Article Text

Abstract
Introduction The peripheral nerves of patients with diabetes are often pathologically swollen, which results in entrapment at places of anatomical narrowing. This results in nerve dysfunction. Surgical treatment of compression neuropathies in the lower extremities (lower extremity nerve decompression (LEND)) results in relief of symptoms and gain in peripheral nerve function, which may lead to less sensory loss (short term) and less associated detrimental effects including foot ulceration and amputations, and lower costs (long term). The aim of the DeCompression trial is to evaluate the effectiveness and (cost-)effectiveness of surgical decompression of compressed lower extremity nerves (LEND surgery) compared with patients treated with conventional (non-surgical) care.
Methods and analysis A stratified randomised (1 to 1) controlled trial comparing LEND surgery (intervention) with conventional non-surgical care (control strategy) in subjects with diabetes with problems of neuropathy due to compression neuropathies in the lower extremity. Randomisation is stratified for participating hospital (n=11) and gender. Patients and controls have the same follow-up at 1.5, 3, 6, 9, 12, 18, 24 and 48 months. Participants (n=344) will be recruited in 12 months and enrolled in all affiliated hospitals in which they receive both the intervention or conventional non-surgical care and follow-up. Outcome assessors are blinded to group assignment. Primary outcome: disease-specific quality of life (Norfolk Quality of Life Questionnaire—Diabetic Neuropathy). Secondary outcomes: health-related quality of life (EuroQoL 5-dimension 5-level (EQ-5D5L), 36-item Short Form (SF-36)), plantar sensation (Rotterdam Diabetic Foot Test Battery), incidence of ulcerations/amputations, resource use and productivity loss (Medical Cost Questionnaire, Productivity Cost Questionnaire) during follow-up. The incremental cost-effectiveness ratio will be estimated on the basis of the collected empirical data and a cost-utility model.
Ethics and dissemination Ethics approval has been granted by the Medical Research Ethics Committee of Utrecht University Medical Center (reference: NL68312.041.19v5, protocol number: 19-335/M). Dissemination of results will be via journal articles and presentations at national and international conferences.
Trial registration number NetherlandsTrial Registry NL7664.
- diabetic neuropathy
- plastic & reconstructive surgery
- neurosurgery
- diabetic foot
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
First randomised controlled trial on bilateral lower extremity nerve decompression surgery with proper control group.
Substantial 4 years of follow-up to study long-term outcomes (ie, ulcer and amputation incidence).
First randomised controlled trial using cost effectiveness as endpoint.
It is not feasible to blind the patients for the allocated treatment. Sham surgery is considered unethical.
Introduction
Current non-surgical care does not have satisfying treatments for the tingling, burning, electrical and painful symptoms of neuropathy and patients have nowhere to go when seeking treatment for the concomitant numbness in their feet. Refractory to therapies like antidepressants and anticonvulsants, symptoms are not treated to satisfaction and the numbness is sadly observed. Neuropathy lowers the quality of life and precedes diabetic foot disease.1–3 Up to 60% of patients with diabetes will be confronted with neuropathy. It has been estimated that the incidence of diabetic foot ulcers (DFUs) at some point during the disease is about 15%.4 DFUs precede 8 out of 10 non-traumatic amputations and the all-cause mortality rate after 5 years is 39%–80%.5–7 This is equivalent to the mortality rates of lung and colorectal cancers.8
The costs for society are sizeable: the average cost for a DFU episode is US$10 827.9 10 In the Netherlands, over one million people have diabetes and the incidence (2.8–3.5/1000 inhabitants) is still rising. In line with aims and priorities defined by the International Working Group on the Diabetic Foot (IWGDF), more effective treatments for our diabetic population are urgently needed. It is now acknowledged that many patients with symptoms of neuropathy also have localised nerve compressions, which contribute to the symptoms.11 Nerves in the legs and feet also suffer from this phenomenon, which are treated surgically by releasing the nerve from the site of compression. In this way, blood flow in the nerve is restored and processes of nerve regeneration are allowed, which relieves symptoms and may consequently result in gain of sensory function.12 It is assumed that these patients have a lower risk of falls, foot ulceration and consequent lower extremity amputations. Current series report considerable pain relief of >4 points (0–10 on a Visual Analogue Scale), occurring in 91% of patients and sensibility improvement in 69% of patients. Health-related quality of life (HRQoL) was still significantly improved in six out of eight SF-36 domains at 24 months and low perioperative and postoperative complication rates are reported (pooled wound dehiscence rate of 15%).13 14
However, no high-quality real-world data exist in which lower extremity nerve decompression (LEND) surgery is compared with conventional, non-surgical care in the diabetic neuropathy population.15–17 Since conventional non-surgical care for the patient with neuropathy outnumbers current practices compared with surgical management of entrapped lower extremity nerves, but the latter having increasingly positive evidence, it is meaningful to further investigate differences in outcomes in a randomised controlled setting.
Research aim and objectives
The aim of the DeCompression (DECO) study is to further investigate the effectiveness and cost effectiveness of LEND surgery.
Methods and analysis
Patient and public involvement
Both a patient panel and patient federation (Patienten Vereniging Nederland) were involved in the design of the study.
Study design and settings
This study is a multicentre, randomised controlled trial (RCT) in which patients with symptomatic neuropathy and bilateral compression neuropathies of the posterior tibial nerve at the tarsal tunnel will be allocated into decompression surgery versus non-surgical follow-up. Additional compression neuropathies of the lower extremity will also be assessed (tibial nerve at soleal sling, common peroneal nerve at the fibular head, superficial peroneal nerve and deep peroneal nerve) and decompressed when in the surgical group.
