Article Text

Abstract
Objectives The aim was to study mortality due to suicide, accidental poisoning, event of undetermined intent and drug-related deaths through 20 years in Iceland.
Design A population-based register study.
Participants Individuals who died due to road traffic injury, suicide, accidental poisoning, event of undetermined intent and drug-related deaths in the population of Iceland during the years 1996–2015. Annual age-standardised rates were calculated, and the trend analysed by Pearson correlation and joinpoint regression.
Setting The population of Iceland framed the study material, and the data were obtained from nationwide registries for information on number of deaths and age-specific mean population in each year by gender.
Results The crude overall suicide rate during the last 10 years was 12.2 per 100 000 persons per year (95% CI 7.4 to 18.1), while the crude overall rate due to road traffic injuries was 4.6 per 100 000 persons per year (95% CI 2.0 to 8.3). Among men, suicide rates decreased, however not significantly (r(19)=−0.22, p=0.36), and for overdose by narcotics the rates increased significantly (r(19)=0.72, p<0.001) during the study period. Among women, the suicide rates increased, however not significantly (r(19)=0.35, p=0.13), for accidental poisoning, suicide and event of undetermined intent combined the rates increased significantly (r(19)=0.60, p=0.006); and the rates for overdose by sedative and overdose by narcotics both increased significantly r(19)=0.49, p=0.03, and r(19)=0.67, p=0.001, respectively.
Conclusion The suicide rates have not changed during 1996 to 2015; however, the rates for the combined accidental poisoning, suicide and event of undetermined intent increased significantly for women. The rise of the overdose rates for sedative among women and for narcotics among both genders are consistent with reports elsewhere.
- epidemiology
- public health
- statistics & research methods
- substance misuse
- suicide & self-harm
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Nationwide data coverage was an advantage in the data analysis and secured completeness.
The causes of death were obtained from death certificates and were systematically reported by International Classification of Diseases, 10th revision.
Under-reporting and misclassification of suicide may occur in unknown magnitude, and thus separate and combined analysis of suicide, accidental poisoning and death due to event of undetermined intent augment the information in the present study.
The combination of deaths because of overdose enhanced the analysis of this topical problem.
Introduction
Suicide rates increased in the USA through 1999 to 2016, and in 25 states more than 30% increases were observed.1 In 2016, the overall suicide rates in the USA was 15.6/100 000 (age adjusted).1 This comprehensive US report1 did not include injury death of undetermined intent, which is conventional in studies in the UK,2 and in accordance with UK Office for National Statistic reporting practice.3 Despite the differences in definition of suicide, the 2017 suicide rate in the UK, combining suicide and deaths of undetermined intent, was 10.1/100 000 (age adjusted) which is the lowest rate observed since 1981,4 and substantially lower than the US rates.
The inverse association between suicides and unintentional poisoning mortality through time has been suggested to be due to misclassification of poisoning deaths5 6; however, the increases in unintentional poisoning and undetermined poisoning rates exceed the reciprocal decrease in suicide rates according to the US studies.5 6
Increasing poisoning mortality rates in the USA and other places7 8 further add to the difficulties in registration of suicides in national data registries. Undercounting of suicide and misclassification of suicides as accidental poisonings or event of undetermined intent diminish the possibility to measure potential effects of prevention and intervention attempts.6 9 The situation is even more difficult in a small population as in Iceland; however, the mortality statistic of the country has been considered of high quality10 and the population dimensions in the National Registry have the character of annual census.11 According to recent overview from the Director of Health, it is not possible to state whether any changes have occurred in the overall death rates of suicides in Iceland through the last decades12 when counting death by intentional self-harm as an underlying cause of death. During the last 10 years, the annual overall suicide death rate in Iceland was 12.1/100 000.12 This report did not mention deaths due to accidental poisoning or event of undetermined intent.12 A work group established by the Director of Health has proposed several detailed measures in attempt to cut down the number of suicides13 and the office has conducted studies on suicidal thoughts and attempts among young people.14
In the light of this uncertainty and the risk of misclassification in the registration of the above-mentioned categories, the aim was to describe mortality due to suicide, accidental poisoning, event of undetermined intent and drug-related deaths by gender through 20 years in Iceland.
