Article Text

Abstract
Objective To investigate the association between work schedules and motivation for behavioural change of lifestyle, based on the transtheoretical model (TTM) in workers with overweight or obesity.
Design A cross-sectional observational study.
Setting A healthcare examination centre in Japan.
Participants Between April 2014 and March 2016, we recruited 9243 participants who underwent healthcare examination and met the inclusion criteria, namely, age 20–65 years, body mass index (BMI) ≥25 kg/m2 and full-time workers.
Exposure Night and shift (night/shift) workers were compared with daytime workers in terms of motivation for behavioural change.
Primary and secondary outcome measures The primary outcome was action and maintenance stages of change (SOC) for lifestyle in TTM. In a subgroup analysis, we investigated interactions between characteristics, including age, sex, BMI, current smoking, alcohol habits, hours of sleep and working hours.
Results Overall, 1390 participants (15.0%) were night/shift workers; night/shift workers were younger (median age (IQR): 46 (40–54) vs 43 (37–52) years) and the proportion of men was lesser (75.4 vs 60.9%) compared with daytime workers. The numbers of daytime and night/shift workers in the action and maintenance SOC were 2113 (26.9%) and 309 (22.2%), respectively. Compared with daytime workers, night/shift workers were less likely to demonstrate action and maintenance SOC (adjusted OR (AOR): 0.85, 95% CI: 0.74 to 0.98). In a subgroup analysis that included only those with long working hours (≥10 hours/day), results revealed a strong inverse association between night/shift work and action and maintenance SOC (AOR: 0.65, 95% CI: 0.48 to 0.86). A significant interaction was observed between long working hours and night/shift work (P for interaction=0.04).
Conclusions In workers with overweight or obesity, a night/shift work schedule was associated with a lower motivation for behavioural change in lifestyle, and the association was strengthened in those with long working hours.
- work schedule
- behavioural change
- the transtheoretical model (TTM)
- obesity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study examined the relationship between work schedules and motivation for behavioural change in workers with overweight or obesity.
Our cross-sectional study includes a relatively large sample with little missing data, and will contribute to the improvement of lifestyle behaviours in night/shift workers with overweight or obesity, particularly in those with long working hours.
Our study has certain limitations: data were obtained from a single centre, data on socioeconomic factors were not obtained adequately and misclassification of work schedules may have occurred since the factors were assessed using a questionnaire.
Introduction
Overweight and/or obesity is increasing worldwide, and is associated with higher risks of related complications including cardiovascular diseases, diabetes and certain cancers.1 2 In addition, overweight and/or obesity increases mortality and healthcare-related costs. Therefore, the management of overweight and/or obesity is relevant to both, individual and public health.3
Although newer interventions, including bariatric surgery and pharmacotherapy have been introduced, lifestyle intervention remains one of the most effective management strategies for overweight and obesity.2 4 The transtheoretical model (TTM), one of the approaches for lifestyle intervention, is used to support the adoption of modifiable lifestyle behaviours.5–8 TTM stratifies patients into a series of five stages based on their motivation: precontemplation (no intent to change behaviour in the near future), contemplation (state their intent to change within the next 6 months), preparation (intends to change usually within the next months), action (overt modifications in one’s lifestyles within the past 6 months) and maintenance (work to avoid relapse and are most often less tempted to deteriorate).9 Knowledge of patients’ TTM stages assists healthcare providers in delivering appropriate support, and in assessing the circumstances for modifying their lifestyle behaviours.10 In a previous study, interventions individually arranged in accordance with patients’ TTM stages led to weight loss, and were associated with the development of motivation for changes in lifestyle behaviours.8
Overweight and/or obesity is associated with various occupational factors, including the work schedule. Currently, about 20% of workers worldwide are believed to be working in night or shift schedules.11 12 A meta-analysis including 28 studies indicated that night/shift work was associated with an increased risk of overweight and obesity.13 14
Several studies have found that poor motivation may be a barrier to behavioural change in adults with overweight and obesity.14 15 Based on previous studies, it is possible that poor-worktime arrangements, such as long work hours and shift work, may discourage motivation for a healthy life and increase the risk of overweight and obesity through an unhealthy diet and reduced physical activity.16 However, little is known about the association between work schedules and behavioural change in workers with overweight or obesity.
