Article Text

Abstract
Introduction Many medicines have adverse effects which are difficult to detect and frequently go unrecognised. Pharmacist monitoring of changes in signs and symptoms of these adverse effects, which we describe as medicine-induced deterioration, may reduce the risk of developing frailty. The aim of this trial is to determine the effectiveness of a 12-month pharmacist service compared with usual care in reducing medicine-induced deterioration, frailty and adverse reactions in older people living in aged-care facilities in Australia.
Methods and analysis The reducing medicine-induced deterioration and adverse reactions trial is a multicentre, open-label randomised controlled trial. Participants will be recruited from 39 facilities in South Australia and Tasmania. Residents will be included if they are using four or more medicines at the time of recruitment, or taking more than one medicine with anticholinergic or sedative properties. The intervention group will receive a pharmacist assessment which occurs every 8 weeks. The pharmacists will liaise with the participants’ general practitioners when medicine-induced deterioration is evident or adverse events are considered serious. The primary outcome is a reduction in medicine-induced deterioration from baseline to 6 and 12 months, as measured by change in frailty index. The secondary outcomes are changes in cognition scores, 24-hour movement behaviour, grip strength, weight, percentage robust, pre-frail and frail classification, rate of adverse medicine events, health-related quality of life and health resource use. The statistical analysis will use mixed-models adjusted for baseline to account for repeated outcome measures. A health economic evaluation will be conducted following trial completion using data collected during the trial.
Ethics and dissemination Ethics approvals have been obtained from the Human Research Ethics Committee of University of South Australia (ID:0000036440) and University of Tasmania (ID:H0017022). A copy of the final report will be provided to the Australian Government Department of Health.
Trial registration number Australian and New Zealand Trials Registry ACTRN12618000766213.
- adverse drug events
- cognition
- nursing homes
- pharmacist
- physical activity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The proposed pharmacist service in aged-care facilities is currently not available in any private or public setting in Australia.
Use of validated tools such as the Montreal cognitive assessment, dynamometer and activity tracker will allow pharmacists to actively detect deterioration in residents’ condition.
Excluding people with moderate or severe dementia and people with significant existing frailty burden mean that the proportion of residents who could be involved in the trial is likely to be low.
Introduction
Multiple medicine use is common in older people living in aged-care facilities, with a 2015 systematic review reporting that up to three-quarters of all residents take more than nine medications.1 The use of multiple medicines places older people at increased risk of harm. Up to 30% of unplanned hospital admissions in the population 65 years and over are medication-related and the majority of these are preventable.2–5 Assessment of medication reviews demonstrates that harm is frequent in the aged-care sector, with one review of 500 persons finding that there were on average three medication-related problems per person; 16% were identified as problems related to risk of adverse reactions.6 In a second study in the Australian aged-care setting, pharmacists retrospectively assessed medication-related problems for 847 residential medication management reviews (RMMRs).7 Overall, 98% of the residents had at least one medication-related problem identified by the pharmacist, with an average of three problems per person; an adverse medicine event was present among 15% of residents.7 Adverse medicine events encompass adverse drug reactions as well as harm that results from medication errors or system failures associated with the manufacture, distribution or use of medicines.8
In addition to recognised adverse medicine events, many medicines often have what might be considered ‘minor side effects’ which are difficult to detect and frequently unrecognised. These side effects, particularly if the cumulative effects build over time, may be misattributed as geriatric syndromes, frailty or ‘changes due to aging’. We describe these cumulative effects as medicine-induced deterioration,9 which encompasses symptoms such as cognitive and functional impairment, the latter of which may be due to muscle weakness or neuropathy, sedation that reduces physical activity, or falls. Additional symptoms that can be medicine-induced include loss of appetite, changes in urinary function and bowel function, changes in respiration and changes in activity or sleep patterns. While these symptoms may occur independently of medicine use, many medicines have side effect profiles that may cause or contribute to these symptoms. Medicine-induced deterioration can be further exacerbated where medicines with differing indications but similar or overlapping side effect profiles are used concurrently.
