Article Text

Abstract
Introduction Type 2 diabetes mellitus (T2DM) is a common and heterogeneous disease. Using advanced analytic approaches to explore real-world data may identify different disease characteristics, responses to treatment and progression patterns. Insulin glargine 300 units/mL (Gla-300) is a second-generation basal insulin analogue with preserved glucose-lowering efficacy but reduced risk of hypoglycaemia. The purpose of the REALI pooled analysis described in this paper is to advance the understanding of the effectiveness and real-world safety of Gla-300 based on a large European patient database of postmarketing interventional and observational studies.
Methods and analysis In the current round of pooling, REALI will include data from up to 10 000 subjects with diabetes mellitus (mostly T2DM) from 20 European countries. Outcomes of interest include change from baseline to week 24 in haemoglobin A1c, fasting plasma glucose, self-measured plasma glucose, body weight, insulin dose, incidence and rate of any-time-of-the-day and nocturnal hypoglycaemia. The data pool is being investigated using two complementary methodologies: a conventional descriptive, univariate and multivariable prognostic analysis; and a data-mining approach using subgroup discovery to identify phenotypic clusters of patients who are highly associated with the outcome of interest. By mid-2019, deidentified data of 7584 patients were included in the REALI database, with a further expected increase in patient number in 2020 as a result of pooling additional studies.
Ethics and dissemination The proposed study does not involve collection of primary data. Moreover, all individual study protocols were approved by independent local ethics committees, and all study participants provided written informed consent. Furthermore, patient data is deidentified before inclusion in the REALI database. Hence, there is no requirement for ethical approval. Results will be disseminated via peer-reviewed publications and presentations at international congresses as data are analysed.
- insulin glargine 300 units/mL
- type 2diabetes mellitus
- clinical practice
- Europe
- pooled analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The large European sample size allows more precise statistical calculations and provides European clinicians with findings relevant to their specific patient populations.
The mixture of interventional and observational studies including information from a wider patient population, such as the elderly or those with comorbidities (who might normally be omitted from premarketing clinical trials), creates a valuable real-world data set.
Bias(es) may exist in some data due to greater representation of certain countries and/or between-study differences in the management of patients.
The power of the extensive sample size of the REALI project may be reduced in certain patient profiles because some data (eg, specific laboratory values or patient-reported outcomes) were not collected in all studies.
The REALI project could function as a blueprint for further evaluation of new treatment strategies aiming to identify markers to optimise the treatment of each patient and to recognise respective clinical subgroups.
Introduction
Diabetes mellitus (DM) is a heterogeneous disease, with a population that exhibits diverse clinical and biological characteristics.1 2 Current American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD) guidelines recommend a patient-centred approach that takes into account individual patient preferences and needs.3 4 Indeed, it has been shown that in addition to pharmacogenetic factors, phenotypic and clinical features, such as body weight, age of diabetes onset and comorbidities, may influence the outcomes of glucose-lowering therapies.1 5 6 Moreover, it is also recommended to have tailored glycaemic targets for each patient.7 Hence, to individualise treatments and glycaemic targets appropriately, it is important to assess treatment effectiveness in different patient profiles to ensure patients receive the interventions that are most likely to provide the greatest benefit.
The most recent ADA/EASD recommendations recognise the need for basal insulin, with low risk of hypoglycaemia or weight gain, in the treatment of patients with type 2 diabetes mellitus (T2DM).4 Insulin glargine 300 units/mL (Gla-300) is a second-generation basal insulin analogue with a more stable and prolonged pharmacokinetic/pharmacodynamic profile than insulin glargine 100 units/mL (Gla-100) that lasts beyond 24 hours.8 9 It was approved in 2015 by both the United States Food and Drug Administration and the European Medicines Agency for the treatment of type 1 diabetes mellitus (T1DM) and T2DM.8 10 The efficacy and safety of Gla-300 compared with Gla-100 has been investigated in several randomised controlled trials (RCTs), including the EDITION Phase III clinical trial programme, which comprised a series of international, multicentre, treat-to-target RCTs conducted in distinct populations of patients with T1DM or T2DM.11 12 The EDITION studies demonstrated comparable reductions in haemoglobin A1c (HbA1c) levels, but with less hypoglycaemia with Gla-300 compared with Gla-100 in people with T2DM12 13 and T1DM,11 irrespective of a patient’s age, body mass index (BMI), age at onset of DM or duration of DM.
