Article Text

Abstract
Introduction Sarcopenia is a geriatric syndrome characterised by progressive loss of skeletal muscle mass and function with risks of adverse outcomes and becomes more prevalent due to ageing population. Elastic-band exercise, vibration treatment and hydroxymethylbutyrate (HMB) supplementation were previously proven to have positive effects on the control of sarcopenia. The purpose of this study is to evaluate the effectiveness of elastic-band exercise or vibration treatment with HMB supplementation in managing sarcopenia. Our findings will provide a safe and efficient strategy to mitigate the progression of sarcopenia in older people and contribute to higher quality of life as well as improved long-term health outcomes of elderly people.
Methods and analysis In this single-blinded, randomised controlled trial (RCT), subjects will be screened for sarcopenia based on the Asian Working Group for Sarcopenia (AWGS) definition and 144 sarcopenic subjects aged 65 or above will be recruited. This RCT will have three groups evaluated at two time points to measure changes over 3 months—the control and the groups with combined HMB supplement and elastic-band resistance exercise or vibration treatment. Changes in muscle strength in lower extremity will be the primary outcome. Muscle strength in the upper extremity, gait speed, muscle mass (based on AWGS definition), functional performance in terms of balancing ability and time-up-and-go test and quality of life will be taken as secondary outcomes. In addition, each participant’s daily activity will be monitored by a wrist-worn activity tracker. Repeated-measures analysis of variance will be performed to compare within-subject changes between control and treatment groups at two time points of pretreatments and post-treatments.
Ethics and dissemination The procedures have been approved by the Joint CUHK-NTEC Clinical Research Management Office (Ref. CREC 2018.602) and conformed to the Declaration of Helsinki. Results will be disseminated through peer-reviewed publications, conferences and workshops.
Trial registration number NCT04028206.
- geriatric medicine
- nutrition & dietetics
- musculoskeletal disorders
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study can provide a safe and efficient strategy to mitigate the progression of sarcopenia in older people.
All interventions including elastic-band exercise, hydroxymethylbutyrate supplementation and vibration treatment are simple to adopt.
This trial cannot be double-blinded as blinding to treatment allocation of subjects is not possible.
Introduction
Sarcopenia is a geriatric syndrome characterised by the progressive loss of skeletal muscle mass and function with a risk of adverse outcomes.1–3 The prevalence of sarcopenia range varies across regions from 1% to 29% in community-dwellers, 14% to 33% in long-term care populations and 10% in acute hospitals.4 According to a meta-analysis on the effect of sarcopenia on health outcomes in older people, sarcopenia significantly increases HRs of falling by 3.23×, functional decline by 3.03× and fracture risk by up to 3.75×, thus making sarcopenia a major risk factor for fragility fracture.5 Sarcopenia is, therefore, an intervention target to tackle.
A recent study reported a randomised controlled trial (RCT) of 3-month intervention of elastic-band exercise alone has shown significant enhancement in skeletal muscle mass by a 0.7 kg gain and a better performance demonstrated by 0.14 m/s faster gait speed.6 A combination of elastic-band exercise, ankle-weight exercise and chair exercise for 60 min twice a week for 3 months was found to be effective in enhancing leg muscle mass by >2%, gait speed by >15% and knee extension strength by ~5% with statistical significance in an RCT by Katayama’s group.7 These indicate that resistance training such as elastic-band exercise has positive effects on muscle mass and performance.
Low-magnitude high-frequency vibration (LMHFV) has previously been shown to be effective in enhancing muscle strength, balancing ability and reducing fall risk. In an RCT involving 710 subjects, community-dwelling elderly people treated at 35 Hz, 0.3 g and 20 min per day for 18 months showed reduced HR for fall or fracture (HR 0.56, 95% CI 0.40 to 0.78, p=0.001), 2.46 kg increase in quadriceps strength (95% CI at 1.70 to 3.22, p<0.001) and overall statistically significant improvements in balancing ability.8 Thus, LMHFV is an evidence-supported novel exercise intervention strategy for sarcopenia.