Medicines can affect a range of physiological systems including cognitive and physical function, both of which are components of frailty.10 This may partially explain the reason why there is significant evidence demonstrating that medicine use is associated with frailty.11–13 Frailty is a risk factor for adverse events including falls, delirium and hospitalisation,14 and frail individuals have worse health outcomes than non-frail individuals.11 12 15 Theoretically reducing medicine-induced deterioration would therefore reduce the potential for people to develop frailty and thus reduce the potential for adverse medicine events. Emerging longitudinal evidence suggests that medicines may worsen frailty, with longitudinal evidence showing that the cumulative load of anticholinergic and sedative medicines is associated with increased risk of developing pre-frail states.16 Once frail, individuals are also more vulnerable to adverse drug reactions.17 An Irish study demonstrated that the odds of developing an adverse reaction in frail persons were double that of a non-frail person (29% compared with 17% respectively, OR 2.1 (95% CI 1.5 to 3.0).17
We therefore hypothesise that pharmacist monitoring of residents’ signs and symptoms of medicine-induced deterioration, including changes in mobility, cognition and strength, can prevent deterioration and reduce the risk of frailty. By detecting the immediate and cumulative influence of medicine use on cognitive and functional ability, as well as nutrition, continence, sleep and other changes in health status, there is the potential for early detection of medicine-induced deterioration and thus prevention of adverse events. The aim of our trial is to determine the effectiveness and cost-effectiveness of a pharmacist intervention compared with usual care in reducing medicine-induced deterioration, frailty and adverse reactions in older people in residential aged-care facilities in Australia. The term residential aged-care facilities is synonymous with nursing homes in the USA where care is provided 24 hours a day, 7 days a week to relatively frail older residents.
Methods and analysis
Study design and setting
The reducing medicine-induced deterioration and adverse reactions (ReMInDAR) trial is a multicentre, open-label, randomised controlled trial with residents allocated in a 1:1 ratio (figure 1). Randomisation will be stratified at the level of the individual and not at the level of the facility. A list of resident randomisation codes and unique resident identification numbers will be generated electronically for each aged-care facility.

ReMInDAR trial flow chart. Study participants will be recruited from aged-care facilities and allocated in a 1:1 ratio to receive either the sessional pharmacist visit or usual care. Study outcome measures will be collected by RA at baseline, 6 months and 12 months. RA, research assistant; ReMInDAR, reducing medicine-induced deterioration and adverse reactions.
A total of 354 residents will be recruited from 39 participating residential aged-care facilities across South Australia and Tasmania in Australia. Recruitment and pharmacist intervention will be rolled out for each site between August 2018 and June 2020. The ‘intervention’ is a sessional pharmacist assessment which will occur every 8 weeks at each facility for 12 months. Residents randomised to the control group will receive usual care provided under the existing aged-care pharmacist service agreement including medication dispensing and RMMR.
Recruitment
Study participants will be recruited from 39 aged-care facilities across two Australian states, South Australia and Tasmania in Australia. Recruitment materials in the form of flyers will be distributed in each residential aged-care facility. Information will be given to all potentially eligible residents informing them of the introduction of the pharmacist service.
Prior to participant recruitment, general practitioners (GPs) providing services to the aged-care facilities will receive a letter introducing the ReMInDAR trial. If the participants are assigned into the intervention group, GPs caring for the participants will receive a follow-up letter informing them of their patients’ trial allocation, and pharmacists make contact with them as appropriate.
Eligibility criteria
Residents will be included if they are using four or more medicines at the time of recruitment, or are taking more than one medicine with anticholinergic or sedative properties. Residents will be excluded if they (i) have significant existing frailty, defined as a score of 0.40 or above using the frailty index,15 (ii) have moderate or severe dementia, measured using the Psychogeriatric Assessment Scales18 or similar tools, (iii) are receiving palliative care or respite care or (iv) are involved in another research project which affects their participation in this study.
Randomisation
A list of resident randomisation codes and unique participant identification numbers (PINs) will be generated electronically for each facility. As participants enrol, they will be assigned to a treatment arm and will be allocated a PIN based on the next randomised allocation. Due to the nature of the intervention (pharmacist service), it is not possible to conceal allocation during the study period.
