Article Text

Abstract
Objectives Two oral targeted therapies, gefitinib and erlotinib, were first approved and then launched into the market for treatment of late-stage non-small cell lung cancer (NSCLC) in Taiwan in 2003 and 2006, respectively. The aim of this study were to determine the trends in lung cancer burden and examine changes in lung cancer-related survival rates and mortality following the launch of these new drugs.
Setting Yearly lung cancer-related data (1994–2013), including incidence, number of newly diagnosed patients, survival rate and mortality, were retrieved from the Taiwan Cancer Registry Database.
Design and outcome measures Using a time series design with autoregressive integrated moving average model, we investigated and projected trends in the incidence and early diagnosis of lung cancer in Taiwan. We also estimated the changes in survival rates and mortality following the launch of targeted therapies using interrupted time series and segmented regression models.
Results The age-standardised incidence of lung cancer increased from 22.53 per 100 000 people in 1994 to 34.09 in 2013, and it was projected to reach 38.98 by 2020. The rate of early-stage NSCLC at diagnosis increased from 12.63% in 2004 to 23.99% in 2013, and it was projected to reach 32.95% by 2020. The 2-year lung cancer survival increased by 19.81% (95% CI 14.90% to 24.71%) 3 years following the launch of gefitinib. Lung cancer mortality declined by 5.97% (95% CI −8.20% to −3.73%) 3 years following the launch of gefitinib.
Conclusions Lung cancer survival rate increased and mortality decreased significantly following the launch of gefitinib and erlotinib in Taiwan.
- targeted therapies
- lung cancer
- incidence
- survival rate
- mortality
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study examined the long-term trends in yearly incidence, the rate of early-stage lung cancer at diagnosis, survival rate and mortality of lung cancer.
Long-term data from the Taiwan Cancer Registry Database were used in this study.
A time series design was used to project the incidence and the rate of early-stage lung cancer at diagnosis.
An interrupted time series design was applied to estimate the changes in survival rates and mortality following the launch of targeted therapies.
This study did not use patient-level data to separate patients by lung cancer subtypes and disease severity.
Introduction
Lung cancer is the leading cause of cancer deaths worldwide.1 Globally, around 1.82 million new patients were diagnosed with lung cancer (12.9% of all cancer diagnoses), and around 1.59 million patients died (19.4% of all cancer mortalities) in 2012.2 The incidence was 23.1 per 100 000 people, and mortality was 19.7 per 100 000 people in 2012,2 which has increased over time.1–3 In the USA, approximately 214 000 new cases of lung cancer (13.3% of all cancer diagnoses) and 168 000 deaths due to lung cancer (27.2% of all cancer mortalities) were estimated in 2012.3
In Taiwan, lung cancer is also one of the most commonly diagnosed cancers as well as the leading cause of cancer deaths. Approximately 12 462 new cases of lung cancer (12.1% of all cancer diagnoses) and 9167 deaths (19.9% of cancer deaths) were projected to occur in Taiwan in 2014.4 About 85% of all lung cancers are identified as non-small cell, and approximately 75% of these are metastatic or advanced at diagnosis, for which no curative treatment is available.5–8 Given most patients are diagnosed with advanced stage diseases, it is considered a terminal illness with a 5-year survival rate of less than 15%.9–11
Oral targeted therapies for non-small cell lung cancer (NSCLC) were launched into the market for patients with epidermal growth factor receptor (EGFR) mutation in Taiwan in 2003 (gefitinib) and in 2006 (erlotinib). These EGFR molecular targeted drugs, gefitinib and erlotinib, were initially approved as third-line or second-line therapy for patients with advanced NSCLC because of their therapeutic benefits, as suggested by randomised clinical trials.12–14 The recent National Comprehensive Cancer Network (NCCN) guideline15 recommends gefitinib and erlotinib as the first-line therapy for EGFR mutation-positive patients with advanced NSCLC based on accumulating evidence showing a significant association between mutated EGFR and the clinical benefits of gefitinib and erlotinib.16–18 In light of rapid disease progression, timely access to pharmaceutical innovations such as targeted therapies is vital to patients with NSCLC. The new targeted therapies, gefitinib and erlotinib, have been reimbursed by Taiwan’s National Health Insurance since 2004 and 2007, respectively, for patients with NSCLC who meet the above requirements based on evidence and clinical need.