The study will be performed in 11 centres in the Netherlands: Utrecht Medical University Center, Utrecht; Diakonessen Hospital, Utrecht; Franciscus Gasthuis & Vlietland Hospital, Rotterdam; Maasstad Hospital, Rotterdam; Jeroen Bosch Hospital, ‘s Hertogenbosch; Isala Hospital, Zwolle; OLVG Hospital, Amsterdam; Amsterdam University Medical Center, AMC, Amsterdam; Amsterdam University Medical Center, VUmc, Amsterdam; Antonius Hospital, Nieuwegein and Meander Medical Center, Amersfoort.
Patient selection
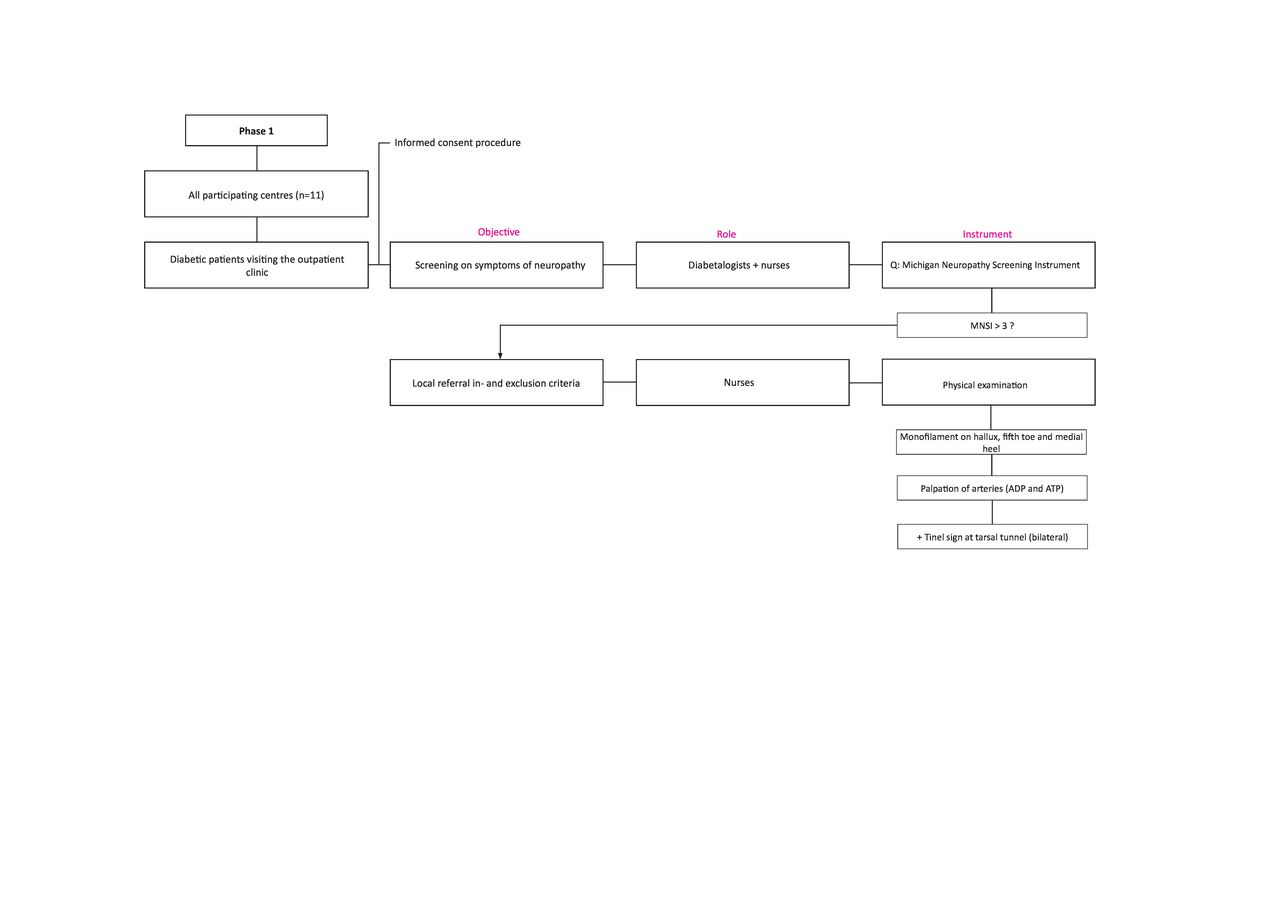
Eligible for participation are all adult patients with diabetes with symptoms of neuropathy in the lower extremities who are visiting the outpatient clinics of the participating hospitals (figures 1–4). The study population concerns patients with type 1 or 2 diabetes with neuropathy symptoms (30%–60% of patients with diabetes) and with signs of superimposed nerve compressions in the leg (up to 35%).18 Of paramount importance is to define how severe the degree of sensory loss is, as measure of peripheral nerve function and to estimate the likelihood of successful surgery.17 19 20 Additional inclusion and exclusion criteria are shown in box 1.
Inclusion and exclusion criteria.
In order to be eligible to participate in this study, a subject must meet all of the following criteria:
Having diabetes mellitus (type 1 or 2).
Patients (>17 and <76 years old).
Symptoms of neuropathy (assessed with the Michigan Neuropathy Screening Instrument, scoring >3).
