Article Text

Abstract
Objectives Central nervous system depressants (CNSDs) such as opioids, benzodiazepine and Z-hypnotics are commonly used. However, CNSDs may influence cognitive function, especially in older hospitalised patients with comorbidities. The aim was to examine the association between CNSD use and cognitive function in older patients. We assessed global and domain specific cognitive function, among hospitalised older patients, including covariates for comorbidity, anxiety and depression.
Design Cross-sectional hospital-based study.
Settings Data was collected consecutively from inpatients at somatic wards of a general university hospital.
Participants Older patients between 65 and 90 years with/without CNSD use for ≥4 weeks.
Outcome measures The main outcome was cognitive function assessed by Cognistat. Secondary outcomes were routine clinical tests in the wards (mini-mental state examination (MMSE), trail making test (TMT) A and B, and clock drawing tests). Analyses were bivariate and multiple linear regression, adjusted for age, gender, and education. Covariates were comorbidity, depression and anxiety scores.
Results The main result indicated that CNSD users (n=100) had (β=–3.4, 95% CI 6.27 to –0.58, p=0.017) lower Cognistat score than non-users (n=146), adjusted for age, gender, education, anxiety and depression, but not significant when including covariate for comorbidity (β= –2.50 - 5.45; –0.46, p=0.097). Comorbidity was associated with cognitive function (β=−0.77, 95% CI −1.22 to −0.14, p=0.014). Cognistat subdimensions associated with CNSD use were language (p=0.017) and calculation (p=0.003). In clock drawing test, users had lower scores than non-users (β=−0.80, 95% CI 1.24 to −0.36, p=0.004), but no significant difference was found with MMSE and TMT A or B. Z-hypnotics were associated with reduced cognitive function.
Conclusion Among older hospitalised patients, global cognition and specific cognitive functions were associated with long-term use of CNSD medication as well as with somatic comorbidity.
Trial registration number NCT03162081, 22 May 2017.
- geriatric medicine
- old age psychiatry
- clinical pharmacology
- substance misuse
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a cross-sectional study that examines the combined effect of central nervous system depressant drugs among a large group of older hospitalised patients based on comprehensive data on medication use.
Comorbidities and affective symptoms are measured and included as covariates in the analyses as they may also influence cognitive function.
Due to the cross-sectional design, this study can only show adjusted associations and not directions of causality.
The patients in the study are from a general university hospital of somatic inpatient units and not general population.
This study suggests the importance of further prospective, longitudinal research on possible cognitive medication side effects in older patients.
Introduction
Older patients have high levels of comorbidity and are consequently among the most frequent users of pharmacological treatment.1 Typical symptomatic complaints from older patients can be moderate to severe pain, anxiety, depression or insomnia. These symptoms are often managed by short-term use of opioids, benzodiazepines (BZD) and hypnotics such as Z-hypnotics (Zopiclone and Zolpidem).2 These medications, which generally have an inhibitory effect on the central nervous system, may collectively be described as central nervous system depressants (CNSDs).
CNSDs are common and a high prevalence of opiate use among older patients has been much discussed internationally.3–5 An American prescription database study showed high BZD use among patients above 65 years of age compared with younger patients.6 Increased BZD and Z-hypnotics medication use with increasing age has been described also in Europe7 8 and the combined use of BZD and opioids is often reported among older patients.9 The high age-related consumption of medication is associated with side effects and risk of abuse of prescribed medications.10 We have recently described the addictive properties and sociodemographic factors associated with use of CNSDs among older patients.11 12 The widespread use of CNSDs is well documented among older patients; polypharmacy further complicates the issue.1 The cognitive effects of CNSDs in general have been less investigated, especially among patients hospitalised for somatic reasons.
The high and increasing consumption of CNSDs represents a considerable risk factor for adverse effects and interaction with other medications. Use beyond 4 weeks is not recommended and can be defined as long-term use based on guidelines for CNSDs. In addition, old age can impact the pharmacodynamics and pharmacokinetics of the drugs and increase the likelihood of adverse effects. Studies report increased falls, toxicity, drug interaction and dependence among BZD and Z-hypnotics users.8 13 14 Opioid users may have opioid-induced hyperalgesia, gastrointestinal, urological issues and addiction-related problems.15 16 Less is known about how long-term CNSD medication use influences cognitive function in older hospitalised patients, and current research is inconsistent. Several studies have suggested that prolonged opioid, BZD and Z-hypnotics consumption among older patients can lead to global cognitive decline.13 17–21 Other studies propose that prolonged CNSD users have domain specific cognitive impairment in working memory, attention and executive function.18 22 23 In addition, increased risk of dementia in long-term users has been proposed.24 25 Other studies found no association between CNSD use and cognitive decline.26–29
Existing studies generally do not differentiate between BZD and Z-hypnotics when examining cognitive function and BZD is over-represented in the studies. Older patients often use combined CNSDs; so their combined effect on cognitive function among older inpatients should be addressed. Our intention is thus to focus on the role of the whole group of the most commonly used CNSDs that also have addictive potential, in potentially influencing the cognitive function of older patients admitted to somatic inpatient departments.