Little is known about the effects of the introduction of new targeted therapies in Taiwan. This study is one of the first to address the gap by examining the changes in lung cancer-related survival rates and mortality following the launch of gefitinib and erlotinib.
Method
Data sources
We obtained data from 1994 to 2013 related to the lung cancer burden in Taiwan from the Taiwan Cancer Registry Database, which were compiled by the Health Promotion Administration, Ministry of Health and Welfare, Taiwan.19 The data include yearly incidence and mortality for various cancer types by age, gender and administrative division. Survival rates within several years of diagnosis of various cancer types are also available from the database.
Through the routine cancer case notification reminders and collection procedures each year, the sources of possible cancer cases and the cancer registration declaration database are combined. Health Promotion Administration calculates the completeness of cancer registration declarations in each year, approximately 98.44% in 2016.20 In addition, in accordance with the practice of the International Agency for Research on Cancer, percentage of death certificate only cases (DCO%) and percentage of morphologically verified cases (MV%) are used as quality indicators of the reporting data. In 2016, as a result of the data collection and comparison, the DCO% was 0.91%, indicating that the coverage of the registration system was complete and the data quality in the system was consistent. In the same year, the MV% of all cancer cases was 92.23%, that of men was 90.79% and that of women was 93.89%, indicating that the diagnosis of cancer cases was accurate.20 Use of these data for research purposes is exempt from review by the Institutional Review Board of the National Cheng Kung University Hospital in Taiwan.
Measurements
To examine the trends in lung cancer incidence, we collected the yearly number of new patients, crude incidence (per 100 000 people) and age-standardised incidence (per 100 000 people) of lung cancer by gender from 1994 to 2013. The global population in year 2000 was used to calculate the age-standardised incidence.21 In addition, the yearly total of new patients with lung cancer (small cell lung cancer (SCLC) and NSCLC) according to stages at diagnosis was collected, and we calculated the rates of early-stage lung cancer over time. Diagnostic stages from 0 to 2 were considered as early stage, and stages 3 and 4 were categorised as late stage.
To evaluate the impacts of the launch of targeted therapies, 1-year and 2-year lung cancer survival rates by gender from 1994 to 2013 were collected. Furthermore, we collected the yearly number of deaths, the crude mortality (per 100 000 people) and the age-standardised mortality (per 100 000 people) for lung cancer by gender from 1994 to 2013.
Statistical analysis
To assess the yearly changes in lung cancer burden using the age-standardised incidence and rate of early-stage lung cancer at diagnosis as defined above, we used a time series design with the autoregressive integrated moving average (ARIMA) model, which was developed by Box and Jenkins.22 The model is generally referred to as an ARIMA(p,d,q) model, where parameters p, d and q are non-negative integers that refer to the order of the autoregressive, integrated and moving average parts of the model, respectively. These models are fitted to time series data either to better understand the data or to determine points in the series.23 We used the estimated rates from the ARIMA model for time series graphs.
To determine the effects of the launch of new targeted therapies for lung cancer on clinical outcomes, we also estimated the changes in the lung cancer-related 1-year and 2-year survival rates and age-standardised mortality following the launches of gefitinib and erlotinib using interrupted time series and segmented regression models, a strong quasiexperimental method.24–26 The method can provide strong evidence of causal effects because it takes into consideration the question of whether an intervention causes abrupt and measurable interruptions in a pre-existing trend.24 27 We used segmented linear regression models to estimate the effects of the launch of new targeted therapies on changes in the level and trend of both survival rates and age-standardised mortality.28 The basic model included terms to estimate the baseline level for each outcome (intercept) (β0), baseline trend (slope) (β1), changes in the level immediately after the drug launch (β2) and changes in the trend after the drug launch (β3) (see the following equation).24 29

The models also controlled for autocorrelation.30 To identify the most parsimonious models, we used backward elimination and excluded non-significant terms (p>0.05).