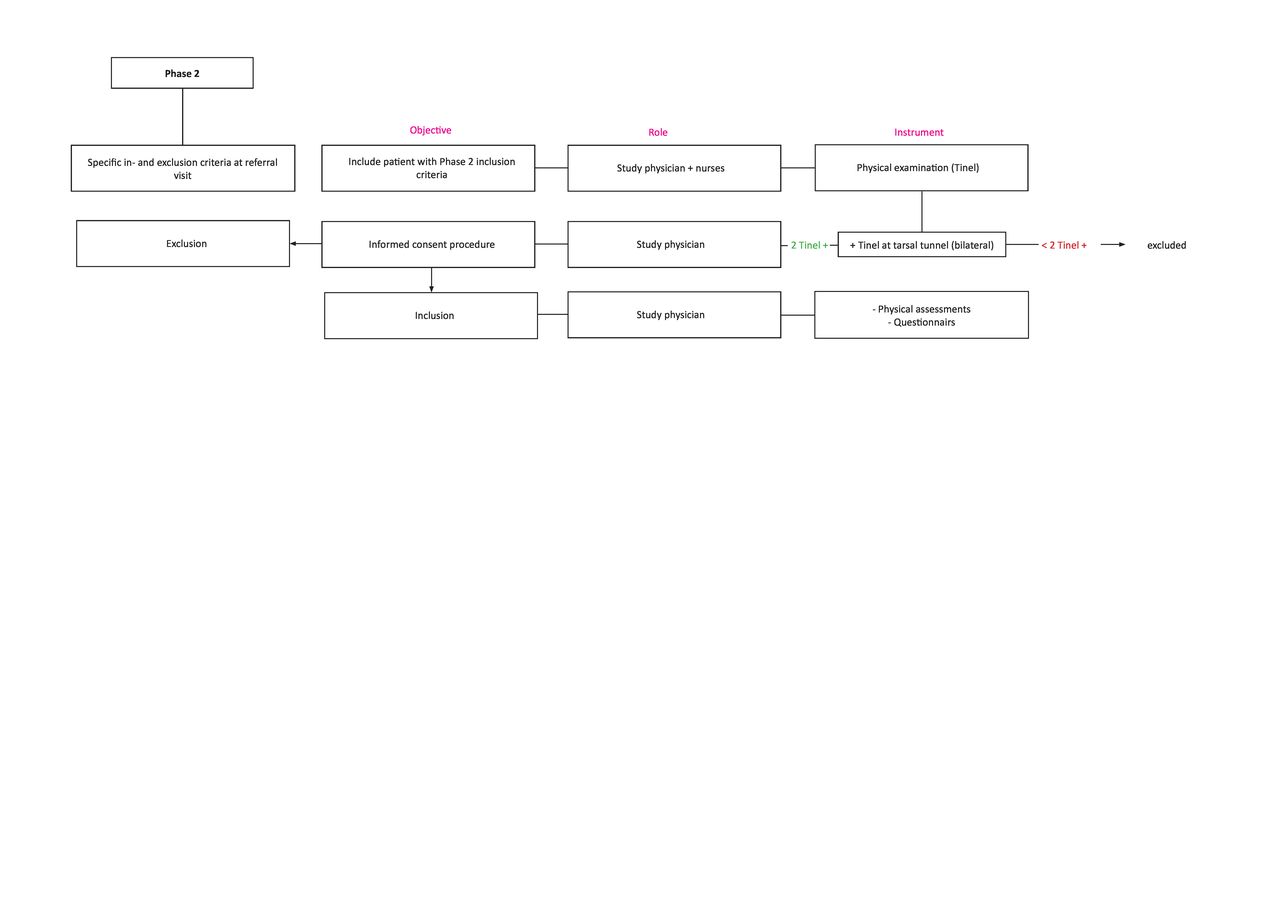
A bilateral Tinel sign at the tarsal tunnel (posterior tibial nerve).
Sufficient circulation to heal lower extremity incisions (by palpating the peripheral arteries of the foot: a palpable dorsal pedis artery or posterior tibial artery is needed). In case of non-palpable arteries, a pedal Doppler arterial waveform is evaluated. A toe brachial index (≥0.75) is performed when the Doppler signal is not triphasic.
Minimal or controlled pedal oedema (assessed with inspection and physical examination).
Being fit for surgery.
Compliant with instructions for their own care.
Intact protective sensation (cutaneous threshold <10 g monofilament) at the plantar side of the foot (plantar hallux and fifth toe).
Written informed consent.
A potential subject who meets any of the following criteria will be excluded from participation in this study:
Diabetic foot ulcer(s) or amputation(s) in history, active radicular syndrome or neurological disease interfering with sensation of the feet, as assessed in the interview and screening questionnaire (eg, HIV and chemotherapy-induced neuropathy).
Previous surgery at lower extremity nerve compression sites.
Active Charcot foot.
Not able to understand written and oral instructions (ie, insufficient command of Dutch language).
Being incompetent (incapacitated).
Current enrolment in a clinical trial which involves surgery of the lower extremity or medical drug trials investigating the effects on neuropathy symptoms.
Glycated hemoglobin (HbA1c) level >11% at baseline.
Pregnant women.

