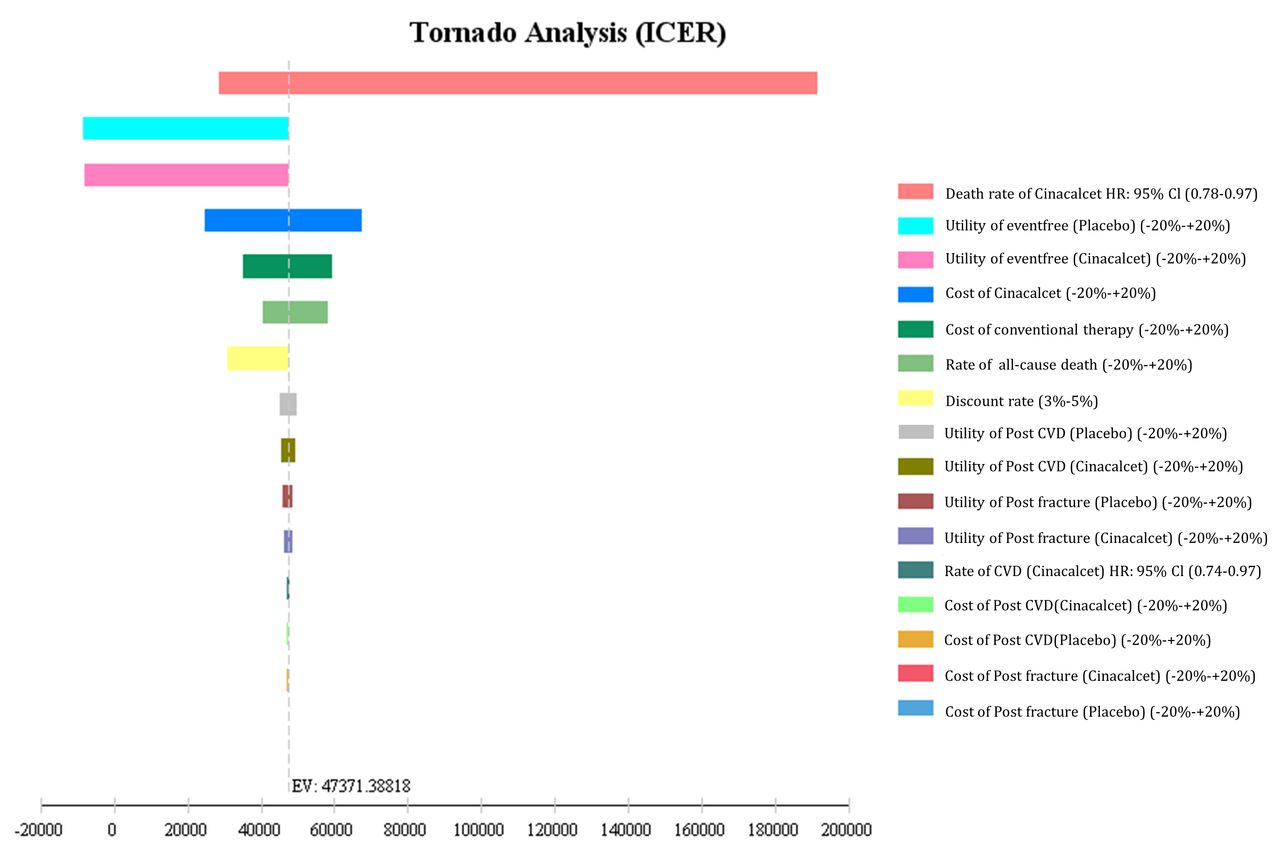
One-way deterministic sensitivity analyses for variables in the model. The vertical line indicates the expected value (in 2018 Renminbi converted into US$). Numbers in the parentheses indicate the range of values used for each variable. CVD, cardiovascular disease; ICER, incremental cost-effectiveness ratio.