The main aim of this cross-sectional study was to examine the association between the use of CNSD medications and both global and domain-specific cognitive function, in hospitalised older patients, with comorbidity, anxiety and depression as covariates. A secondary aim was to assess whether results of routine clinical cognitive tests used in our hospital wards are associated with CNSD use. Our primary hypothesis was that CNSD medication use among older patients is associated with reduced global and dimension-specific cognitive function.
Method
Design and settings
We performed a cross-sectional study in the somatic wards of a general university hospital. Older patients were included consecutively, at the first or second day of their stay at Akershus University Hospital (Lørenskog, Norway), from the Neurology, General Internal Medicine, and Geriatric departments between May 2017 and August 2018. Data were collected through interviews, tests, questionnaires and electronic patient record (EPR).
Participants
The flow chart of participants in the study is shown in figure 1. Inclusion criteria were: inpatients from the somatic general university hospital departments between the age of 65 and 90 years. Exclusion criteria were: psychosis, moderate-to-severe depressive disorder, brain tumour, traumatic brain injury, stroke and unable to participate due to medical condition. Patients with active delirium during the hospital stay were excluded as they were unable to complete cognitive examination. Patients fulfilling Diagnostic and Statistical Manual of Mental Disorders, fourth edition, (DSM-IV) criteria for dementia,30 and DSM-V criteria for major neurocognitive disorder,31 were excluded. Patients with moderate-to-severe depressive episodes were excluded according to the International Statistical Classification of Diseases and Related Health Problems, 10th Revision.32 We also excluded patients with an mini-mental state examination (MMSE) score lower than 21 to avoid the inclusion of patients with reduced consent ability.33

Study participation flow chart at baseline. Footnote: the neurobehavioral cognitive status examination (Cognistat). MMSE, mini-mental state examination.
Data collection
History of CNSDs use was collected from participants, the general practitioners (GPs) medication lists and the EPR. Supplementary information on medication type/name was provided by close relatives, required only in few cases (≤5). CNSD medication use was defined as using opioid, BZD, Z-hypnotics or a combination of them, regularly ≥4 weeks prior to hospital admission. Non-use was defined as no CNSD use or sporadic use below the aforementioned threshold. We collected sociodemographic data as well as reason for admission, clinical diagnoses and comorbidities. All clinical data and measurements were collected at baseline, and done by the first, second and occasionally last author, except routinely collected MMSE, clock and trail making test (TMT) A and B, which were at times conducted by a trained occupational therapist in the wards, who also trained the collecting authors on using the routine cognitive tests.