While RCTs are generally considered the gold standard for evaluating the effects of drugs in specific disease and patient settings, it is often challenging to extrapolate their results to more general patient populations in real-life clinical circumstances.14 Real-world evidence (RWE), resulting from the rigorous analysis of diverse sources of data, including electronic health records, claims data, disease registries and data from personal devices/software applications, is an important complementary component to clinical trial data as it provides a broader and unique insight into patient information, which could improve clinical decision-making in DM management.14 Real-world studies conducted in large T2DM patient populations in the USA, such as the DELIVER D+,15 DELIVER 216 and the LIGHTNING17 studies, provide complementary findings that support results from RCTs and reflect the effectiveness of Gla-300 in real-world clinical practice. Similarly, in Europe where daily clinical practice may differ from the USA, a number of postmarketing interventional, observational and RWE studies are being conducted to assess the effectiveness and safety profile of Gla-300 under real-life daily clinical practice conditions.18
Summary statistics, such as those derived from systematic reviews and pooled data analyses, are important tools to discover further novel insights and to guide clinical thinking, practice, education and research in DM treatment.19 Specifically, combining and analysing European data from different observational and interventional studies would increase the precision with which to describe the overall treatment effect of Gla-300 and would be useful to compare clinical outcomes in various subpopulations of interest that may be less represented in RCTs (eg, patients with renal impairment, older adults, patients a thigh risk of hypoglycaemia, etc). In the present paper, the rationale and methodology of the REALI project, which is an ongoing incremental data pooling initiative including postmarketing interventional and observational studies of Gla-300 in different real-world settings across Europe, is reported.
Methods and analysis
Overall project design
The REALI project will create a pooled database that combines data from more than 16 studies covering 20 European countries, and will comprise real-world data from over 10 000 patients with T1DM or T2DM who were initiated on Gla-300, or switched from other glucose-lowering therapies to Gla-300, due to unsatisfactory glycaemic control. The data set used for the REALI project consists of a mixture of information generated from both interventional (single-arm or multiarm) and observational studies conducted in the postmarketing setting.
The REALI project extracts information from each study on characteristics (ie, baseline information and relevant effectiveness and safety parameters) that constitute the minimum required variables common to all studies included in this database. All other patient-level variables are also captured in the REALI database. Study-level characteristics (design, country and follow-up length) are also extracted from each trial included in the data set. Once a study has been conducted, a case report form, which includes details about the variables of interest, is collected. The study’s database is then cleaned and locked, and subsequently made available to the country of origin for local statistical analysis, while being sent simultaneously for central deidentification. Following this process, the data added to the REALI database are mapped and pooled into a common database for statistical analysis. Figure 1 illustrates the overall REALI project design.

Project design of REALI. CRF, case report form; CRO, contract research organisation; EU, European Union.
All studies included in the database were conducted according to Good Clinical Practice and the Declaration of Helsinki. Ethical approval was obtained for each study and all participants provided written informed consent.
