Article Text

Abstract
Objectives Continuous improvement in the delivery of health services is increasingly being demanded in the UK at a time when budgets are being cut. Simulation is one approach used for understanding and assessing the likely impact of changes to the delivery of health services. However, little is known about the usefulness of simulation for analysing the delivery of sexual health services (SHSs). We propose a simulation method to model and evaluate patient flows and resource use within an SHS to inform service redesign.
Methods We developed a discrete event simulation (DES) model to identify the bottlenecks within the Unity SHS (Bristol, UK) and find possible routes for service improvement. Using the example of the introduction of an online service for sexually transmitted infection (STI) and HIV self-sampling for asymptomatic patients, the impact on patient waiting times was examined as the main outcome measure. The model included data such as patient arrival time, staff availability and duration of consultation, examination and treatment. We performed several sensitivity analyses to assess uncertainty in the model parameters.
Results We identified some bottlenecks under the current system, particularly in the consultation and treatment queues for male and female walk-in patients. Introducing the provision of STI and HIV self-sampling alongside existing services decreased the average waiting time (88 vs 128 min) for all patients and reduced the cost of staff time for managing each patient (£72.64 vs £88.74) compared with the current system without online-based self-sampling.
Conclusions The provision of online-based STI and HIV self-sampling for asymptomatic patients could be beneficial in reducing patient waiting times and the model highlights the complexities of using this to cut costs. Attributing recognition for any improvement requires care, but DES modelling can provide valuable insights into the design of SHSs ensuing in quantifiable improvements. Extension of this method with the collection of additional data and the construction of more informed models seems worthwhile.
- organisation of health services
- sexual dysfunction
- HIV & AIDS
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We used 12 months’ data from the electronic patient record of the Unity sexual health clinic (SHC) to populate our model, and such a model has not been developed previously to assess the likely impact of changes to the delivery of sexual health services while containing costs.
The discrete event simulation model presented here could be reconfigured for a different geographical location and repopulated with the appropriate data to inform service improvement.
The care pathways were developed through discussions with staff at the Unity clinic and are based on the actual clinic workflow. However, in order to make the model manageable, we simplified the number of clinical care pathways and combined some.
We assumed that no men who have sex with men will use online-based self-sampling as this patient type usually prefers clinic-based face-to-face sampling by a healthcare practitioner, but this may not always be the case in clinical practice.
We did not include fixed overheads such as building and administration in our cost estimations as these overhead costs do not fluctuate with service activity. The cost of providing online self-sampling was based on actual practice undertaken at the Unity SHC.
Introduction
The number of sexually transmitted infections (STIs) continues to rise in the UK with a 5% increase since 2018.1 This has resulted in Public Health England (PHE) concluding in 2019 that local and national services for the prevention, diagnosis, treatment and care of STIs need to be delivered to the general population, as well as a focus on groups with greater sexual health needs.1 A new recommendation in 2019 is that individuals having condomless sex with new or casual partners should have an annual STI screen and HIV test.1 This new emphasis on the importance of providing sexual health services (SHSs) for the general population has come at a time when budgets for SHSs are being cut. SHSs in England are funded from the public health grant to local authorities, and between 2013/2014 and 2017/2018, this decreased by 8% in real terms from £2.7 billion to £2.4 billion with a further 2.6% cut in 2019/2020.2 SHSs have improved their productivity with a 13% increase in attendances between 2013 and 2017, but there is a limit to how much this can happen before quality will start to suffer.2
One option for improving access and potentially reducing costs is through the provision of online-based STI and HIV self-sampling for asymptomatic patients.3–6 Service users can order a test kit online, collect their own samples, return the samples and receive their test results. Patients who test positive for an STI or HIV would then be offered a clinic appointment. Online services for STI and HIV self-sampling at home may address barriers to clinic use such as inconvenient opening hours, long waiting times, perceived stigma and travel cost.3 7 8 Furthermore, online services are less expensive than a traditional clinic attendance, but patients do have concerns about privacy and ability to take the test accurately.3–5 A recent randomised controlled trial indicates that online-based self-sampling increased the uptake of STI testing for all groups, including high-risk groups.6 However, such a service would generate new demand, increasing the number of tests and total cost of testing, but it would reduce the cost per test4 and would help address the PHE recommendation of ensuring access for the general population to SHSs.1
Many patients attending SHSs for STI and HIV testing have no symptoms5 9 and could potentially self-sample without the need to attend a sexual health clinic (SHC). The Unity SHC delivers SHSs for Bristol, North Somerset and South Gloucestershire in the UK. The clinic provides booked appointments and walk-in clinics 6 days a week. As the workload at Unity continues to increase, booked appointments become increasingly difficult to access and walk-in patients frequently have to queue.10 This problem is often compounded as the clinic uses the same waiting areas and front desk staff for both walk-in and booked patients. In a recent survey,10 patients reported spending too long in the clinic. In response to this problem, as part of a wider evaluation of the Unity SHC, we developed a computer simulation model to examine whether introducing an online service for STI and HIV self-sampling for asymptomatic patients, in addition to existing clinic-based services, would decrease patient waiting times and improve resource use compared with the current system without online-based self-sampling.