Materials and methods
The primary source of data was from the website of Statistic Iceland (National Cause of Death Registry, a nationwide death registry), accessed April 2018,15 and from the same website the age-specific population figures were obtained from the National Registry. The available age groups were 0 to 5 years, 6 to 15 years, 16 to 20 years, 21 to 66 years and 67 years and older. The registered cause of deaths was according to death certificates which were issued by physician according to Icelandic law.16 The causes of death have been coded according to the 10th revision of the International Classification of Diseases (ICD-10) since 1996,17 and available were the external cause of injury mortality. The registry contains only one main cause of death per individual. No information was available as to whether the death certificate was issued by medical coroner or other physicians; however, assertion of drug-related deaths had been confirmed after forensic investigation. The National Registry contains all inhabitants of Iceland and is continuously updated. The mean population was 269 thousand in 1996 and increased to 331 thousand in 2015, and during the period the proportion of foreign citizens grew from 2% to 7%.11
The injury mortality categories of interest were the following: V02–V89 motor vehicle transport accidents, called road traffic injuries; X40–X49 accidental poisoning by and exposure to noxious substances; X60–X84 intentional self-harm (suicide); Y10–Y34 event of undetermined intent; X40–X49, X60–X84 and Y10–Y34 combined accidental poisoning by and exposure to noxious substances, intentional self-harm and event of undetermined intent, called poisoning, suicide and undetermined; X41, X61 and Y11 combined accidental poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified, intentional self-poisoning and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified, and poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified, undetermined intent, called overdose by sedative; X42, X62 and Y12 combined accidental poisoning by and exposure to narcotics and psychodysleptics (hallucinogens), not elsewhere classified, intentional self-poisoning by and exposure to narcotics and psychodysleptics (hallucinogens), not elsewhere classified, poisoning by and exposure to narcotics and psychodysleptics (hallucinogens), not elsewhere classified, called overdose by narcotics. Road traffic injury is included as decrease in mortality due to this category has been widely observed and often contrasted to increase in suicidal rates.9
The number of injury deaths per category were all cases in the population and these were related to population age and gender-specific numbers in the annual midyear versions of the National Registry through the study period.11 Annual crude mortality was calculated per 100 000 for the last 10 years of the study period with 95% CIs. Annual gender-specific age-adjusted mortality rates were calculated using modified World Standard as a reference. Pearson correlation coefficient were computed for annual changes during the study period. Differences were judged significant based on a two-sided test if p values were less than 0.05. The changes in rates from 1996 to 2015 were analysed by joinpoint regression model.18 The smallness of the data limited the possibility to apply complex models; however, the estimated annual changes in rate from the beginning to the end of the study period were calculated for road traffic injury, the combined categories of poisoning, suicide and event of undetermined intent, and suicide. The slopes were converted to annual percentage changes (APC) showed with 95% CI.
Patient and public involvement
No patient involved.
Results
Altogether there were 722 suicide, 195 accidental poisoning and 126 deaths due to event of undetermined intent. The crude overall suicide rate (ICD-10 codes: X60–X84) representing the last 10 years were 12.2 per 100 000 persons per year (95% CI 7.4 to 18.1). The crude overall rate for combined accidental poisoning, suicide and events of undetermined intent (ICD-10 codes: X40–X49, X60–X84 and Y10–Y34) during the same period was 14.8 per 100 000 persons per year (95% CI 9.3 to 22.1). The crude overall rate due to road traffic injuries (ICD-10 codes: V02–V89) was in comparison low 4.6 per 100 000 persons per year (95% CI 2.0 to 8.3).