Measurements
Cognitive outcome measures
The neurobehavioral cognitive status examination
The neurobehavioral cognitive status examination (Cognistat),34 was conducted to examine global and domain-specific cognitive function in users and non-users. We used the Norwegian paper version from 2015 (translated and revised by Arne Rønningen/Gørel Swedhner). The standardised manual with instructions on how to conduct and interpret the test was used. Cognistat takes approximately between 15 and 20 min to perform and addresses general domains (consciousness, orientation and attention) and major domains (language comprehension, memory, construction and reasoning). Moreover, Cognistat uses a screening and metric approach that allows unimpaired individuals to complete the examination in a shorter time.35 Cognistat can be used to examine cognitive profiles in different populations of patients, including dementia, mild cognitive impairment, psychiatric illness and substance abuse.35 On the other hand, Cognistat can be influenced by age, gender and education level, which should be taken into consideration during assessment and adjusted for in analyses.36 The total Cognistat score and scores for each Cognistat domain were calculated.36
Mini-mental state examination
The patients were also assessed by clinical tests in routine use at the hospital. The Norwegian version of MMSE is a screening tool for cognitive impairment,37 which gives an overall score of 30 points, with <25 indicating cognitive impairment. It takes approximately 10 to 15 min to complete. The standardised manual for MMSE was used to conduct and interpret the test in the current study. MMSE is easy to use, frequently used in hospitals and is suitable for detection of general cognitive impairment in older patients.38
Clock drawing test
The Norwegian version of clock drawing test was used, This measures executive function, construction, visual-spatial skills and gives a score from 4 to 5 (normal) and <3 (impaired). The standardised manual was used to conduct and interpret the test. Clock drawing test is often used together with MMSE.39
Trail making test A and B
TMT A and B measure information processing speed and attention, with results given as time (s) for completion of the test, higher score indicates slower processing speed when completing the test.40 The test was administered in the patients hospital room, instructions were given according to the standardised manual for TMT A and B.40
Other measures
Cumulative illness rating score geriatrics
The cumulative illness rating score geriatrics (CIRS-G) total score was used to assess comorbidity among patients. The scale was used to assess biopsychosocial factors of disease, scoring from no problem (score 0) to extreme problems (score 4); a higher score indicates higher burden of disease in major organ systems—neurological, psychiatric, metabolic and musculoskeletal systems.41 The assessment was done by using EPR, looking for previous and current diagnoses by researcher SC.
The hospital anxiety and depression scale
The Norwegian version of the hospital anxiety and depression scale (HADS) is a 14-item scale. Each item is scored 0 to 3, giving a sum between 0 and 21, with higher score indicating that the symptoms are more severe. Half of the items represent an anxiety scale (HADS-A, items 1, 3, 5, 7, 9, 11 and 13) and the other half a depression scale (HADS-D, items 2, 4, 6, 8, 10, 12 and 14). The score may be used as a total score (all items), as well as separate anxiety and depression scores.42 We used all the three scores in our analyses. In the hospitalised older patients, the internal consistency reliability assessed by Cronbach's alpha was 0.82 for the entire scale. Cronbach's alpha for subscales were: HADS-A 0.78 and HADS-D 0.7142
The alcohol use and disorder identification test
The alcohol use and disorder identification test (AUDIT) is a screening tool used to examine excessive drinking and alcohol use disorder. The AUDIT has a 10-item list giving a total score of 40, with score above 8 indicating problematic use. We used the Norwegian version of AUDIT.43 The internal consistency of AUDIT is reported to be high. In a review, Cronbach's alpha ranged from 0.94 to 0.81 across various population groups.44
Ethics
Participation was by informed signed consent. We chose to exclude patients with MMSE score <21 due to possibility for reduced consent ability. The data was stored in anonymised form on a secure hospital server.
Statistical analyses
IBM SPSS statistics software (IBM Corp, released 2015, IBM SPSS Statistics for Windows, V.23.0. Armonk, New York, USA) was used for the analyses. The distribution of continuous variables was assessed by graphically inspecting the histograms (Cognistat, MMSE, clock, TMT A and B, education, age, HADS, CIRS-G and AUDIT). Categorical variables (gender and smoking) were described by frequencies and percentages, whereas continuous variables were described by means (M), median, range or SD. CNSDs users and non-users were compared by independent samples t-test or χ2 test.
The main outcome was cognitive function defined as the mean score of multidimensional Cognistat test. Secondary outcomes were mean scores of the routine tests—MMSE, clock and TMT A and B.
Bivariate linear regression models were estimated to assess the relationship between the main and secondary outcomes, and CNSD use versus non-use. Two multiple linear regression models were estimated for each outcome. Both models were adjusted for the variables gender, age at baseline and education, and included the main covariates: HADS and CIRS-G total score. Model 1 contained CNSD use versus non-use, age, education and HADS total score. As the construct of HADS and CIRS-G partially overlap, they were not included in the same model. Thus, in model 2, HADS total score was replaced by CIRS-G. For the main and secondary outcome analyses, we used a p value cut-off at p≤0.05. Assumptions of linear regression models were assessed by using standard tests. An interaction model was performed between medication use and CIRS-G below (5.5) and above (5.6) median for Cognistat.
We performed two explorative post hoc tests to examine associations between CNSD use versus non-use, and subdomains of Cognistat. The same bivariate and multiple linear regressions were used as main outcome models and a p value cut-off at p≤0.05. Finally, an additional explorative post hoc analysis was performed to examine the differences in Cognistat by medication groups. The results are presented in a bivariate analysis, not adjusted for confounder due to small sample size among some of the medication groups. We used a p value cut-off at p≤0.01 to avoid multiple comparison issues. All missing data are given in the table footnotes.