Patient population
Studies include adult patients (≥18 years of age) with a confirmed diagnosis of T1DM or T2DM who initiated Gla-300 and were uncontrolled on their previous glucose-lowering treatments. The minimum treatment duration required for the REALI studies is 24 weeks (6 months) of Gla-300 therapy, with at least two study visits: at baseline and at week 24. Although both T1DM and T2DM patients are included in REALI, the majority of patients have T2DM. For insulin-naïve patients with T2DM, uncontrolled on oral glucose-lowering therapy, Gla-300 is added with or without adjustment of their previous treatment(s), whereas patients with T1DM and T2DM pretreated with basal insulin are switched to Gla-300 treatment. There are no restrictions on the number of previous glucose‐lowering therapies. The inclusion and exclusion criteria for each individual Gla-300 study are defined in the corresponding country’s clinical study protocol. In all observational and most interventional studies, the inclusion criteria have been broadly defined to allow for inclusion of any patient who would benefit from Gla-300 insulin therapy to improve diabetic control.
Outcomes
Studies are included in the REALI database if they report on the following demographic and clinical characteristics at baseline: age, gender, BMI, comorbidities, disease characteristics such as type and duration of diabetes, and previous and concomitant therapies.
With respect to the effectiveness of Gla-300 therapy, the outcomes of interest, related to glycaemic control, are as follows:
HbA1c(%) change from baseline to week 24.
Proportion of patients achieving HbA1c targets (<7.0% and <7.5%) at week 24.
Fasting plasma glucose (mg/dL) change from baseline to week 24.
Self-measured plasma glucose (mg/dL) change from baseline to week 24.
Safety endpoints include the following:
Overall safety of Gla-300: frequency and type of adverse events and serious adverse events.
Incidence and event rates of hypoglycaemia defined according to the ADA classification20 and by time of day (any-time-of-the-day and nocturnal hypoglycaemia).
Other outcomes that are collected in all included studies consist of the following:
Body weight (kg) change from baseline to week 24.
Change in Gla-300 daily dose (U/kg/day) from baseline to week 24.
Additional outcome measures, which are collected in only some studies, include patient-reported outcomes, low-density lipoprotein cholesterol, estimated glomerular filtration rate (eGFR) and vital signs at baseline and week 24.
Data that were requested in certain studies but were not collected will be described as ‘missing data’, whereas those that were not requested will be described as ‘unavailable data’.
Statistical analyses
The overall population comprises all patients who are identified in the locked individual databases as having entered a study, while the treated population includes all patients who are identified as having entered a study in addition to having been treated with at least one reported injection of Gla-300 within the individual study period.
To enhance the informative output of the pooled database, the REALI project uses two statistical methodological approaches: a conventional descriptive and modelling analysis, and a subgroup discovery approach.
The conventional descriptive analyses assess patient characteristics and clinical effectiveness and safety outcomes in the overall population as well as in patient subgroups of interest such as the following:
Insulin-naïve versus insulin-pretreated patients.
Patients with eGFR <60 mL/min/1.73 m2 versus ≥60 mL/min/1.73 m2.
Patients <65 years of age versus those between 65 and 75 years versus ≥75 years.
Early-onset versus late-onset diabetic patients, based on age threshold.
Moreover, this approach allows for comparisons between interventional and observational studies. For the conventional descriptive approach, data will be analysed at the patient level. Descriptive subgroup analyses by age, eGFR, gender and insulin pretreatment status are being conducted. Univariate and multivariable analyses are being performed to identify potential factors that predict improved glycaemic control as well as adverse events, such as baseline BMI evaluated as a continuous variable (using a linear function). Further statistical methods may be considered as the project evolves and will be defined in the statistical analysis plan.