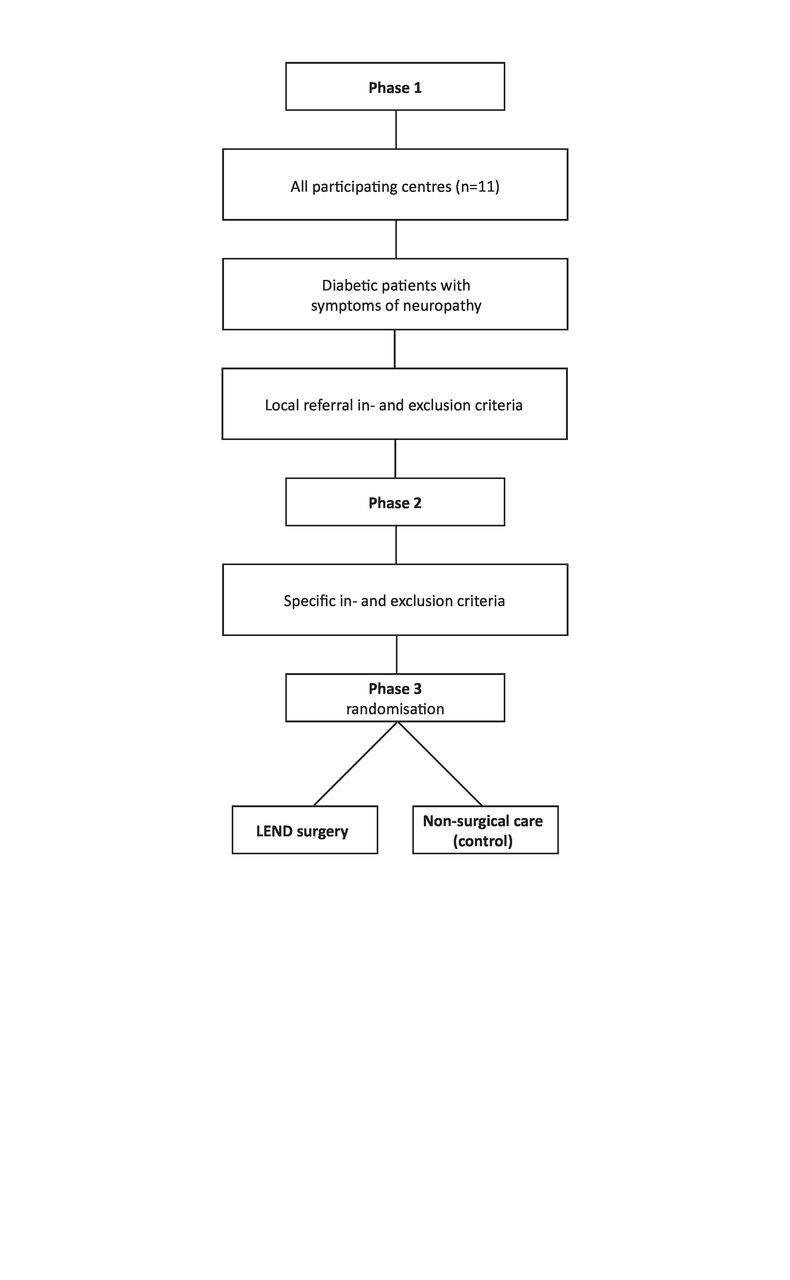
Study flow chart. LEND, lower extremity nerve decompression.
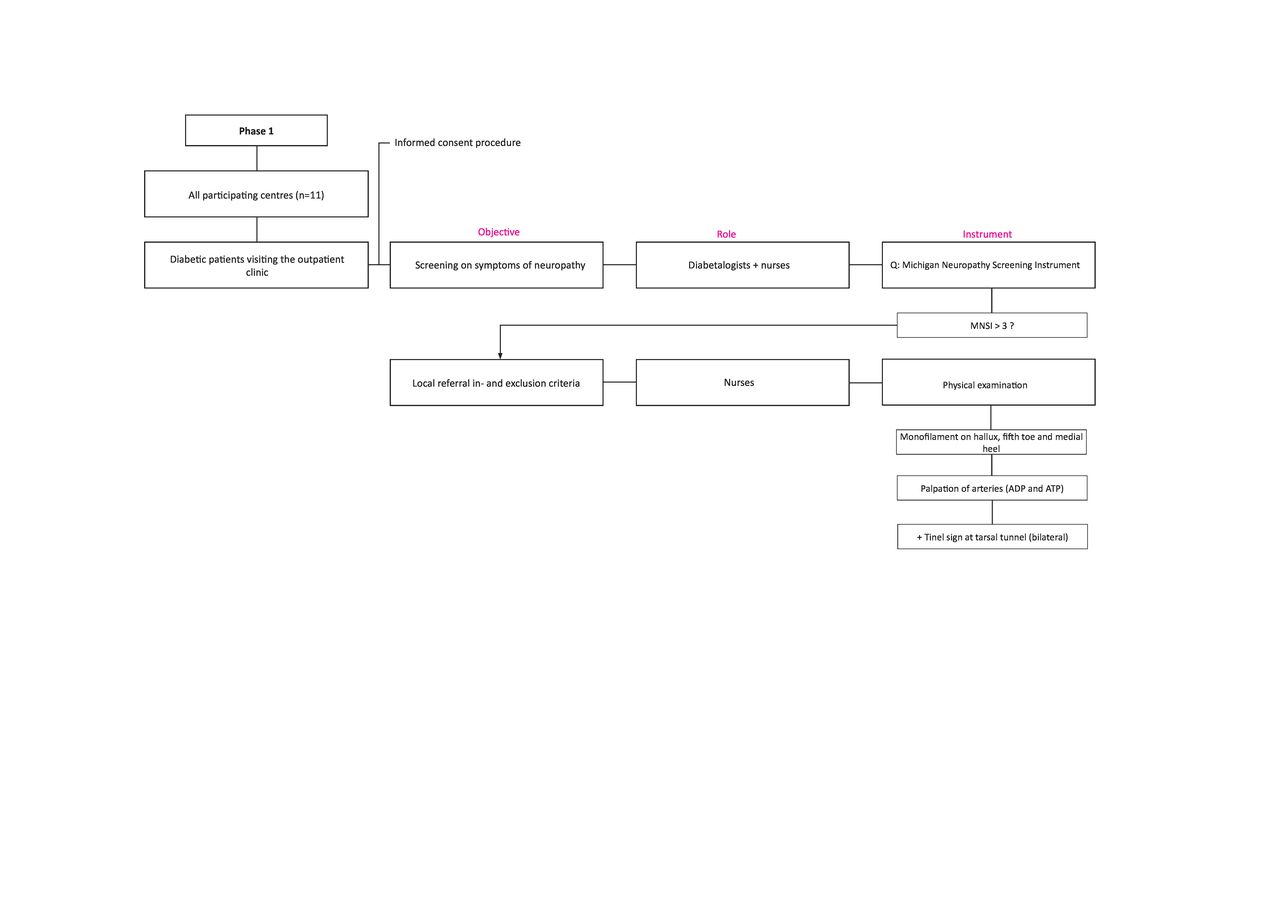
Study flow chart. LEND, lower extremity nerve decompression; MNSI, Michigan neuropathy screening instrument; ADP, a. dorsalis pedis; ATP, a. tibialis posterior; +, positive.