In this study, we investigated the cross-sectional association between work schedules and change of lifestyle behaviours in workers with overweight or obesity. This was based on the relatively large volume of data from annual health check-up examinations in Japan.
Methods
Participants
This was a cross-sectional observational study. We used the data from participants attending the Health Examination Centre of the Urasoe General Hospital between April 2014 and March 2016. More than 25 000 individuals visit this centre to undergo annual examinations for health check-ups. All participants were asked about their work schedule, motivation for lifestyle change, health-related habits and medical history during each examination using standard self-administered questionnaires.
The inclusion criteria were as follows: age between 20 and 65 years, body mass index (BMI) ≥25 kg/m2 and working full time.2 17–19 Subjects with missing information on stages of change (SOC) for lifestyle and work schedules, and pregnant women were excluded.
Data collection
We used a self-administered questionnaire to collect information regarding comorbidities, medications, lifestyle behaviours (eating, exercise, sleep, among others), work schedule, average working hours per day, habits of smoking and alcohol drinking and SOC for lifestyle. Height and weight were measured automatically at the study visit without shoes or heavy clothing in order to calculate BMI (kg/m2).
Exposure
The primary exposure was type of work schedule, which was categorised into two groups, namely, night/shift work and daytime work. Each participant was questioned on the working history based on a self-administered questionnaire, which included the work schedule (daytime work, night work, shift work and other employment, such as part-time jobs) and the average working hours per day (within 8, 9, 10, 11 and ≥12 hours). In the questionnaire, participants were asked whether they were employed in daytime work, night work (permanent night shift, night and daytime shift), shift work and other employment (eg, part-time jobs). We categorised participants into two groups: participants who responded to ‘daytime work’ were considered to be ‘daytime workers’ and those who responded to ‘night work’ or ‘shift work’ were considered to be ‘night/shift workers’ respectively. In addition, we did not include participants who answered ‘other employment’ or not answered their work schedules.
Outcomes
In accordance with previous studies, the primary outcome was demonstration of action or maintenance stages for lifestyle based on TTM SOC.6 8 20 We investigated the SOC for lifestyle using the same questionnaire. In the questionnaire, participants were asked about their motivation for behavioural change of lifestyle (eg, daily activity, eating behaviours) and instructed to choose from these answers which reflected five stages in TTM, as follows: ‘I do not plan to change lifestyle behaviours during the next 6 months’ (precontemplation), ‘I am planning to change lifestyle behaviours during the next 6 months’ (contemplation), ‘I am planning to change lifestyle behaviours during the next month’ (preparation), ‘I have changed lifestyle behaviours for less than 6 months’ (action) and ‘I have changed lifestyle behaviours for more than 6 months’ (maintenance).
Statistical analysis
To describe the characteristics of the groups, categorical variables have been presented as counts and percentages. Continuous variables with normal and skewed distributions have been presented as the mean (SD) and median (IQR) values, respectively. In order to evaluate the association between demonstration of action or maintenance SOC and work schedules (daytime vs night/shift), a multivariable logistic regression model was used to calculate the OR and the 95% CI. Adjustments were made for potential confounding factors including age (<40 years vs ≥40 years), sex, BMI (25–29.9 kg/m2 vs ≥30 kg/m2), comorbidities such as diabetes (defined as fasting plasma glucose≥7.0 mmol/L (126 mg/dL), postprandial plasma glucose≥11.2 mmol/L (200 mg/dL), HbA1c≥6.5%, self-reported diabetes previously diagnosed by physicians or use of antidiabetic agents),21 coronary artery disease, cerebrovascular disorders, any cancer, current smoking (yes vs no), alcohol habits (<3 times/week vs ≥3 times/week), average working hours per day (<10 hours vs ≥10 hours)22 and hours of sleep per day (<7 hours vs ≥7 hours).23 We also performed an analysis after re-categorising the work schedule into three groups, namely daytime, night and shift work, using the same model as that of the primary analysis.
