Article Text

Abstract
Objective To systematically identify and describe studies that have evaluated the impact of gardens and gardening on health and well-being. A secondary objective was to use this evidence to build evidence-based logic models to guide health strategy decision making about gardens and gardening as a non-medical, social prescription.
Design Scoping review of the impact of gardens and gardening on health and well-being. Gardens include private spaces and those open to the public or part of hospitals, care homes, hospices or third sector organisations.
Data sources A range of biomedical and health management journals was searched including Medline, CINAHL, Psychinfo, Web of Knowledge, ASSIA, Cochrane, Joanna Briggs, Greenfile, Environment Complete and a number of indicative websites were searched to locate context-specific data and grey literature. We searched from 1990 to November 2019.
Eligibility criteria We included research studies (including systematic reviews) that assessed the effect, value or impact of any garden that met the gardening definition.
Data extraction and synthesis Three reviewers jointly screened 50 records by titles and abstracts to ensure calibration. Each record title was screened independently by 2 out of 3 members of the project team and each abstract was screened by 1 member of a team of 3. Random checks on abstract and full-text screening were conducted by a fourth member of the team and any discrepancies were resolved through double-checking and discussion.
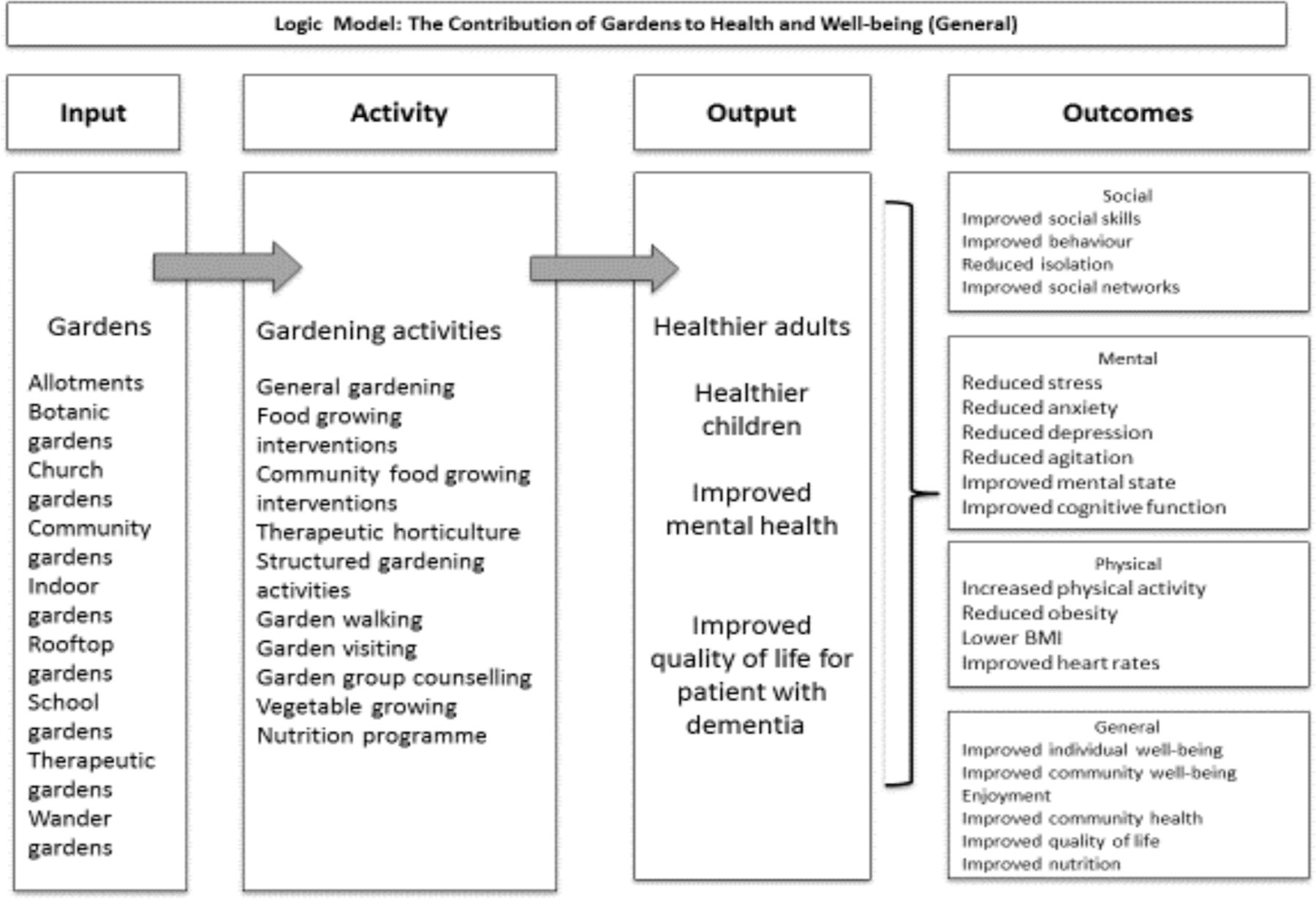
Results From the 8896 papers located, a total of 77* studies was included. Over 35 validated health, well-being and functional biometric outcome measures were reported. Interventions ranged from viewing gardens, taking part in gardening or undertaking therapeutic activities. The findings demonstrated links between gardens and improved mental well-being, increased physical activity and a reduction in social isolation enabling the development of 2 logic models.