All analyses were carried out with SAS software V.9.4 (SAS Institute).
Patient and public involvement
Patients and the public were not involved in the design or planning of the study.
Results
Table 1 presents the past trends (1994–2013) and future projections (2014–2020) of the age-standardised incidence of lung cancer by gender in Taiwan. The overall age-standardised incidence of lung cancer increased from 22.53 (per 100 000) in 1994 to 34.09 in 2013, and it was projected to reach 38.98 by 2020 based on the trend during 1994–2013. By gender, the age-standardised incidence for males increased from 30.11 (per 100 000) in 1994 to 43.01 in 2013, and it was projected to reach 48.11 by 2020; the age-standardised incidence for females increased from 13.82 (per 100 000) in 1994 to 26.16 in 2013, and it was projected to reach 31.57 by 2020.
1994–2013 trends and 2014–2020 forecast of incidence of lung cancer in Taiwan
Table 2 shows the past trends (1994–2013) and future projections (2014–2020) of the rate of early-stage lung cancer by type of lung cancer in Taiwan. The rate of early-satgeNSCLC at diagnosis grew rapidly from 12.63% in 2004 to 23.99% in 2013, and it was projected to reach 32.95%, based on the trend during 1994–2013. In contrast, the rate of early-stage SCLC at diagnosis declined from 4.78% in 2004 to 4.10% in 2013 and was projected to reach 3.11% by 2020.
2004–2013 trends and 2014–2020 forecast of the rate of early-stage lung cancer at diagnosis in Taiwan
Survival rate following the launch of gefitinib