Methods
Patient care pathways within the Unity SHC
The clinic provides services to both booked and walk-in patients requiring sexual healthcare. Patients are managed according to national guidelines from the British Association for Sexual Health and HIV11 and the Faculty of Sexual and Reproductive Healthcare.12 For booked patients, the appointments are either booked over the telephone or scheduled after previous clinic appointments. For walk-in patients, a slot system is operated where the number of appointments allocated is based on a clinical need and type of clinicians available and spaced evenly throughout the day. As demand usually exceeds supply, many patients queue in the morning to access the slots. Patients complete an initial registration form which identifies the next point of care. Patients who disclose sexual assault and/or are under the age of 18 years are prioritised and given an early slot.
Patients attending the service have a range of clinical needs (complex or non-complex). There are several factors which influence the duration of a consultation. For example, complex consultations with men who have sex with men (MSM) take longer than non-complex consultations with asymptomatic patients who only require an STI or HIV screening. Details about how clinical consultations have been grouped are described in table 1.
List of clinical presentations and diagnoses considered as complex or visual
Patients considered complex include patients at high risk of an STI or HIV, or other complex needs such as aged under 18 years who are assessed for risk of child sexual exploitation. For patients requiring a physical check/examination, this may only involve a visual examination or, in addition, treatment may be required, for example, genital warts. Specimens may also be needed for microscopy, which in women requires a speculum examination which is categorised simple unless they have complex needs for which an internal bimanual pelvic examination is required, as detailed in table 1. In men, microscopy (ie, testing for urethritis and proctitis) also increases duration of the consultation. Asymptomatic patients do not require a physical examination being able to use self-taken anogenital tract specimens for gonorrhoea and chlamydia nucleic acid amplification test (NAAT) testing. Thus, asymptomatic low-risk patients who only require STI or HIV screening are described as non-complex. However, if they are female and have other considerations, such as contraception or are under the age of 18 years, they are then described as complex.
All MSM patients irrespective of whether they need an examination are described as complex as they require detailed discussion about risk behaviour and hepatitis B and human papilloma virus vaccination. About two-thirds of MSM patients have bloods taken for HIV and syphilis serology. For some patients, it is also necessary that they see a health adviser at their visit. For example, when a woman in her early 20s attends the walk-in clinic with lower abdominal pain, she would then have a clinical discussion followed by speculum examination with samples collected for culture, microscopy and NAAT testing for chlamydia and gonorrhoea, a bimanual pelvic examination and blood taken for HIV and syphilis serology. If pelvic inflammatory disease is confirmed, she would then receive treatment and may be referred to a health adviser. Health advisers see patients with complex sexual health needs and for partner notification following a positive test. If follow-up is required, patients can be managed by an appropriate practitioner in a booked clinic.
