Article Text

Abstract
Objective The Strategic Regional Plan of the Cree Board of Health and Social Services of James Bay (CBHSSJB), serving the Quebec Cree communities, mandates the objective of integrating oral health within primary healthcare. Emerging evidence suggests that the integration of oral health into primary healthcare can decrease oral health disparities. This research study aimed to answer the following research question: how and to what extent does the integration of oral health into primary healthcare address the oral health needs of the Cree communities?
Design We used a multiple-case study design within a qualitative approach and developmental evaluation methodology. The Discovery, Dream, Design and Destiny model of appreciative inquiry was selected as a study framework among existing frameworks of the developmental evaluation.
Setting Four purposefully selected Cree communities.
Participants Healthcare providers, administrators and patients at the community wellness centres and hospital.
Outcome measures Integration of oral health into primary healthcare.
Results A total of 36 interviews and 6 focus group discussions were conducted. We identified ten themes in discovery and dream phases. The Discovery phase identified the strengths of the organisation in facilitating enablers of integration including strategic planning, organisational structure, cultural integration, coordinated networks and colocation. In the Dream phase, participants’ oral healthcare stories expressed various dimensions of integration and their wish for strengthening integration via extending public oral healthcare programmes, increasing resources and improving organisational management. In the Design phase, recommendations were formulated for a future action plan within the CBHSSJB.
Conclusion This study results suggested that the CBHSSJB has been successful in implementing oral health integration into primary care following its strategic planning. At present, the organisation could extend the level of integration into full integration by following study recommendations derived from the perspective of local stakeholders.
- primary care
- public health
- qualitative research
- health services administration and management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Appreciative inquiry is, for the first time, used in the field of indigenous oral health research that allows better recognition of Indigenous culture and values in organisational health services.
The multiple-case study design helped to gain insight into the integration of dental services into primary healthcare services in Cree communities and enabled the Indigenous participants to enunciate their experiences from a holistic perspective.
The trustworthiness of the study was ensured through member checking and triangulation of multiple methods, data sources and investigators.
This evaluation research could be instrumental in developing evidence on optimal implementation of integrated primary oral healthcare model in other similar communities/settings.
This study might have encountered bias due to various types of study participants such as administrators, healthcare providers and patients.
Introduction
Indigenous communities experience a substantially greater extent of oral health disparities than the general population.1–4 These disparities are associated with a broad range of social determinants at proximal (such as health and oral health behaviour, education, income), intermediate (health and oral healthcare systems, educational system, cultural continuity) and distal (colonialism, racism and social exclusion) levels.5 The oral health disparities within this complex intersection and interrelation of health determinants need to be broadly tackled by system-focused collaborative approaches such as an integrated care approach.6 Therefore, the integration of oral healthcare within primary health has been proposed as a strategy for addressing oral health disparities.7 8
Integrated care is defined as ‘a coherent and coordinated set of services which are planned, managed and delivered to individual service users across a range of organisations and by a range of cooperating professionals and informal carers’.9 Primary oral healthcare (POHC) is defined as ‘the integration of services that promote and preserve oral health, prevent oral disease, injury and dysfunction and provide a regular source of care for acute and chronic oral diseases and disabilities’.10
The Cree Board of Health and Social Services of James Bay (CBHSSJB), as a pioneer in the Canadian province of Quebec, implemented a model for the integrated delivery of health and social services that includes primary oral healthcare.11 12 This organisation is responsible for providing health and social services to the Crees of Northern Quebec.11 ‘Eeyou Istchee’ (the land of the people) is the homeland of the Crees of Northern Quebec who live in nine communities with a total population of over 18 000.13 The CBHSSJB’s Strategic Regional Plans 2004–2014 and 2016–2021 mandated a model for the integrated delivery of health and social services in the Cree communities. Henceforth, the integration of oral health within primary healthcare was one of the specific objectives of this strategic planning.11 14
Available evidence indicates the gap in knowledge about integrated oral healthcare programmes and their outcomes and supports performing evaluation research to create evidence-based data on this topic.15 Therefore, this study was conducted in collaboration with the CBHSSJB to evaluate its integrated POHC programme.