Patient and public involvement
A user advisory board established at the Akershus University Hospital, Health Services Research Unit, which includes both representatives of patients and health service officials, supported this study. The board met on a regular basis throughout the study period. They provided feedbacks on the current project regarding the ethics, design and methodology.
Results
Participants
A total of 246 patients were included in the study; 100 patients were CNSD users, and among these, 42% used solely Z-hypnotics, 21% used opioids and 7% used BZD alone. Thirty per cent used more than one medication group (mostly opioids and Z-hypnotics). Most were long-term users of their CNSD medications, with overall median duration of use of 52 weeks (min: 4, max: 988). Individually, opioids were used for a median of 42 (range: 4 to 988) weeks, BZD for 51 (range: 4 to 208) weeks and Z-hypnotics for 52 (range: 4 to 232) weeks; there was no significant difference regarding the length of use (p=0.393).
The demographic characteristics of the study sample are shown in table 1. CNSD users were significantly older (p<0.001) and had lower education (p=0.011) than non-users. Users had higher HADS depression (p<0.001) and HADS total scores (p=0.003). CNSDs users had higher levels of comorbidity measured by CIRS-G than non-users (p<0.001). The distribution of users and non-users were different between the three departments (geriatric department 22% CNSD users (n=54) vs 16.7% non-users (n=41), neurology 14.6% users (n=36) vs 32.9% non-users (n=81) and general internal medicine 4.1% users (n=10) vs 9.8% non-users (n=24)). There was a significant difference between the departments (p<0.001). No significant differences between users and non-users regarding smoking or alcohol use were found. We also compared patients who completed and who did not complete the Cognistat test; there was no significant difference in age, gender, education, HADS and CIRS-G score between these two groups.
Baseline characteristics among CNSD users and non-users
Cognitive outcomes in CNSD users and non-users
As a descriptive comparison, we examined the patients who were precluded or said no to participation (n=369). Their mean age was 77.6 years (SD 7.4), there was no significant difference in age between participants and non-participants (p=0.097). More males (n=205) than females (n=164) said no to participation, with a significant difference in gender between participants and non-participants (p=0.003). The patients were admitted to Geriatrics (n=150), Neurology (n=166) and General Internal Medicine (n=53) departments. We found no significant difference between non-participants and participants (p=0.802) across the departments. This indicates similar pattern in age and department of admission between non-participating sample compared with the participating sample.
Main outcome
Cognistat scores
In the bivariate model, CNSD medication use was negatively associated with total Cognistat score (table 2); users had, on average, 5.0 units lower Cognistat score than non-users (p<0.001). In the multivariate model 1, where the main covariate was HADS, adjusting for confounders age, gender and education did not alter the association between medication use and Cognistat score. The users had, on average, 3.4 units lower Cognistat score than non-users (p=0.017). Age was the only significant adjusted variable in model 1 (p=0.011).
In the multivariate model 2, where the main covariate was CIRS-G, adjusted for confounder age, gender and education, the association between medication use and cognitive function was no longer significant (p=0.097). However, CIRS-G score was significantly associated with cognitive function (p=0.014). In stratified post hoc analyses; medication use was associated with worse cognitive function among those with CIRS scores (ie, comorbidities) above median (5.5). We found no evidence of significant interaction between CIRS-G score and medication use (p=0.063).
Cognistat subdomains
To examine the different subdomains of Cognistat and their effect on CNSD user versus non-users, an explorative post hoc analysis was conducted by performing bivariate and multiple linear regression modelling, using the same models as for the main outcome.
The bivariate model indicated significantly lower scores for CNSD users in the following dimensions; language (repetition) (β=−1.0, 95% CI −1.60 to −0.29, p=0.005), calculation (β=−0.7, 95% CI –1.07 to −0.28, p=0.001), construction (β=−0.7, 95% CI –1.35 to –0.14, p=0.016), memory (β=−1.1, 95% CI −2.02 to −0.11, p=0.029) and similarities (β=−0.6, 95% CI −1.09 to −0.05, p=0.032) (figure 2).

Cognitive subdomain in Cognistat. Footnote: mean scores (M) and SD among CNSD users and non-users. Bivariate linear regression, *p≤0.05, **p≤0.01 (missing Orientation=1, Comprehension=1, Construction=4,. Calculation=1, Similarities=1, Judgement=1). CNSD, central nervous system depressant.
