Article Text

Abstract
Objective Because married couples have many environmental influences in common, spouses may develop similar diseases. This study aimed to determine the concordance of hypertension, diabetes and dyslipidaemia, which are major risk factors for cardiovascular disease, among married couples in Japan.
Research design and methods We conducted a cross-sectional study of married couples who were both aged ≥40 years using the 2016 Comprehensive Survey of Living Conditions, which is a Japanese national survey. We first determined the proportions of wives and husbands who were receiving therapy for each of the diseases of interest. We then conducted logistic regression analyses using the wives undergoing therapy for each disease as outcomes and the husbands undergoing therapy for the same disease as the principal exposure, adjusting for covariates.
Results The subjects of the analyses were 86 941 married couples. The wives of male patients were significantly more likely to be receiving therapy for the same disease. Logistic regression revealed that when husbands were undergoing therapy for these diseases their wives had ORs (95% CIs) of 1.79 (1.72–1.86) for hypertension, 1.45 (1.34–1.58) for diabetes, 2.58 (2.41–2.75) for dyslipidaemia and 1.87 (1.80–1.93) for any of these diseases.
Conclusions If men have hypertension, diabetes or dyslipidaemia, their wives were also more susceptible to the same disease. Medical professionals and couples may need to recognise these results and consider couple-based interventions to help the prevention, early detection and treatment of these diseases.
- primary care
- diabetes & endocrinology
- preventive medicine
- public health
- social medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to determine the concordance of major diseases in married couples in Japan, using a nationally representative database.
Our findings suggest that we should target not only the patients in front of us, but also their family members.
It was a cross-sectional study and causal relationships cannot be inferred.
We used the surrogate measure of ‘undergoing therapy’ because there was no information to definitively establish whether the participants had diseases or not.
There was no information about genetic factors.
Introduction
Cardiovascular disease is increasing in prevalence and is now the leading cause of death and disability in both developed and developing countries.1–5 Hypertension, diabetes and dyslipidaemia are major risk factors for cardiovascular disease5 6; therefore, preventing and treating these diseases to reduce the incidence of cardiovascular disease is important for the health of the population and to minimise healthcare costs. Both genetic and environmental factors contribute to the incidence and progression of these diseases, of which the impact of environmental factors is considered to be greater.7
In Japan, the prevalence of hypertension is decreasing because of a reduction in salt intake that is attributable to public health interventions and westernised dietary patterns.8 However, the westernisation of the traditional Japanese diet has also increased the prevalences of obesity, diabetes and dyslipidaemia.8 In 2018, in Japanese women of over 20 years of age, the prevalences of hypertension, diabetes and dyslipidaemia were 26.0%, 9.3% and 21.1%, respectively, while those in Japanese men over 20 years of age were 36.2%, 18.7% and 12.2%, respectively.9 Though Japan has one of the longest-living populations in the world, the control of these chronic diseases is important to further extend both life expectancy and healthy life expectancy.
Married couples have many environmental influences in common. Thus, although there is generally no genetic connection between spouses, they usually live together, share meals and influence each other’s lifestyles, such as the level of drinking and smoking, physical activity and everyday routines.10 11 When one spouse has hypertension, diabetes or dyslipidaemia, the other appears to have a higher risk of developing the same disease, compared with someone whose spouse is unaffected. Therefore, by determining the spousal concordance for these diseases, it may be possible to identify preventable risks that could be reduced by changing habits. If the spousal concordance of these diseases is high, couples-based interventions may help prevent, detect and limit the progression of these diseases.
There have been several previous studies of the spousal concordance of disease,12–20 and it has been posited that the degree of spousal concordance depends on the community being studied.16 In Japan, to the best of our knowledge, no studies have been conducted using nationally representative data regarding the spousal concordance of hypertension, diabetes or dyslipidaemia. In this context, the present study aimed to determine the spousal concordance of hypertension, diabetes and dyslipidaemia, which are major risk factors for cardiovascular disease, in married couples in Japan.