The statistician responsible for the main outcome analysis will be provided the PIN only and will be blinded to the intervention arm allocation. No data on the number of services provided during the course of the study will be provided to the statistician who will maintain blinding of intervention arm allocation.
Intervention
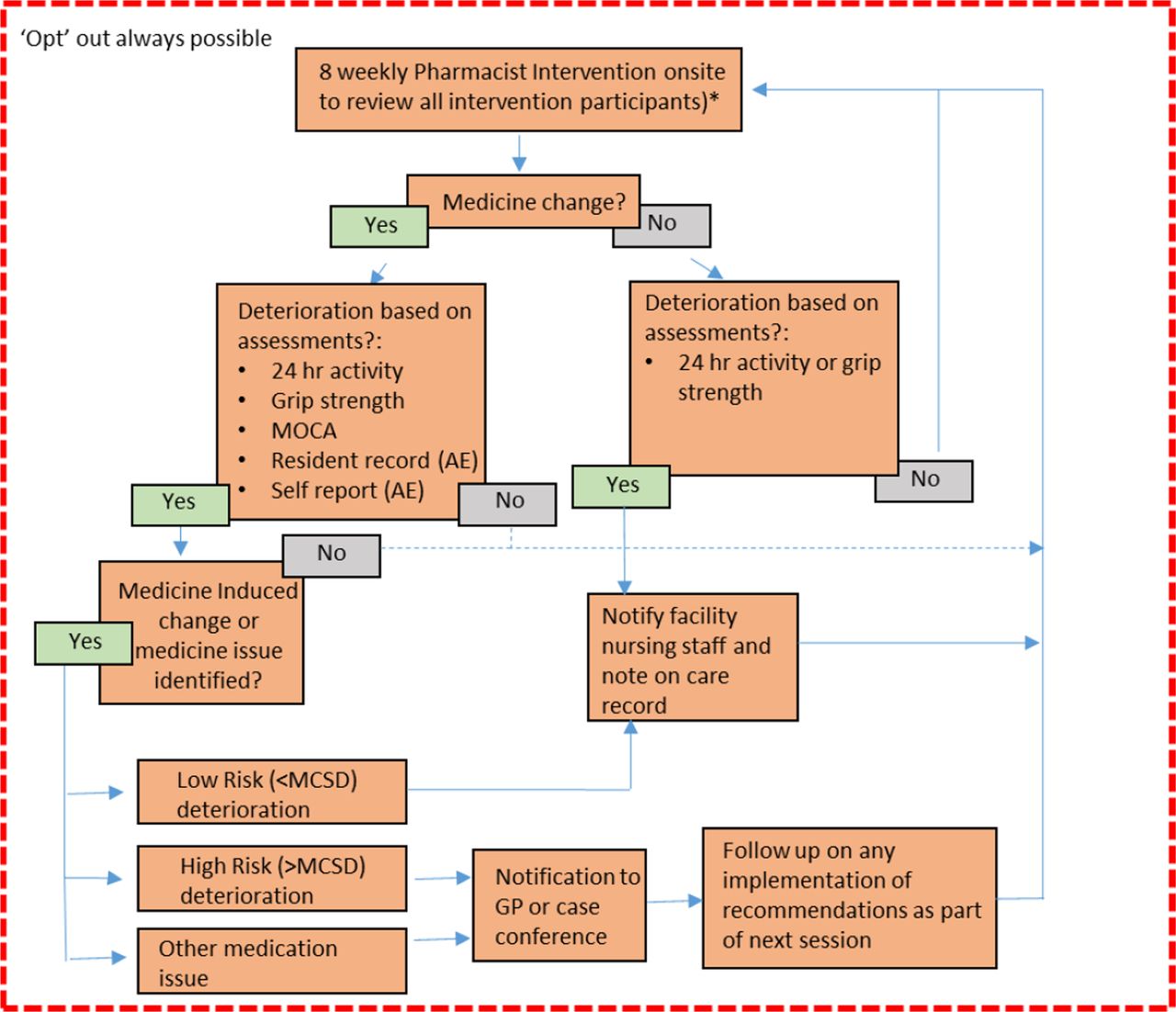
The intervention group will receive a sessional pharmacist service which occurs every 8 weeks (figure 2). The 8-weekly session is considered a feasible time frame for a potential nationally implemented service. Analysis of data from aged-care facilities showed an average of seven medication changes per resident per year, thus approximately every 2 months. Australian evidence shows that the majority of adverse events occur within the first 4 weeks of starting a medicine.19

{kind=link}
{kind=link}
Flow chart for sessional pharmacist visit which occurs every 8 weeks. Pharmacists will identify any medication changes that have occurred since the last visit, assess for medicine-induced deterioration and adverse events, interview the participants and care staff to identify any concerns and make recommendations to the GP where necessary. AE, adverse event; GP, general practitioner; MCSD, minimal clinically significant difference.