Table 3 details the parameter estimates from the segmented regression models of changes in the lung cancer survival rate following the launch of targeted therapies. Overall, 1-year and 2-year survival rates increased by 10.18% (95% CI 6.77% to 13.59%) and 19.81% (95% CI 14.90% to 24.71%) 3 years following gefitinib’s launch in 2003 (see figure 1). Among men, 1-year and 2-year survival rates increased by 10.70% (95% CI 9.34% to 12.06%) and 14.25% (95% CI 3.27% to 25.24%); and among women, 1-year and 2-year survival rates increased by 14.82% (95% CI 6.92% to 22.71%) and 31.12% (95% CI 15.64% to 46.60%) (table 3) (figure 1).
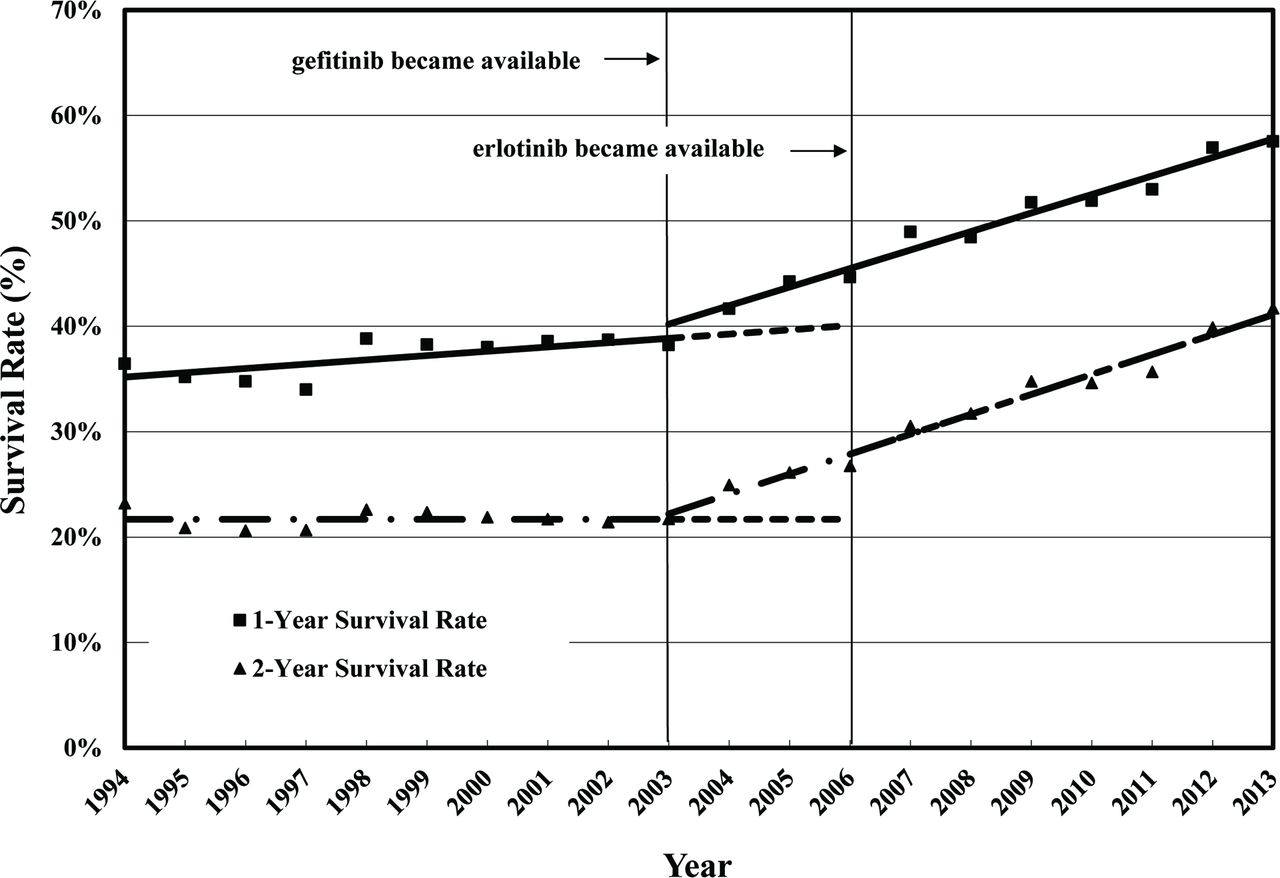
Yearly lung cancer survival rates in Taiwan (1994–2013).
Estimated changes in lung cancer survival rates following the launch of targeted therapies (gefitinib and erlotinib) using interrupted time series and segmented regression models
Survival rate following the launch of gefitinib and erlotinib
Overall, there were no significant changes in 1-year and 2-year survival rates 3 years following gefitinib and erlotinib’s launch. Figure 1 shows the 1-year and 2-year survival rates of lung cancer in Taiwan over time. Among men, 1-year and 2-year survival rates did not change; however, 1-year and 2-year survival rates reduced by 13.34% (95% CI −20.48% to −6.20%) and 11.77% (95% CI −22.36% to −1.18%) among women.
Mortality following the launch of gefitinib
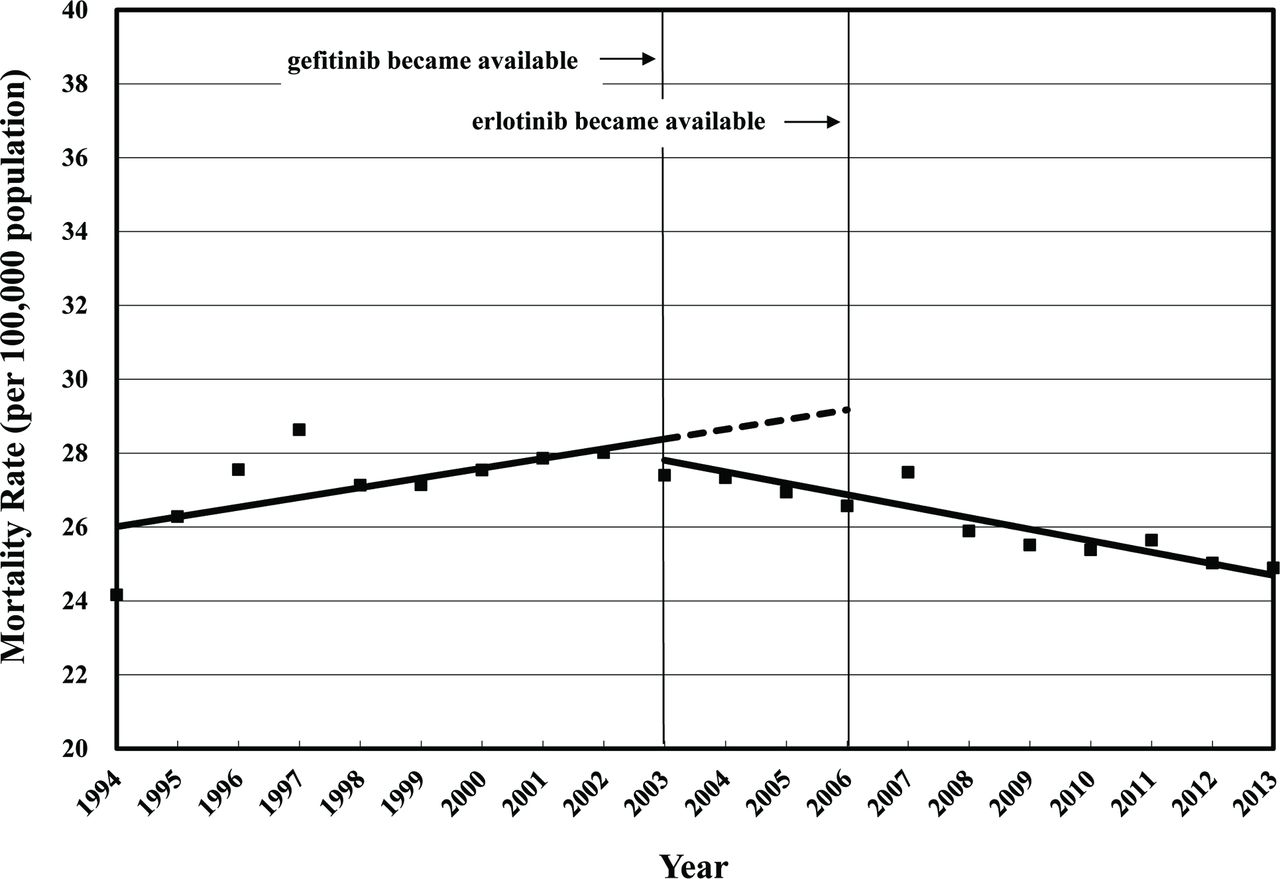