A previous RCT showed that beta-hydroxy-beta-methylbutyrate (HMB) supplementation on 10-day bed-rested older adults aged 60–76, 3.0 g/day was effective in maintaining total lean mass, appendicular lean mass, leg and arm lean masses with significant differences.9 Our preclinical data demonstrated enhancement in grip strength and reduction in intramyocellular fat content (9.23%, p=0.011) in sarcopenic mice models receiving 3-month HMB supplementation.10 Therefore, HMB is a promising intervention to prevent intramyocellular fat infiltration in sarcopenia.
Although sarcopenia is a widely prevalent syndrome affecting a large population, there is currently no approved drug for it, nor consensus on the treatment or prevention of sarcopenia. Furthermore, since it is a relatively understudied field, studies on exercise, nutrition and supplements often reported variations in outcome measures making choosing the clinical management more difficult for doctors. Therefore, sarcopenia is a syndrome that is currently not clinically managed.
A systematic review with meta-analysis by Courel-Ibáñezet al reported that the effect of HMB supplementation in addition to physical exercise was not significant on improving muscle strength or physical performance in adults aged 50–80 years compared with exercise alone.11 This conclusion was drawn based on 10 RCTs that involved healthy and younger subjects from 50 years of age, with heterogeneous dosages of HMB supplement and exercise programmes. However, very few data exist that test the combined effects of HMB and exercise on the musculoskeletal health in older, frailer or sarcopenic people. The application of HMB supplement alone is a promising strategy for sarcopenic patients and the effects of combining HMB and exercise in older people are mostly positive. Our animal study demonstrated that 3-month combined LMHFV and HMB supplementation enhanced muscle strength and decreased percentage fat mass and intramuscular fat infiltration as compared with either treatment alone in sarcopenic mice models.10 One pilot non-randomised control trial on sarcopenic patients with gastric cancer reported that a preoperative daily exercise programme (handgrip training, walking and resistance training) with nutritional support including HMB could reduce sarcopenia.12 More clinical trials should be conducted to provide additional evidence to support treatment choices for older, frailer or sarcopenic people.
In this study, a combination of elastic-band exercise or vibration treatment and HMB supplementation was proposed to improve muscle strength and physical function in older people. The aim of this study is to evaluate the effectiveness of elastic-band exercise or vibration treatment with HMB supplementation on the control of sarcopenia.
Methods and analysis
Sample size determination
Based on the latest published data13 on a similar study employing the same exercise programme (designed by our project team) with or without nutritional supplement (milk formula), the outcome of muscle strength by leg extension (one repetition maximum) (kg) in sarcopenic subjects after 3 months (12 weeks) were 14.81±4.86 kg, 18.57±8.56 kg and 17.21±5.84 kg. Based on the actual sample size from this reference study (n=403 637), and the average SD of ±6.3 kg, the calculated effect size was 0.248 which was of moderate effect size. Using this calculated effect size as an assumption in this study, estimated at α=0.05 and power=0.81 with three groups (Control, EXE + HMB and VT + HMB) evaluated at two time points, the total sample size required to detect between-factor statistical significant difference by repeated-measures analysis of variance (ANOVA) is n=123 (n=41 per group by G*Power V.3.1.9.2). Assuming 15% of participants will drop out of the study, total sample size of n=144 (or n=48 per group) is required for the RCT study. At the same effect size, sample size required to detect within-factor differences, and interactions by repeated-measures ANOVA based on a correlation among repeated measures of 0.5 are n=36 and n=45, respectively.14 Thus, a total of 144 subjects will be recruited.