The research question was: how and to what extent does the integration of oral health into primary care address the oral health needs of the Cree communities? Based on an appreciative inquiry (AI) approach,16 the study objectives were to (1) Discover the strengths of the CBHSSJB’s oral healthcare policies in the integration of services; (2) Explore the Cree communities’ members’ oral-health experiences and their dreams for oral care services and (3) Develop recommendations to support planned actions within the communities.
Methods
The study is part of a larger Canadian Institutes of Health Research funded project on Oral Health Integration into Primary Care.17 We followed the Standards for Reporting Qualitative Research guideline for reporting qualitative studies for writing this manuscript.18 This study was performed in compliance with the ethical guidelines of Ownership, Control, Access and Possession for First Nations.19
Study setting
We purposefully selected four Cree communities based on the identification of diverse characteristics such as demography, geography, culture and oral healthcare. Each of the nine Cree communities has a Community Miyupimaatisiiun (wellness) Centre (CMC).20 21 These centres offer a wide variety of health services including dentistry.20 21 The CHBSSJB also operates one regional hospital, a regional public health department, homes for troubled youths, Cree Patient Services (Wiichihiituwin) liaison offices as well as human resources recruitment office.21
Study design
We used a multiple-case study design within a qualitative approach and developmental evaluation methodology.22 23 A case study is the most common design used in evaluation research that helps in examining contemporary phenomena in real-life situations.22 Developmental evaluation is useful in adapting an intervention under complex conditions such as health system issues in culturally diverse contexts, where influences from multiple factors make it difficult to anticipate what will happen as the intervention progresses.23 24
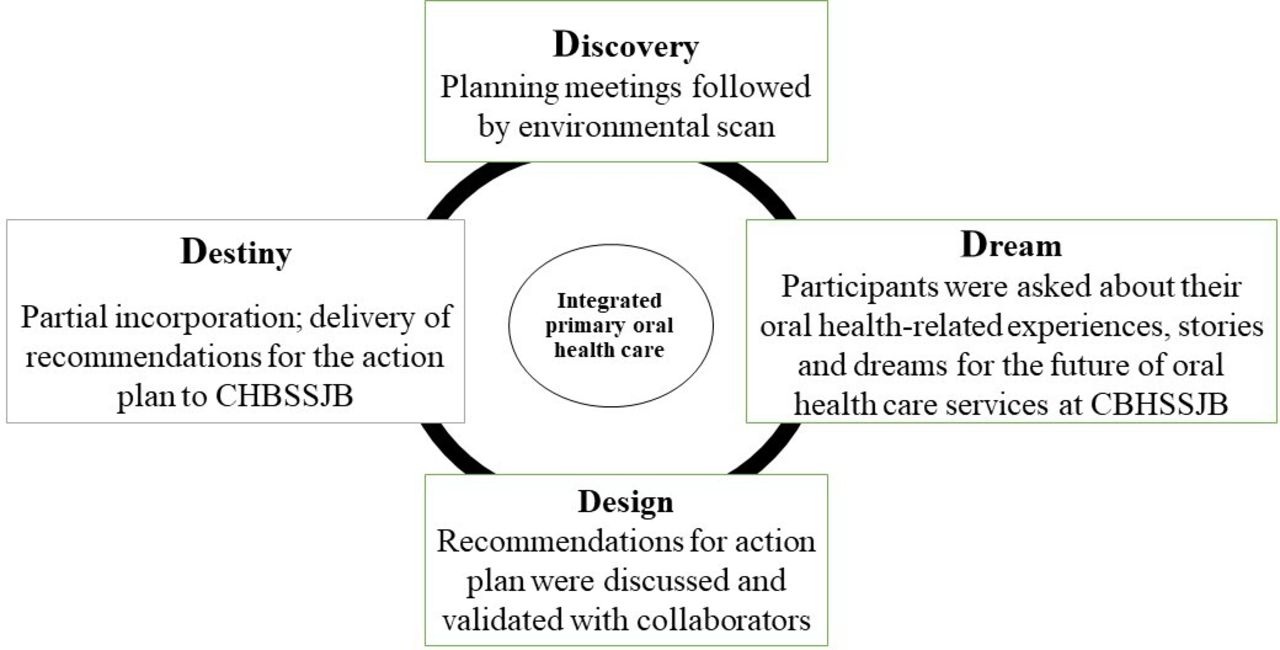
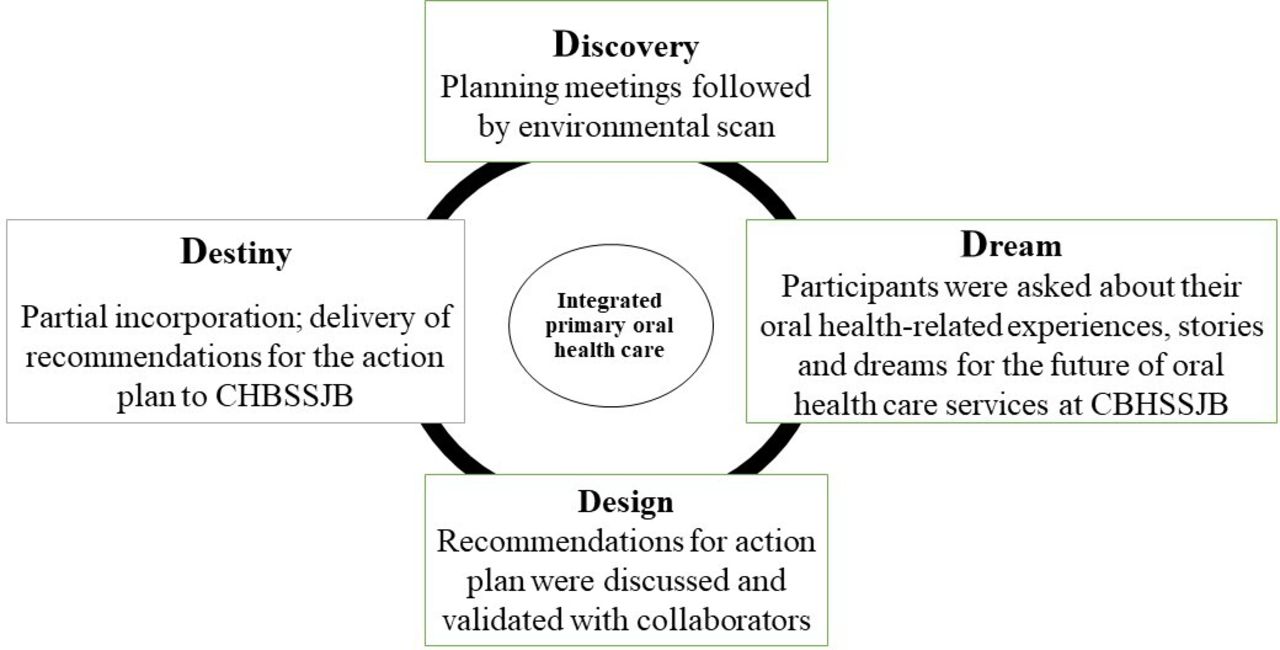
Among various frameworks of developmental evaluation, we selected AI. AI is a philosophical, cooperative and systematic approach for transformational change that searches for ‘what gives life’ to the organisation, recognises the best in individuals, organisations and the world around them to create a better future.25 26 We selected AI because it is a success focused, culturally responsive and cost-effective framework that encompasses the diverse perspectives and experiences of the stakeholders.27 The four phases of AI’s Discovery, Dream, Design and Destiny model guided this project as illustrated in figure 1.16
{kind=link}
Study phases as per AI’s 4 D model. AI, appreciative inquiry; CBHSSJB, Cree Board of Health and Social Services of James Bay; 4 D, Discovery, Dream, Design and Destiny.