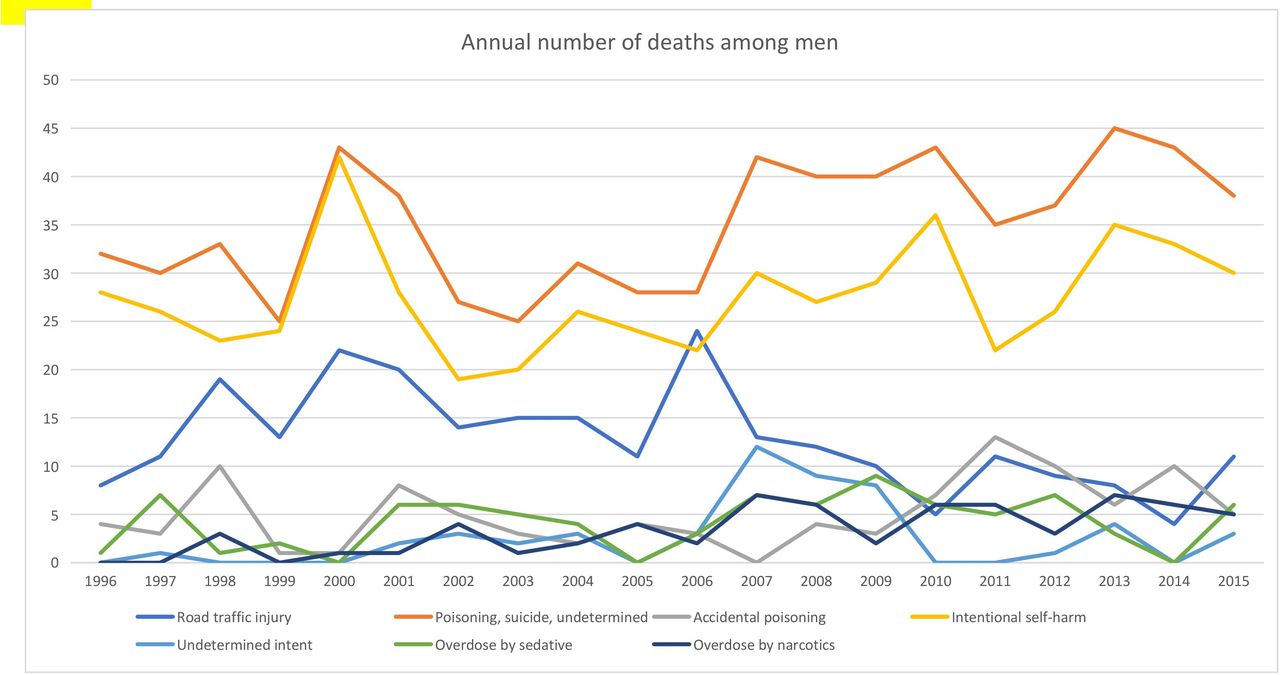
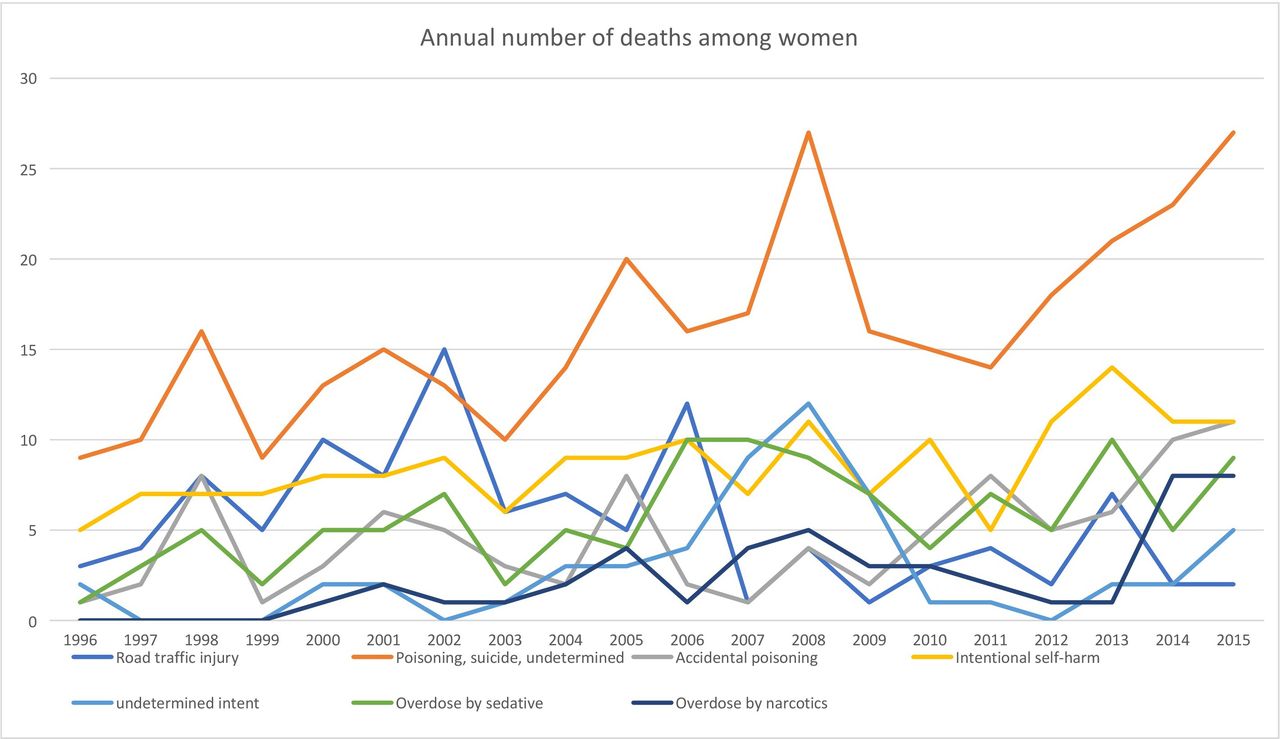
Figures 1 and 2 show the annual number of the selected categories of external causes of deaths: road traffic injuries, accidental poisoning, suicide, event of undetermined intent, these last three categories combined, overdose by sedative and overdose by narcotics in male and female, respectively, through 1996 to 2015. In some of these categories for some years there are no deaths or one or two, and overall the figures are low per