Materials and methods
Data
We conducted a cross-sectional study using ‘household cards’ and ‘health cards’ of the 2016 Comprehensive Survey of Living Conditions (2016 CSLC). The CSLC is a nationally representative survey conducted by the Ministry of Health, Labour, and Welfare (MHLW) to characterise the way of life of households and their members, including the family structure, health status, use of health and long-term care, income and savings.21 The sampling method is based on the enumeration districts (EDs) defined in the census, each of which includes approximately 50 households. For the 2016 CSLC, 5410 EDs were randomly sampled from the EDs in the 2010 census. All households (~290 000) and household members (~740 000) in the selected EDs were surveyed using self-administered questionnaires.
We restricted the present sample to married couples in which both spouses were aged ≥40 years. A married couple was defined as the combination of a male householder and a female spouse or a female householder and a male spouse who were living together. The reason for studying couples of this age is that younger couples are less likely to have the target diseases. We excluded couples with missing values for the variables used in the analysis. Figure 1 shows a flow chart for the sampling procedure.
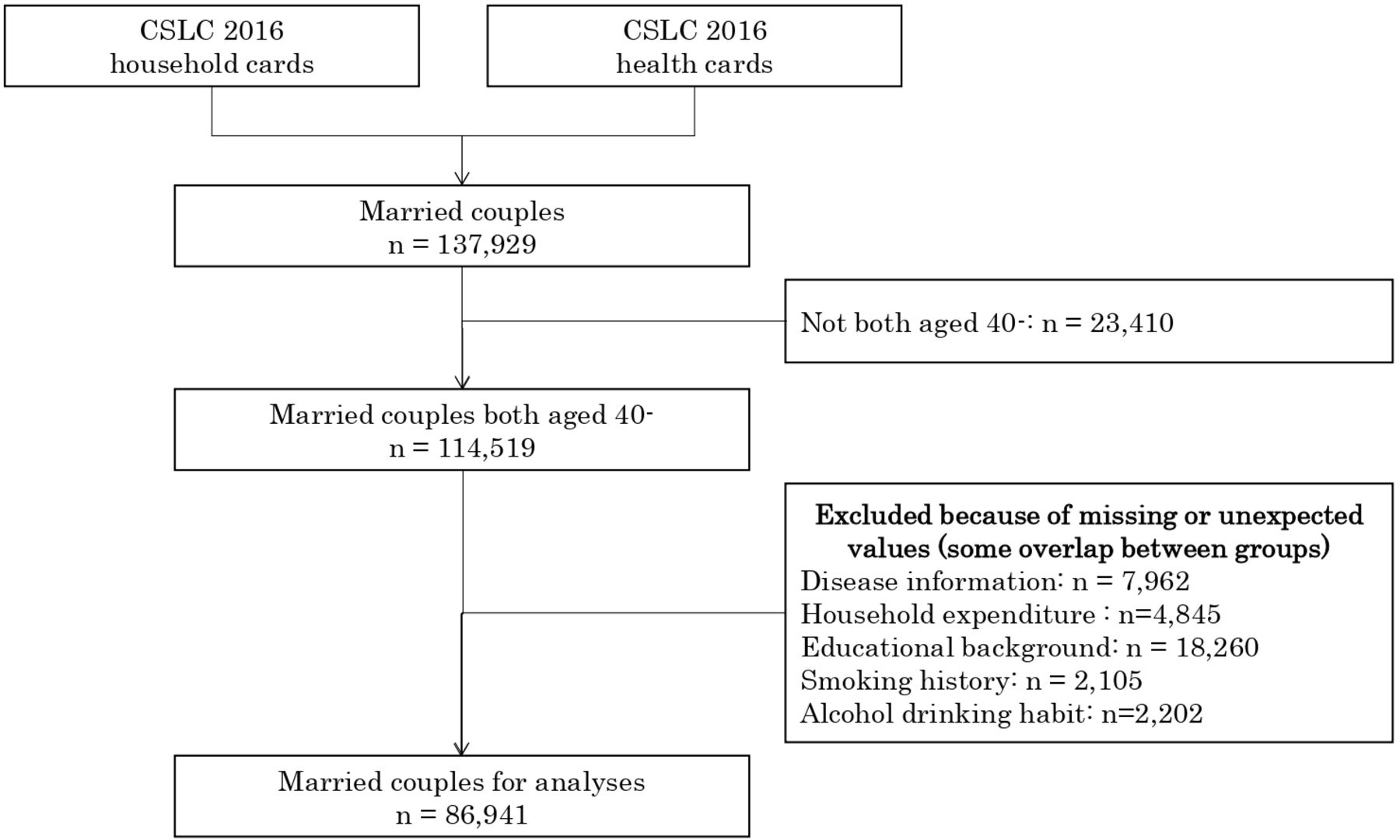
Flow chart describing the sampling process. 2016 CSLC, 2016 Comprehensive Survey of Living Conditions.