Discrete event simulation (DES)
DES has been widely applied in modelling healthcare systems.13 This method can replicate the behaviour of a complex system as a sequence of well-defined events over time. Each event occurs at a time-point and marks a change of state in the system. A DES model is a network of queues (eg, queue for registration on arrival and queue for receiving treatment) and activities or service points (eg, having consultation and receiving treatment). A service point represents the interaction between a patient and resources, which takes time to complete. One of the major advantages of using a DES model is its flexibility to incorporate patient demographics, such as gender and age and complex clinical scenarios at the individual level to influence the care pathway taken and the time between events.13 14 Typically, within a DES model, individuals enter a system, pass through a series of queues and visit various service points before exiting the system. The variables that govern the movement of modelled individuals (such as patient arrival time and duration of treatment) can be drawn randomly from underlying distributions to readily capture the variation that is inherent in healthcare.
Model formulation
The patient care pathways consisted of patient registration, consultation and clinical check/examination with sample collection (blood, urine and/or vaginal swab) and processing, results counselling and treatment, health promotion counselling and nurse-led booked follow-up consultation. The care pathways for male booked and male walk-in patients are identical, and are also identical for female booked and female walk-in patients. A DES model schematic of the patient care pathways is shown in figure 1. Asymptomatic patients who opted for self-sampling were managed by a virtual receptionist in our model, but these patients would obtain their self-sampling kits via a computer interface. If an infection was identified, the patient would be notified by telephone and offered a clinic appointment for treatment.6 15 The model was coded to allow patients to receive results counselling and treatment from the same healthcare practitioner (HCP) who examined them earlier in the care process.

Patient care pathways within the Unity SHC using SIMUL8 software. The care pathways for MB and MW patients are identical, and are also identical for FB and FW patients. The service points within the MB, MW, FB and FW care pathways are also shown in column 1 of table 2. The four service points labelled as consultation MB, consultation MW, consultation FB and consultation FW are dummy activities through which patients are only directed to the next points of care. This was achieved by setting the process time of these activities to zero using a fixed distribution. BF, booked follow-up; FB, female booked; FW, female walk-in; HCP, health care practitioner; HA, health adviser; MB, male booked; MW, male walk-in; MSM, men who have sex with men; Q, queue; SHC, sexual health clinic.
The arrival time of patients, gender, appointment type (booked/walk-in) and proportion of patients at each service point were derived from the electronic patient record (EPR) of the Unity SHC covering from 3 January 2017 to 31 December 2017. These data related to 24 010 patient visits, of whom 12 226 (51%) were women with an average age of 28.8 (9.1, SD) years and 11 784 (49%) were men (including 3616 (31%) MSM) with an average age of 32.1 (10.8) years. We randomly sampled (Poisson number/exponential interarrival) the arrival time of patients at the clinic based on an estimated 11 patients arriving every hour on average. The number of patients arriving each hour was represented by the Poisson distribution, while the exponential interarrival times were set for the hourly segments of each day. This was achieved through the ‘day planner’ option in SIMUL8. We did not select the ‘equally spaced within interval’ option as it is not recommended for life-like simulations. Given that patients arrive to the Unity clinic via one queue, some patients with booked appointments might be late in reporting to the reception. As such, we did not select the 'equally spaced within interval' option since this might not always be adhered to in a life-like situation via a common entry to the clinic. To mitigate this, the interarrival times were set for the hourly segments of each day rather than a longer time segment. We applied the same approach for the analysis of all scenarios to produce valid comparisons.
It is possible that a walk-in patient can turn up in the morning, get a slot in the afternoon and come back nearer the time. We did not model this delay because this patient will essentially be one of the hourly 11 patients arriving later in the day. If we were to model this delay, it would have had an unrealistic impact on the average walk-in patient waiting times in the clinic. A patient who does not get a slot can always come back another day and be included in that day’s arrival.
Proportions of patients from reception (and subsequent service points) to the next point of care are shown in table 2; for example, 2% of the female patients come to the clinic for health promotion counselling. Service time data (eg, duration of consultation, examination and treatment) were estimated by three clinical consultants (MC, PH and HW) because these data were not readily available from the EPR. We used probability distributions to model the variation in service times (table 2), as these vary depending on the workloads, number of staff, patient factors and demands from the rest of the clinic.