Study design and grouping
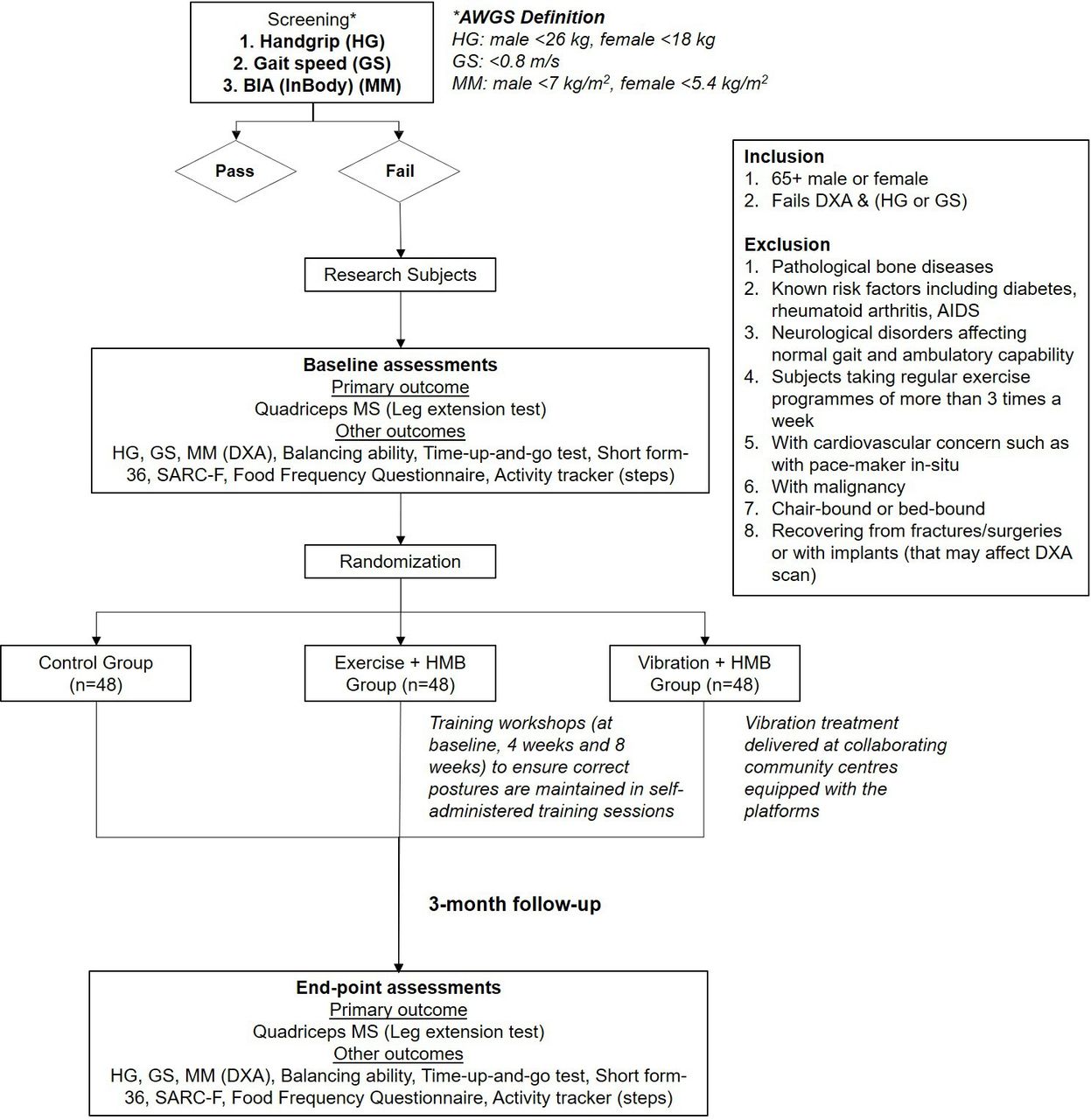
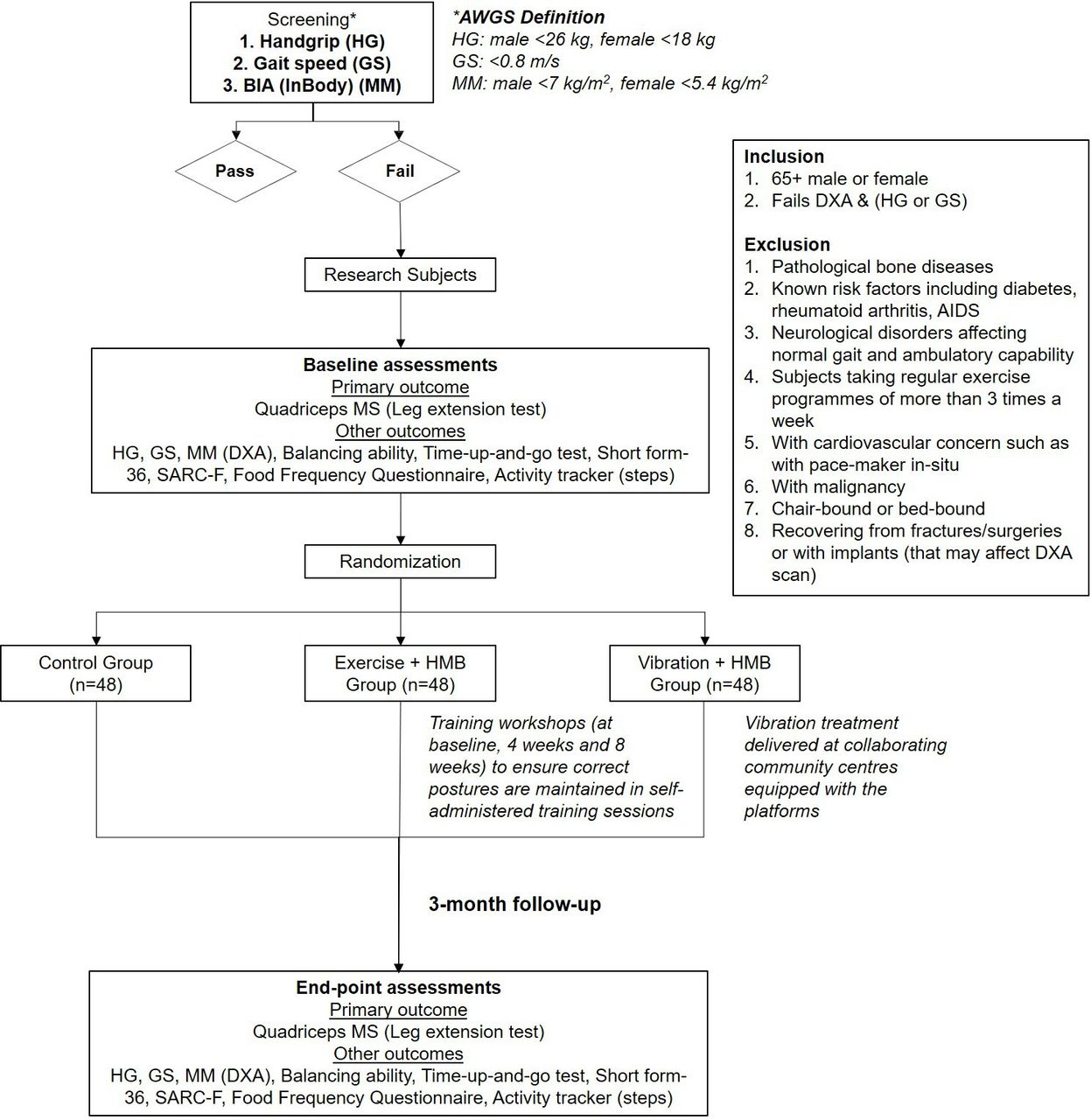
A single-blinded RCT will be adopted and has been registered at the ClinicalTrials.gov. The study will be conducted in an academic hospital in Hong Kong and data will be collected from subjects recruited across all districts of the city. Subjects will be screened for sarcopenia based on the Asian Working Group for Sarcopenia (AWGS) definition and 144 sarcopenic subjects aged 65 or above will be recruited. The AWGS criteria measures sarcopenia with hand-grip strength (male at <26 kg, female at <18 kg), gait speed test (<0.8 m/s) and lean body mass measurement by dual-energy X-ray absorptiometry (DXA, male at <7 kg/m2 and female at <5.4 kg/m2). A flow diagram of the whole trial is shown in figure 1. This RCT will have three arms to investigate the effect of (1, EXE + HMB) combined treatment of elastic-band exercise (30 min/day)13 and HMB supplementation (at 3.0 g/day)9 for 3 months; (2, VT + HMB) combined treatment of vibration exercise (at 35 Hz, 0.3 g and 20 minutes/day)8 and HMB supplementation (at 3.0 g/day) against (3, CTRL) a control group of sarcopenic subjects with no intervention. Prior to screening, all the three groups will receive the same level of educational talks and each subject will be given a booklet containing diet and exercise strategies. Subjects will be monitored on daily activity by a wrist-worn activity tracker15 16 and quantitative data will be taken into account for analysis. An exercise calendar will also be given to each participant for self-reporting and encourage compliance.
{kind=link}