Measurements
The outcome variables were the wives undergoing therapy for hypertension, diabetes, dyslipidaemia or any of these diseases. We obtained this information using the questions ‘Are you currently going to a hospital, clinic or treatment facility due to illness or injury?’ and ‘What kind of illness or injury are you going there for?’. The diseases of interest are selected from the viewpoint of being chronic, lifestyle-related and quite prevalent. We must also recognise the difference among the diseases; hypertension and dyslipidaemia can generally be controlled using drugs, whereas lifestyle improvement should be especially weighed in diabetes.
The main exposure was the husbands undergoing therapy for the same disease. The definition of ‘undergoing therapy’ and the identification of the disease were the same as for the outcome variables.
We also obtained information about covariates: the location of the residence of the couple and their household expenditures, as well as the characteristics of the wives: their ages, educational backgrounds, smoking histories and alcohol drinking habits. All of these factors have been found to be associated with undergoing therapy for the target diseases in the previous studies.22–28 The location of residence was classified into a large city, a medium-sized or a small city and the countryside. To describe household expenditure, the logarithm of the total household expenditure in May of the survey year was used. The ages of the wives were categorised as 40–49, 50–59, 60–69, 70–79 or >80 years. Their educational backgrounds were classified into attendance for 4 years at a college, university or graduate school or not. Smoking history was classified into non-smoker, smoker and past smoker. Alcohol-drinking habits were classified into drinking (the equivalent of) a mean of 180 mL or more of Japanese sake per day, or not. In addition, because whether an individual undergoes therapy can be affected by their access to healthcare, the presence or absence of having undergone therapy for another disease and its interaction with age group were also incorporated into the model.
Statistical analyses
We first performed descriptive analyses of the proportion of wives and husbands who were receiving therapy for each disease or any of the diseases. We calculated the proportions of wives who were undergoing therapy, classified according to age group and to the presence or absence of their husbands undergoing therapy for the same disease, and determined the degree of concordance within the couples using the χ2 test.
We then conducted logistic regression analyses using the wives undergoing therapy for each disease as the outcomes and the husbands undergoing therapy for the same disease as the principal exposure. The model included all the covariates described above (location of residence; household expenditure and wife’s age, educational background, smoking history, alcohol drinking habits, the presence or absence of having undergone therapy for another disease and its interactions with age group). Given that smoking or drinking habits may have been largely influenced by the spouse, we also constructed another model that did not include the wife’s smoking history or alcohol drinking habits. In addition, we made adjusted predictions of the proportions of wives who were undergoing therapy, classified according to age group and to the presence or absence of their husbands undergoing therapy for the same disease. In this, if a husband was undergoing therapy, a score of 1 was awarded, and if not, a score of 0 was awarded; mean values were used for the remaining covariates.
In addition, we conducted logistic regression analyses in which a husband undergoing therapy for each disease was used as the outcome and a wife undergoing therapy for the same disease was used as the principal exposure.
Stata was used for all statistical analyses (V.14.1; Stata Corp LP, College Station, Texas, USA). P<0.05 was considered to represent statistical significance. We followed STROBE guidelines for study design and manuscript preparation (research checklist).
Patient and public involvement
No patients were involved in this study. Members of the public were not directly involved in this study.