Study phases
Discovery
This phase included planning meetings followed by an environmental scan. The planning meetings were conducted in the form of a workshop and videoconference that involved several activities such as presentations, focus group discussions (FGD) and interviews.12 They engaged representatives of Cree community members, health and oral healthcare service providers and administrators to solicit their feedback and to facilitate the development of agreement and community consensus on the project evaluation plan.16 Various evaluation models were also discussed with these stakeholders, and they selected the Five foundations of integrated care28 as a model for this project evaluation.
The planning meetings were followed by an environmental scan. It comprised observations of four CMCs and a documentation review. The documents were obtained from identified key collaborators and the CBHSSJB website. The environmental scan helped in retrieving background information and clarifying purposes, rationale, historical insight and the most recent information related to the oral health policies at the CBHSSJB.29
Dream
Key stakeholders such as administrators, health and oral healthcare providers and patients at the community Miyupimaatisiiun centres and hospital were asked about their oral health-related experiences, stories and dreams for the future of oral healthcare services at the CBHSSJB during FGD and individual interviews.16
Design
This phase involved formulating recommendations for deploying the ‘dreamed’ oral healthcare at CBHSSJB.16 The results and recommendations realised through the previous phases were discussed and validated for the stakeholders’ review, acceptance and confirmation during various CHBSSJB official meetings and precisely planned meetings.
Destiny
This phase was partially incorporated since it included the delivery of recommendations for the action plan to the CBHSSJB in the form of lay and scientific reports.
Sampling and data collection
Maximum variation sampling and snowball techniques were used to identify and recruit participants for data collection.30 Cree community partners at CBHSSJB helped in selecting potential participants, including administrators, care providers and patients. The maximum variation sampling allowed the emergence of diverse viewpoints. Through snowball sampling, selected participants recommended other potential candidates for the study.30 The data collection included the environmental scan, FGD and individual in-depth interviews. FGD and individual interviews were conducted in English or French by two research team members trained in qualitative methods. Data collection continued until saturation was achieved.30 The semistructured interview guide was developed based on the Rainbow model of integrated care and AI, which was tailored based on the participants’ profiles (online supplementary file 1).27 31 Accordingly, based on the Rainbow model, we included questions on each dimension of integration, and based on AI, we involved questions focusing on successful processes and outcomes of integration.27 31 The interviews, on average 40 min in length, and FGD, on average 1 hour and 15 min in length, were conducted between January 2016 and December 2017 in a quiet room at the Miyupimaatisiiun centres or hospital. They were digitally recorded and transcribed verbatim as text documents.
Supplemental material
Data analysis
The study used the community as the unit of analysis. This research combined the Rainbow model of integrated care and the Five Foundations for Integrated Care model as conceptual frameworks for analysing the data.28 31 This data analysis was inspired by multiple case study analysis by Yin22 and Miles and Huberman.32 At first, the data analysis was conducted at the within-case level to explore and describe the findings for each case. This was followed by cross-case analysis to identify similarities and differences across the cases to synthesise the findings and draw conclusions as a whole.32 33
Data analysis included transcription, debriefing, codification, data display, thematic content analysis and triangulation.34 Raw data were coded and analysed both within and across cases using ATLAS.ti, a qualitative analysis software. Recordings and quotations from collected data were deidentified to ensure the participants’ and communities’ confidentiality. All transcripts were read and reread, and initial coding was conducted. We developed a coding list based on the coding of the first few transcripts and was discussed with the team members to bolster the consistency of the data interpretation as well as the coding strategy.
Mixed deductive and inductive approaches were used to identify themes. Conceptual frameworks were used to develop themes deductively, whereas new themes from the data were identified inductively. The codes were collapsed to potential themes and final themes via an iterative process by critically analysing concepts and linking them across the data. Word table and matrixes were used to visually examine and synthesise the data for each case and across cases. Any differences in interpretation were resolved by discussion until consensus was achieved (online supplementary file 2 outlines the example of a code tree).
Supplemental material
To establish trustworthiness, member checking using synthesised data was done. During member checking, preliminary results were provided to stakeholders, and they were asked to suggest any change or additional information. Other strategies to enhance trustworthiness included the triangulation of multiple data collection methods and data sources as well as investigators triangulation.