The flow chart summarises the design of this study. AWGS, Asian Working Group for Sarcopenia; DXA, dual-energy X-ray absorptiometry; HMB, hydroxymethylbutyrate; MM, muscle mass; MS, muscle strength.
Recruitment strategy
Subjects will be recruited for this RCT through three approaches: (1) promotional and educational talks at community centres; (2) street booths set up at commercial centres situated in densely populated public housing estates across entire Hong Kong and (3) home visits in collaboration with social workers from each collaborating community centre in their outreach programmes. The latter two approaches specifically target home-dwelling older people who would normally not engage in community centre activities. Participants will first be screened by the portable bioimpedance analysis (Inbody, USA), gait speed test and handgrip test on site. Those who fail the screening are defined sarcopenic and will be invited to participate in this study.
Before recruitment, they will be informed of the potential benefits and risks of the interventions in this study. They will then be required to fill out an informed consent (online supplementary file 1) and can withdraw from this study without any condition.
Supplemental material
Inclusion and exclusion criteria
Adults aged 65 years or above failing the sarcopenia screening (defined by AWGS) will be included. Exclusion criteria are subjects with pathological bone diseases; chronic inflammatory conditions known to affect muscle metabolism, including diabetes, rheumatoid arthritis; neurological conditions affecting normal gait and dependent ambulatory capability; subjects taking regular guided exercise programmes of more than three times per week; subjects with cardiovascular