Table 4 presents the parameter estimates from the segmented regression models of changes in the lung cancer mortality following the launch of targeted therapies. Overall, mortality decreased by 5.97% (95% CI −8.20% to −3.73%) 3 years following gefitinib’s launch in 2003 (see figure 2). Among men, mortality reduced by 5.40% (95% CI −10.08% to −0.73%), and among women, mortality decreased by 4.38% (95% CI −7.50% to −1.25%) (table 4) (figure 2).
{kind=link}
{kind=link}
Yearly lung cancer mortality in Taiwan (1994–2013).
Estimated changes in lung cancer mortality following the launch of targeted therapies (gefitinib and erlotinib) using interrupted time series and segmented regression models
Mortality following the launch of gefitinib and erlotinib
Overall, there were no significant changes in lung cancer mortality 3 years following the launch of gefitinib and erlotinib in 2006. Figure 2 shows the overall lung cancer mortality in Taiwan over time. Among men, mortality reduced by 7.20% (95% CI −9.69% to −4.71%) but mortality did not change significantly for women.
Discussion
This study projected 7 years (2014–2020) of lung cancer incidence in Taiwan based on the observed incidence from 1994 to 2013 (20 years). We also projected rates of early-stage lung cancer at diagnosis for 2014 through 2020 based on the past trends. Furthermore, the present study is the first study to examine the national trend in lung cancer survival rates and mortality following the introduction of targeted therapies in Taiwan using an interrupted time series design.