Patient and public involvement
Cree community members participated during the planning phase of the project. Patients were involved in the recruitment and conduct of the study. The research results have been shared with the CHBSSJB organisation to facilitate integrated care in oral health services at this organisation.
Results
The total number of key participants in Discovery phase was 27 and in Dream phases was 44 (table 1). In total, 6 group discussions and 36 interviews were conducted, and ten major themes emerged in the Discovery and Dream phases. For confidentiality purposes, all quotations have been rendered in English.
Total number key informants in Discovery phase and Dream phase
Discovery phase
In this phase, from four FGD and three interviews, five themes were identified as strengths of the organisation in integrating oral healthcare.
Theme 1: Cree illustration of the integration
The concept of integration is embedded in the Cree culture, which promotes working and moving forward interdependently. Working together helped them to claim their rights and sign their land claim agreement ‘the James Bay and Northern Quebec Agreement’. Consequently, from a vision of integration, the CBHSSJB developed its first strategic regional plan in 2004 as a tool for integrating health and social services in the Cree communities.
The concept of working together or integrated services is not new to Cree people; we are people who are very interdependent. We believe that in order to move forward, we need each other. And the signing of ‘the James Bay Northern Quebec agreement’ is one big example of when we achieved working together. (Administrator 1, FGD)
Theme 2: organisation committed to a clear vision
All the stakeholders appreciated the development of an integrated care delivery model in the CBHSSJB organisation’s strategic plans including the integration of oral health. They also valued organisations’ continuous efforts in working towards achieving their planned goals and objectives mentioned in their strategic plans.
We're going to make a structure that will be facilitating to bring in the integrated services that have been the vision since 2004–2014. Then, we are working on the strategic plan, then we will look at the objectives that are expected, [….] we are working with epidemiology and statistics. (Administrator 2, FGD)
The CBHSSJB organisation works for integrating oral health by facilitating interprofessional teamwork and oral health promotion during health promotion activities.
There is a connection with dental for a couple of years; […] people see that oral health is within health in general, … we had a presentation with diabetes, we have links with the physicians that send us patients …, we work with the Community Health Representatives (CHR) …. It is the same principle with the school and the daycare… it's part of our goals to integrate within the health field … but if you look in the south, it's rare for a dental clinic to be inside the hospital. (Dental health care provider 1, FGD)
Theme 3: engaged professionals within an effective organisational structure
Another strength of the CBHSSJB is its multilevel organisational structure under the strong leadership of the board of directors and executive directors. It creates a sound work environment for the professionals to be fully engaged within their roles and responsibilities.
We have the chief of department fully engaging in the administrative duty of the department of the nine clinics, which is very unique. Because of that, we have built up a very good structure. We are close-knit families in between the communities. We often have meetings with the dentists, dental hygienists. (Administrator 3, FGD)
Participants reported that the CBHSSJB has multiple incessant challenges because of the higher prevalence of health problems as well as associated health needs in the communities. Nevertheless, participants praised the organisation’s efforts to provide services adapted to the population’s local needs.
Local directors in each community… to get a little more local control in adapting the needs of the local communities […], but how do we work is all together and the patients feel that everything flows well for them. (Administrator 2, FGD)
Theme 4. operational structure that supports integration of oral health
The CBHSSJB has developed an infrastructure facilitating the co-location of the dental clinic with other primary care services. The organisation also provides a supportive environment by providing free basic and referral oral healthcare services.
It’s all the relationship, we are in the same building, and we are workers. Now, it’s comfortable, we are talking about the nurses, the physicians, for sure physicians could help … to deal together with them. (Dental care provider 2, FGD)
Theme 5. significance of Cree language in healthcare provision
The importance of the Cree language in the provision of health and oral healthcare was one of the strengths of integrated care delivery at CBHSSJB. The use of Cree language in service delivery promotes Cree traditions and customs. However, translating from English to the Cree language is sometimes difficult due to the unavailability of some scientific terms in the Cree language. Henceforth, this theme pointed out developing and translating the Cree dental terms based on the definition and explanation of the scientific terms.