The service includes assessment for adverse medicine events and medicine-induced deterioration including assessment of cognition (using the Montreal cognitive assessment (MoCA)),20 24-hour movement behaviour including sleep (Activinsights Bands, Activinsights Ltd21 fitted for 1 year), and hand grip strength (dynamometer, Jamar).
All reviews across the 12-month period will be conducted by the same pharmacist assigned to the specific site, except under special circumstances such as pharmacist moving interstate. During the visit, the pharmacists will review electronic and/or hard copy participant care records to identify any new illnesses or conditions present since the last assessment. The pharmacists will review the care record to identify any adverse events (eg, falls, delirium events, bowel or urinary changes, weight loss) or any signs or symptoms noted in the care record that could be indicative of adverse events (eg, changes in nutritional status, pain). The pharmacists will document any adverse events detected by GPs, nurses and care staff, and detect additional adverse events based on their clinical judgement. The pharmacists will also access the medication chart to identify any medication changes that have occurred since the last visit. The pharmacist will discuss with the participants and care staff to identify any concerns that they may have.
The pharmacists will compare the results for the 24-hour movement behaviour, MoCA test, grip strength and weight with the most recent previous assessment and with baseline data to identify immediate and cumulative changes in each category. Where medicine-induced deterioration is detected in the intervention-group participants and considered clinically significant, the pharmacists will liaise with the participants’ GPs to discuss the participants’ condition, provide recommendations on medication-related problems, communicate recommended actions to and follow-up with the GP and facility staff. The pharmacists will reassess the participant at the next sessional visit to determine if medicine-induced deterioration or adverse events have resolved and document this.
Usual care
Residents in the aged-care facilities are eligible to receive RMMRs,22 and where required as part of usual care during the study period, this will still occur for participants in both intervention and control group. The RMMR is a comprehensive medication review conducted by an accredited pharmacist following a referral from the resident’s GP.22 Accredited pharmacists are funded to conduct an RMMR every 12–24 months, or where there has been a significant change in the residents’ condition or medication regimen.23
No intervention, other than usual care, will be provided to participants in the control group.
Primary outcome
The primary outcome is the reduction in medication-induced deterioration from baseline to 6 and 12 months, as measured by change in the frailty index.15
The frailty index15 is a 39-item instrument covering the following four domains: physical, medical, psychological and social. Measures within the physical domain include ability to undertake the physical activities of daily living, while within the medical domain comorbidities are included. Within the psychological domain, measures of cognitive function are assessed. Because medicine-induced deterioration is not limited to a single event, but can occur in either the physical, medical or psychological domains (eg loss of physical function or poorer cognition), an outcome measure that captures multiple domains is required. For this reason, the frailty index, which captures relevant domains, is being used as a surrogate measure of medicine-induced deterioration.
The frailty index has been validated in the population recruited for the Australian Longitudinal Study of the Ageing, where it was shown to have good predictive ability for adverse events of falls and hospitalisations.15 24
Secondary outcomes
The secondary outcomes are mentioned below.