Conclusions Gardens and gardening can improve the health and well-being for people with a range of health and social needs. The benefits of gardens and gardening could be used as a ‘social prescription’ globally, for people with long-term conditions (LTCs). Our logic models provide an evidence-based illustration that can guide health strategy decision making about the referral of people with LTCs to socially prescribed, non-medical interventions involving gardens and gardening.
- social medicine
- public health
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first scoping review to explicate the breadth and depth of evidence about the impact of gardens and gardening on a range of health and well-being outcomes.
Gardening as a construct lacks definition leading to associated challenges with the location and curation of papers.
Lack of a ‘standardised’ garden or gardening approach has influenced a myriad of research designs, preventing meta-analysis.
Our paper provides robust evidence-based guidance via logic models to guide health strategy decision making.
Rationale
Long-term conditions (LTCs), also referred to as chronic diseases, such as cardiovascular disease, chronic respiratory disorders and cancer, remain a significant cause of death globally.1 Contributing to these figures, mental ill-health is the largest single cause of disability worldwide representing 14% of the global population, with depression accounting for 4.3%.2 Socioeconomic factors such as education and employment can also influence health and well-being and health inequalities, and can often lead to increased risk of chronic conditions.3
In the UK, the management of LTCs is challenged by unmet social needs which are attributed to increased attendance at General Practitioner (GP) surgeries.4 Patients with LTCs require multipurpose, complex interventions combining interprofessional and intra-agency responses. Hence, it is predicted that LTCs will outstrip universal health and social care service provision, forcing healthcare strategists to appraise the effectiveness of existing pathogenic interventions. However, the traditional medical management of people with LTCs does not tackle their social needs leading to repeat primary care appointments and unnecessary admissions to secondary care.5 Consequently, there is a demand to explore alternative, non-medical, salutogenic (non-pathogenic) global approaches that could empower patients with LTCs to reduce their dependence on health and social care services.6
Social prescribing is a non-medical method of care which ‘links patients in primary care with sources of support within the community to help improve their health and well-being’.7 This salutogenic process focuses on promoting well-being by referral to a range of non-medical approaches, from exercise on prescription, to arts-based activities and beyond.6–9 The complex relationship between health communities and its citizens is largely influenced by wider social determinants.10 Place-based community organisations which invest in the community are able to respond to and support the wider social determinants of health.10
A popular social prescribing approach offered by place-based organisations is the use of gardens and gardening as a nature-based activity to improve health and well-being.11 The use of nature as an intervention is increasingly being recognised worldwide as a means of improving social, emotional, mental and physiological outcomes and is of potential value for people with LTCs. In a recent meta-analysis by Soga et al, the impact of gardening and gardens on a range of physical and mental health outcomes was demonstrated to have positive health and well-being benefits.11 However, this meta-analysis only considered a limited range of methodologies, focusing on papers that compared health outcomes in control and treatment groups after participating in gardening. Typically, nature-based interventions comprise a broad spectrum of interventions, activities and outcomes that include plants, the natural environment and living creatures, and of interest here, is the recognition that gardening supports people with LTCs.12 People with chronic conditions can engage in nature through being in gardens and through gardening activities such as allotment gardening13 to guerrilla gardening14 and community gardening.15 Gardens are used to cultivate flowers, exercise, connect with others and grow food. In this article, we adopt this broad definition of gardening and evaluate the full range of interventions within our scoping review. In doing so, we produce a range of logic models and results to demonstrate the benefit of different forms of gardening across the globe.
