Article Text

Abstract
Objectives To assess the effectiveness of radiofrequency denervation (RD) of lumbosacral anatomical targets for the management of chronic back pain.
Design Systematic review and meta-analysis of randomised controlled trials (RCTs).
Methods A database search (Medline, Medline in Process, Embase, CINHAL and the Cochrane library) was conducted from January 2014 to April 2019 for placebo or no-treatment controlled trials of RD for the management of chronic back pain. Included trials were quality assessed using the Cochrane Risk-of-Bias Tool and the quality of outcomes assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. Meta-analysis was conducted to calculate mean difference (MD) in post-treatment Pain Score.
Results Nineteen RCTs were included in the review. There appears to be short-term pain relief (1–3 months) provided by RD of the sacroiliac joint (five trials, MD −1.53, CI −2.62 to 0.45) and intervertebral discs (four trials, MD −0.98, CI −1.84 to 0.12), but the placebo effect is large and additional intervention effect size is small (<1 on an 11 point (0–10) Pain Scale). Longer-term effectiveness (>6 months) is uncertain.
Conclusions RD of selected lumbosacral targets appears to have a small, short-term, positive effect for the management of patients with chronic back pain. However, the quality of evidence for the majority of outcomes is low or very low quality and there is still a degree of uncertainty, particularly around the duration of effect.
- back pain
- rheumatology
- neurology
- pain management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This review brings together a number of recent trials with earlier trials so that there is a sizeable sum of evidence on which to assess the effectiveness of radiofrequency denervation (RD) for back pain.
Due to the invasive nature of the procedure, it is difficult to perform truly patient or provider-blinded trials and this brings some uncertainty around findings.
There is limited reporting of long-term outcomes (>6 months) for the effectiveness of RD.
Introduction
Back pain is an extremely common symptom experienced by people of all ages, and can be attributed to a wide variety of disease processes.1 2 Low back pain is now the leading cause of disability worldwide and back pain is associated with a substantial economic burden, with high medical and societal costs.3 Studies have shown that a large proportion of medical costs come from hospital admissions and physical therapy for the management of back pain.4 However, there are also indirect costs associated with chronic or recurrent back pain that are difficult to quantify relating to work absenteeism and related productivity.1 3 4 In many cases, back pain is non-specific, or structural pathology amenable to surgical correction cannot be identified.5–7 Hence, patients and practitioners continue to seek non-surgical alternatives for the management of back pain.
Radiofrequency denervation (RD) involves the application of an alternating electric current (250–500 kHz) via a needle probe to induce a highly localised rise in tissue temperature at the needle tip.8 The needle tip is usually placed under fluoroscopic guidance to enable selective ablation of sensory nerve branches that supply facet joints, sacroiliac joint or other structures that comprise the lumbosacral spine. RD would, therefore, offer relief of pain by attenuating sensory signals from the lumbosacral spine.9
Despite its use for over 20 years,10 the effectiveness of RD targeted at the anatomy of the lumbosacral spine is not yet established, with randomised controlled trials (RCTs) continuing to be performed. A number of trials have been published since the publication of the last high-quality review in 201511 and our systematic review aimed to bring together this evidence in an attempt to evaluate whether RD is an effective intervention for the management of chronic non-specific back pain.
Materials and methods
Search strategy
A search was conducted in Medline, Medline in Process, Embase, CINHAL and the Cochrane library from January 2014 to April 2019 (online supplementary appendix 1). Previous systematic reviews were used to obtain additional relevant studies published before 2014.