Results
The participants comprised 86 941 married couples in which both spouses were aged ≥40 years and for which there was no missing data. The proportions of wives and husbands who were undergoing therapy were 17.4% and 23.2%, respectively, for hypertension, 5.0% and 10.3%, respectively, for diabetes, 9.7% and 7.2%, respectively, for dyslipidaemia and 25.7% and 32.5%, respectively, for any of these diseases. The concordance within the couples (the proportion of couples in which both or neither spouse was undergoing therapy) was 73.2% for hypertension, 86.5% for diabetes, 86.5% for dyslipidaemia and 67.5% for any of these diseases (table 1). In all the age groups and for all the diseases, wives whose husbands were undergoing therapy showed a significant tendency to have the same disease (figure 2). The degree of divergence varied according to age group and the disease concerned, but overall, divergence was more likely among older age couples and with respect to hypertension or dyslipidaemia, rather than diabetes.
Proportion of wives and husbands undergoing therapy for hypertension, diabetes, dyslipidaemia or any of these diseases, among 86 941 married couples
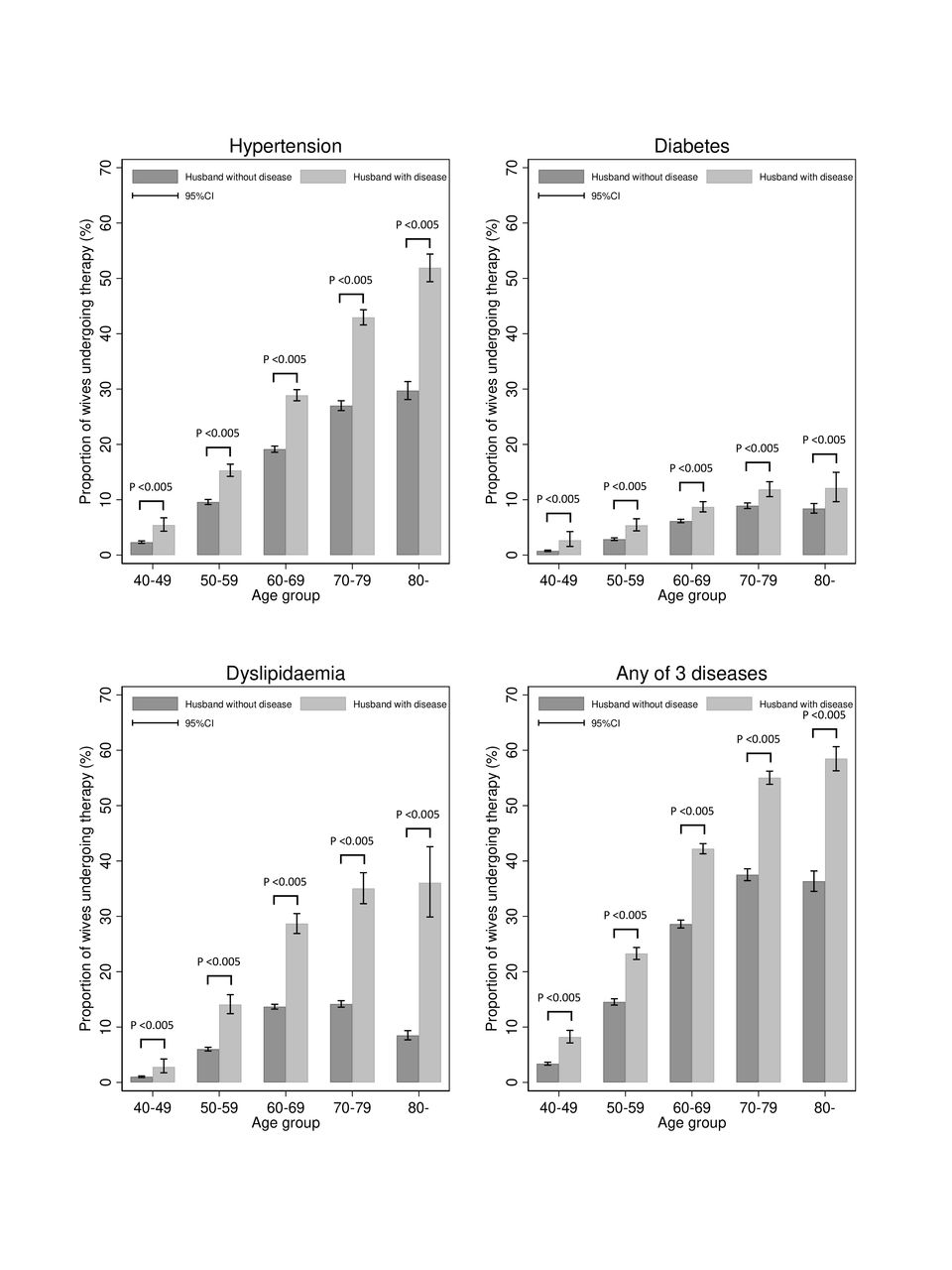
Proportion of wives undergoing therapy, classified according to age group and the presence or absence of their husbands undergoing therapy for the same disease n=86 941. P values were calculated using the χ2 test to determine the degree of concordance of each disease within the couples.