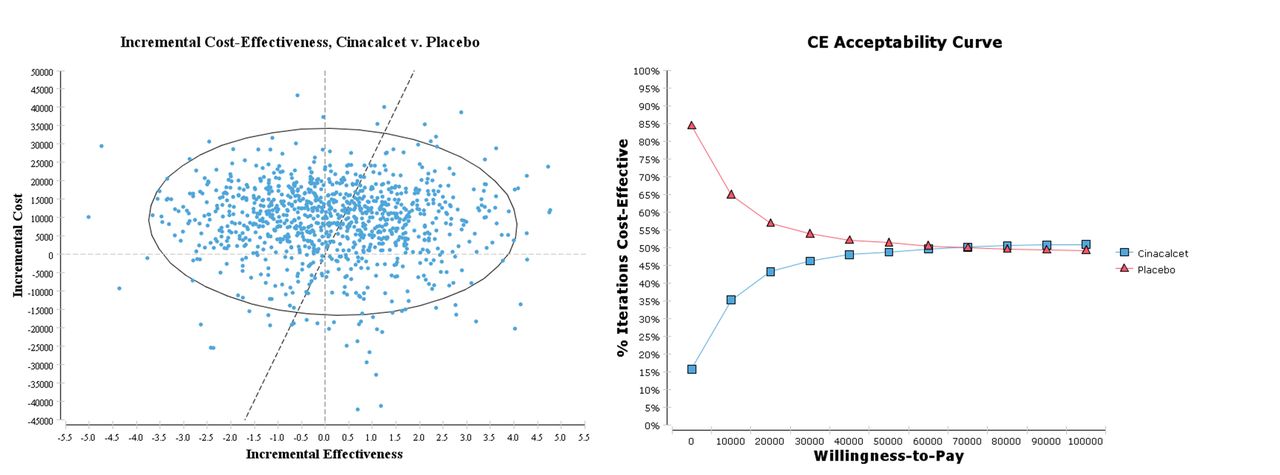
Probabilistic sensitivity analyses are presented as cost-effectiveness acceptability curves (figure 3). When the willingness-to-pay threshold is less than US$26 508, which was three times China’s GDP in 2018, the probability of cost-effectiveness of standard strategy (53.8%) is greater than that of cinacalcet strategy (46.2%). This means cinacalcet is not cost-effective at the current willingness-to-pay threshold. With the willingness to pay threshold increasing, the probability of cost-effectiveness of cinacalcet strategy increases gradually, while that of standard strategy decreases gradually. The same results are seen in the incremental cost-effectiveness scatter plot (figure 3). The scatter point at the lower right of willingness-to-pay slant indicated cinacalcet strategy represented a cost-effective use of healthcare resources when applying a willingness-to-pay threshold of US$26 508 per QALY.

{kind=link}
{kind=link}
{kind=link}
Incremental cost-effectiveness scatterplots (left panels) and cost-effectiveness (CE) acceptability curves reporting the probability of being cost-effective for willingness-to-pay threshold (right panels).
Discussion
By using covariate-adjusted ITT analysis and unadjusted ITT analysis, the current research found that the ICERs of cinacalcet strategy versus standard strategy were US$44 400 per QALY and US$87 210 per QALY, respectively. This is consistent with the research from Belozeroff et al on the pharmacoeconomic evaluation of cinacalcet based on EVOLVE trial.18 However, the results suggested that cinacalcet strategy has no cost-effectiveness under current Chinese willingness-to-pay threshold.
In previous pharmacoeconomic evaluation,11–16 the efficacy of cinacalcet in SHPT was usually evaluated via biomarkers with the hypothesis that reduction of serum calcium, phosphorus and PTH levels by cinacalcet would result in the improvement of clinical outcomes. However, the change of the surrogate marker could not always be translated into favourable effects on outcome. This divergence can be addressed only through the relevant evaluation of hard outcomes from randomised clinical trials. The completion of EVOLVE trial provided a reference for resolving the inconsistent result of above pharmacoeconomic evaluation on cinacalcet; furthermore, it made possible the estimation of the effect of cinacalcet on hard outcomes directly within the scope of the trial. Therefore, the advantage of our analysis is that it directly evaluates the effect of cinacalcet treatment on clinical outcomes based on a randomised controlled trial.
The results of one-way sensitivity analysis ranked all variables in the form of Tornado Map, in which the pharmacoeconomic model was most sensitive to survival rate. This effect was further evidenced by the ICER of approximately US$30 123 per QALY and US$87 210 per QALY associated with assumptions of the lag-censoring effect estimates (20% improvement in mortality) and the unadjusted ITT effect estimate (6% improvement in mortality). However, one-way sensitivity analysis only considers the impact of one variable on the results without the confounding factors and the relationship between variables. For example, in the lag-censoring analysis, the report of cinacalcet is overestimated, while in the real world, the report of cinacalcet and other oral drugs is known to decrease with time.25 To fully understand the impact of various factors on results and eliminate the confounding factors, we further carried out probability sensitivity analysis to help decision-makers make decisions on the optimal scheme for unit health output in the context of willingness-to-pay. The results showed that with the increase of willingness-to-pay threshold, the possibility of achieving treatment expectations was increased in cinacalcet strategy group but decreased in the standard strategy group. When the cost is within the scope of the current willingness-to-pay, standard strategy is recommended as the preferred treatment from the cost-effectiveness perspective, which verifies the stability of the roll back results.
Consistent with the EVOLVE trial design, we modelled PTx as an outcome, rather than as a treatment control. For patients with moderate to severe SHPT, either PTx or medical treatment can be an acceptable treatment. Previous studies have highlighted the potential cost-effectiveness of PTx compared with drug therapy,26 and PTx is also recommended as the first choice for the treatment of refractory SHPT in China. In EVOLVE trial, severe persistent SHPT still frequently occurred despite of drug treatment, so we assumed that more people may need PTx in clinical settings due to unsatisfactory drug control or intolerance to symptoms such as ostealgia, bone malformation, myatrophy and so on. In covariate-adjusted ITT analysis, we hypothesised that patients receiving PTx in the conventional treatment group increased to 7.5% and 10% and found the result that ICER decreased to US$28 546 per QALY and US$26 750 per QALY, respectively, which was partly benefitted from PTx and has better cost-effectiveness.