Various model inputs
The human resources in the model included three receptionists, eight HCPs (two for male booked patients, two for female booked patients, two for male walk-in patients and two for female walk-in patients), four nurses (two for booked follow-up patients and two for laboratories who work between the laboratories depending on demand) and one health adviser (who serves patients from both booked and walk-in clinics). The cost parameters shown in table 2 are based on staff time only and derived from nationally published pay scales of NHS employers for 2019.16 We did not include diagnostic, treatment, building and administration costs in our estimations. All patients, apart from those who came for health promotion counselling or contraception only, were assigned a fixed cost of £2.61 based on 5 min of two healthcare assistants’ time (£0.26 per minute) for processing STI and HIV specimens.
We added the provision of online-based self-sampling to existing clinic-based services. Based on findings from the literature,3 6 we assumed that 50% of asymptomatic patients would opt for an STI or HIV self-sample. We then varied this assumption in sensitivity analyses by ±20%. The average cost of managing each patient via online (self-sampling and testing) was estimated to be £6.42 (online supplementary appendix 1), which is based on testing provided in-house at the Unity SHC. We also conducted two ‘what if’ scenario tests. First, we increased the number of HCPs from eight to ten (two for male booked, three for male walk-in, two for female booked and three for female walk-in patients) in a system without online-based self-sampling. This scenario explores the extent to which online-based self-sampling might act as a substitute for increasing clinic staff resources. Second, we increased the number of patients arriving to the clinic by 10% (from 11 to 12 per hour) in a system with online-based self-sampling for 50% of asymptomatic patients and compared this to the current system without online-based self-sampling with 11 patients arriving per hour, to explore how the system responds to increased demand that might be generated by the greater accessibility of online-based self-sampling.
Supplemental material
The model was constructed using the SIMUL8 software. The model simulated the Unity SHC over a 4-week period, operating 8 hours a day from Monday to Saturday. Each simulated individual was tracked through the care process; the population effect was then estimated from the sum of the individual effects. We performed a trial of 1000 model runs and considered patient waiting times as the main outcome measure. The Unity SHC that we modelled starts and ends the day empty, hence it was not necessary to incorporate a warm-up time in the model.
The model was developed in close collaboration with the clinical experts; meetings were held at various stages of the model development process to discuss the structure and parameters underlying the model. This included developing the appropriate patient care pathways to adequately capture all relevant events, that data inputs were relevant and clinically appropriate, and ensuring outputs were consistent and of clinical importance. The continuous engagement of the clinical staff throughout the study significantly increased the confidence in the face validity of the model. The model coding was cross-checked to detect any errors wherein PH verified the coding written by SM. Two one-way sensitivity analyses (the provision of online-based self-sampling was varied by ±20%) were performed to ensure varying parameter inputs had a viable and hypothesised impact on the model outputs. We also tested the internal working of each model component during the model development phase. For example, in demand generation processes, the model was run to check if it was generating as many patients as expected. Patient waiting time data were compared with those observed with the existing configuration of the service.10
Patient and public involvement
No patient or public was involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
We identified some bottlenecks under the current system, particularly within the consultation and treatment queues for male and female walk-in patients. However, these bottlenecks receded when the provision of online-based STI and HIV self-sampling for asymptomatic patients was added to the current system. Table 3 shows that patients spent on average 31% less time (88 vs 128 min) in the clinic following the addition of online-based self-sampling for 50% of asymptomatic patients. Female walk-in patients were found to spend approximately 39% less time (110 vs 179 min), while male walk-in patients spent approximately 38% less time (100 vs 162 min) in the clinic. There was no effect on the time patients spent for health promotion counselling and nurse-led booked follow-up appointments. This is because resources assigned within these activities are not required elsewhere in the system. Sensitivity analyses had the expected impact when we varied the provision of online-based self-sampling for 50% of asymptomatic patients by ±20% (table 3).
Impact on patient waiting times (min) in the system (ie, from arrival to exit) under different scenarios
The average cost of staff time for managing each patient was higher for the current system (£88.74) compared with the average costs for the current system with the addition of online-based self-sampling for the following proportions of asymptomatic patients: 50% (£72.64), 30% (£80.46) and 70% (£64.84). Under the 'what if' scenario of increased HCP numbers (from two to three for the male and female walk-in clinics), the average patient waiting time decreased by 50 min (78 vs 128 min) for all patients (table 3), but increased the average cost for managing each patient substantially from £88.74 to £116.23.