The logistic regression model revealed that when husbands were undergoing therapy, their wives were more likely to be undergoing similar therapy, with ORs (95% CIs) of 1.79 (1.72–1.86) for hypertension, 1.45 (1.34–1.58) for diabetes, 2.58 (2.41–2.75) for dyslipidaemia and 1.87 (1.80–1.93) for any of these diseases (table 2). Adjusted predictions for the proportions of wives who were undergoing therapy, classified according to age group and the presence or absence of their husbands undergoing therapy for the same disease, and calculated using the described covariates (the variables used in the logistic regression model other than age group), are shown in figure 3 (adjusted from the corresponding data in figure 2). After adjusting for these covariates, the differences between the proportions of wives undergoing therapy, according to the presence or absence of their husbands undergoing therapy, decreased slightly in magnitude. The characteristics of the wives, classified according to whether their husbands were undergoing therapy for each disease, are shown in online supplementary table 1. The logistic regression model that did not include the wife’s smoking history or alcohol drinking habits yielded very similar results (online supplementary table 2).
Supplemental material
Supplemental material
Relationships between wives undergoing therapy for hypertension, diabetes, dyslipidaemia or any of these diseases, and their husbands undergoing therapy for the same disease

{kind=link}
{kind=link}
{kind=link}
Adjusted predictions for the proportion of wives undergoing therapy, classified according to age group and the presence or absence of their husbands undergoing therapy for the same disease. Adjusted for the location of residence; household expenditure and the wife’s educational background, smoking history, alcohol drinking habits and the presence or absence of having undergone therapy for another disease. P values were calculated using logistic regression, including the above variables, to determine the degree of concordance of each disease within the couples.
Adjusted for the location of residence; household expenditure and the wife’s age, educational background, smoking history, alcohol drinking habits, the presence or absence of having undergone therapy for another disease and its interaction with the age group.
The outcomes of logistic regression analyses using a husband undergoing therapy for each disease are shown in online supplementary table 3. The results were similar to those in which a wife undergoing therapy for the same disease was used as the outcome (table 2).
Supplemental material
Discussion
The results of the present study suggest that if men have hypertension, diabetes or dyslipidaemia, their wives are also susceptible to the same disease. The non-adjusted results (figure 2) show that the wives of male patients are likely to have the same disease. Therefore, medical professionals may need to consider not only the health of the relatives of an individual with one of these diseases, but also of their spouse. Health promotion and disease prevention, in the form of consultation or treatment, should involve obtaining information about a spouse and/or considering couples together. Furthermore, the recognition that patients and their spouses share the risk of diseases may encourage them to have medical check-ups and to improve their lifestyles, in terms of diet and/or exercise, together. However, whereas the recognition of the importance of couples or family-based interventions for chronic diseases is increasing, the main purpose of current procedures is the optimisation of individual patient therapy,29–32 and there have been few attempts to improve the health of couples or family units together. Additionally, regular screening may be recommended for the spouses of patients with these diseases, just as this would be recommended for the family members of individuals with an inherited predisposition to a form of cancer.33 34 Because these diseases and the cardiovascular disease they predispose towards place a serious financial burden on society,35 it would be beneficial for governments and insurers to help prevent the onset and progression of diseases by using this approach.