Supplemental material
Inclusion criteria
RCTs comparing RD of the spine with a control in patients with back pain with or without sciatica were included. Only trials of radiofrequency procedures for the purpose of ablating or denaturing sensory nerve branches or nociceptors that supply the lumbosacral spine were considered for inclusion. Trials of pulsed Radiofrequency (RF),12 or other forms of ‘neuromodulatory’ procedures that do not aim to ablate or denature these targets, were excluded from the review. Control groups where there was no active treatment were considered for inclusion but trials with potentially effective comparators, for example, corticosteroid injections, were excluded. Only trials of patients with back pain without a definite or surgically remediable cause (chronic non-specific back pain) were included in the review. The outcome for the review was patient-reported Pain Score, for example, Visual Analogue Scale or Numeric Rating Scale.
Data collection and quality assessment
Trial characteristics were recorded from included studies. Study results were extracted independently by two authors (MEC and PT), with any disagreements resolved by consensus. The overall strength of evidence was assessed using the GRADE approach.13 Risk of bias was assed using the Cochrane Risk-of-Bias Tool.14 Any outcome where more than half of trials were considered to have a high or unclear risk of bias was downgraded. Outcomes were also downgraded where heterogeneity in the meta-analysis was greater than 50%. Optimal sample size was taken to be 85 participants per study arm (as calculated in the Juch et al trial)15 and studies with less than 170 participants, and/or where the 95% CIs included the line of no effect, were downgraded for imprecision. Publication bias was assessed using funnel plots and outcomes downgraded where there was a high certainty of publication bias.
Data analysis
Meta-analyses were conducted in RevMan16 with random effects models since the included studies investigated effectiveness in different population groups with varying intervention and control group treatments. Pain Score at 1–3 months was taken as the primary outcome (longest time point used for studies reporting multiple time points), allowing outcome from a larger number of studies to be combined. Pain Score data were reported on a 0–10-point scale (Visual Analogue Scale or Numeric Rating Scale) in all studies and the mean difference (MD) was, therefore, calculated without standardisation as done in the previous Cochrane review.11 Studies with different spinal targets, for example, facet joints, sacroiliac joints or intervertebral disc, were separated in the analysis. A sensitivity analysis was conducted to check the validity of findings by removing studies considered to have a particularly high risk of bias. Subgroup analysis to explore study heterogeneity was not conducted because of the small number of studies and high likelihood of reaching spurious conclusions.
Results
Study characteristics
The search identified 922 citations of which 229 were duplicates. Studies were excluded as shown in figure 1. Of the 693 citations reviewed, 8 new trials were identified as well as 11 from a previous Cochrane review.11 Exclusions were made as shown in figure 1. Nineteen trials were included in the review and their characteristics are shown in online supplementary appendix 2. Trials investigated the effectiveness of RD of the facet joint (supplied by medial branch of the dorsal spinal ramus),15 17–24 the sacroiliac joints,15 25–28 the intervertebral discs29–33 or vertebral end plate (supplied by the basivertebral nerve).34 The majority of trials used a sham-control group but one large trial compared RD with no treatment (both groups received an exercise programme) and one small trial compared RD plus conventional medical with conventional medical management alone (including self-care, medications and physical and cognitive therapy).
Supplemental material

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Study quality
Sham-controlled trials generally appear to have conducted adequate randomisation but allocation concealment was often unclear. Processes were in place to blind patients and providers and outcome assessors. In some trials, maintenance of blinding was unclear as it was evident that patients undergoing sham procedures were offered RD in case of sham treatment failure. In these cases, blinding would have been broken. Most trials did not report dropouts and there was unclear risk of attrition bias. The outcome for this review was Pain Score and this was reported in all trials and reporting bias was not considered to be an issue in the review. Four trials were identified as having high risk of bias and were removed in the sensitivity analysis.17 19 24 25
Overall quality of the evidence
The majority of outcomes were graded down for imprecision and all outcomes were downgraded for potential risk of bias. Consequently, almost all outcomes were graded as low quality. However, in some cases, high heterogeneity was also present and these outcomes were graded as very low quality. Publication bias was suggested by asymmetry in a number of the funnel plots. However, there was uncertainty due to the small numbers of studies and outcomes were not graded down for publication bias.