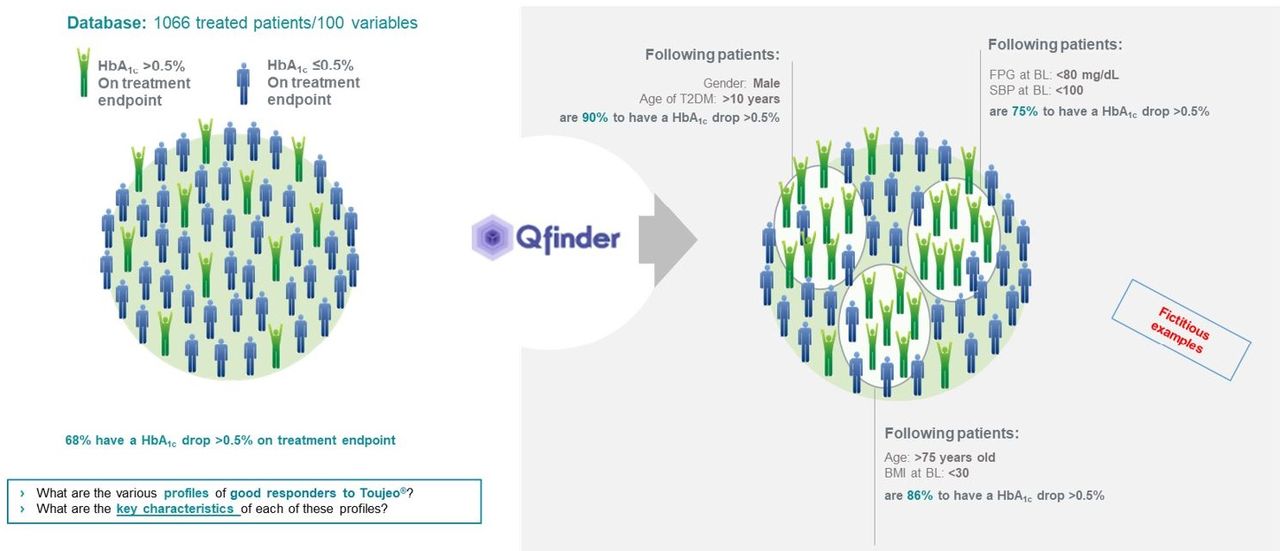
The subgroup discovery approach is a broadly applicable data-mining technique that aims to discern clusters of patients with more favourable or less favourable glycaemic outcomes and who, therefore, may benefit the most or the least from Gla-300, without pre-existing hypotheses.21 This tool generates data-driven hypotheses, which may confirm existing hypotheses or facts relating to Gla-300 efficacy and safety and/or may be novel empirical hypotheses to increase understanding of treatment response. For the subgroup discovery approach, Q-Finder (Quinten, Paris, France), a proprietary non-parametric supervised learning algorithm working with no particular assumption regarding distributions of outcomes or explanatory variables, will be used to generate new empirical hypotheses and produce patient profiles of good responders to Gla-300.22 23 In this respect, the raw data from the interventional and observational studies are first checked for consistency, and only patients with available HbA1c values at baseline and week 24 from the pooled database are included. This information is then flattened from one row of data per patient per visit, to one row per patient and one column per visit. Next, the data are consolidated into a learning matrix, which includes the outcome and patient baseline characteristic values. Three learning matrices are produced: one for learning on two-thirds of the interventional studies (hypotheses generation), one for testing on the remaining third of the interventional studies and one for testing on the observational studies (hypotheses testing). Only the hypotheses validated on at least one of the test data sets are carried through. According to the hypotheses generated, Q-Finder extracts potential profiles of responders to Gla-300 from the database and examines the key characteristics of the patients who match these profiles (figure 2). In order to reduce the risk of false-positive findings and to confirm the significance of the findings, each patient profile will be adjusted for confounding factors and a Bonferroni correction will be applied.

{kind=link}
{kind=link}
Q-Finder methodology. BL, baseline; BMI, body mass index; FPG, fasting plasma glucose; HbA1c, haemoglobin A1c; SBP, systolic blood pressure; T2DM, type 2 diabetes mellitus.
REALI project progress
From the end of 2017 to July 2019, eight European studies were included in the REALI pooled raw database, of which three are interventional and five observational (n=7121) (table 1). Three studies are currently being mapped to be added to the REALI data pool, leading to a total of 7584 patients included in the REALI database by mid-2019. Further studies are still ongoing, which will increase the number of patients with T1DM and T2DM to more than 10 000 (table 1). At the end of the REALI programme, 20 European countries will be represented in the data pool.