Further, subgroup analyses for the main outcome, and interactions between work schedules and prespecified subgroups, which were thought to be important for possible interactions and clinical implications, were evaluated using multivariable logistic regression models. The subgroups were based on: age (<40 vs ≥40 years), sex, BMI (25.0–29.9 vs ≥30), current smoking (yes vs no), alcohol habits (<3 times/week vs ≥3 times/week), hours of sleep (<7 hours vs ≥7 hours) and working hours (<10 hours vs ≥10 hours). In addition, interactions between work schedules and prespecified subgroups were evaluated in the multivariable logistic regression models.
We also performed secondary analysis to assess the relationship between work schedules and obesity-related lifestyle behaviours, namely, skipping breakfast (<3 vs ≥3 times/week), having dinner immediately before bedtime (dinner within 2 hours of bedtime; <3 vs ≥3 times/week), taking snacks after dinner (<3 vs ≥3 times/week), drinking sweet beverages (<1 vs ≥1 bottle/day), eating until full, eating quickly and doing moderate exercise (≥30 min moderate exercise more than twice a week for ≥1 year; yes vs no). Since the missing data in the present study were <5%, we performed complete case evaluation for all multiple regression analyses. A two-tailed P-value<0.05 was considered to be statistically significant. All analyses were conducted using the Stata version 15.0 (Stata Corporation, College Station, TX, USA) software package.
Patient and public involvement
There was no patient and public involvement.
Results
Participant flow
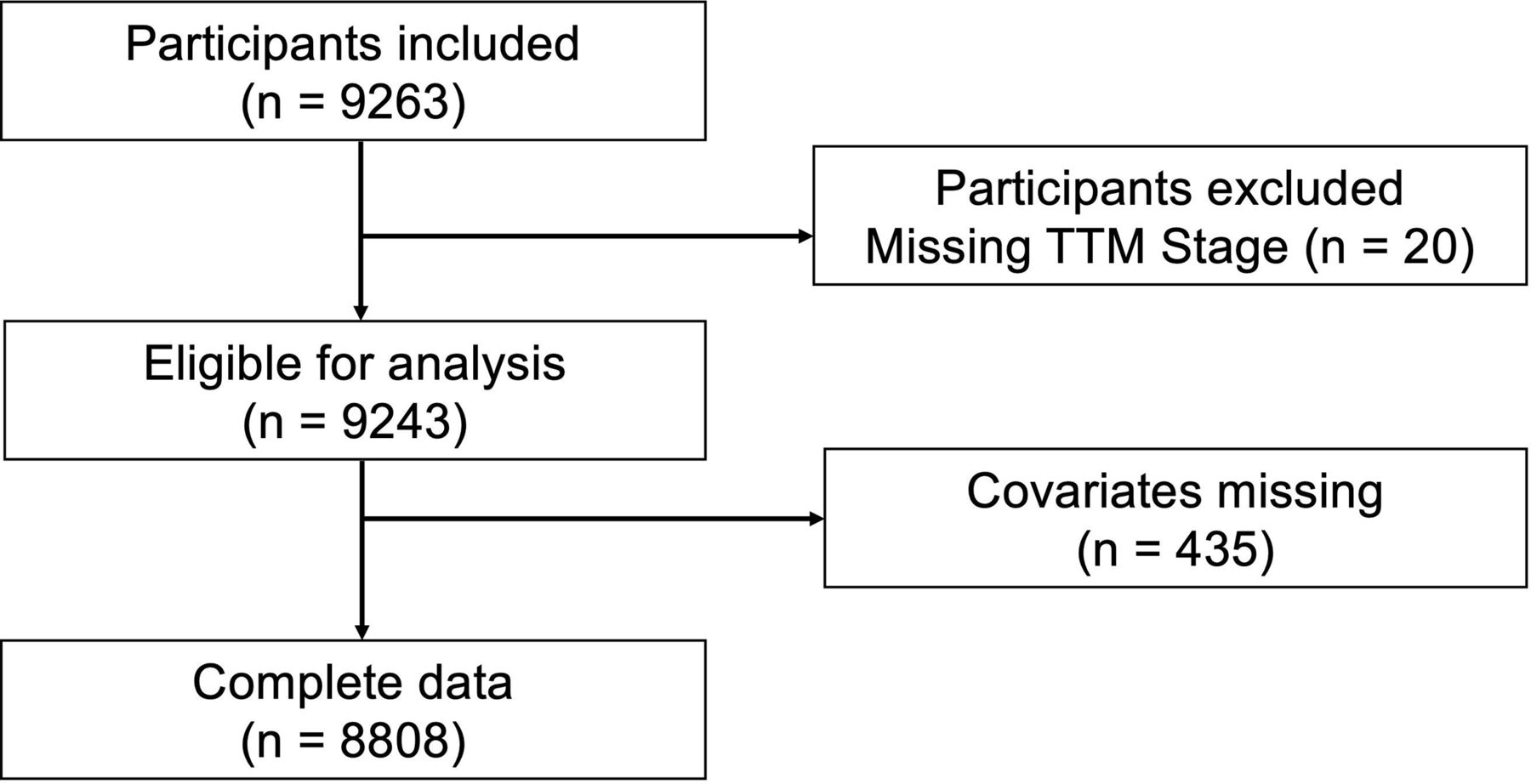
A total of 38 029 participants underwent healthcare examinations between April 2014 and March 2016. We included 9263 participants who met the inclusion criteria; 20 participants who met the exclusion criteria were excluded. In addition, only 0.2% of participants (n=20) had absent information on TTM stage. The remaining 9243 patients were eligible for analysis (figure 1).

Flow diagram of the study. TTM, the transtheoretical model.
Participant characteristics