Change in cognition scores
Changes in cognition will be assessed using the MoCA test.20 This is the same tool that will be used in the pharmacist intervention, and which is validated for screening in mild cognitive impairment.25
Change in 24-hour movement behaviour
Changes in 24-hour movement behaviour will be assessed using the GENEActiv accelerometer, a research-grade activity tracker which has been validated in adults for physical activity26 and for sedentary behaviour.27 The GENEActiv will be initialised to collect unfiltered, triaxial acceleration data at a sampling rate of 80 Hz. Output data will include number of sedentary and active bouts, sleep and active time using previously established cut-points. The GENEActiv will be worn on the wrist by participants in both the intervention and control group for a 7-day period.
Change in grip strength
Grip strength will be measured using a handheld dynamometer (Jamar). The measurement will be undertaken using the dominant hand. Three measurements will be taken and the maximum of the three scores will be used. Cut-off points for grip strength that are considered reflective of sarcopaenia are 27 kg for men; 16 kg for women.28
Change in weight
Data on the weight of participants will be extracted from the resident serial weight chart, which forms part of the resident care assessment record.
Percentage robust, pre-frail and frail
The proportion of participants who are frail, pre-frail or robust will be measured using the frailty phenotype.29 The frailty phenotype comprises five criteria: unintentional weight loss, low grip strength, self-rated exhaustion, low walking time and low physical activity. In the frailty phenotype, individuals are classified as frail if they meet three or more of the five criteria, and pre-fail if they have one or two attributes. Individuals who meet none of the criteria are classified as robust.
Rate of adverse medicine events
The rate of adverse medicine events will be measured as a composite outcome of any of the following adverse events: falls (non-injurious and injurious including fractures), delirium, faecal impaction and hospitalisation. The number of adverse medicine events will be reported per resident per year.
Change in health-related quality of life
Health-related quality of life will be assessed using the EQ-5D. The EQ-5D is a simple generic health-related quality of life measure which provides utility weights enabling cost-effectiveness analysis.30 The questionnaire contains five dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) and a visual analogue scale (range 0 to 100) representing current health state.
Change in health resource use (and costs and net costs/savings associated with the intervention)
Data will be collected on intervention-associated resource use, such as pharmacist, doctor, nursing and care staff time, changes in medication and non-medication management and resource use associated with any adverse events.
Follow-up
All participants will undertake follow-up assessments at 6 and 12 months where the research assistant will collect data on the study outcome measures.
Data collection and storage
Table 1 outlines the data that will be collected throughout the study period. Research assistants at the aged-care facilities will be responsible for collecting data for all participants at baseline, 6 months and 12 months and for entry into a custom-built web-based data management information system. The pharmacists will be responsible for collecting data on medicine changes, medicine-induced deterioration and adverse events during the sessional pharmacist visits. Data will be stored in secure settings at the Quality Use of Medicines and Pharmacy Research Centre, University of South Australia. All study data will be stored in a de-identified format.
Assessment and pharmacist service schedule
Source data documentation and monitoring
A member of the research team will check data entered by each research assistant to ensure accurate data entry. Data for the first 50 participants entered into the electronic case report forms will be cross-referenced to the original source information by two members of the research team. In addition, two members of the research team will perform on-going source data verification (10% random sample of participants’ data) and review to confirm that the source data (eg, progress notes, medication chart, outcome measures) entered by the research assistants into the electronic case report forms are accurate, complete and verifiable from the source documents. Each audit trail entry will be time-stamped, including when discrepancy occurs and data in the electronic case report forms are created, modified or deleted.
The study statistician will conduct regular remote monitoring on the web-based database by applying validation and consistency rules, with regular data cleaning to ensure the integrity of the study data.
Training
The research assistants will receive training on the protocol and procedures, administration of study measures and completion of the electronic case report forms. Standard operating procedure manuals will be supplied for the research assistants and pharmacists to ensure consistency in study operation.
Pharmacists who agree to provide intervention services under the trial will be provided a 3-hour training session prior to commencement of the service. These pharmacists have a range of community, hospital and medication review (accredited) backgrounds. The training related to the trial will cover identification of medicine-induced deterioration, use of the assessment tools (Activinsight band, handgrip dynamometer, MoCA, Resident Care Assessment Record Form), data collection and interpretation of data.