To date, there have been no studies that have specifically explored the breadth of literature about the effectiveness of gardens and gardening that could help prevent the impact of rising levels of chronic disease.
Review aim and objectives
Our scoping review aimed to identify and describe the evidence base on the impact of gardens and gardening on the physical and mental health and well-being of populations. The objectives were to understand the benefits of gardens, provide a map of the literature, types of gardens and health outcomes and build evidence-based logic models to guide healthcare strategists’ decision to use of gardens and gardening as a non-medical, social prescription. We agreed on the following review question ‘What evidence is there on the physical, mental, health and well-being benefits of gardens?’.
Methods
To address the global gap in evidence, we employed a scoping review methodology. Scoping reviews provide a systematic and robust means of reviewing the breadth of evidence in a wide field and are useful in synthesising the increasing arsenal of evidence, in contrast to a more traditional systematic review that focuses on answering a particular question.16 We employed Arksey and O’Malley’s validated framework to map the evidence.17 This was particularly relevant as the aim of the scoping review was to explicate the impact of gardens and gardening on diverse outcomes and populations. The resultant map of the evidence was used to develop evidence-based logic models to illustrate the key health and well-being outcomes as graphic tools to support clinician and commissioner decision making.18 The initial scoping review framework was refined to provide an appropriate method based on the following steps.19 20 This involved: 1. Identifying the research question. 2. Identifying relevant studies. 3. Study selection. 4. Charting the data. 5. Collating, summarising and reporting the results. 6. Consultation. Stages 1–4 were conducted iteratively. Stage 5 was undertaken following stages 1–4 and stage 6 (consultation) occurred throughout the lifetime of the review between our research team and our external national stakeholder. Boxes 1 and 2 detail the databases and journals searched.
Databases searched
Database name
MEDLINE
CINAHL
PsychINFO
Web of Knowledge/Science
Scopus
HMIC
Science Direct
Social Care Online
ASSIA
Cochrane Database of Promoting Health Effectiveness Reviews
Joanna Briggs systematic reviews
Greenfile
Environment Complete
AMED
Social Policy and Practice
Journals searched
International Journal of Agricultural Sustainability
Journal of Environmental Planning and Management
Health and the Natural Outdoors
Journal of Environmental Psychology
Psychological Science
Environment and Behaviour
Environmental Health Perspectives
Landscape and Urban Planning
Urban Forestry and Urban Greening
Journal of Social Issues
International Journal of Environment and Health
International Journal of Environmental Health Research
International Journal of Environmental Research and Public Health
Journal of Public Health
Public Health
Environmental Science and Technology
Journal of Epidemiology and Community Health
Health and Place
Environmental Sciences
Search and selection of studies
We undertook a comprehensive and iterative search to capture the range of perspectives relating to gardens. We searched from 1990 onwards to capture evidence as recommended by Arksey and O’Malley.17 In April 2017, we searched 15 electronic databases and six key journals capturing health, social, psychological and environmental perspectives, grey literature sources and websites (including Google Scholar). We repeated the search in September 2018 and November 2019 to capture additional literature published. It is recommended that scoping reviews engage interprofessional teams as they bring a breadth and depth of knowledge.19 Correspondingly, our team was interdisciplinary with subject and methodological expertise comprising a nurse with experience in social prescribing and nature-based approaches, a geographer with expertise in urban agriculture and sustainable cities, and two health information specialists with additional expertise in systematic review methodology. Our external stakeholder was a national body representing a wide range of gardening interests. We defined gardens as being:
intimate private spaces attached to private households but they can also be large private or formal gardens open to the public, or part of hospitals care homes or hospices.21
We modified the protocol throughout the initial search and filtering process to ensure the project remained manageable and faithful to the initial research question and definitions. We searched in a wide and sensitive manner to encompass the diverse types of gardens that could be located within green space or nature-based type of activities. A range of thesaurus and free-text terms (adapted per database) to describe the different types of gardens, and potential breadth of health outcomes were used (see online supplementary appendix for example). To ensure robustness, our search followed the agreed protocol and the results were stored on Endnote web reference management software function to manage and track references throughout the scoping review process which was shared across the project team. We recorded search strategies with details of the date the search was undertaken and the number of results obtained and issues arising during the searching to provide a complete history of the search process and provide transparency of the review process.