category per years and varied considerably through the years obscuring trend when comparing individual years to each other.
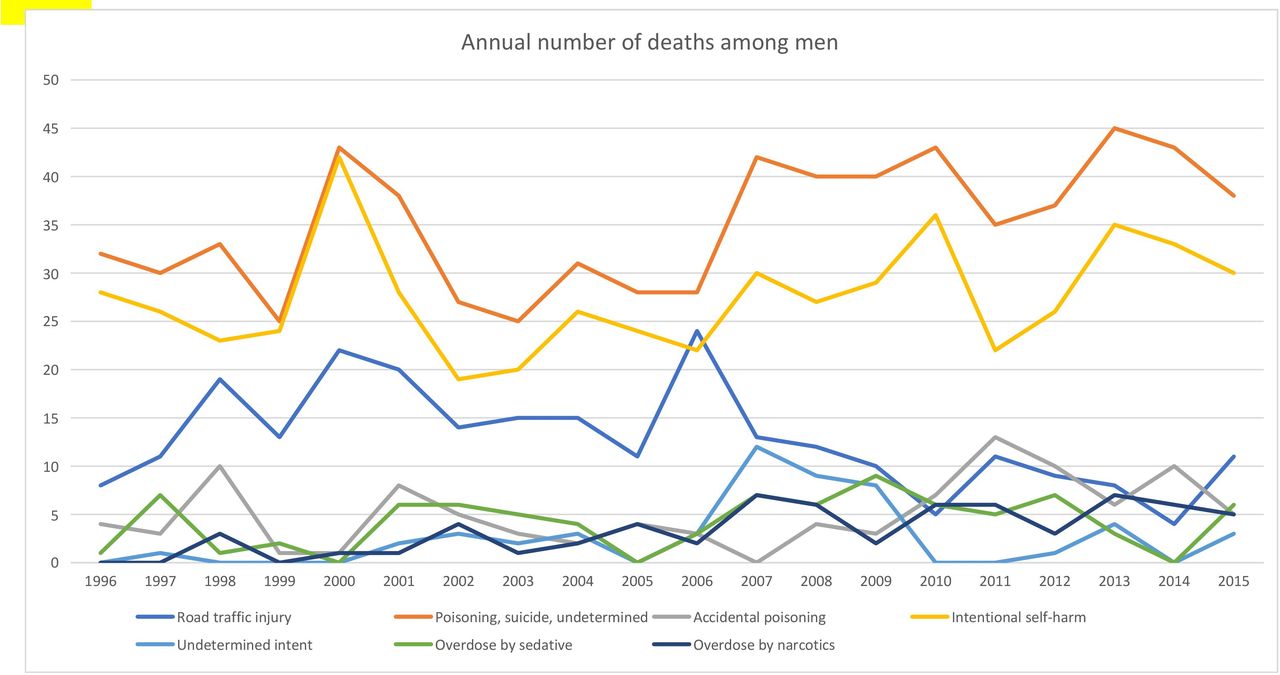
Annual number of deaths among men through the years 1996 to 2015 in the categories: road traffic injury V02–V89; poisoning, suicide and undetermined X40–X49, X60–X84, Y10–Y34; accidental poisoning X40–X49; intentional self-harm (suicide) X60–X84; event of undetermined intent Y10–Y34; overdose by sedative X41, X61, Y11 and overdose by narcotics X42, X62; Y12.