To provide further training to pharmacists in the assessments and to ensure the intervention is able to be integrated into existing work flows, the clinical research leader or experienced clinical pharmacists will provide the intervention pharmacists with on-site support during the first sessional visit. The on-site support also aims to ensure consistency in that the pharmacists can adhere to the study protocol and are able to use the standardised tools correctly. Additional on-site support and training sessions will be conducted where necessary. Pharmacists are only able to undertake independent intervention delivery once clinical research leader is confident in their capacity to implement intervention as planned. Regular pharmacist discussion groups (every 2 months) will be convened to verify effective use of the tools, to support interpretation of the data and algorithms, to provide mentoring and to discuss solutions to all identified problems.
Analysis plan
Sample size calculation
The sample size calculation is based on the primary outcome, the change in frailty over 12 months and uses data from the Australian Longitudinal Study of Ageing.31 If the intervention is assumed to prevent medicine induced frailty of half a deficit, then the treatment effect is a change in the frailty index of 0.015 with a SD of 0.06.3
Assuming a correlation in the frailty index over 12 months of 0.7, a sample size of 302 will provide 80% power with two-sided α=0.05 to detect a difference in the change in the frailty index over 12 months of half a deficit. Allowing for a loss to follow-up of 17% based on a study of 12-month death rates in Australian aged-care residents with mild to moderate frailty,32 the total sample size required is 354.
Quantitative analysis
The trial analysis will follow a pre-specified statistical analysis plan. Participants will be analysed according to the treatment they were randomised to receive using an intention-to-treat approach. Multiple imputation for missing data in the primary outcome only will be performed using a ‘Missing At Random’ assumption and the ‘de jure estimand’ approach of Carpenter et al.33
Analyses will use mixed-effects models to account for correlated measurements from the same individual over time. To test whether the outcomes differ between the intervention groups, models will include fixed effects for treatment group, time point and an interaction term between treatment group and time point. Treatment effects will be reported separately at 6 and 12 months post-randomisation and statistical significance will be assessed at the two-sided 0.05 level. Both unadjusted and adjusted analyses will be performed, with the adjusted analyses including the stratification variables (aged-care facility and gender) as covariates. If adjusting for a covariate prevents models from converging (eg, from small facilities), the covariate will be excluded and this will be noted in the reporting. Continuous outcomes will also be adjusted for baseline values. Conclusions on group differences will be based on the adjusted analyses. Planned subgroup analyses of the primary outcome are gender, baseline frailty phenotype, use of sedative and anticholinergic medications.
For continuous outcomes, linear regression models will be used with no planned data transformations. For ordinal categorical outcomes, proportional odds models will be used. Poisson or negative-binomial regression models will be used for the count outcomes, as appropriate. If the mixed models fail to converge, generalised estimating equations will be used instead.
Health economic analysis
The primary economic analysis will be a trial-based cost comparison from the perspective of the Australian healthcare system (public and private funded healthcare costs). The primary economic outcome will be average change in total health resource expenditure (net costs/ savings), associated with the pharmacist intervention, per resident, over a 1-year time horizon. These costs will be collected during the trial.
The analysis will use participant data on an ‘intention to treat’ basis (ie, residents will be analysed according to the intervention group to which they were randomised). Pharmaceutical benefits scheme (PBS) and medicare benefits schedule (MBS) administrative claims data, as well as administrative claims data for hospital admissions will be linked to the clinical effectiveness data collection set and used to inform the economic evaluation.
A trial-based cost effectiveness analysis and a trial-based cost-utility analysis will be conducted, if a reduction in medicine-induced frailty is shown. These analyses will provide preliminary first-year estimates of (i) the average incremental cost per adverse medicine event avoided and (ii) the incremental healthcare cost per quality-adjusted life year gained in health-related quality of life, as measured within trial by the EQ-5D score.
Governance
The study will be governed by the trial steering committee comprising representatives from all consortium organisations. This committee will review and agree to all study planning documents and monitor the progress of the study. A trial management plan will be the master planning document outlining all requirements for successful implementation and completion of the study. This will be supported by a communications management plan, data management plan, quality management plan and intellectual property management plan. Standard operating procedures will be established to operationalise aspects of all plans. A risk register and intellectual property register will be maintained and reviewed regularly.