In multivariate models, CNSD users had lower scores than non-users on the Cognistat subdomains; language (repetition), depending on adjustment for HADS (β=−0.9, 95% CI −1.60 to −0.16, p=0.015) or CIRS, (β=−0.8, 95% CI −1.56 to −0.03, p=0.042). CNSD users had lower scores in the calculation subdomain after adjusting for HADS (β=−0.6, 95% CI −1.07 to −0.22, p=0.003) but not for CIRS-G, (β=−0.3, 95% CI –0.85 to 0.06, p=0.085).
In addition, higher CIRS-G score were associated with significantly lower Cognistat subdomains; calculation (β=−0.1, 95% CI −0.20 to −0.03, p=0.008), construction (β=−0.1, 95% CI −0.30 to −0.002, p=0.047), similarities (β=−0.1, 95% CI −0.25 to −0.03, p=0.017) and judgement (β=−0.1, 95% CI −0.17 to −0.004, p=0.039) in the multivariate models. HADS was only negatively associated with the Cognistat subdomain comprehension (β=−0.02, 95% CI −0.03 to −0.01, p=0.005).
Secondary outcomes
Routine cognitive tests
Clock drawing test (table 2): In the bivariate model (mean and SD shown in table 1), medication status was negatively associated with total score; users had, on average, 0.8 units lower Clock score than non-users (p<0.001). The multivariate models indicated similar results, with age as the only other significant predictive variable in model 2 (p=0.014).
MMSE (table 2): In the bivariate model (mean and SD shown in table 1), medication use was negatively associated with MMSE score; users had on average 0.9 units lower MMSE score than non-users (p=0.015). However, after adjusting for age, gender, years of education and HADS total score (model 1) or comorbidities using CIRS-G (model 2), the association was no longer significant. Age was negatively associated with MMSE score in both multivariate models (p<0.001).
TMT A and B (table 2): No significant association between CNSD use and performance on TMT A or B tests was found in the bivariate model (table 1) or in the three multiple models (table 2). Age was associated with TMT B (model 2, p=0.035).Comorbidity (CIRS-G), was positively associated with TMT B (p=0.024).
Post hoc analyses of Cognistat and CNSD groups
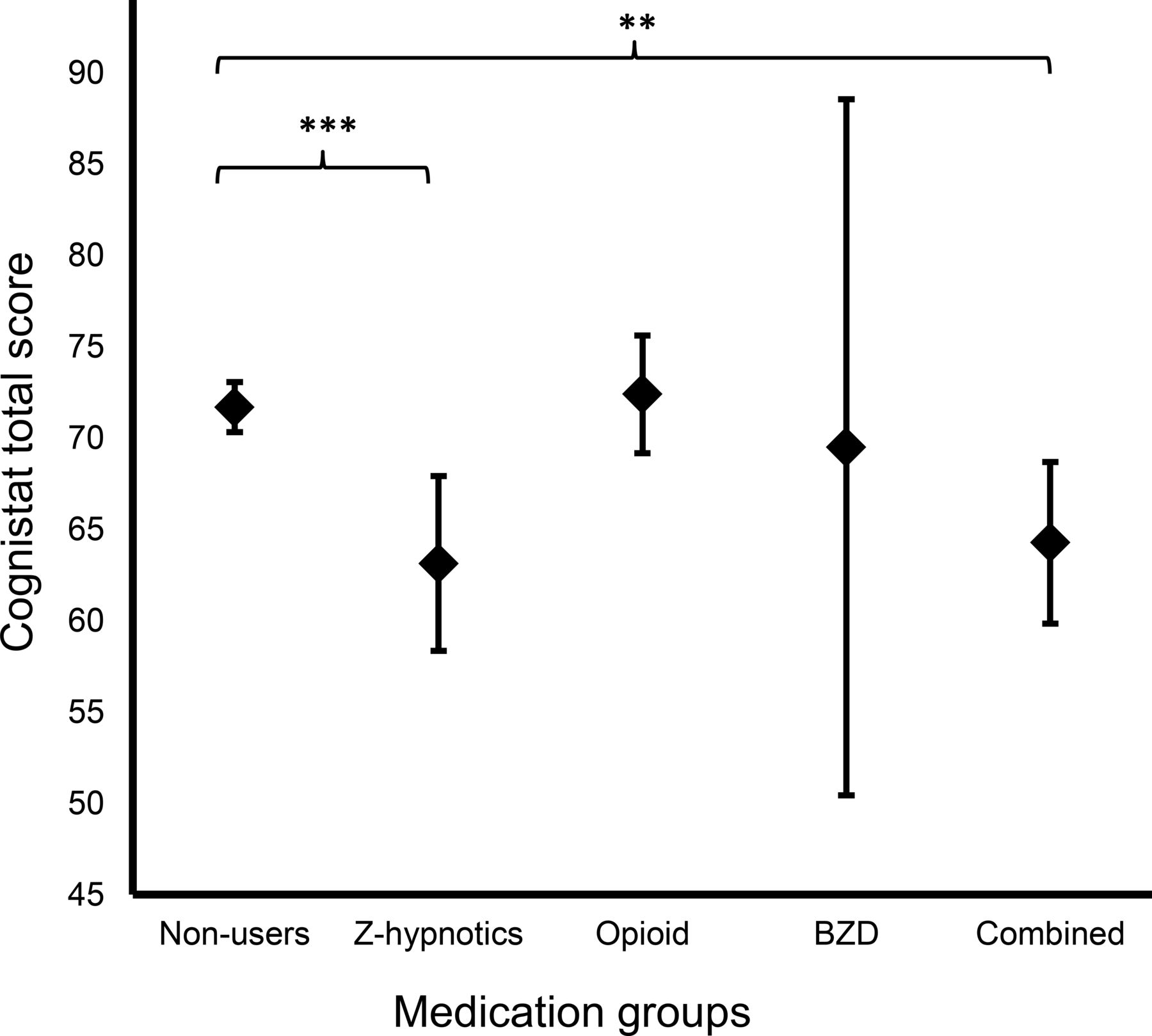
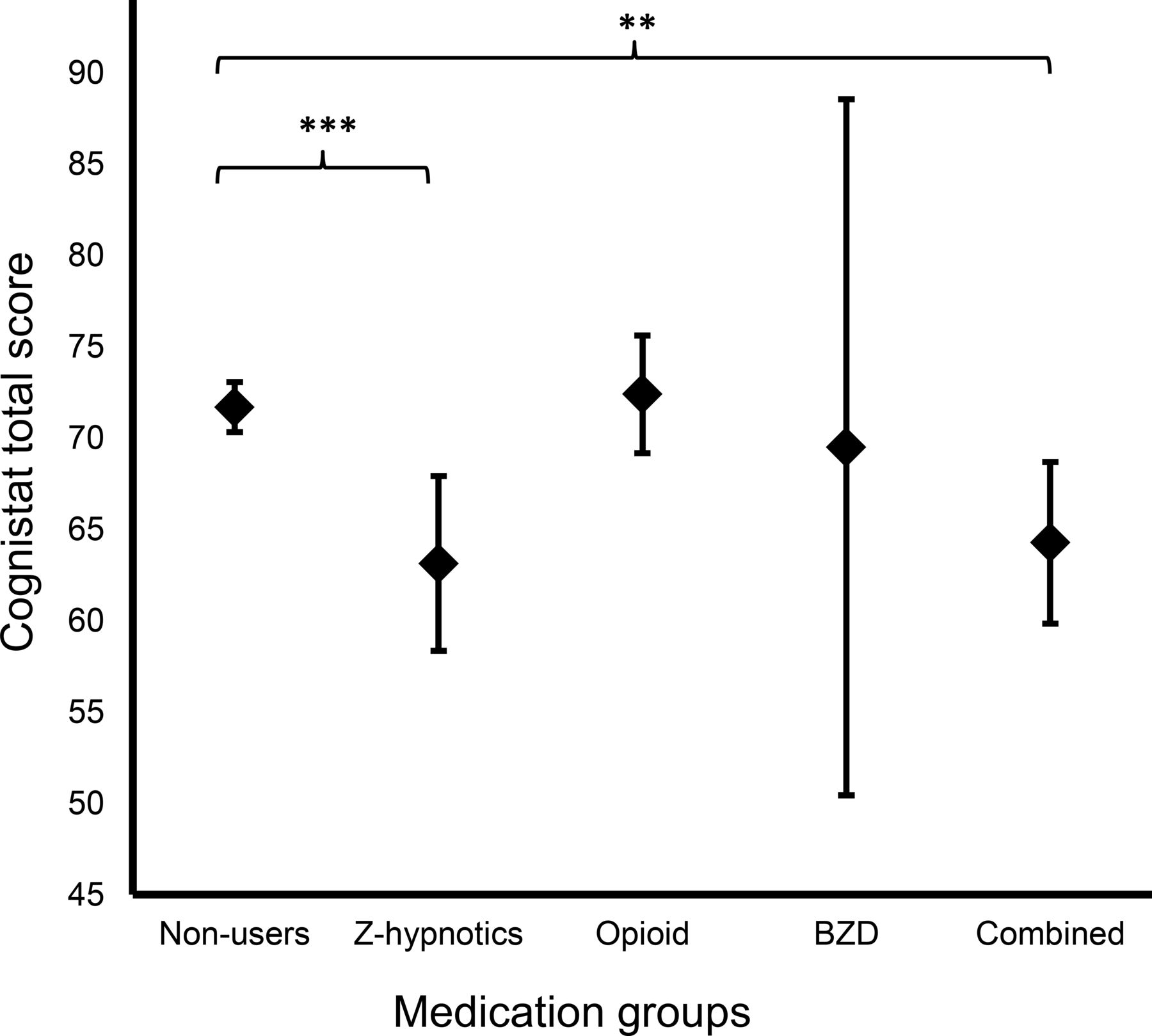