Study flow chart.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Study flow chart. LEND, lower extremity nerve decompression.
Patients with symptoms of neuropathy have to be examined regarding the presence of compression neuropathies in the lower extremity, using the physical examination (Tinel’s sign) as recommended by the American Association of Neuromuscular and Electrodiagnostic Medicine.18 21 Patients will undergo a thorough screening of their lower extremities (sensory tests, vascular status). The instruments of the Rotterdam Diabetic Foot (RDF) Study Test Battery will categorise each patient in their sensory loss, thereby determining whether they will be allegeable for LEND surgery.17 21 The RDF Test Battery is used as a measure of nerve function and likelihood of nerve regeneration after surgery.17 22 The investigator assesses foot morphology.
Surgical intervention
Interventions will take place in all affiliated hospitals, in which both plastic surgeons and neurosurgeons will perform LEND surgery. The aim is to operate patients within 6 months after randomisation. A surgical release of up to four nerves in one leg will be carried out (the common, superficial and deep peroneal nerves and tibial nerve at the soleal sling and tarsal tunnel). After release of the flexor retinaculum at the tarsal tunnel, the calcaneal branch and medial and lateral plantar nerves will be released via the same incision.23 Postoperatively, patients will be allowed to use the operated leg full weight bearing immediately and will use a walker for 3 weeks when necessary. In the patient who did not have preoperative pain and who experiences pain due to nerve regeneration, a regimen of neuropathic pain medication may be started, according to the current national protocols on neuropathic pain.24 The contralateral leg will be operated 3 months later, with similar follow-up accordingly. Participating surgeons are trained to standardise the method of treatment and number of patients treated is recorded.
The following postoperative instructions are given to the subjects in the surgical group:
The wound has to stay dry for 7 days.
The patient should keep the operated leg elevated when resting.
The patient is allowed to walk small distances the next days after the operation.
Long distance walking, running or walking the dog is not recommended and is allowed 3 weeks after surgery in case of normal wound healing.
Swimming and bathing are allowed after 14 days.
Performing sports is allowed after 3–6 weeks.
Patients will be instructed about wound problems.
Patients need to be instructed when he/she needs to contact the hospital.
Conventional non-surgical care
The control group is treated to care as usual, being conventional non-surgical care, and is defined as care in line with national and international guidelines for the treatment of neuropathy and diabetic foot disease. Non-surgical care includes the treatment with analgesics, according to the national guideline on painful neuropathy, preventive measures and education for patients at risk for diabetic foot ulceration. Biomechanical offloading and foot infection treatments are provided in both groups, when required during follow-up.
Randomisation
Patients will be randomised (1:1, stratified for hospital) to LEND surgery (intervention group) or current conventional non-surgical care (control group), using a web-based randomisation system (Castor Electronic Data Capture). Randomisation is stratified for centre and gender, implying that approximately the same numbers of LEND and control patients are treated in each centre. We acknowledge that practice variation across centres may exist, but this will not bias the overall estimated effect size of LEND versus control treatment. Patients who decline randomisation will be treated to care as usual. After the end of the study, control subjects have the possibility to undergo surgery, if the surgery is proven to be superior.
Outcome measurements
Primary objective
Primary outcome: to study the influence of LEND surgery on disease-specific quality of life as measured on the Norfolk Quality of Life Questionnaire—Diabetic Neuropathy (Norfolk-QoL-DN) questionnaire, at 48-month follow-up.
Description: The Norfolk-QoL-DN questionnaire is developed to assess patients’ subjective perceptions of symptoms associated with specific nerve fibre damage occurring in diabetes and is validated in other populations.25 26 Questions relate to physical functioning, large fibre neuropathy, activities of daily living, symptoms, small fibre neuropathy and autonomic neuropathy and are summed into a total score. The questionnaire is administered at different time points during follow-up (table 1).
Visit plan of the DeCompression trial
Secondary objectives are (short term)
To study the influence of LEND surgery on balance and gait parameters at 24 months.
Secondary outcome: the difference between pedobarographic and pedothermographic imaging results between the intervention and control group.
Description: pedobarographic imaging will be used to assess differences in plantar pressure distributions during standing and gait. Pedothermographic imaging will assess differences in vascular supply at the foot sole. Increased plantar pressure relates to the development of DFUs.27 Temperature measurements are shown to be of value in the prediction of tissue breakdown.28–30 The before mentioned measurements are carried out at baseline and 12 and 24 months of follow-up (table 1).
To study to what extent preoperative electrodiagnostic studies (used to grade the severeness of diabetic sensorimotor polyneuropathy (DSP)) account for the variation in surgical outcome (HRQoL: Norfolk-QoL-DN, SF-36, EQ-5D) at 24 months.
Secondary outcome: the influence of electrodiagnostic parameters (compound muscle action potential (CMAP), distal motor latency (DML), sensory nerve action potential (SNAP)) on the difference in scores of HRQoL between the intervention and control group.
Description: since diabetes induces nerve damage, surgical outcome after LEND is presumably related to the degree of preoperative nerve functioning. To assess this relationship, validated electrodiagnostic parameters are used to grade nerve functioning, as well to monitor nerve parameters during follow-up, according to an established protocol from the Rotterdam Study.31
To study to what extent preoperative nerve damage influences the results of LEND surgery on balance and gait parameters, Visual Analogue Scale (VAS) neuropathy scores, HRQoL and symptoms at 24 months.
Secondary outcome: the influence of RDF Test Battery/quantitative sensory testing (QST) scores on the difference in balance and gait parameters, VAS neuropathy scores, HRQoL and symptoms (Michigan Neuropathy Screening Instrument (MNSI)) between the intervention and control group.