‘Minapidesuu’ (the one who pulls teeth out), that's the name of dentist …. So, the fear factor and trauma come back in that word …. So, in order to have the activity of oral dental health care, people take personal responsibility, they won’t because of that fear factor in that trauma […]. I asked better word for oral health care with the CHR for translating for the unilingual speaking or even to children with mothers, they say ‘Minapideo’ (‘to have better-looking teeth’), I say the term ‘Minapideo’ would be a better term for good oral healthcare. (Administrator 4, FGD)
Environmental scan
Our results from the documentation review identified five categories of documents from a total of 232 documents, including planning documents, health outcome reports, administrative documents, procedural documents and educational tools. Table 2 outlines environmental scan data on common POHC services in Cree communities. These services include services at CMC, Â Mâshkûpimâtsît Awash, Elementary school-based programmes and Daycare and homecare programmes provided by various dental and non-dental primary healthcare providers. Table 3 provides the contextual description of the four cases and table 4 compares elements of integrated POHC across all four cases.
Common primary oral healthcare services in Cree communities
Contextual description of four cases
Elements of integrated primary oral healthcare across all four cases
From the environmental scan, we identified three strengths of the CBHSSJB organisation that support the integration of POHC: (1) provision of dental services proportional to the communities’ population; (2) development of strategies for incorporating oral health into service delivery within CMCs and public health programmes and (3) guidelines for multidisciplinary team working. We also identified the colocation of the dental clinic, the referral system for public programmes and specialised services, and the shared medical record system as facilitators for coordination among care providers. However, some challenges existed in regard to the ill-defined role of general practitioners, the non-optimal referral procedure and follow-ups within health centres, and the need for more standardised protocols and guidelines.
Dream phase
A total of two FGD and 33 individual interviews were conducted during this phase and five themes emerged for our analysis.
Theme 1: anticipating the expansion of oral health promotion and faster access to care
Participants shared stories about their satisfaction with the quality of dental services at the clinic. This theme also confirmed findings from the previous phase in terms of the recognition participants gave to the colocation of the dental clinics, the provision of free dental services as well as the oral health promotion programmes.
[happy with the services for oral health?] Yes! I think there are more services here than down south. (Non-dental care provider 1, Interview)
Most participants mentioned the challenge of booking dental appointments due to the long waitlists. Therefore, they dreamed of promoting immediate appointment scheduling especially in cases of urgent needs. Furthermore, they wished extended oral health promotion programmes especially for the elderly and people with special needs.
I think there should be an improvement … even for special needs …, they should do at least visits because some of them are at home either & they can’t come directly here. (Non-dental care provider 2, Interview)
Theme 2. ameliorating human resource management
Participants praised the CBHSSJB in appointing Cree healthcare workers and permanent health professionals. Appointing Cree employees reflects a cultural-appropriate way to render health services. However, they still dreamed of having more Cree and permanent employees for compensating problems associated with long waitlists for the appointment.
Cree employees make a difference. […] When you have someone that speaks in Cree to you, you tend to listen more, you tend to ask more questions. (Administrator 5, Interview)
I wish we had more dentists so they can have regular check-ups …. I think one dentist is not enough. (Patient 1, Interview)
Theme 3: envisioning enhanced care coordination and navigation
They recognised strong team working and effective coordination among professionals as the strength of this organisation. It creates a pleasant environment not only for care professionals but also for patients. Moreover, shared physical medical and dental records facilitate care coordination and referral services.
The key success of your clinic is the interaction between everybody when it works well. Here it does. […] First of all, it’s much more pleasant for me because it’s a good environment to work in, but it’s good for the patient as well, he can feel that things are going well, that it’s pleasant. (Dental health care provider 3, Interview)
These participants hoped to strengthen the care coordination especially for chronically ill medical patients by developing more accessible protocols and guidelines for appointment scheduling and interdepartmental referral. They also desired digitalising health records for quick access to health information and streamlined health data.