We estimated an ongoing gradual increase in the age-standardised incidence of lung cancer for both men and women in Taiwan. According to our results, the overall incidence of lung cancer in Taiwan (35.4 per 100 000) was lower than that in the USA (38.4) and Canada (37.9) in 2012, but it was higher than that in the UK (30.0), Australia (27.0), Japan (24.6) and South Korea (28.7).31 Between 1994 and 2013, the age-standardised rate steadily increased by 42.84% for men and by 89.29% for women, and there was an estimated overall 51.31% growth rate (table 1). According to these trends, incidence would reach 48.11 per 100 000 for men and 31.57 per 100 000 for women by 2020. Our findings showing these increasing trends are similar to those of previous studies32 33 investigating earlier trends (up to 2008) in Taiwan. However, decreasing trends for both men and women in other countries have been observed. For example, lung cancer incidence decreased for both men and women in the USA (2004–2009),34 China (1997–2005 for men and 2001–2005 for women),35 Hong Kong (1983–2000)36 and Singapore (1980–2007).37 The incidence decreased for men but increased for women in the Czech Republic (1984–1998).38 Previous studies have provided evidence of a reduction in the prevalence of smoking following smoking bans.39–41 Lung cancer in non-smokers can be caused by exposure to radon gas, secondhand smoke, air pollution or other factors in addition to workplace exposure to asbestos, diesel exhaust or specific other chemicals that can also cause lung cancers in some people who do not smoke.42 43 It is important to identify key drivers (other than smoking) of these increasing trends in Taiwan.
The incidence of lung cancer in Taiwan has increased over time and the rate of early-stage NSCLC at diagnosis gradually increased, but the ratio was still low (less than 25%) until 2013, and the rate of early-stage SCLC at diagnosis has remained very low (less than 5%) without a significant increase. There are almost no symptoms at the initial stage of lung cancer, thus, it is difficult to detect it early.44 However, the National Lung Screening Trial45 conducted by the National Institutes of Health in the USA found that the use of low-dose CT in high-risk groups for lung cancer could detect tumours earlier and reduce mortality by 20%. Hence, the NCCN guideline recommends screening for people who smoke more than one pack of cigarettes a day, have smoked for more than 30 years, have quit smoking for less than 15 years or are 55–74 years old.46 The Taiwan Lung Cancer Society followed the NCCN guidelines and announced, in 2015, an expert consensus to further improve the early diagnosis rate. Early diagnosis through lung cancer screening might improve in the upcoming years.
For many years only chemotherapies were available for treatment of lung cancer. Then, the first targeted therapy, gefitinib, was approved for marketing in 2003, followed by the second targeted therapy, erlotinib, which became available in 2006. Compared with chemotherapies, most clinical trials have shown that when these two targeted drugs were used as the first line of treatment for advanced NSCLC with EGFR mutations, overall survival did not increase significantly, although progression-free survival increased significantly by 3–8 months.16 47–50
We used real-world data to examine changes in lung cancer survival and mortality following the launch of these two targeted therapies in Taiwan. Gefitinib and erlotinib were reimbursed by Taiwan’s National Health Insurance soon after marketing approval and their utilisation has increased rapidly over time. Our study of gefitinib and erlotinib prescribing trends during 2004–201351 found that the number of patients using gefitinib increased from 228 (5.48% of all patients using antineoplastic agents) in 2004 to 5558 (38.08%) in 2013; and the number of patients using erlotinib increased from 499 (8.44%) in 2007 to 2984 (20.44%) in 2013. Using rigorous research methods, the current study found that the 1-year survival rate increased by about 10%, and the 2-year survival rate increased by about 20% in both men and women 3 years after the first targeted therapy (gefitinib) was launched. However, the subsequent survival rate did not change markedly after the launch of the second targeted therapy (erlotinib) because it is not a so-called ‘breakthrough innovation’, as was the case for the first targeted therapy. Together, findings from our prior and current studies suggest improved lung cancer survival and mortality following the launch of the first two targeted therapies and their increased use in Taiwan.