concern such as with pace-maker in situ or malignancy as they are not suitable to receive vibration treatment; chair-bound or bed-bound subjects as they cannot stand on the vibration platform and subjects recovering from fractures/surgeries or with implants (that may affect DXA scan).
Randomisation and blinding
After obtaining written consent and completing all screening tests, each subject will draw a sealed envelope with a randomly assigned number representing either treatment or control group only known to one of the research staff. Subjects’ activity will be tracked by a wrist-worn activity tracker to control for potential variations between groups. Except for the research staff responsible for grouping randomisation and the subjects, all other participating personnel including investigators, outcome assessors, statistician will be blinded from the grouping assignment to prevent bias.
Intervention
After baseline visit, regular phone reminders will be used to remind subjects to complete their corresponding interventions and about the date of their end-point assessments. Contacts will be provided for any queries during the study.
HMB supplement
HMB supplementation will be started on day 1 after the first visit to the Prince of Wales Hospital for baseline measurements. HMB capsules (Double Wood Supplements, USA) will be given to subjects at baseline, and to be taken three times daily, 1 hour before exercise or vibration and with meals at 1 g doses (3.0 g/day) during the 12-week treatment period.9 Subjects will be instructed to adhere to the prescribed dosage and keep unused supplements which will be collected at their next follow-up visit for end-point compliance evaluation.