The demographic characteristics of the daytime and night/shift workers are shown in table 1. The night and shift workers were combined for analysis in view of the sample sizes and cohort characteristics. Overall, the median age of the participants was 46 years, and 73.2% were male; the median BMI was 27.3. A total of 1390 participants (15.0%) were night/shift workers. Compared with daytime workers, night/shift workers were younger (median age: 46 vs 43 years), had fewer male workers (75.4% vs 60.9%), had higher BMI (median: 27.3 vs 27.7) and reported lower alcohol intake (52.2% vs 42.0%).
Baseline characteristics stratified by work schedule
The characteristics of participants with missing covariates are shown in online supplementary table 1. The majority of missing covariates were related to diabetes (341 participants).
Supplemental material
Association between work schedules and SOC for lifestyle based on TTM
The primary outcome, demonstration of action and maintenance SOC for lifestyle, was observed in 2113 (26.9%) and 309 (22.2%) daytime and night/shift workers, respectively. Multivariable logistic regression showed that night/shift workers were less likely to demonstrate action or maintenance SOC than daytime workers (adjusted OR (AOR): 0.85, 95% CI: 0.74 to 0.98) (table 2).
The association between work schedules and SOC for lifestyles based on TTM—OR for demonstration of action or maintenance stages
While recategorising the work schedule into three groups, the association was consistent with that of primary analysis; compared with daytime work, night work (AOR: 0.84, 95% CI: 0.66 to 1.07) and shift work (AOR: 0.85, 95% CI: 0.72 to 1.01) was associated with lesser action or maintenance SOC (online supplementary table 2).
Subgroup analysis
On subgroup analysis, the association between work schedules and demonstration of action and maintenance SOC did not differ by prespecified subgroups except for the longer work hour (≥10 hours/day) subgroup (figure 2), when participants were limited to those with long working hours, results revealed a strong inverse association between night/shift work and action and maintenance SOC (AOR: 0.65, 95% CI: 0.48 to 0.86). A significant interaction was observed between long working hours and night/shift work (P for interaction=0.04).