We further explored the association between separate medication groups and cognitive function in a bivariate model. We did not perform multivariate analyses due to low power and a small sample size in some of the medications groups. As shown in figure 3, patients using Z-hypnotics had lower Cognistat score than non-users (p<0.001), and combined users had lower Cognistat scores compared with non-users (p=0.005).
{kind=link}
{kind=link}
{kind=link}
Cognistat and CNSD medication use. Footnote: Cognistat (mean total score) and CNSDs group. bivariate linear regression ** p value≤0.01, ***p value<0.001. BZD, benzodizepine; CNSD, central nervous system depressant.
Discussion
This study examined the association between cognitive function and use of CNSD medication including opioids, BZD and Z-hypnotics in hospitalised older patients. The first finding was that cognitive function measured by Cognistat was lower among users of CNSD medication than non-users. Z-hypnotic users and multi-CNSD users had reduced cognitive function in bivariate models. Both calculation and language sub-dimensions of Cognistat were associated with CNSD use.
The second finding was that higher comorbidity scores measured by CIRS-G were associated with lower cognitive function among older patients. Subdimensions calculation, construction, similarities and judgement were associated with comorbidity. The significant association between CNSD use and cognitive function was removed after including comorbidity. Symptoms of anxiety and depression were not associated with cognitive function.
We also examined the interaction between cognitive function, CNSDs and comorbidity. CNSD use was associated with worse cognitive outcome in the group with high (above median) comorbidity. Finally, among routine clinical cognitive tests (MMSE, Clock drawing test and TMT A and B), only the clock test showed significant negative association with CNSD use also after including comorbidity, anxiety and depression covariates.