Elastic-band exercise
Subjects enrolled in the elastic-band exercise group will be instructed with one session of group training (at baseline) and one follow-up home visit (at 4 weeks) including instructions on 5–10 min warm-up and cool-down routines, 30 min chair-based resistance exercises using Thera-Bands as previously reported13 with training to both upper and lower body muscle groups including both hand and knee extensor muscles. Subjects will perform the instructed exercises three times per week, 1 hour after HMB intake, for 12 weeks. The elastic band strengths will be progressively increased from 1.3 kg to 2.1 kg (yellow to green) of tensional force as instructed by a qualified coach in our project team based on each subject’s ‘multiple repetition maximum’, which is defined by reaching fatigue by eight repetitions of stretching. Participants will be provided with Thera-Bands and an exercise leaflet. Training workshops will be conducted for subjects to ensure that correct postures are maintained in self-administered training sessions. Compliance of the exercise programme will be monitored by a wrist-worn activity tracker recording motion and heart rates,15 16 supplemented with a self-reported exercise calendar as a backup measure.
Vibration treatment
Subjects enrolled in the vibration treatment group will be assigned a collaborating community centre close to their home equipped with a vibration platform (V-health, Hong Kong) that delivers cyclic mechanical loading at 35 Hz and 0.3 g as previously reported.8 Treatment scheme is 20 min per day, at least 3 days per week for 12 weeks. A user card will be given to the subject to record compliance.
Outcome measures
The following assessments will be taken at the baseline and endpoint of 3 months. A print-out on dietary and exercise advice (online supplementary file 2, the Ensure NutriVigor shown is an example of a product that is known to contain HMB, but that it is not used as an intervention in this study) will be given to each participant based on their body conditions at their end-point assessments.
Supplemental material
Primary outcome
Muscle strength in the lower extremity
Quadriceps muscle strength will be evaluated as the primary outcome of this study as previously reported8 13 in order to compare the treatment effects between (1) elastic-band exercise +HMB, (2) vibration treatment + HMB against the (3) control group. Active lower leg extension will be instructed to the subject on sitting position with both feet free from the ground and the hip and knee joint flexed at 90° angle and pelvis fixed. The peak isometric forces will be measured three times on each leg using a digital dynamometer (Landtek, Guangzhou, China) and the maximum value will be taken.
Secondary outcome
Muscle strength in the upper extremity
Handgrip strength will be measured by a dynamometer (5030JI, JAMAR, USA) on each hand of the subject in order to compare the treatment effects between (1) elastic-band exercise + HMB, (2) vibration treatment +HMB against the (3) control group. Participants will be instructed to hold the device with the arm at right angle and elbow to the side of the body. The maximum effort will be taken from three tries (male at <26 kg, female at <18 kg).
Gait speed
A 6 m walk test will be used to calculate the gait speed of each participant. Gait speed lower than 0.8 m/s is the cut-off value defined by AWGS for sarcopenia diagnosis.
Muscle mass
Height-adjusted skeletal muscle mass (total skeletal muscle mass/height2; kg/m2) will be measured by DXA (Horizon, Hologic, USA). A whole-body scan will be performed by an independent certified technician at the Prince of Wales Hospital. Total appendicular muscle mass will be calculated by summation of muscle mass measured in the four limbs, with the operator adjusting the cut lines of the limbs according to the specific anatomical landmarks (male at <7 kg/m2 and female at <5.4 kg/m2).
Balancing ability
Biodex Balance System SD (BioSway, Biodex Medical Systems, USA) will be used to measure the balancing ability of the subjects. This is a verified assessment tool to measure the angular excursion of subject’s centre of gravity during movement. Parameters of balancing ability include reaction time, movement velocity, maximum/end-point excursion and directional control in Limit of Stability Test.8
Timed-up-go test
Time will be recorded for participants to rise from a chair, walk 3 m, turn around, walk back to the chair and sit down.