Description: the relationship between the degree of preoperative diabetes-induced nerve damage and surgical results of LEND on before mentioned outcomes will be assessed.17
Secondary objectives are (long term)
To study if LEND surgery is cost effective, compared with conventional non-surgical care (HRQoL, resource use, productivity loss), at 48 months.
Secondary outcome: the difference between HRQoL, resource use (based on data from hospital financial systems, general practitioner, national databases) and productivity loss (Medical Cost Questionnaire and Productivity Cost Questionnaire) between the intervention and control group. Cost effectiveness will be evaluated as the incremental cost–utility ratio (ICUR/incremental cost-effectiveness ratio (ICER)) of LEND surgery compared with conventional non-surgical care.
Description: cost effectiveness of LEND compared with conventional care is estimated by comparing HRQoL, medical costs (resource use due to DFUs, amputations, falls) and productivity loss between the two strategies at 48 months of follow-up (table 1).
The influence of LEND surgery on gain in sensory function at 48 months.
Secondary outcome: the difference in RDF Test Battery scores and QST between the intervention and control group.
Description: since the compression component in neuropathy of peripheral nerves is released with LEND surgery, processes of remyelination and axon outgrowth are allowed. To study these processes over time, somatosensory testing of the (foot) skin is conducted at different time points during follow-up (table 1).17 19 20
To study to what extent this surgical procedure results in lower risk of diabetic foot ulceration, amputation and falls at 48 months.
Secondary outcome: the difference in incident diabetic foot ulceration, amputation and falls between the intervention and control group.
Description: reinnervation of the skin presumably relates to lower odds of lower extremity complications and falls during follow-up. To study this, besides quantification of skin sensation, incident ulceration, amputations and falls are monitored during the total duration of the study (table 1).
To study to what extent preoperative nerve damage influences the results of LEND surgery (ie, HRQoL, sensory function and the incidence of ulceration, amputation and falls) at 48 months.
Secondary outcome: the influence of baseline nerve function, as assessed with the RDF Test Battery and QST instruments, on HRQoL, RDF Test Battery scores, QST, incident ulceration, amputation and falls.
Description: it is expected that the degree of preoperative nerve damage serves as an effect modifier on these outcomes.17 19 20
Study procedures
Utrecht Medical University Center is the coordinating centre and responsible for training the participating surgeons in both the anatomy lab and during live surgery demonstrations. Outcomes will be evaluated in terms of HRQoL (Norfolk QoL-DN, EQ-5D-5L, SF-36), balance and gait parameters, sensory function, incident ulceration, amputation and falls, resource use and productivity loss (table 1). The follow-up moments are at 1.5, 3, 6, 9, 12, 18, 24 and 48 months and include clinical checkups and wound checkups. Outcome assessors are blinded to group assignment (locations of incisions are blinded, and patients are instructed before the assessment). Patients will be asked regarding their resource use according to the intervals.
All participants are treated according to current standards of diabetic foot care, according to national and international (IWGDF) guidelines. The duration of the study is 5 years in total. Inclusion of participants is expected to last 12 months in total. The follow-up period is 48 months.
Laboratory results and relevant data on the medical history will be retrieved from the patient file. In screening patients on neuropathy symptoms, the MNSI will be used. Degree of neuropathy symptoms will also be evaluated with the VAS and will be used for both legs and feet separately. The VAS is a straight line, the ends of which are the extreme limits of the sensation being assessed. The line is 10 cm in length, using a 10-point scale ranging from 1 to 10, with 1 being barely perceptible and 10 being intolerable. All patients are given questionnaires to assess baseline neuropathy symptoms (Norfolk QoL-DN) and quality of life (SF-36, EQ-5D5L).
Sensory status
The RDF Study Test Battery consists of monofilament testing, two-point discrimination, vibration sense testing and questions on previous ulcers/amputations and its clinical utility has been validated.19 20 The RDF Study Test Battery instruments (tuning fork, monofilament) are validated and part of both the neuropathy and diabetic foot care guidelines.32 The total time needed to execute the tests of the RDF Study Test Battery is approximately 30 min.
Quantitative sensory testing
To study the effects of LEND surgery on sensory loss (small and large fibre functions) and sensory gain (hyperalgesia, allodynia (ALL), hyperpathia), we combine the instruments of the RDF Test Battery with the instruments used in the battery of the German Research Network on Neuropathic Pain (DFNS). In two centres (in total 80 patients, 40 in each arm), the QST measurements will be carried out. The DFNS instruments measure thermal detection thresholds for the perception of cold, warm and paradoxical heat sensations (PHS), thermal pain thresholds for cold and hot stimuli, mechanical pain sensitivity (MPS) including thresholds for pinprick and blunt pressure, a stimulus-response function for pinprick sensitivity and dynamic mechanical ALL and pain summation to repetitive pinprick stimuli. The procedures described below are derived from and according to the QST protocol for clinical trials of the DFNS and are applied at the plantar side of the foot.33
Thermal detection, thermal pain thresholds and PHS
The tests for thermal sensation are performed using a TSA (MEDOC, Israel) thermal sensory testing device. Cold detection threshold and warm detection threshold are measured first. The number of PHS is determined during the thermal sensory limen procedure (the difference limen for alternating cold and warm stimuli), followed by cold pain threshold, and heat pain threshold. Of three consecutive measurements, the mean threshold temperature is calculated. All thresholds are obtained with ramped stimuli (1°C/s) that are terminated when the subject presses a button. Cut-off temperatures are 0°C and 50°C. The baseline temperature is 32°C (centre of neutral range) and the contact area of the thermode is 7.84 cm2. During the session, subjects are not able the watch the computer screen. All tests are first demonstrated over an area that is not tested in the session.