List of REALI studies
Discussion
This collaborative European project aims to advance our understanding of the effectiveness and real-world safety of Gla-300 predominantly in patients with T2DM, uncontrolled by their current glucose-lowering regimen and in need of basal insulin therapy. The large REALI database is being explored using two different statistical methods to investigate the profiles of patients whose glycaemic control is improved in varying degrees after initiation of Gla-300 treatment. At the time of writing this paper, data from 7584 patients are being included in the REALI data pool, and this number is set to grow further as shown in table 1.
Pooled data analyses have previously been conducted to inform treatment options for T2DM. A 2011 pooled analysis of 38 phase II and phase III studies evaluated the safety and tolerability of the dipeptidyl peptidase-4 inhibitor vildagliptin, administered as a monotherapy or in combination with metformin, thiazolidinediones, sulfonylureas or insulin for ≥12 weeks up to 2 years in patients with T2DM.24 Moreover, a recent posthoc pooled analysis, of three pivotal RCTs in adult patients with T2DM using only basal insulin (EDITION 2, EDITION 3 and EDITION JP 2), was conducted to evaluate the risk of nocturnal hypoglycaemia with Gla-300 versus Gla-100. This pooled analysis found a lower incidence of nocturnal hypoglycaemia with Gla-300 versus Gla-100, which was confirmed using all analysed time windows, showing a consistently reduced risk with Gla-300 compared with Gla-100.25 Similarly, a 2013 pooled analysis of 24-week data, from nine prospective, open-label, multicentre, phase III/IV, two-arm, parallel-group RCTs, was undertaken to compare the efficacy and safety of insulin glargine versus comparator treatments (including rosiglitazone, pioglitazone, insulin lispro, insulin lispro 75/25, neutral protamine Hagedorn (NPH) insulin, NPH insulin 30/70 and lifestyle/dietary measures) in 2938 older (≥65 years) and younger adults (<65 years) with T2DM. In this analysis, insulin glargine was associated with better glycaemic control and a reduced incidence of daytime and any-time-of-the-day (24 hours) hypoglycaemia compared with comparator interventions in both younger and older T2DM patients.26
So far, however, the pooled efficacy and safety of Gla-300 have been examined only in preplanned meta-analyses of pivotal registration trials, and RWE related to the effectiveness and safety of Gla-300 is mainly available for North America. Thus, the REALI programme expands the analyses on the effectiveness and real-world safety of Gla-300 to include Europe, where healthcare delivery systems are different from those in North America, yet similar management guidelines are adopted. Furthermore, the REALI project aims to identify and understand the variation in patients’ experiences when treated with Gla-300, and to gauge selected patient characteristics that may be of interest to describe subsets of European populations with diabetes. To achieve these goals, the REALI programme uses two complementary statistical approaches, which enhance the chance of correctly identifying subgroups of patients with specific effectiveness and real-world safety patterns. Highlighting the profiles of patients who achieve greater glycaemic control will allow clinicians to provide personalised treatment plans to patients with diabetes.
Strengths and limitations
Considering that there may be differences in daily clinical practice between Europe and other regions, one of the strengths of the REALI pooled analysis is the creation of a large and prospective database from several multicentre and/or multinational studies conducted across diverse diabetic populations in different European countries. The use of such databases in diabetes research has several advantages. Aside from generating new hypotheses, a large database is representative of the target population, and once set up, it is relatively quick and cheap to use compared with primary data collection.27 The REALI project is a unique database that provides the opportunity to evaluate the effects of Gla-300, even in patient subgroups with low representation in individual studies, and to address alternative questions. Moreover, it allows us to confirm the effectiveness and tolerability of Gla-300 in real-world clinical practice. Another strength of the REALI project is that data collection of key clinical and demographic characteristics at baseline, as well as outcomes assessed at conventional time points, was predefined for all studies, thereby limiting heterogeneity between the pooled studies. Moreover, the mixture of study types, that is, observational and interventional, affords the opportunity to validate some assumptions in one study type and to apply them in the other.