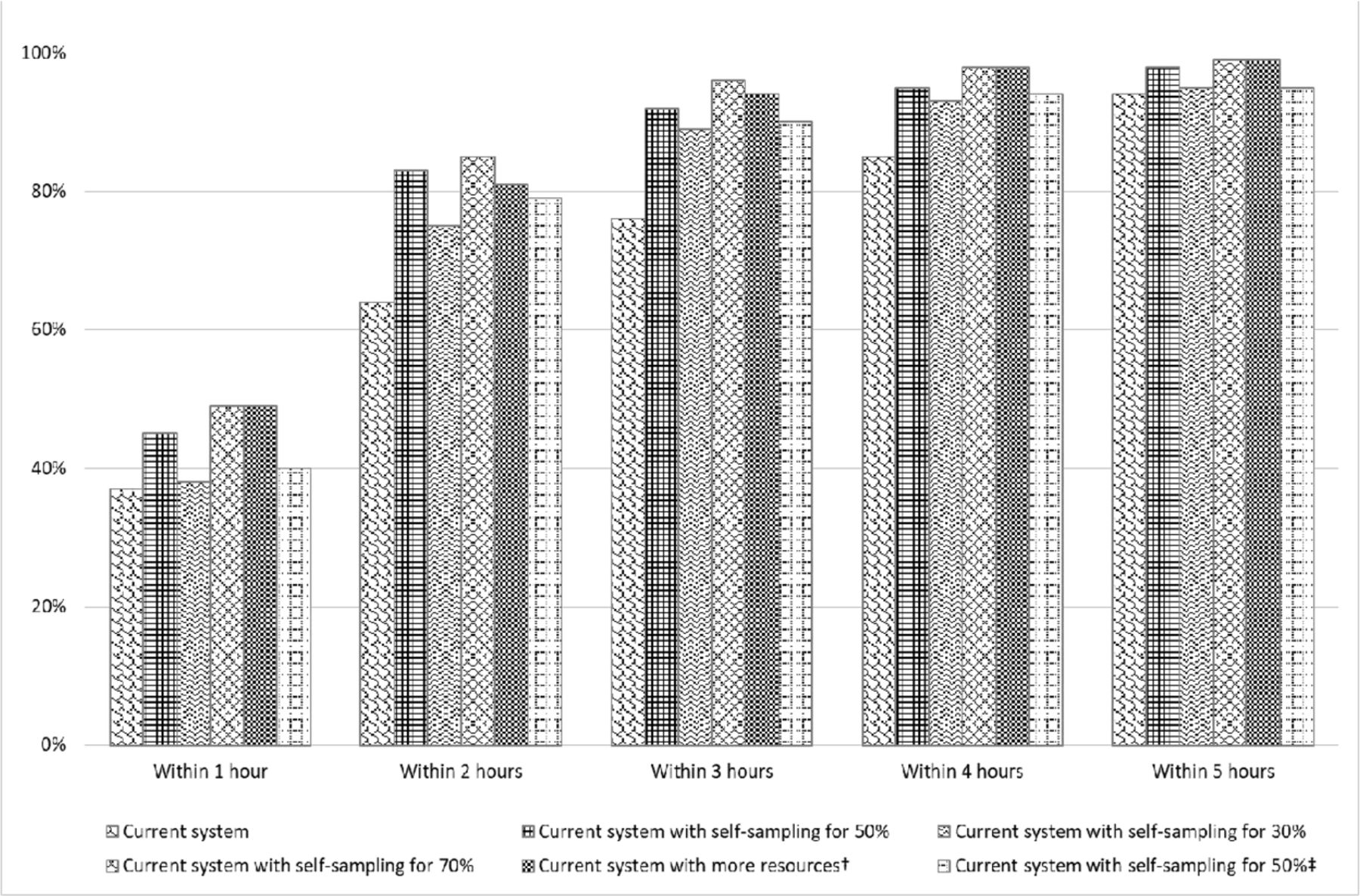
Figure 2 shows that the proportion of patients who went through the system (ie, from arrival to exit) within 2 hours increased substantially after introducing the provision of online-based STI and HIV self-sampling to the current system.