It takes a long time before the report comes in, so … by digital, It’s faster. (Non-dental care provider 1, Interview)
Theme 4: organisation working towards continuous improvement
Participants praised CBHSSJH’s continuous efforts to develop advanced technology and infrastructure, providing logistical support and conducting regular meetings and evaluations.
For the administration part, we have everything … like we have more than enough … material, … equipment, I’m happy with what I have. (Dental care provider 4, Interview)
Some communities have excellent infrastructure, while others are very crowded. They dreamed of new bigger infrastructure in the communities where this was not available.
We need the space; we need a new hospital. We have 3–4 chairs, actually at the moment. We have some period of time when specialist doctors come to the dental clinic. They use the same room as the dental hygienist. We need the dental hygienist that week to not provide her services. So, it’s a question of space. (Administrator 6, FGD)
Theme 5: focus on integrating culture into oral healthcare
Participants appreciated the integration of traditional practices into health services by creating a specific department (Nishiiyuu Miyupimaatisiiun Department) that works on integrating traditional knowledge and culture for their health and well-being. They also valued the role of Cree traditional healing in health and oral health problems.
We have the cultural department now in the community … it’s only been up a couple of years now. We even have a book on traditional medicine. […] I know one specific medicine, [….] that’s been used before, … how is tooth pain taken care of? […] The only way I knew was feces. Feces wrapped in a cloth and put it in your tooth; then you had to bite on it. And I saw it too! it worked on my sister! […] I know they talked about using fire ashes to brush your teeth. (Administrator 7, interview)
They praised non-Cree health professionals’ interest in learning culture with their own experiences working in Eeyou Istchee. Non-Cree employees even pointed out more relevance of immersing in the Cree culture than getting trained on the culture. These non-Cree employees while dealing with Cree clients, emphasised learning Cree history and sharing their experiences with the elders in the communities to better understand their clients.
(If) you understand the culture, easier your work is. At the beginning, it was so hard because we take all our knowledge from the south … and we try to apply them here, and […], it doesn’t help. Experience, you have to come, and … because those things cannot be taught, you need to live with people to realize. (Dental care provider 4, interview)
The non-judgment of the patient is that we will learn to have more openness to cultural differences…; then it's sure that after listening, you have to know the history of the Cree […] You have to know what they lived. […] Then there are times when I do not understand what's going on with the client, … I go to sit down with social services, and then I say there's something I do not understand, is that what Can you explain to me? Then they will not give you the answer right now, they will give you a big history before. Then, there are lots of times I've been stuck, and then I go to … the elder in social services, I need help there, I'm stuck, you explain to me and in general, I'll have feedback, okay, that's why this person is like that because culturally you do not say it, it's unsaid, but that's what happened. (Non-dental care provider 3, Interview)
However, they wished to raise community awareness about traditional medicines and to integrate cultural oral health practices by learning about traditional healing from elders. This will not only help in keeping their traditional Cree healing alive but also will be beneficial in achieving holistic health.
Some of our elders … can help fix the toothache or can fix health, a lot of stuff with traditional medicine, AMAZING! … Respect what we know because it's something that's really amazing … [we need] to integrate all the knowledge … from the elders. (Non-dental care provider 4, Interview)
People need to be shown … how to work with the [traditional] medicines and … educating them would be a vital thing for the community … that’s what I think needs to be done. (Administrator 7, Interview)
Design phase
Recommendations for an action plan were discussed and validated with key collaborators and were presented to administrators and healthcare providers. These recommendations were divided into the following categories: increasing promotive and preventive services, faster access to dental services, improving management, better coordination, and promoting cultural integration. (table 5).
Recommendations developed and validated in design phase
Discussion
To our knowledge, this is the first study that uses AI in the field of Indigenous oral health research. The use of AI in evaluation allows for better recognition of Indigenous culture and values in organisational health services. Our results suggest that the CBHSSJB has developed a grassroots innovation in integrating POHC. Commencing with the identification of oral health needs in the communities, this organisation is progressively working on the regular development of policies for organisational governance, management and the coordination of services. The recommendations derived from the results can help to optimise the integrated POHC services in the CBHSSJB organisation. Also, these recommendations will help in providing new scientific evidence on the integration of oral health into primary care, which could be instrumental in improving the quality of oral healthcare.