{kind=link}
{kind=link}
Adjusted ORs for primary outcome (demonstration of action or maintenance stages) in selected subgroups. *Each OR (for primary outcome: demonstration of action or maintenance stages) was adjusted for age (<40 years vs ≥40 years), sex, comorbidities (diabetes, CAD, CVD, cancer), BMI (25–29.9 kg/m2 vs ≥30 kg/m2), current smoking status (yes vs no), alcohol habits (<3 times/week vs ≥3 times/week), hours of sleep (<7 hours vs ≥7 hours), hours of work (<10 hours vs ≥10 hours). Interactions between work schedules and prespecified subgroups were evaluated in the multivariable logistic regression models. BMI, body mass index; CAD, coronary artery disease; CVD, cerebrovascular disorder; SOC, stages of change.
Secondary analysis
On secondary analysis, multivariable regression analyses showed that night/shift workers were more likely to have some lifestyle behaviours, namely, skipping breakfast, having dinner late, taking snacks after dinner and drinking sweet beverages (table 3).
The association between work schedules and lifestyle behaviours—ORs (95% CI) in night/shift workers for each lifestyle behaviour
Discussion
In this observational study, we found that compared with daytime workers with overweight or obesity, those involved in night/shift work were less likely to be motivated to change their behaviour. There was a positive relationship between night/shift work and certain actual unhealthy lifestyle behaviours. When we assessed the interaction between work schedules and long working hours, the relationship between night/shift work and motivation for behavioural change was strengthened. In conjunction, these findings indicate that work schedules may be associated with the workers’ motivation to modify their unhealthy behaviour, particularly in night/shift workers who engage in long hours of work.
To explain the relationship between work schedules and obesity, previous studies have focused on the endocrine mechanisms and circadian rhythm.16 24 According to the endocrinal model, work-related stress may cause neuroendocrine stress, which leads to increased secretion of cortisol, catecholamines and interleukin-6, that may lead to fat accumulation, insulin resistance and lipid abnormalities. In addition, night/shift work disturbs the circadian rhythm, restricts sleep and increases neuroendocrine stress, which may cause overweight and obesity. Behavioural change is also an important factor to clarify this relationship. In terms of behavioural change, psychosocial stress induced by work-related stress may lead to an unhealthy lifestyle.16 Lower motivation for healthy lifestyle behaviours may indirectly increase the risk of weight gain and obesity. The factors include an unhealthy diet, which includes fatty and sweet foods, sedentary behaviour when not working and reduced sleep. Hence, motivation and lifestyle can be modifiable through behavioural pathways, some studies have described the progression of this development based on the hypothesis that the SOC (progressing to action and maintenance stages in TTM) may be closely associated with lifestyle and weight changes. One randomised controlled clinical trial reported that interventions focused on TTM led to a higher progression to action or maintenance stages, and a loss of body weight in obese participants.8 Another randomised controlled clinical trial found that TTM-based care significantly improved the lifestyle compared with usual care, which included factors such as calorie intake from fat, vegetable consumption and duration of exercise.6 20 In the present study, we found that night/shift workers were less motivated to change their lifestyles. Based on the previous results, a plausible explanation for the association found in the present study is that night/shift work may cause work-related stress, which is one of the factors known to lower motivation for changing an unhealthy lifestyle. Since TTM-based care addresses stress-related lifestyle issues, it is able to address the stress associated with night/shift work.