Despite these strengths, several limitations of this project must be acknowledged. First, even though the REALI project is extracting information on predefined minimum required variables common to all the studies included in the database, data collection may vary across these studies, which can lead to inconsistency between the results. Second, the combination of observational and interventional data could increase the heterogeneity of the findings and may introduce bias. However, this issue will be addressed through stratified analyses of interventional and non-interventional studies. Third, bias(es) may exist in some data due to greater representation of some countries and/or between-study differences in the management of patients, particularly regarding basal insulin titration. Finally, the REALI project shares the intrinsic methodological limitation of the observational study design, with potential selection bias and the increased likelihood of ‘missing’ or ‘not collected’ data compared with RCTs.28 Nevertheless, the size and diversity of the patient populations of REALI, derived from both interventional and observational studies and from different therapy regimens, guarantee robust RWE closer to daily clinical practice than classical RCTs.29
ETHICS AND DISSEMINATION
Ethical considerations
The REALI project does not involve collection of primary data. Moreover, all protocols were approved by the independent local ethics committee/institutional review board at each study site or country, and all study participants provided written informed consent. Furthermore, patient data is deidentified before inclusion in the REALI data pool. For these reasons, no ethical approval is required for the REALI project.
Dissemination plan
The authors will disseminate the findings of this project through publications in peer-reviewed journals and presentations at international congresses as data are analysed.
Acknowledgments
The authors would like to thank Niki Panagiotaki, PhD, and Jane Juif, MSc, from HealthCare21 Communications Ltd (Macclesfield, UK), as well as Thomas Rohban, MD, and Magalie El Hajj, MPharm, from Partner 4 Health (Paris, France) for providing medical writing support. Conventional descriptive statistical analyses are being performed by IDDI (Louvain-la-Neuve, Belgium), while subgroup discovery analyses are being carried out by Quinten (Paris, France).
References
Footnotes
Contributors MB and AC led the protocol elaboration and organised data collection and contributed to the statistical analyses plan. GB and CM contributed to the conventional descriptive statistical analyses section and data pooling. MR contributed to the subgroup discovery design and its analysis plan. NF, RCB, PG, DM and DMW provided guidance on the design of data collection and pooling and contributed to the statistical analyses plan. All authors provided input into and reviewed and edited the manuscript, and approved the final version prior to submission.
Funding The REALI project is supported by Sanofi (Paris, France), including performance of statistical analyses and medical writing.
Competing interests NF: research, travel or consultancy: Takeda, Pfizer, Biogen, Tesaro, Allergan, Ipsen, Sanofi and AstraZeneca. RCB: speakers’ bureau: Sanofi, Merck, Sharp & Dohme, Bristol-Myers Squibb, AstraZeneca and Janssen; Advisory panel: Merck, Sharp & Dohme, Eli Lilly, Sanofi and Johnson & Johnson. PG: research: AstraZeneca, Novo Nordisk and Sanofi; speakers' bureau and consultancy: Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck Sharp & Dohme, Novartis, Novo Nordisk, Sanofi, Servier and Takeda. DM: consultancy and/or speakers’ bureau: Almirall, Ascensia, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Eli Lilly, Ferrer, Janssen, Menarini, Merck, Sharp & Dohme, Novartis, Novo Nordisk and Sanofi. DMW: speakers’ bureau and consultancy/advisory panel: Amgen, AstraZeneca, Boehringer Ingelheim, MSD (Merck & Co.), Novartis, Novo Nordisk and Sanofi. GB: IVIDATA employee on behalf of Sanofi. CM: IDDI employee. MR: Quinten employee. AC and MB: Sanofi employees.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.