Facilitators of integrated oral healthcare are similar to those identified in previous studies, such as interprofessional collaboration, geographical proximity, shared health records, supportive operational policies and native health workers.35 36 Similarly, barriers in this regard were also in line with what has been identified in previous literature; for example, lack of exclusive bidirectional interprofessional education, lack of human resources and staff turnover.35
In general, there are few integrated health programmes such as Medicaid, Affordable Care Act, CareMore health systems that offer dental coverage; most of them have very limited or only emergency based dental coverage especially for vulnerable populations.37 38 Several organisations and associations including Neighborcare, Dorchester House Multiservice Centre, Kaiser Permanente, Marshfield Clinic, Boston Medical Centre have used novel ideas to integrate oral healthcare into primary care, such as colocation, cross-referral process, cross-training on oral health screening for physicians oral healthcare screening in schools, interprofessional collaboration, shared electronic health records, case management and performance measurement.36–40 The CBHSSJB is actually addressing most of the recommendations for developing an integrated POHC approach from available evidence of various organisations.7 39 For instance, it established a population-based health management approach, shared health records, assured geographical proximity, had dental coverage, interprofessional collaboration and referral.39
The themes derived from this study coincide with all the dimensions of integrated care as per the Rainbow model and the five foundations of integrated care model. As reported by Leutz, the degree of integrated POHC at the CBHSSJB corresponds to the coordination and linkage rather than full integration.41 Based on the extent of integration of dental care described by Atchison et al, the CBHSSJB represents an example of co-location and closer integration of medical and dental providers.36
The selection of four cases represents a reasonable number to achieve diversity among the key variables as well as the transferability of our findings. The diverse roles and responsibilities of the study participants support the applicability of these findings among the stakeholders of different healthcare organisations. However, this study might have encountered bias due to various types of study participants such as administrators, healthcare providers and patients. Nevertheless, a large sample size would have outweighed such biases by ensuring representativeness from all participants’ range. Being qualitative in nature, this study does not support the generalisability of its findings; however, our study findings contribute to integrated POHC research and can be applicable to other similar settings.
Conclusion
This study results suggest that the CBHSSJB has developed a grassroots innovation in integrating POHC. This organisation has been successful in implementing strategic planning on oral health integration into primary care at all levels of integration, nonetheless, the organisation needs further strengthening for full integration.
Acknowledgments
We would like to acknowledge the Cree Board of Health and Social Services of James Bay, Cree communities and research team members for their constant help and support. The authors gratefully acknowledge the administrators, healthcare providers and patients that participated in this study. We are thankful to Lucie Papineau, Evelyne Lefebvre and Nicole Jolin for their continuous support, valuable suggestions and worthy contributions.
References
Footnotes
Contributors RS contributed to study conception, design, data collection, transcription, reviewing transcripts, coding, analysis, interpretation of data and manuscript writing. YC participated in study conception, data collection, data interpretation and critical revision of the manuscript. FG contributed to data collection, data interpretation and critical revision of the manuscript. CB and MEM were engaged in data interpretation and critical revision of the manuscript. JT contributed to study concept and design, data interpretation and critical revision of the manuscript. EE contributed to study concept and design, project administration, data collection, data analysis, data interpretation, manuscript drafting and critical revision of manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Funding This study was supported by the funding from the Canadian Institutes of Health Research (grant number: GI1-145123). It has been cofunded by the Institut de recherche en santé publique de l’Université de Montréal, Quebec Population Health Research Network, the Network for Canadian Oral Health Research, the Network for Oral and Bone Health Research and Fondation de l’Ordre des dentistes du Québec. RS is a doctorate student funded by the merit scholarship programme for foreign students (PBEEE) by the Fonds de recherche du Québec – Nature et technologies.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The ethical approval for this study was obtained from the Institutional ethics review board of the Université de Montréal (15–130-CERES-P), McGill University (A10-B39-18A) and research committee of Cree Board of Health and Social Services of James Bay.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplementary information. The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.