Quality of life by Short-Form-36
Health-related quality of life8 will be assessed by the validated Chinese version of the 36-item Short-Form Health Survey.
SARC-F questionnaire
A short questionnaire with five components will be used for a rapid sarcopenia diagnosis. The score ranges from 0 to 10, with 0–2 points per component. A score that is predictive of sarcopenia will be greater than or equal to 4.
Daily activity
A wrist-worn activity tracker will be given to each participant15 16 to track their daily activity. Number of steps taken per day will be used to control for potential differences in activity levels between groups and within subjects.
Dietary status by Food Frequency Questionnaire
A detailed and validated Food Frequency Questionnaire17 will be used to record the dietary intake at the baseline and end-point of 3 months to validate the consistency in their diet during the study period. All subjects are advised to adhere to their current dietary intake and habits throughout this period. Potential differences between groups and within subject groups will be analysed.
Data management
All information concerning the subjects will be recorded and saved on password-protected computers. A detailed database will be set up to track each subject’s progress through this trial, including the scheduling of baseline and end-point assessments. All the generated data will be stored on password-protected computers or servers that are only accessible to the research team.
Data statement
Data and resources will be shared with other eligible investigators through academically established means. The protocol and datasets used and/or analysed in this study will be available from the corresponding author on reasonable request. Researchers who provide a methodologically sound proposal may access data to achieve aims in the approved proposal.
Statistical methods
All data will be entered into a database and analysed using SPSS V.20.0 software (IBM). Data analysis will be performed based on the intention-to-treat principle including all randomised participants. Normality will be assessed by visual inspection of Q-Q plots. For the primary outcome of muscle strength, within-subject changes will be compared between control and treatment groups (EXE +HMB and VT + HMB) by two-way repeated-measures ANOVA at baseline and 3-month follow-up, followed by post hoc Bonferroni adjustment for group-wise comparison. Analysis of covariance will be used to analyse the differences between interventions over time to further evaluate the effectiveness of the interventions in improving the secondary outcomes. Covariates applied to the analysis will include age, gender, physical activity and baseline assessments. Statistics on between-group treatment effects, within-group effects, between-factors interaction, and the effect sizes will be evaluated. Rank or skewed (not follow normality) data will be examined using Wilcoxon signed-rank test. Statistical significance is considered at p<0.05 with missing data addressed using multiple imputation.
Patient and public involvement
Patients and the public were not involved in the design or planning of the study. Members of the public are involved in recruitment of participants or conduct of the study. We will report test results to participants in plain language after their end-point assessments are completed. Results will be available to the public and patients in the forms of educational talks and booklets or flyers and published in open access peer-reviewed journals.
Ethics and dissemination
This study was approved by Joint CUHK-NTEC Clinical Research Management Office (Ref. CREC 2018.602) and conformed to the Declaration of Helsinki. Trial results will be published in peer-reviewed journals and disseminated at relevant conferences and to the public via educational talks and booklets or flyers.
Discussion
This study is designed as a single-blinded RCT to test the effectiveness of elastic-band exercise or vibration treatment with HMB supplementation on the progression of sarcopenia. As the world’s population is ageing, there will be higher prevalence of sarcopenia in elderly people. The onset of sarcopenia can lead to functional decline, and eventually occurrence of falls and fractures. Thus, it is important to derive ways to provide a safe and efficient strategy to mitigate the progression of sarcopenia in older people.