Our findings are partially consistent with findings of global cognitive impairment in users of CNSD medication.18 19 45 46 Others did not find a relationship between cognitive function in patients using BZD and Z-hypnotics.27 29 47 A possible explanation is that the above studies either used simple clinical tests such as MMSE or included short-term users or patients with dementia and psychotic disorders in the study. Our study used several different cognitive measures to get a more comprehensive picture of cognitive profile in long-term use (52 weeks) and excluded patients with psychosis, major depression and dementia. In addition, we found that comorbidities in older patients have an impact on their cognitive function. Others have also found a link between somatically ill patients and reduced cognitive function.48 Thus, both comorbidities and CNSD use influence cognitive function among hospitalised older patients. Higher comorbidities may lead to more use of medications or medication use might lead to higher comorbidity. This may impact the cognitive function by both CNSD use and comorbidities in older patients. However, as this is a cross-sectional study, the direction of the relationship cannot be determined.
We found impairment of domain-specific cognitive functions, such as executive function, visuospatial skills, calculation and language, to be associated with CNSD use. Other domains showed trends of lower performance on memory, construction and similarities task in users compared with non-users, although this did not reach the adjusted significance level. Compared with our research, others have suggested that older patients using CNSD medication have impairment in different cognitive domains such as memory17 18 and language comprehension.22 In contrast to our results, others have found impaired reaction time,49 attention and processing speed18 in patients using CNSD medications. One explanation for this discrepancy might be that the majority of patients in our study were using Z-hypnotics. Other studies have a majority of BZD users, in combination with Z-hypnotics, or opioids separately. Another explanation can be that our patients were frail elderly with comorbidity on long-term CNSD use, while others have generally examined short-term use among healthier older participants without comorbidity. However, more in-depth assessment and follow-up studies are needed to examine the specific functions involved in long-term CNSD medication use among older patients.