Study findings
The results of the meta-analyses are shown in table 1.
Results of the meta-analyses of randomised controlled trials
RD of the facet joints
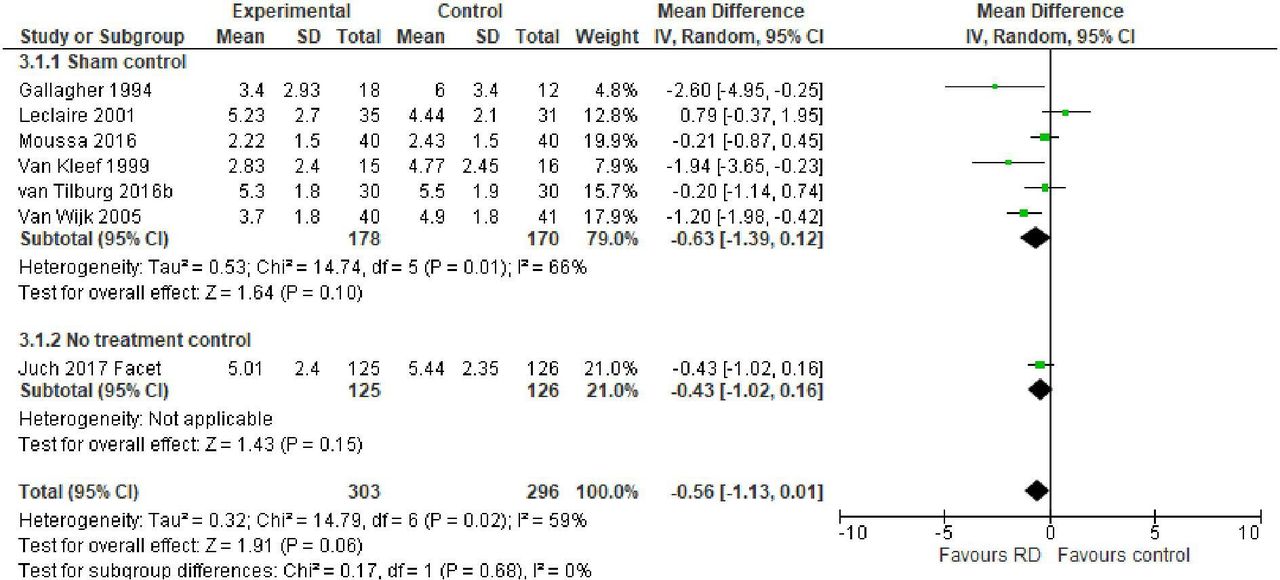
Meta-analysis of Pain Scores at 1–3 months post procedure (longest time point used for studies with multiple time points) (marked on a 0–10 scale) is shown in figure 2 and table 1. The effect size was similar when all trials were included (seven trials, MD −0.56, CI −1.13 to 0.01) or where just the sham-controlled trials were included (six trials, MD −0.63, CI −1.39 to 0.12) but the effect was not significant for either. We also considered outcomes at 6 and 12 months, where data were available to explore longer term outcomes, but did not find any significant effect (table 1).

Post-treatment Pain Score for radiofrequency denervation of the facet joints versus control at 1–3-month follow-up (longest time point used for studies with multiple time points).
RD of the sacroiliac joints
Figure 3 shows the meta-analysis of trials for Pain Score at 1–3 months (longest time point used for studies with multiple time points). There was a significant effect of RD for the analysis including all trials (five trials, MD −1.53, CI −2.62 to 0.45) or just sham-controlled trials (four trials, MD −1.89, CI −3.45 to 0.34). Only one trial15 assessed outcome at later time points and this showed no significant difference compared with a no-treatment control (table 1).

Post-treatment Pain Score for radiofrequency denervation of the sacroiliac joints versus control at 1–3-month follow-up (longest time point used for studies with multiple time points).