{kind=link}
{kind=link}
Proportion of patients who went through the system within various time limits. †increased the number of healthcare practitioners from two to three for the male and female walk-in clinics and ‡increased the number of patients arriving to the clinic from 11 to 12 per hour.
Under the what if scenario with 10% increased patient demand, the average patient waiting times still decreased substantially from 128 to 99 min for all patients, from 162 to 117 min for male walk-in patients and from 179 to 127 min for female walk-in patients, while the average cost for managing each patient also decreased substantially from £88.74 to £72.98. This shows that the provision of online-based STI and HIV self-sampling can help decrease the average patient waiting times and also release resources to manage the increase in demand for access to services.
Discussion
Regular testing for STIs and HIV with rapid treatment and partner notification are important strategies for control.1 17 SHSs in the UK are under increasing pressure to improve patient experience and halt the rise in STIs while also reducing costs.1 2 We developed a DES model for providing integrated sexual healthcare within a specialist SHC and adapt this to represent introduction of an online service for STI and HIV self-sampling for asymptomatic patients. Our results suggest that the provision of online-based STI and HIV self-sampling alongside existing clinic-based services would decrease the average patient waiting times and reduce the cost of staff time for managing the patients. In addition, it would save money and release resources when provided in-house, which could be used to provide funding for the increased new demand that such a service will generate.4
Strengths and limitations
This paper uses a computer simulation method to capture the behaviour, performance and resource requirements of a specialist SHC to inform service improvement and business case preparation for services who are under pressure to reduce costs and considering introducing a service for STI and HIV self-sampling. The care pathways were developed through discussions with staff at the Unity SHC and are based on the actual clinic workflow. We grouped the patient care pathways into various categories: 4 for heterosexual men, 3 for MSM and 7 for women based on a consultation complexity and need for examination with or without microscopy. This has similarity with the approach to costing used by pathway analytics.18
In order to make the model manageable, we simplified the number of clinical care pathways and combined some. For example, not all follow-up patients were seen within the nurse-led booked follow-up clinic; some were also seen within the booked and walk-in clinics, but incorporating this for the purposes of this model was felt to be unnecessarily complex. We feel this was a reasonable compromise and is unlikely to alter the overall conclusions which can be drawn from the model. We assumed that no MSM patient will use online-based self-sampling as this patient type usually prefers clinic-based face-to-face sampling by HCPs,19 20 but this may not always be the case. However, the overall patient waiting time and cost of staff time would likely be further reduced if some MSM patients were to use online-based self-sampling.
We did not include fixed overheads such as building and administration in our cost estimations as these overhead costs do not fluctuate with service activity.5 Nor did we include diagnostic and treatment costs as within the scenarios explored these will remain the same; diagnostic tests are undertaken within the same laboratory and patients diagnosed with an infection are assumed to attend for treatment. The cost of providing online self-sampling was based on actual practice undertaken at the Unity SHC. This is currently managed through the chlamydia screening programme (CSP) with patients accessing the online service via the Unity SHC website. The CSP has considerable experience of using telephone consultations to arrange patient treatment either through a local pharmacy or by attending the Unity SHC and undertaking partner notification.15 We did not include the cost of adapting the clinic website to enable online test ordering. The Unity SHC is moving to an online registration and booking facility (MillCare, Mill Systems, Belper, Derbyshire) through which online-based self-sampling can be administered. We did not explore the effect of providing online services through an external provider, which would be more expensive (>£30)4 compared with £6.42 and would require disinvestment in microbiology services with the cost savings agreed locally.
We are not aware of any other patient flow model of a specialist SHC which includes available care pathways and the ability to incorporate the probabilities that these will be used based on actual data from EPR. We used 12 months of EPR data to populate the model, and such a model has not been developed previously to examine the patient pathways of care as this was felt to be too complex.21 However, service time data were estimated by three clinical consultants (MC, PH and HW) since these data were not readily available from the EPR. A usual supposition is that the distribution for most activities in a project network is right skewed, but it does not guarantee the use of a specific distribution. It might have been more appropriate to use a log normal distribution to sample the service time data, but we used an average distribution in simulations as we only needed to input our estimate of the average (mean) of the time and a large variability was desired. An average distribution in SIMUL8 is a normal distribution with the SD set to ±25% of the mean. This was mitigated by using the same distributions for the analysis of all scenarios. The use of a log normal distribution would require one to collect two parameter values (mean and SD) to potentially incorporate uncertainty more appropriately.