{kind=link}
{kind=link}
Annual number of deaths among women through the years 1996 to 2015 in the categories: road traffic injury V02–V89; poisoning, suicide and undetermined X40–X49, X60–X84, Y10–Y34; accidental poisoning X40–X49; intentional self-harm (suicide) X60–X84; event of undetermined intent Y10–Y34; overdose by sedative X41, X61, Y11 and overdose by narcotics X42, X62; Y12.
Table 1 shows the age standardised rates per 100 000 males per year for road traffic injuries, accidental poisoning, suicide, event of undetermined intent, these last three categories combined, overdose by sedative and overdose by narcotics. Across 1996 to 2015, rates decreased for road traffic injuries, calendar years and rates were negatively correlated, r(19)=−0.66, p=0.001. For suicide the rates also decreased however not significantly (r(19)=−0.22, p=0.36). For other categories or combined categories, the rates did not change significantly during the study period except for overdose by narcotics where the rates increased significantly (r(19)=0.72, p<0.001).
Annual age standardised rates per 100 000 people of selected external causes of deaths with Pearson correlation coefficient (r) and p-values among men
Table 2 shows the age standardised rates per 100 000 females per year for road traffic injuries, accidental poisoning, suicide, event of undetermined intent, these last three categories combined, overdose by sedative and overdose by narcotics. Similarly, as among the males across 1996 to 2015, the rates decreased for road traffic injuries, calendar years and rates were negatively correlated, however not significantly (r(19)=−0.38, p=0.09). For the separate categories of accidental poisoning, suicide and events of undetermined intent, the rates were found to increase, however not significantly, the calendar years and the rates were moderately positively correlated. For accidental poisoning, suicide and event of undetermined intent combined, the rates increased significantly (r(19)=0.60, p=0.006). The rates for overdose by sedative and overdose by narcotics increased significantly with a positive correlation, r(19)=0.49, p=0.3, and r(19)=0.67, p=0.001, respectively.
Annual age standardised rates per 100 000 people of selected external causes of deaths with Pearson correlation coefficient (r) and p-values among women
In the joinpoint regression analysis, the trend was analysed through the study period for road traffic injuries rates where the APC indicates decrease by 5.5 (95% CI −8.3 to −2.6) for men and decrease by 6.4 (95% CI −12.2 to −0.2) for women. During the same period the combined categories accidental poisoning, suicide and event of undetermined intent, the APC was increased by 0.2 (95% CI −1.1 to 1.6) for men, and the APC was increased by 2.6 (95% CI 0.9 to 4.2) for women. Corresponding for suicide, the APC was decreased by 0.7 (95% CI −2.4 to 1.1) for men and increased by 1.1 (95% CI −0.7 to 3.0) for women.
Table 3 shows the number and percentages of causes of death for accidental poisoning, intentional self-harm and event of undetermined intent during 1996 to 2015. The pattern for the categories accidental poisoning, self-poisoning and poisoning when the intent is undetermined show some similarities. However, there were some exceptions, the proportion of overdose by sedative is highest for undetermined intent, the proportion of overdose by narcotics is lower for self-poisoning than for the other two categories and the proportion of poisoning by other gases and vapours is higher for self-poisonings than for the other categories. When alcohol was involved, the proportion was highest for the category accidental poisoning followed by undetermined intent and was unusual for suicide. Hanging, strangulation and suffocation was the most common methods for suicide followed by self-poisoning and firearm. These violent methods were uncommon for undetermined intent, where poisoning were about 85%.