This study also estimated the age-standardised mortality of lung cancer for both men and women in Taiwan. We found that the overall mortality of lung cancer in Taiwan (25.0 per 100 000) was lower than that in the USA (28.6), Canada (28.4) and the UK (25.4) in 2012, but it was higher than that in South Korea (21.3), Australia (18.5) and Japan (17.4).31 The mortality of lung cancer increased from 1994 to 2003 and decreased from 2003 to 2013 in Taiwan. However, it has gradually increased in Japan, has remained steady in Canada and Australia and has decreased in the USA and the UK.51 52
The present study also found that mortality for both men and women was approximately 5% lower than expected 3 years following the launch of gefitinib. However, mortality for men was 7% lower than expected 3 years following the launch of the second drug, erlotinib, without changes in mortality detected for women. Before the molecular testing of EGFR was established, the indication of gefitinib was considered mainly by using four factors: adenocarcinoma, non-smoker, Asian and female. It is possible that male patients gained more benefits after the molecular testing became routine practice in the clinic.
There are some limitations to this study. First, targeted therapies are only appropriate for patients with advanced NSCLC and EGFR mutation. Patients with advanced NSCLC account for about 64% of overall patients with lung cancer in Taiwan.5–8 Among them, approximately 40%–50% of patients have EGFR mutation. This study found improved lung cancer survival and mortality following the launch of targeted therapies, gefitinib and erlotinib. However, improvements in survival and mortality related to lung cancer may be due to other factors. Other diagnosis and treatment factors, including the availability and use of diagnostic tools (such as molecular testing), earlier diagnosis, sequential or combination treatment strategies, personalised care, multimodality care, palliative care support and psychological support, have roles in outcome improvements. Other factors, including patient’s living habits and the global management of patients with cancer, may also contribute to the improvement in outcomes. Further studies considering these factors are needed. Second, pemetrexed, a cytotoxic chemotherapy, has been approved in Taiwan since 2004. Pemetrexed is indicated for non-squamous NSCLC, broader than EGFR-mutated NSCLC, thus, it could affect the mortality of lung cancer specially after the approval of the platinum-pemetrexed combination therapy in 2008. We did not have data on pemetrexed in this study to examine the survival or mortality of lung cancer in Taiwan following the launch of pemetrexed. However, based on our previous study53 of prescribing trends of antineoplastic agents in Taiwan, the prescription rate of folic acid analogues (including pemetrexed) during 2009–2012 remained steady (prescription rate from 16.7% to 17.13%; growth rate of market share: 0.43%). Finally, we did not examine survival and mortality by lung cancer subtypes following the launch of targeted therapies. We did not have patient-level data to separate patients by lung cancer subtypes (NSCLC or SCLC) and disease severity (cancer stages). This study used data from the Taiwan Cancer Registry Database to estimate the two diagnostic indicators of lung cancer (incidences and rate of early-stage cancer at diagnosis) over time, and to evaluate changes in the two clinical indicators (survival rates and mortality) after the launch of targeted therapies. Notwithstanding these limitations, this study should provide an important basis for additional research.
Conclusion
In summary, our findings suggest that the incidence of overall lung cancer and rate of early-stage NSCLC at diagnosis increased in the past and that this trend is likely to continue in the future. Importantly, this study found that the survival rate and mortality of patients with lung cancer improved in Taiwan following the launch of targeted therapies (especially the initial one, gefitinib). However, further research is warranted to determine if these results are applicable to specific subtypes and stages of lung cancer.
References
Footnotes
Contributors JCH, CFW and SCY conceptualised and designed the study. PCL and YCL provided suggestions for the research design from a clinical perspective. CFW collected data, performed the analyses and drafted the manuscript. JCH and CYL reviewed all data and revised the manuscript critically for intellectual content. All authors approved the final version for submission.
Funding This work was supported by Taiwan Ministry of Science and Technology grants (grant numbers: MOST 104-2320-B-006-005, MOST 106-2320-B-006-039).
Disclaimer The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Use of data from the online Taiwan Cancer Registry Database for research purposes is exempt from review by the Institutional Review Board in Taiwan because the data used are public and aggregated population-level information.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article. The authors obtained nationwide data from 1994 to 2013 (20 years) related to the lung cancer incidence in Taiwan from the Taiwan Cancer Registry Database, compiled by the Health Promotion Administration, Ministry of Health and Welfare, Taiwan.