RD of the intervertebral discs
Pain Score at 1–3 months post treatment was significantly lower for RD compared with control in all trials (four trials, MD −0.98, CI −1.84 to 0.12) but not for sham-controlled trials alone (three trials, MD −0.63, CI −1.36 to 0.10) (figure 4). Pain Score was significantly lower for RD when all trials and sham-controlled trials were considered at 6 months but, for one trial assessing outcome at 1 year, it was not (table 1).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Post-treatment Pain Score for radiofrequency denervation of the intervertebral discs versus control at 1–3-month follow-up (longest time point used for studies with multiple time points).
Sensitivity analysis
Four studies were removed in the sensitivity analysis due to a high risk of methodological bias17 19 24 25 and the two non-sham-controlled trials were also removed.15 32 After the removal of these trials, outcome at 1–3 months for facet joint sham trials was still not significant (four trials, MD −0.57, CI −1.60 to 0.46) and 1–3 month outcome for sacroiliac sham trials became non-significant (three trials, MD −1.21, CI −2.59 to 0.16). The facet joint sham trial outcome at 6 months also became non-significant (one trial, MD 0.18, CI −2.80 to 3.16).
Discussion
Main findings
This systematic review presents evidence suggesting that RD of the lumbosacral spine may have a small positive but short-lived effect in patients with chronic back pain, depending on the precise part of the anatomy that is being targeted by the procedure. The quality of evidence for the majority of findings is low or very low quality and there is still a degree of uncertainty around this assertion, particularly around the duration of effect. The size of benefit appears to be small (<1 point on a 0–10 Pain Scale) and there are limited data for outcomes beyond 6 months. These assertions apply to RD for sacroiliac joints, whereas evidence for benefit to other targets is more limited. RD for facet joints did not show a significant benefit on 1–3-month outcome. There is a suggestion that there may be a benefit of RD for intervertebral discs but there is some inconsistency, with insignificant effect for short-term outcomes.
What is also clear from the review is that both treatment and sham/no-treatment groups improved during the trials. In the sham-controlled trials, this may, in part, be due to placebo effect. However, the large trial by Juch et al15 used a ‘no additional treatment’ control (both groups received an exercise programme) but all study arms improved over time. This may be because a high proportion of control study participants actually received RD (~30%) due to crossover during the trial. However, this may also be explained by self-selection of participants who volunteer for research trials,35 and hence are likely to make more of an active effort to manage their back pain. Such participants may be more likely to engage with, and be diligent in, exercise programmes and seek medical assistance where needed.
In the trial by Juch et al, control group improvements may also be explained by the conservative management that they received. The exercise programme employed was multidisciplinary and comprised individual sessions over 8–12 hours focused on quality of movement and behaviour, with access to psychological care. There is evidence suggesting that patients with chronic back pain can benefit from pain management programmes that are of sufficient quality and duration.36 Where patients have not received an adequate trial of conservative therapy, they may benefit from further exercise programmes and other conservative management. It remains unclear whether patients who are either unable or unwilling to engage with conservative approaches to pain management would benefit from RD-based interventions as a first-line or isolated modality of treatment. Hence, there should be some reservation when considering the use of RD treatment as a first-line or isolated modality of pain management.
Regression to the mean may also have played a role in control group improvements since patients in the trial were recruited with elevated pain, responsive to an anaesthetic block. Back pain has been shown to have a varied aetiology, with some patients experiencing fluctuating levels of pain over time, while other experience constant high levels of pain.37 38 For the majority of trials that reported it, duration of back pain in participants prior to enrolment was 2–5 years and a proportion of these was likely to have had high levels of constant pain. Some, however, may have been experiencing fluctuating or recurrent pain within this period since the actual inclusion criteria for most trials was pain for >3 or 6 months based on patient recall. If they were recruited at a point where their pain had flared acutely, there would be a natural tendency for that painful episode to resolve over time.