Logistic regression analyses showed that a husband undergoing therapy was associated with a greater likelihood that their wife would also be undergoing therapy for one of these diseases, and vice versa. Whether smoking and drinking habits were included as covariates did not have a great impact on the OR for the principal outcome. Therefore, we consider that the concordance within married couples with regard to these diseases is due to other lifestyle factors, especially dietary factors, such as westernised diet and salt intake, which are major risk factors for these diseases in Japan. The present findings are very similar to those of the previous studies conducted in other countries with regard to diabetes and hypertension risk.12–18 However, for dyslipidaemia, we have identified a much higher level of concordance than has been identified in the previous studies.12 14 Further research is needed to ascertain whether this can be explained by differences between the study populations or by other factors, such as the limitations discussed below. Additionally, some cohort studies conducted in the Middle East have generated different results: having a wife with diabetes did not significantly increase her husband’s risk of diabetes,19 and having a spouse with hypertension did not increase the risk of hypertension.20 The establishment of a cohort study in Japan would allow us to evaluate this issue in more detail.
There were a few limitations in this study. first, because this was a cross-sectional study, causal relationships cannot be inferred. Thus, we cannot know whether the fact of a husband having a disease is caused by his wife having the same disease, or vice versa. For the same reason, although several theories have been proposed to explain spousal concordance, such as assortative mating and convergence in behaviour and lifestyle,11 it is also difficult to determine the most important factors. To reduce the impact of these limitations, an appropriate cohort study should be conducted.19 20 Second, because there was no information about each case that allowed us to definitively establish whether the participants had diseases or not, we used the surrogate measure of ‘undergoing therapy’. Because patients could only undergo therapy if they had access to medical facilities, we included the presence or absence of a participant having undergone therapy for other diseases and its interaction with age group as covariates in the logistic regression analyses, to attempt to control for this variable. However, there remains the possibility that if the husband were undergoing therapy, this might lead to a similar outcome for his wife, for example, if a man had a certain disease and was being treated, his wife might go to see a doctor because she was worried that she might also have the same disease, which would increase the overall probability of diagnosis. Therefore, concordance may have been slightly overestimated compared with the use of clinical data as outcomes. The recent increase in prescriptions for antidyslipidaemic medication and the likelihood that relevant information will be passed between spouses may at least partially explain the high concordance of dyslipidaemia identified. Finally, there was no information about genetic factors. Further interesting studies may be possible if information about genetic factors is available and the interaction between genetic and environmental factors is examined.
Nevertheless, this is the first study to determine the concordance of major diseases in married couples in Japan, using a nationally representative database, and we consider the results to be of great significance for medical professionals and couples. In conclusion, our findings suggest that for the prevention, early detection and to stop the deterioration of disease, healthcare professionals should target not only persons with these chronic diseases, but also their family members.
Acknowledgments
We would like to thank the members of the Department of Health Services Research, University of Tsukuba. We also thank Mark Cleasby, PhD, from Edanz Group (https://en-author-services.edanzgroup.com/) for editing drafts of this manuscript.
References
Footnotes
Contributors TW designed the study, analysed data and wrote the initial draft of the manuscript. TS contributed to analysis and interpretation of data, and assisted in the preparation of the manuscript. HT, HN and NT have contributed to data collection and interpretation, and critically reviewed the manuscript. All authors approved the final version of the manuscript, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was supported by a grant-in-aid from the Ministry of Health, Labor and Welfare; Health and Labor Sciences Research Grant, Japan (H28-junkankitou-ippan-009, H30-choju-ippan-007).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study approved by the Research Ethics Committee of the University of Tsukuba (Nos. 1165, 1324).
Provenance and peer review Not commissioned; externally peer reviewed.