In this study, the intervention consists of combined treatment of elastic-band exercise or vibration treatment with HMB supplementation. The composition of the interventions is based on previous studies suggesting interventions by multimodal exercise and high-protein intake with dietary advice to tackle sarcopenia. The European Working Group on Sarcopenia in Older People and the International Working Group on Sarcopenia reported that exercise intervention generally showed some positive effects on muscle mass and performance, as evidenced by improvements in muscle mass and physical performance (chair-rise, stair-climb and 12 min walk).4 Effectiveness was generally found to be better in studies lasting over 3 months. Resistance exercise training has been reported to exert anabolic and anti-inflammatory effects. It could activate anabolic signalling pathways such as Akt/mTOR pathway (Protein kinase B/mammalian target of rapamycin) which might help to attenuate the loss of muscle mass and reduce proinflammatory status which is common in sarcopenic people.18 As for nutritional interventions, many studies have reported various schemes of interventions, mostly including protein supplements, essential amino acid supplements, HMB supplements or fatty acid supplements. Among them, HMB supplementation was shown to be effective in maintaining muscle mass9 and improved muscle strength and performance.19 Moreover, our laboratory showed that LMHFV was effective to enhance muscle strength, balancing ability and reduce fall risks in elderly people.8 In sarcopenic animal model, HMB supplementation plus LMHFV treatment enhanced muscle strength and decreased percentage fat mass and intramuscular fat infiltration as compared with either treatment alone.10 However, the beneficial effects of HMB supplementation combined with exercise to preserve muscle mass and function in older adults are not well investigated.11 Thus, this clinical trial can provide a better understanding of the effectiveness of combined treatment in managing sarcopenia.
A strength of the interventions in this proposed study is their simplicity. The elastic-band exercise programme is simple to adopt and elderly people can carry out at home that is not restricted to space limitation. They can also have easy access to vibration platforms in a community centre in their neighbourhood. Oral supplementation of HMB is simple to administer with a prescribed dosage recommended to elderly people. All these simple interventions may help ensure good compliance.
There are some limitations in this study. First, it is impossible to conduct a double-blinded clinical trial as blinding to treatment allocation of subjects is not possible. We will carefully check the extent to which raters are blind to the group allocation. Second, only subjects without mobility impairment from the community will be recruited as it will be difficult to reach those people who are predominantly inactive or frail. Third, the use of self-report on HMB intake, vibration or exercise session compliance may subject to reporting bias. Thus, we will adopt calendar-reporting approach and instruct subjects how to record their corresponding interventions. Reminders will be given via regular phone calls as well. Lastly, the current study design limits our ability to identify effects in muscle mass or strength or physical performance contributed by HMB, vibration or elastic-band exercise due to the lack of HMB-only group.
The results of this RCT will provide further high-quality clinical evidence regarding combined treatment on the control of sarcopenia and their efficacy to improve muscle mass/strength. This trial may contribute to higher quality of life as well as improved long-term health outcomes of elderly people.
Trial status
The trial was commenced on 30 June 2019 and is currently at the stage of recruiting patients. The first subject was recruited on 4 September 2019. The anticipated date of recruitment completion is 29 July 2021.
Acknowledgments
We would like to thank all the colleagues in the Fall Prevention Team and the Bone Quality and Health Centre of the Department of Orthopaedics and Traumatology, Faculty of Medicine, The Chinese University of Hong Kong for their support and help in this work and all the subjects for their participation in this study; and the Evangelical Lutheran Church Social Service for the support and coordination of community events.
References
Footnotes
Contributors SK-HC, Y-NC, RM-YW and W-HC designed the study protocol. KC-CC provided advice about elastic-band resistance exercise training programme. SK-HC, Y-NC, KY-KC, C-YH and W-TH contributed to the implementation of this study protocol, data acquisition, analysis and interpretation of data. SK-HC and Y-NC drafted the protocol and all other named authors critically revised, contributed to the intellectual content of the protocol and approved the final manuscript.
Funding This trial is funded by Health Care and Promotion Scheme, Food and Health Bureau, The Government of the Hong Kong Special Administrative Region (Ref: 02180118).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval This study was approved by Joint CUHK-NTEC Clinical Research Management Office (Ref. CREC 2018.602) and conformed to the Declaration of Helsinki. Results will be disseminated through peer-reviewed publications, conferences and workshops.
Provenance and peer review Not commissioned; externally peer reviewed.