The majority of CNSD users were long-term users (median use of 52 weeks) in our sample. This is also described by others.8 50 Both long-term use of Z-hypnotics alone and in combination with opioids has been shown to be associated with cognitive decline in older patients.46 According to guidelines for appropriate prescription of medications for older patients, long-term combined use of CNSD medication is not recommended due to age-related changes and increased side effects in older patients.51 Despite these recommendations, inappropriate prescription is still prevalent as suggested by previous research.52 Our current results further highlight this.
Our study has some limitations. The direction of association is not possible to determine in a cross-sectional design. It can be argued that the medication use is driving the cognitive impairment, but it is also possible that cognitive impairment leads to CNSD medication overuse. The results should be interpreted with caution as the regression models are not corrected for multiple modelling. Moreover, some of the participants might still have been on antidepressants. However, we excluded patients with moderate-to-major depression, and the CIRS-G scale examines the antipsychotics use, including depression and anxiety severity. Moreover, we included patient with multiple illnesses and affective symptoms, while other patients with more specific illnesses might have a different cognitive profile. We have adjusted for effects of comorbidities in our analyses. Another limitation might be that our patients are representative for a hospitalised older population, and not for the general older population. However, population-based studies are consistent with our findings, suggesting poor cognitive function in users of CNSD medications in general population.21 25 Finally, variables included were mainly pre-decided based on previous publications on factors known to influence cognitive function. The limited sample size also precluded the inclusion of too many additional predictor variables.
On the other hand, the strength of our study is that the sample is representative for a large, pragmatic hospitalised geriatric population, with individual patient data on psychological, biological and social factors that can influence medication use. We collected medication use information from several sources (EPR, self-report, paper list of medications by GP and information from next of kin) to limit information bias. Future studies should conduct in-depth neuropsychological testing as well as prospective studies to further examine the specific effect of CNSD medication on cognitive domains. Such studies should also consider the effect of disease burden on cognition in older patients. Moreover, in order to address the issue of direction of causality, intervention studies are suggested to examine the effect on cognitive function of discontinuing these medications. This may be easier to achieve if at-risk patients are identified in hospital-derived samples.
Conclusion
Among hospitalised older patients, both comorbidities and CNSD use may affect cognitive function. Our results suggest that the nature of these associations is such that more domain specific instruments for assessment of cognitive function than those in routine clinical use may be required (with the possible exception of the clock test). In-depth neuropsychological testing may be useful to further describe medication-burden and disease-burden related cognitive impairment. A raised awareness of possible cognitive side effects of CNSD medications in older patients with comorbidity is important when such medications are considered, among prescribing physicians and other healthcare workers as well as to inform patients and next of kin. When possible, other treatment options, including psychological treatment of insomnia, anxiety and chronic pain, should be considered.
Acknowledgments
We gratefully acknowledge statistical support of research professor Jūratė Šaltytė Benth. In addition, we appreciate the support during data collection from department secretaries, occupational therapists, physiotherapists, care assistants, nurses and doctors in Geriatric, General Neurology and Internal Medicine departments at Akershus University Hospital. We also recognise the extraordinary commitment of patients that participated in this study.
References
Footnotes
Contributors The authors TGS, CL, SC, MG, ESK and RG designed the study and wrote the protocol. TGS, SC and CL collected the data. TGS managed the literature searches and analyses. TGS, RG and CL undertook the statistical analysis, and TGS wrote the first draft of the manuscript. All authors contributed to and have approved the final manuscript.
Funding This work was supported by a grant from the Norwegian Research Council (256431) and the Health Services Research Unit of the Akershus University Hospital. CL also received funding from the South Eastern Norway Regional health authority. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests CL has participated on an advisory board and received payment for lectures arranged by AbbVie Pharma AS and Roche AS, Norway. He has also received research sponsorship from AbbVie Pharma. All other authors declare that they have no conflicts of interest.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval The data collection and storage were approved by the Akershus University Hospital data protection officer and the Regional Committees for Medical and Health Research Ethics (2016/2289). Written informed consent was obtained from patients for their anonymised information to be published as a research article.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data that supports the findings of this study are available upon reasonable request.