Viana et al22 developed a composite model in which a DES model of a hospital outpatient department that treats patients with chlamydia was combined with a system dynamics model of the infection process in the community. Their model shows how the prevalence of chlamydia at a community level affects operational level decisions made in a hospital outpatient department. We believe our model complements other modelling approaches which have investigated the potential impact of innovations in SHSs on quality of care and costs.21 23–25
Implications
The outcomes reported here are hypothetical, but the model is readily adaptable for use by both commissioners and providers to examine the costs associated with introducing an online service and its potential effect on capacity at SHSs, including ability to release costs. Given the reduction in funding and the continuing rise in STIs1 with a new requirement to increase testing access for all who practise unprotected sexual intercourse with a new or casual partner, online-based self-sampling offers the opportunity to increase capacity to do this. However, if asymptomatic patients are actively directed to online-based STI and HIV self-sampling, this may result in about one-third not testing.4 5 We observed that there would be a cost saving if the provision of online-based STI and HIV self-sampling is provided in-house and thus releases resources to respond to increased demand for services by approximately 10%. Developing an in-house service could be achieved through reallocation of staff roles, enabling time to realise savings through natural wastage and/or using these staff to see more complex patients given the continuing increase in demand.
Turner et al4 observed that "Online services for STI testing are not ‘standalone’. They change STI testing behaviour with impacts on all elements of the sexual health economy". The provision of online-based self-sampling can be considered in addition to existing clinic-based services in order to increase the uptake of STI and HIV testing and to decrease the average patient waiting times, but this should not be viewed as a panacea for cutting costs. Online services for STI and HIV self-sampling for asymptomatic patients would free up staff time for seeing more complex patients, but careful consideration needs to be given to how these services can be provided and integrated with traditional face-to-face services.
Further innovations, in addition to the availability of online-based self-sampling in the provision of SHSs, are required, which do not reduce the quality of face-to-face services provided if more at risk people are to be tested while reducing costs as necessitated, given the reduction in public health funding. Although the introduction of point of care testing has the potential to be cost saving, this remains to be demonstrated.21 23 24 The Unity SHC is in the process of implementing the introduction of an online service for STI and HIV self-sampling in conjunction with a new rapid STI service which can potentially provide the result of gonorrhoea and chlamydia NAATs within 4 hours from the time of collection. This is being formally evaluated by National Institute for Health Research Applied Research Collaboration West (https://arc-w.nihr.ac.uk/). This will be the subject of a future publication. We propose to model the potential impact of near patient or point of care testing for STIs using the DES methodology described here and then formally to evaluate how the model would reflect the observed outcomes with the new Unity rapid STI service incorporating an in-house online-based self-sampling service.
Conclusions
The DES model presented here could be reconfigured for a different location and repopulated with the appropriate data without the large organisational changes that are required if changes are tried out in the real world to estimate the potential savings and benefits of introducing an online-based service for STI and HIV self-sampling. SHSs in different geographical areas may differ slightly in terms of opening hours or number of human resources in service but will share many common features in terms of patient care pathways. The provision of online-based STI and HIV self-sampling for asymptomatic patients intending to attend SHSs could be beneficial in reducing the average patient waiting times, and the model highlights the complexities of using this to cut costs. Attributing recognition for any improvement requires care, but DES modelling can provide useful insights into the design of SHSs ensuing in quantifiable improvements. Extension of this method with the collection of additional data and the construction of more informed models seems worthwhile.
References
Footnotes
Contributors SM developed the model and identified the model parameters, including use of statistical analyses conducted by RG. PH, MC and HW commented on the clinical validity of the model. SM and PH drafted the manuscript. WH and PM revised the draft critically, while JS and JT commented on the draft.
Funding This research was supported by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care West (NIHR CLAHRC West), now recommissioned as NIHR Applied Research Collaboration West (NIHR ARC West).
Disclaimer The views expressed are those of the authors and are not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.