In the present study, in addition to the association between work schedules and motivation for healthy lifestyle, we also investigated the direct association between work schedules and various unhealthy lifestyle behaviours, namely, skipping breakfast, having dinner immediately before bedtime, taking snacks after dinner, eating until full, drinking sweet beverages, eating quickly and not doing moderate exercise.25–28 Among these unhealthy lifestyle behaviours, statistically significant associations were observed between night/shift work and skipping breakfast, having dinner immediately before bedtime, taking snacks after dinner and drinking sweet beverages. Although not significant, there was a tendency for night/shift works to engage in several other unhealthy lifestyle behaviours, such as eating until full, eating quickly and not doing moderate exercise. Previous studies have revealed the association between obesity and unhealthy lifestyles.25–28 A possible explanation is that night/shift workers are forced to change their lifestyles for their work-related schedule, our results confirm that participants with overweight or obesity were at a higher risk of having unhealthy lifestyles if they were night/shift workers. Therefore, the present study indicates that night/shift workers with overweight or obesity require particular care. For example, advice for night/shift workers on topics such as eating patterns on night/shift work, timing of naps and sleeping patterns after night/shift work might be useful.24 29
On subgroup analysis, we found that night/shift workers with overweight or obesity who work for long hours were less likely to demonstrate action or maintenance SOC. The P-value for interaction was statistically significant, suggesting that long working hours had an interaction effect on the association between night/shift work and lower motivation for healthy lifestyles. Similar to night/shift work, long working hours increase the risk of overweight or obesity by the mechanism of endocrine pathway and behavioural pathways. In addition, systematic reviews have reported that shift workers have an increased risk of overweight or obesity13 30; some studies have reported a positive association between long working hours and obesity.16 31 32 However, these studies did not include work schedules. In view of the findings from these prior studies and knowledge on behavioural pathways,16 our findings suggest that night/shift workers with long working hours may be at a higher risk of overweight or obesity owing to difficulties in choosing a healthy lifestyle. Since night/shift workers are indispensable to society, they should avoid working for long hours to ensure good health.
The present study has several strengths. First, our study includes a relatively large sample, with little missing data (4.7%). Second, to the best of our knowledge, this is the first study to examine the relationship between work schedules and motivation for behaviour change in workers with overweight or obesity. Third, since we had data on both, work schedules and working hours, we could examine the relationship in detail, using interaction terms.
However, our study has limitations. First, our findings were based on cross-sectional evaluation. Associations found in our study did not confirm the causal relationship though motivation of workers may be less likely to affect work schedules. Second, in the questionnaire, SOC in TTM evaluated all aspects of the lifestyle, and was not restricted to overweight and obesity. Therefore, the responses to the SOC did not specifically reflect motivation related to overweight and obesity, but also to other unhealthy lifestyle behaviours, namely, smoking, drinking and shorter hours of sleep. We accordingly investigated the association of other unhealthy lifestyle behaviours during subgroup analysis. A similar tendency was noted irrespective of other unhealthy lifestyle behaviours. Third, since the work schedule was assessed by a questionnaire, a possibility of misclassification remains. For example, in our questionnaire, the participant might not clearly differentiate ‘night work’ and ‘shift work’ in their timetables. Therefore, some misclassification may have occurred between ‘night work’ and ‘shift work’. However, any bias introduced by this misclassification in the primary analysis would be small. Fourth, adjustment using unmeasured confounders, such as education, income, detailed physical activity levels and type of work was not possible. Fifth, although there was a statistically significant relationship between work schedules and SOC in the main analysis, the difference between day and night/shift workers in the action or maintenance SOC was not substantially large (4.7%). Finally, our cohort comprised individuals who underwent healthcare examinations at a single centre; therefore, these findings may not be generalised to other populations. Further studies including more diverse populations are warranted.
Conclusions
In conclusion, in workers with overweight or obesity, work schedules were found to be associated with motivation for behaviour change, particularly in those working for long hours. Further research is needed to understand the detailed association between work schedules, motivation and behaviour changes among various types of workers.
Acknowledgments
The authors would like to thank Y. Uehara from the Healthcare Examination Centre Urasoe General Hospital, who assisted with data extraction and management, and all individuals who cooperated in conducting this study.
References
Footnotes
Contributors YT, MK, SF and YY designed the research. YT, MI and TH conducted the research. YT and YY analysed the data. YT, MK and YY prepared the manuscript. YT had primary responsibility for the final content. All the authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval It adhered to the principles of the Declaration of Helsinki, and was approved by the ethics committee of the Kyoto University Graduate School and Faculty of Medicine (approval number: R-1345).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.