Mechanical pain threshold (MPT) for pinprick stimuli
MPT is measured using a set of seven custom-made weighted pinprick stimulators that exert forces between 8 and 512 mN. Using the method of limits, the final threshold is the geometric mean of five series of ascending and descending stimulus intensities.
Stimulus-response functions: MPS for pinprick stimuli and dynamic mechanical ALL for stroking light touch
MPS is tested using the same weighted pinprick stimulators as for MPT. To obtain a stimulus-response function, these seven pinprick stimuli are applied in a balanced order, five times each, and the subject is asked to give a pain rating for each stimulus on a 0–100 numerical rating scale (‘0’ indicating ‘no pain’, and ‘100’ indicating ‘most intense pain imaginable’). Stimulus-response functions for dynamic mechanical ALL are determined using a set of three light tactile stimulators: a cotton wisp exerting a force of ±3 mN, a cotton wool tip fixed to an elastic strip exerting a force of ±100 mN and a standardised brush (Somedic, Sweden) exerting a force of ±200–400 mN. The three tactile stimuli are applied five times each with a single stroke of approximately 1–2 cm in length over the skin. They are intermingled with the pinprick stimuli in balanced order and subjects are asked to give a rating on the same scale as for pinprick stimuli.
Wind-up ratio (WUR): the perceptual correlate of temporal pain summation for repetitive pinprick stimuli
In this test of temporal summation, the perceived magnitude of a single pinprick stimulus was compared with that of a train of 10 pinprick stimuli of the same force repeated at a 1/s rate (256 mN). The train of pinprick stimuli is given within a small area of 1 cm2 and the subject is asked to give a pain rating representing the pain at the end of the train using a numerical rating scale. Single pinprick stimuli are alternated with a train of 10 stimuli until both are done five times at five different skin sites. The mean pain rating of trains divided by the mean pain rating to single stimuli is calculated as WUR.
Pressure pain threshold (PPT)
The pressure pain threshold (PPT) is determined with three series of ascending stimulus intensities, each applied as a slowly increasing ramp of 50 kPa/s, using a pressure gauge device (FDN200, Wagner Instruments, USA).
The total time needed to execute the tests of the DFNS protocol is approximately 20 min.
Electrodiagnostic tests
In two centres (in total 80 patients, 40 in each arm), the electrodiagnostic tests will be carried out, according to the protocol of the Rotterdam Study.31 The sural sensory nerve will be measured bilaterally and the peroneal motor nerve unilaterally, since these nerves are considered the most sensitive to detect DSP. The distal peroneal nerve CMAP amplitude and DML are recorded at the extensor digitorum brevis muscle. Stimulation is applied to the anterior side of the ankle, 8 cm proximal to the recording electrode. CMAP baseline peak amplitudes below 1.1 mV and DML values above 6.5 ms are considered abnormal. Sural SNAP amplitudes are measured bilaterally with a standard recording electrode placed behind the lateral malleolus. Stimulation is applied on the posterior side of the calf, 14 cm proximal to the recording electrode. SNAP baseline peak amplitudes below 4.0 μV are considered abnormal. Electrophysiology is performed using standard techniques of percutaneous supramaximal stimulation.
Balance and gait
In two centres (in total 80 patients, 40 in each arm), balance and gait parameters will be obtained. A pedobarographic and pedothermographic image will be made of both feet of each patient. The pedobarographic image will be made using a platform with pressure sensors measurement system (Tekscan Matscan, Massachusetts, USA or similar) and a pedothermographic image of the microvasculature will be made using an infrared camera (FLIR ONE Pro, FLIR Systems, Oregon, USA). Both pedobarographic and pedothermographic images will be made of both feet of each patient. The pedothermographic image will be obtained after a 15 min acclimatisation period in an air-conditioned room (ie, constant temperature and humidity). The plantar surface of both feet will be recorded during unloaded conditions. Next, patients will be asked to stand for 3 min on a dedicated polyethylene thermographic ‘foot mirror’, while recording the dynamic change of the pedothermographic image. For the pedobarographic measurements, patients will be asked to walk barefooted 5 times over a measurement system using a 2-step protocol with a self-selected, but constant walking speed.
Incidence of falls, ulcers and amputations
The incidence of falls, ulcers and amputations will be assessed at 6-month intervals. Ulcer characteristics will be determined using the IWGDF Perfusion, Extent, Depth, Infection and Sensation (PEDIS) and Society for Vascular Surgery Wound, Ischemia and foot Infection (WIfI) classification systems.34 35
Sample size calculation
Sample size was calculated as a difference in quality of life of the total Norfolk-Qol-DN score at 48 months (primary outcome), based on our own RDF Study cohort data and the literature on LEND surgery.33 The sample size calculation was based on the natural logarithm-transformed Norfolk QoL scores, given the skewness of these data. The mean of the ln-transformed scores is 2.46. The SD is 1.058. For this superiority study question, we used the usual parameters: type I error=5% (two sided) and type II error=20% (power=80%). A minimal 15% reduction of symptoms is anticipated after LEND surgery, which resulted in a total sample size of 129 per group, ratio=1:1). Adjusting for an anticipated 25% lost to follow-up renders our total study size to be 344 patients (129*100/75=172 patients per group (±32 patients per centre (n=11)). These numbers are also sufficient to demonstrate a reduction in the other outcome measures between the groups, such as ulceration rates: 2% vs 15% at 48 months (alpha=0.05 (two sided), beta=0.20 (power 80%), ratio=1:1, corrected for multiple testing.14
Data collection, management and analysis
All patients will be analysed according to the schedule in table 1. Data from initial visits, hospitalisation and follow-up visits will be entered into a database via an electronic data capture system (Castor EDC). Data will be recorded and analysed without any personal identifiers by using coded information. Source documents and identifiers will be archived. All analysis will be performed on the basis of intention to treat. Reporting of this RCT will be performed according to the Consolidated Standards of Reporting Trials/Consolidated Health Economic Evaluation Reporting Standards (Enhancing the QUAlity and Transparency Of Health Research) guidelines. Missing data will be reported and handled with depending on the mechanism of missingness within the DECO-trial dataset.