Number and percentages of cause of death according to death certificates: accidental poisoning, (ICD-10 codes X40–X49), intentional self-harm (suicide) (ICD-10 codes X60–X84) and event of undetermined intent (ICD-10 codes Y10–Y34) during the study period
Discussion
The suicide rates in men and women did not appear to change noticeable during the study period in Iceland. The suicide rates were approximately threefold higher in men than in women. The rates for combined accidental poisoning, suicide and event of undetermined intent increased for women, but not for men. The rates for road traffic injuries, which is based on fewer cases in the population, decreased among both genders, and significantly so for men. The rates for overdose by sedative increased among women, and the rates for overdose by narcotics increased significantly among both genders. The smallness of the population may explain some of the fluctuations of the annual rates.
The overall suicide rate reported in the present study is of similar magnitude as was seen in a previous study on suicide mortality trends in the Nordic countries.19 However, the rate is somewhat higher than in the recent reports from the UK4 and lower than reported from the USA,1 and in these studies the overall rates were calculated for the last 10 years as in the present study. In the study of the Nordic countries, the Icelandic rates stood out as the lowest suicide rates, and the Icelandic rates did not decline through the years 1980 to 2009 as was the case in most of the other countries.19 Still earlier report on suicide in Iceland showed stable suicide rates through the years 1950 to 2000.20
The decreasing trend for road traffic mortality seen in the present study has also been reported recently in several western countries, however not in all.21 This finding may indicate appropriateness of the present methodological approach of the small size data.
The increased rates of overdose by sedative and narcotics in the present study are notable and in accordance with reports from other populations.7 8
In the breakdown of the causes of death by the categories accidental poisoning, suicide and event of undetermined intent, the proportion of death due to poisoning/intoxication may be considered to show some similarities. However, there are differences between the categories, which in the light of possible misclassification, and relatively few cases, rule out firm conclusion from the figures. The causes of death for undetermined intent are dominated by poisoning while more violent causes are proportionally few as compared with causes of death reported as suicide. Some studies discuss the suicide methods in attempt to suggest possible preventive actions,19 however that was not the scope of the present study.
Strength and limitation
The use of the comprehensive population registries, such as the National Cause of Death Register and the National Registry strengthens the study. Only one version of the classification of cause of death, namely the ICD-10, was used during the study period; however, the registration of cause of death depends on different attesting persons. Death certificates in Iceland are issued by a physician. If the deceased person’s physician is not able to attest the cause of death, or in cases where the circumstances of the death are unexplained, unusual, suspicious, due to intoxication or following an accident, the death is reported to the police and the medical examiner, who decides whether to arrange for an autopsy and forensic investigations before the death certificate is issued.16 The quality of death registration at a global level have been studied, and the data from Iceland were evaluated as high overall and ranked in the same category as data from 23 developed countries, including the USA and the UK.10
The small material and the distribution according to gender and calendar years across study period of 20 years is an obvious drawback; however, the registries ensure the completeness of the data. The age groups available were rather crude and the low numbers in some of the ICD-10 categories preclude meaningful detailed description of the mortality according to age groups.
Injury, poisoning and certain other consequences of external cause according to ICD-10, that is codes S00 to T98, particularly concerning poisoning by drugs, medicaments and biological substances would have given different and perhaps more precise information. However, these codes were not available from the website of Statistic Iceland.15
Conclusions
The suicide rates in Iceland have not changed during 1996 to 2015; however, the rates for the combined accidental poisoning, suicide and event of undetermined intent increased significantly for women. The rise of the overdose rates for sedative among women and for narcotics among both genders is according to the increase in rates of prescription and non-prescription drug overdose deaths reported elsewhere.
Footnotes
Contributors OSG and VR contributed to the conception and design, VR obtained the data and conducted the analyses, OSG and VR interpreted the data, drafted the article and revised it, and approved the final version of the submitted manuscript.
Funding The study was supported by grant from Landspítali–the National University Hospital Research Fund, grant number 311055-2249.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Data Protection Commission and the National Bioethics Committee (VSNb2019040011/03.03) approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All basic data available from the website of Statistic Iceland.