Supplemental material
We agreed an initial set of inclusion and exclusion criteria following the scoping searches and set these out in the protocol. A study was included if it met the definition of gardens,21 had a measurable outcome on health or well-being, and was published in English after 1990. Ultimately, gardens comprise numerous interacting components, outcomes and populations and may be described as complex interventions.22 We therefore ensured that there were no restrictions on study design, biometric indicators or population groups. Systematic reviews summarise the results of studies answering a focused question and within the evidence-based healthcare policy context, they are acknowledged as ‘gold standard’ evidence;23 no systematic reviews covered the breadth of our review question, so they were included as studies in their own right. We searched for non-experimental and quasi-experimental studies, which included non-equivalent control group pretest post-test studies and single group non-controlled designs19 and studies that determined causality through non-randomisation. We excluded other green spaces such as forests or parks and studies on access to green spaces or living near green spaces. We excluded biological indicators of soil or plants, dissertations, theses, conference presentations, abstracts or posters. We also excluded studies which used process indicators rather than health outcomes and studies which included gardening as part of other interventions where the effects could not be separated.
Three reviewers (AB, MHo, MHa) jointly screened 50 records by titles and abstracts to ensure calibration. Once this was achieved each record title was screened independently by two out of three members of the project team (AB, MHa, Mho), then each abstract was screened by one member of a team of three (AB, MHa, Mho), and full-text screening was conducted by one member of a team of three (AB, MHa, Mho). Random checks on abstract and full-text screening were conducted by a fourth member of the team (MM). Any discrepancies were resolved through double-checking and discussion.
Charting, collating and summarising the data
We used Microsoft Excel to create a data extraction template that could automatically populate evidence tables. Through team discussion we agreed on elements to extract (column headings) based on study characteristics, green space characteristics, intervention characteristics, health condition, age group, outcome measures, findings and author conclusions. When reporting findings for experimental studies, effect sizes and CIs were included as appropriate; for systematic reviews and other designs narrative findings were reported. One member of the project team (MM) extracted all the data up to 2017 and MHo to 2019. We used the evidence tables to organise and synthesise the data to enable us to map the benefits of gardens in relation to different types of gardens, health outcomes (physical, mental and well-being) and health conditions.
Consultation with partners and patients
We engaged local nature-based partners throughout this review process. We involved a national nature-based stakeholder organisation in developing the review protocol and presented and sought feedback on the results at an Economic Social Research Council funded event of community leaders (including the national stakeholder organisation), third sector organisations, the general public and public health representatives with an interest in gardens and gardening.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy. However, we consulted the general public through a community engagement event with residents and local providers of gardening programmes.
Results
Search results
From 8896 citations, we located 77 full-text studies* (figure 1).24

PRISMA diagram: searching and sifting process (adapted from Moher et al [24]). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Description of studies
A total of 77 studies was included in this review.11 25–100 Country of origin included the UK, USA, Brazil, South Korea, Taiwan, Japan and the Netherlands. All the studies described complex interventions, using heterogeneous methodologies, comprising 14 types of study designs. The scoping review highlights the methodological challenges associated in determining causality with complex interventions. There was an even split between experimental/quasi-experimental (29%) and non-experimental studies located (37%). Non-equivalent control group and single group pretest, post-test were the most frequently used quasi-experimental study designs (20%). There were 8 randomised controlled trials (9%)28 31 35 43 56 59 65 96 and 13 (16%) systematic reviews.26 32 42 44 60 64 75 83 86 90 94 97 98 All, barring one60 of the systematic reviews reported heterogeneous complex interventions. We present two evidence-based tables detailing higher-level evidence from systematic reviews and randomised controlled trials (see tables 1 and 2); full evidence tables available from authors on request.
Evidence summary: randomised controlled trials
Evidence summary: systematic reviews
Description of gardening interventions
The scoping framework17 enabled us to locate and include a broad range of evidence, likewise, using the predetermined21 definition of gardens enabled the capture of diverse types of gardens. Typical gardening interventions included ‘allotment gardening’ (n=8) and ‘Community gardens’ (n=11). The most common garden intervention reported was horticultural therapy (n=17) which integrates a structured gardening programme with qualified therapist input. The second most popular approach was ‘structured gardening’ (n=17) which provides a structured programme of activities but does not include a qualified therapist. Irrespective of garden ‘type’ all garden activities were characterised through a range of physical activities such as ‘planting seeds’, ‘potting on’, ‘taking cuttings’, ‘pricking out’, ‘sweeping and maintaining the garden’, ‘using and cleaning tools’ and other similar tasks.