We analysed the cost-effectiveness from the perspective of Chinese healthcare system. Although EuroQol five-dimensional questionnaire (EQ-5D) data had been collected in EVOLVE trial to evaluate the utility of health status,21 there are cultural differences in the quality of life of EQ-5D between the eastern and western countries. Since there is still a lack of literature on the utility of various events in patients with SHPT in China, we used the utility values of similar events in Japanese patients with SHPT,16 which are relatively close to us in this study among the published literature. It must be acknowledged that the cost of treatment for CV events or fractures may vary greatly in different regions of China. Conservatively, the cost of model simulation was mainly based on China Health Statistics Yearbook in 2018. The cost of therapeutic drugs referred to Zhejiang Pharmaceutical Equipment Purchasing Center, which could be largely represent the price of specific drugs across the country with little difference. It is noteworthy that whether dialysis costs should be included in the total cost is still controversial. The social view is that all costs and benefits, whoever generates them, should be included in the analysis.27 However, we did not include the cost of dialysis in the direct medical cost of SHPT treatment, because dialysis is the main treatment for patients with ESRD but not for SHPT. Dialysis is a treatment with high cost that the annual medical cost of HD in China is about US$16 100 per capita. With the extension of dialysis treatment, additional life costs will be added. As a result, cost-effectiveness analysis incorporating these costs may lead to rejection of relatively inexpensive interventions that could improve survival. This viewpoint is also accepted by other cost-effectiveness analysis of dialysis population.16 18
The cost-effectiveness analysis showed that the risk of all-cause mortality, PTx, CV events or fracture in cinacalcet strategy group was lower than that in the standard strategy group, but its cost-effectiveness was not superior under the current willingness-to-pay threshold. In our opinion, we cannot simply assume that this is a negative result. The benefits (including all-cause deaths, CV events and fractures) of cinacalcet are not dose dependent, and even at low doses, these benefits are still significant.17 Clinicians may be more accustomed to considering the use of cinacalcet when the condition develops to an irreversible state. However, there are quite a few opinions that the clinical benefit of patients with CKD–MBD is expected to be maximised by the use of cinacalcet in the early stages of development of CKD–MBD.28 Whether the early use of cinacalcet is cost-effectiveness still needs further verification. Based on the existing results, it is suggested that cinacalcet may be more optimal if used in patients who meet one of the following conditions: (1) patients unable to perform PTx due to medical or personal reasons, (2) patients with high risk factors of CV or fracture events and (3) patients with low symptoms who can accept high long-term medication costs.
The main limitation of this study is the heterogeneity of the patient population. Because of lack of domestic clinical studies, we used data from EVOLVE trial, which was performed in the USA, and it may have some influence on the outcome, but the sensitivity analysis verifies the stability of the outcome to a certain extent. Our study did not explicitly establish a model of adverse events, because cinacalcet-related adverse events (mainly nausea and vomiting) were considered relatively slight and inexpensive in treatment. Their impact on patients was implicitly included in utility analysis (5% reduction in event-free status). Since cinacalcet has a positive, although small, overall beneficial effect on health-related quality of life, we believe that the relief of symptoms caused by cinacalcet may outweigh or at least balance any potential short-term impact of adverse events.29 The study only included direct medical costs, without considering indirect and direct non-medical costs, which may underestimate the total cost of patients. Our simplified disease progression model may limit the accuracy of the overall model because chronic diseases are complex and affected by many environmental, biological and physiological factors. In the real world, the medication report of patients cannot reach 100%. Therefore, the effect of cinacalcet on CV events risk might be even smaller than reported in the EVOLVE trial, meaning that the QALYs gained by taking cinacalcet may be overestimated. Similarly, for patients treated with standard strategy, the control of SHTP is often worse than that in the EVOLVE trial.
In conclusion, the choice of therapeutic outcome estimates in the model has a significant impact on the cost-effectiveness evaluation of cinacalcet strategy. However, whether it is using the treatment effect from unadjusted ITT analysis or covariate-adjusted ITT analysis, cinacalcet strategy has no cost-effectiveness when applying a willingness-to-pay threshold of US$26 508 per QALY.
Acknowledgments
This article was supported by Zhejiang Medical and Health Science and Technology Project (grant number 2018RC031).
References
Footnotes
Contributors LL designed the model, performed analysis and wrote the first draft of the manuscript. DH and KM supervised the process and provided input into data analysis and interpretation of results. BW and XL provided critical comments on model structure and data analysis. All authors contributed to the critical revision of the manuscript and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article.