Strengths and limitations
A major strength of this review is that it collates a larger body of evidence than previous systematic reviews, with the addition of a number of recent trials and thorough assessment of the quality of the evidence. The review is able to tentatively answer the question about the effectiveness of RD for back pain; an assertion that, to date, has proved to be very difficult due a paucity of evidence in this field.
This review uses evidence from a previous Cochrane review11 but the inclusion criteria for our review had a narrower scope (included only sham-controlled trials or conservative management-controlled trials of conventional neuroablative RD). Since the previous review appears to be of high quality, and we updated it with a thorough search of the literature to date, there is assurance that all relevant trials were included.
A limitation of this review is that it was difficult to truly assess risk of bias in trials included in the review. Trial integrity rested heavily on the blinding of participants and the outcome was likely to be highly subject to patients’ preconceptions of the different interventions given. Most trials did not report information that providers gave to the patients about the different possible treatment arms, for example, did providers suggest to patients that RD was the effective treatment and that sham or no treatment would be ineffective? Where blinding was broken, these viewpoints may have influenced patients’ response. In some of the sham-controlled studies, this was clearly evident. For example, in some studies, before randomisation, patients were told that, if randomised to sham, they could receive RD if they gained no benefit. Where blinding was broken, these opinions were likely to influence patients’ perception of their pain. In other studies, information from providers was not reported and it is difficult to assess whether this type of bias occurred.
The review may also be limited in its ability to ascertain the technical quality of individual research trials. Even when examining the reported trial methodology, it is difficult to conclusively identify trials that employed procedures that may be more or less successful in denervating the specific lumbosacral anatomy. Some aspects of RD procedures in earlier trials are considered outdated39 40 but the advantages of more recent procedures for RD remain unproven, and there is no clear evidence of their superiority. Sensitivity analysis based on technical quality was, therefore, considered unhelpful and not performed.
The review is also limited by the lack of long-term data from trials. Most studies do not attempt to blind patients for more than 3 months and the longer follow-up outcomes are considered to be at higher risk of bias. It is still, therefore, unclear whether RD of lumbosacral anatomy has long-term benefits for back pain.
Finally, the review is limited in its ability to identify any aspects of patient or intervention characteristics that may make RD treatment more likely to be beneficial. There is, to date, no reliable predictor of benefit on back pain for RD procedures based on clinical or imaging findings or diagnostic injections.41 The relative advantages of different RD technologies used in included trials (eg, ‘cooled’25 26 32 and ‘bipolar’30 32 RD) remain to be established. Due to the small number of studies at each time point, subgroup analysis was not considered appropriate. However, the publication of more sham-controlled trials and trials comparing different RD technologies may make this type of investigation possible. Technical advances and advances in knowledge and experience may allow for better selection of anatomical targets and patients for RD, and hence improve clinical outcomes. It is important that these developments are formally assessed and published.
In conclusion, within the limitations in this review and the published literature, there appears to be at least short-term benefit from RD of selected lumbosacral anatomical targets for chronic back pain. However, the mean size of effect appears to be small and, overall, clinical significance may be marginal. Hence, chronic back pain remains a highly challenging condition to treat.
Acknowledgments
Thanks to Julie Aikens and Kerry Herbert at Hinchingbrooke Healthcare Library for their assistance in designing and running the search strategies for the review.
References
Footnotes
Contributors MEC contributed to the planning of this work, selected articles for inclusion, extracted data, quality assessed studies and drafted and redrafted the manuscript. RL contributed to the planning of this work, reviewed the manuscript and approved the final version. PT extracted data from the trials, reviewed the manuscript and approved the final version. MA contributed to the planning of this work, reviewed the manuscript and approved the final version. ML contributed to the planning of this work, reviewed the manuscript and approved the final version.
Funding RL is supported by the Medical Research Council (MC_UU_12015/2). ML is supported by AABGI Foundation project grant (RCZB/071).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article or uploaded as supplementary information.