Description of outcome types
We located a range of study methods which reported outcomes related to mental health, physical impact, nutritional behaviour changes and overall general well-being. There were over 35 validated health and well-being outcome measures reported. Most papers examined the impact of gardens on mental health (36%). General well-being represented 32% of the total outcomes reported. There was an even split between those papers reporting on specific physical outcomes (14%) and those reporting on nutrition as an outcome (18%). The heterogeneous outcomes may explain the paucity of meta-analyses (3.7%).
Development of the logic models
A secondary objective was to use this evidence to build evidence-based logic models to guide health strategy decision making about gardens and gardening as a non-medical, social prescription. Logic models illustrate causal relationships between service inputs, resultant activities, outputs and goals, emphasising the contributory factors to successful programmes.101 The structure and organisation of logic models enable the results from scoping reviews and systematic reviews to delineate complex interventions, such as those without specific, controlled parameters thus enabling greater insight into the interactions between the intervention, in this case gardens and gardening, and the multiple outcomes.102 Logic models can represent causal processes and encapsulate complex interventions and illustrate heterogeneous outcomes.18 Hence, logic models provide an evidence-based tool that can support policy makers, healthcare strategists and/or primary healthcare clinician’s decisions about commissioning non-medical approaches through social prescribing.
Logic model: evidence evaluating the impact of gardens on mental health
There were 29 (36%) studies that focused on the impact of gardening on mental health. We set parameters for mental well-being to include four main areas of interest: psychological well-being, depression, anxiety and mental status. In the latter, we resolved that mental status included pathological disorders such as dementia, schizophrenia, bipolar and other chronic LTCs. Some categories overlapped, for example, papers with a focus on psychological well-being often captured outcomes relating to depression making the creation of distinct categories problematic. Commonly reported data collection methods included validated tools such as the Warwick-Edinburgh Mental Well-being Scale103 or New Economic Foundation’s Five Ways to Well-being,104 which offer observational subjective data as opposed to direct causality. Evidence from our review indicated a range of benefits that gardening had on diverse populations. Typically, gardening enabled greater social interaction with others92 and improved physical activity,100 thus improving overall mental well-being,32 reducing depression76 and anxiety.59
A significant percentage of papers (36%) focused on mental health, and of these, the majority (57%) used experimental or quasi-experimental designs. The causal relationships illustrated in our first logic model highlights the range of garden activities that contributed to an improvement in mental health (see figure 2). These papers typically reported that gardens and gardening augmented physical activities resulting in improved physiological outcomes such as reduced cortisol levels32 35 96 and saliva amylase levels.96 Additionally, the logic model graphic enables visual representation of how mental health was improved through enhancing sociological outcomes leading to reduced socialisation through improved social networks.

Logic model: mental health.
Logic model: evidence evaluating the impact of gardens on general well-being
In determining a parameter for well-being, we used the study by Dodge et al105 who asserts that ‘stable ‘well-being’ is when individuals have the psychological, social and physical resources they need to meet a particular psychological, social and/or physical challenge’. Hence, a range of well-being indicators were reported that relate to both mental and physical well-being outcomes. A total of 26 (32%) papers reported general well-being and typically focused on positive health; examples are27 78 100 social health, 26 30 32 47 48 subjective well-being 54 94 and/or quality of life.35 38 77 79 98 Typical LTCs studied included chronic lung disease27 diabetes, hypertension and kidney disease.70 Outcomes that measured impact of gardens on nutrition were broad and included dietary changes, and increase in fruit and vegetable intake. There were 13 studies that explicated the impact of gardens and gardening on nutritional intake.29 31 42 51 54 58 60 75 81 86 96 98 Key outcomes used as predictors for nutritional impact included validated scales for well-being, emotional health, mental health and physiological indicators. Overall, the findings report that the gardening interventions have a positive impact (81%) on nutritional intake of fruit and vegetables and a range of physiological outcomes and general well-being.
The second logic model (see figure 3) provides an illustration of how gardens can benefit general well-being. The range of garden types located in the scoping review influenced activities that led to improved well-being outputs for adults, children and older people. Several positive outcomes were reported including social: involving skills, behaviours and networks; general mental well-being, such as stress reduction,35 94 reduced anxiety and depression.28 60 65 As with the mental health logic model, the graphic illustration enables visual representation of the overlap between the mental, physical, social and emotional outcomes. Thus, papers that reported impact on general well-being also included outcome measures that indicated increased physical activity resulting in reduced body mass index43 and healthier blood glucose levels,43 and general well-being that benefited community growth,66 social interaction62 68 and quality of life.44 66 76
{kind=link}
{kind=link}
{kind=link}
Logic model: well-being.