Statistical analyses
The difference between groups in change between baseline and follow-up in QoL will be used as primary outcome. Baseline characteristics will be described with conventional statistics: means (95% CI) for continuous variables with normal distributions, medians (IQR) for variables with skewed distributions and the χ2 test (or Fisher’s exact test, if appropriate) for discrete variables. Between-group comparison of the primary endpoint (Norfolk Qol-DN score) will be performed using repeated measurements analysis with time, allocated group and time * allocated group as determinants. Stratified for randomisation are hospital and number of nerves involved. Basically, the same method will be followed for analysis of EQ-5D5L and SF-36 profiles, over time (a different method may be selected, depending on the precise shape of the distributions). Between groups comparisons of sensory function will be performed using Wilcoxon rank-sum test repeated measurement analysis. The between-group cumulative incidence of DFU, amputations and falls will be tested using the χ2 test. Between groups comparison of the time to these events will be estimated using Kaplan-Meier analysis. The role of preoperative loss of sensation (nerve damage) as a possible effect modifier of effectiveness will be studied by adding this variable to the repeated measurements and the Kaplan-Meier analysis. Differences in surgical outcome are investigated by assessing possible effect modifiers like hospital, surgeon’s experience and patient factors. Between group comparisons of balance and gait parameters will be performed using Wilcoxon rank-sum test repeated measurement analysis. Regression analysis will be used to study the influence of preoperative electrodiagnostic parameters on Norfolk QoL-DN symptom scores at 24 months. Regression analysis will be used to study the influence of preoperative RDF Test Battery scores on balance and gait parameters, VAS pain scores, HRQoL and symptoms at 24 months. Parameters on preoperative nerve damage as possible effect modifier of effectiveness will also be studied by adding this variable to the repeated measurements and the Kaplan-Meier analysis.
Cost-effectiveness analyses
We will assess the cost effectiveness of LEND surgery versus conventional non-surgical care over a period of 48 months. We will perform a cost–utility analysis using a disease progression model, quality of life and costs data. Cost effectiveness will be evaluated as the ICUR (ICUR/ICER) of LEND surgery compared with conventional non-surgical care. The CI of the ICUR point estimate will be obtained with bootstrapping. Data from the DECO study will be used to quantify length of life (survival), quality of life (based on the EQ-5D5L utility scores for which ‘Dutch tariffs’ are available) and costs. In the view of the long-term study perspective, estimated costs are adjusted for inflation (Gross Domestic Product (GDP) index) as well as for societal time preference (discounting). Uncertainty of the estimated ICUR will be quantified using univariate sensitivity analysis (‘tornado’ plots) and probabilistic sensitivity analysis, depicted as cost-effectiveness plane and acceptability curves. Heterogeneity will be studied in subgroup analyses, in order to resolve uncertainty and guide subgroup-specific treatment decisions.36 37 Examples of subgroups include age, duration of diabetes, metabolic control, socioeconomic status (level of education and current activities of daily life) and degree of nerve damage at study entry. Estimating the cost–utility acceptability curves of both treatment strategies and value of information analysis will support decision-making. The economic analysis will be based on the societal perspective and on the healthcare perspective in which the direct medical and productivity costs in both groups will be compared. The friction cost method will be used to estimate the indirect costs of disease, which explicitly considers economic circumstances that limit production losses due to disease, according to recent Dutch guidelines. The costs per unit of medical consumption will be estimated, using the methods from the most recent Dutch Manual for Costing in Economic Evaluations. The biggest gain in lowering costs is expected from the long-term prevention of diabetic ulcers and amputations. Other factors include time to ulcer and remaining life expectancy. Hospital data will be used to estimate the costs of surgery. Implementation costs of training surgeons will be considered.
The study will be monitored by Julius Center, Zeist, the Netherlands. At least one monitoring visit per year per centre will be conducted. During the complete study period, all adverse events will be reported (table 1).
Ethics and dissemination
The study will be conducted according to the principles of the Declaration of Helsinki and in accordance with the Medical Research Involving Human Subjects Act and General Data Protection Regulation. Previous studies have proven that LEND surgery has beneficial effects on the pain and restoration of sensation in patients with neuropathy symptoms. However, the long-term effects of LEND surgery are not yet known regarding restoration of sensation, prevention of ulceration and amputations and cost effectiveness, compared with conventional non-surgical care. Recruitment of patients starts in November 2019 and will be finished when all 344 patients have been followed up for 4 years, which is expected at the end of 2024.
Discussion
A proper RCT, designed and based on thorough knowledge of peripheral nerve pathology, its associated surgical treatments and patient selection, does not yet exist in the current literature and is much needed to breach this status quo. Since current care does not provide a solution to the refractory problems of neuropathy, and the incidence of diabetes is still rising, new treatments like LEND surgery might give solutions regarding efficacy and expediency. RCTs on LEND surgery are pled for in the medical community and our previous work, the RDF study, forms the perfect precursor of the DECO trial.38 39
References
Footnotes
Contributors WDR designed the study, acquired data and is primary investigator and coordinator of the trial. TMF contributed to medical ethical considerations and conducted trial preparations. MCC, EB and JHC contributed to the trial design and trial preparations. All authors read and approved the final manuscript.
Funding This work was supported by ZonMw (Netherlands Organisation for Health Research and Development), grant number 852001906. ZonMW’s reviewers of the DECO trial project proposal did suggestions on trial design and methods of analysis, but do not have influence on data nor interpretation of this study. Sponsor: Utrecht University Medical Center. Contact information: JH Coert MD, PhD, email address: j.h.coert@umcutrecht.nl.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.