These evidence-based logic models report the diversity of gardens and gardening interventions and subsequent benefits on a range of populations that may typically live with LTCs. The resultant outcomes reported provide confidence for clinicians considering gardens or gardening as a social prescription for a range of populations.
Discussion
The increasing interest in social prescribing as a non-medical approach, has gained international attention.106 Salutogenesis influences the question ‘what makes people healthy?’ rather than, ‘how do we treat disease?’. Well-being is increasingly promoted through contemporary public health strategies to help reduce LTCs.107 Although research explicating the impact of gardens and gardening may be inhibited by the broad construct, the paradox here, suggests that it is the range offered that instigates the salutogenic response, ultimately impacting on the wider social determinants of health and benefiting diverse populations. Our findings indicate that diverse populations with LTCs could benefit from gardens and gardening as a salutogenic, social prescription and is the first to use a robust scoping review using a systematic approach to highlight these benefits.
Typically, gardening can help improve physiological outcomes associated with LTCs such as blood glucose levels, cortisol levels, HRV, blood lipids and salivary stress cortisol. Similar findings were identified by Nicklett et al84 and Ohly et al86 who reported positive physiological outcome measures on a range of biometrics including urinalysis, total fat, body mass index and systolic/diastolic blood pressure as outcomes. These findings, coupled with this review, demonstrate positive outcomes for a range of population needs including those living with obesity, diabetes, cardiovascular disease and other LTCs. The well-being of an individual is fundamental to health and is predicated on the social progression and quality of life, typically influenced by positive physical and mental health. Similar to Bragg et al30 our review identified that gardens and subsequent activities can help improve mental health. Bragg et al30 suggest that growing food can help combat stress and reduce associated depression. Likewise, Kam et al59 report positive emotional and social improvements for those who participated in a gardening programme. The benefits of gardening on mental health outcomes also extends to other LTCs known to influence frequent attendance to Accident & Emergency (A&E,) front-line health providers or GPs.108
Our scoping review has implications for researchers seeking to explicate the impact of nature-based solutions on populations. There is a predilection for the use of quasi-experimental pretest, post-test designs as they appear to provide a good opportunity to test out nature-based solutions in a range of contexts and populations. This suggests that research favours natural experiments that enable observation of communities and populations with allocation of control. As an assessment of effectiveness rather than efficiency, natural experiments may also provide opportunity for external validity and local meaningful generalisation.109 However, challenges associated with refining nature-based interventions and controlling confounders may have influenced the dearth noted in natural experiments within this review. The lack of definition limited the ability of the review to categorise gardens and gardening as typical interventions. Ultimately, this also resulted in a plethora of methods used to examine the impact of gardens, and limited opportunities for meta-analysis. The prevailing positivist paradigm needs to be revisited within this context and greater consideration proffered for the use of natural experiments or those that use mixed methods to demonstrate impact rather than causality. Hence, natural experiments that include mixed methods are a potential solution to this methodological quagmire that exists within contemporary evidence for complex nature-based interventions.
The multiple benefits reported in this scoping review illustrate the breadth of the literature, and highlight the benefits of gardens and gardening on diverse populations. This has wider implications for healthcare practitioners and can offer non-clinical solutions that build on traditional asset-based community approaches. Our findings suggest that socially prescribed referrals to gardens and gardening have the potential to change people’s behaviours and activate well-being. In addressing the wider determinants of health, social prescriptions using nature-based solutions could help improve mental, physical and physiological outcomes, ultimately influencing a potential to minimise inappropriate GP consultations and A&E attendance and improve resilience. As a social prescription, nature-based solutions, such as gardening, provide clinicians with an evidence-based opportunity to promote well-being through non-medical methods.
Conclusions
A strength of our scoping review was its rigorous and systematic approach to locate and understand the breadth of evidence reporting the effects of gardens and gardening on people with LTCs. The scoping review has exposed a myriad of paradigmatic solutions that have been used to capture well-being outcomes. Irrespective of the heterogeneous methods used, our scoping review indicates that gardens and gardening could have a positive dual benefit on a range of mental, social and psychological outcomes, and thus, may be of relevance to those considering gardens and gardening as a non-medical, social prescription. Our logic models could be used as a decision support aid to enable more confident referral to nature-based solutions as part of a wider social prescription.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110110.
Footnotes
Contributors MH, AB, MH, MM made substantial contributions to the conception or design of the work and drafted the work and provided final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. No primary data were used. The search protocol is available on request.