Patient and public involvement
Throughout the ReMInDAR trial stakeholders will be engaged through a number of mechanisms. The two primary mechanisms include a stakeholder advisory group and a consumer reference group. Representatives from key healthcare professional organisations, including aged-care, medical and pharmacy organisations, will meet annually as a stakeholder advisory committee to provide advice and support to the study. The consumer reference group will be convened prior to the trial commencing and again during the study implementation. Subsequent meetings will occur bi-annually. Residents and carers will be engaged to provide a consumer perspective on the study activities.
The trial pharmacists and residential aged-care staff will be invited to participate in discussion groups to review the study activities and the fit of these activities into staff workflows. In addition, qualitative interviews will form part of the study evaluation to determine participant satisfaction with the service.
‘Opt out’ approach and consent to link data
The study will adopt an ‘opt out approach’, as requested by the residential aged-care facilities. In compliance with the National Statement of Ethical Conduct in Human Research section 2.3.6, flyers will be put up at all participating residential aged-care facilities at least 1 month prior to recruitment to inform the residents, family members and staff of the introduction of the pharmacist service. In addition, flyers will be provided to all potential residents. The flyer will explain the pharmacist service, information on what to do if the residents do not wish to participate and inform the residents that they can opt out at any time throughout the study period.
Our study will exclude persons with moderate or severe dementia, meaning that the eligible residents will have the capacity to decline participation if they wish to do so. Written consent will be obtained separately from residents to access their MBS, PBS and state hospital data through the respective data custodians.
Participants who have enrolled in the study can withdraw from the study for any reason or without having to give a reason.
Discussion
The proposed pharmacist service in aged-care facilities is currently not available in any private or public setting in Australia. It is expected that the proposed pharmacist service will reduce the occurrence of adverse medicine events through early detection of medication-induced deterioration. Early detection of medicine-induced deterioration and prevention of deterioration by recommending changes to medicines have the potential to significantly reduce medication-related problems and hospital admissions in older people, leading to substantial cost-savings in the Australian healthcare system. A recent study highlighted the need for well-designed, unbiased randomised controlled trials to include data relating to clinical outcomes associated with medicines use and our trial addresses this need.34
The increasingly complex healthcare system and rapid evolution of digital health tools mean it is essential to recalibrate research priorities of medicine safety to integrate consumer-based wearable technologies. In 2017, the Australian Digital Health Agency established a new Medicines Safety Programme which aims to integrate digital health within the healthcare setting to improve medicine use and safety.35 The development of digital health tools and resources creates an opportunity to understand and monitor medication safety; however, very little has been published in this field, including research involving older people living in aged-care facilities. In our study, the research-grade activity tracker (GENEActiv), which is used as a study outcome measure, provides raw triaxial acceleration data which will enable us to investigate how physical activity, including posture and sedentary behaviour (sitting or lying down) changes over 1 year in older people. In addition, use of the health professional-grade activity tracker (Activinsights) fitted over 1 year in the intervention group will allow us to actively detect deterioration in physical activity as well as understand the effects of medicine changes on physical activity in older people.
The focus of the trial is to investigate the effect of a pharmacist service to prevent deterioration caused by medicines. Studies have shown that medicine changes such as anticholinergic cessation do not improve cognitive function in people who have dementia.36 37 Therefore, we will exclude residents with moderate or severe dementia because we needed residents whose cognitive function is likely to change or deteriorate due to medicine use. In addition, residents with significant existing frailty burden, defined as frailty index score ≥0.40, will be excluded because frailty index appears to reach a plateau by 0.5,38 meaning medicine changes affecting frailty may be harder to detect in residents who have a frailty index above 0.40. The exclusion criteria mean that the proportion of residents who could be involved is likely to be low because more than 50% of residents living in aged-care facilities in Australia have dementia39 and between 50% and 90% of aged-care residents are frail.40
Continuous engagement with our stakeholder advisory group and consumer reference group will mean that the intervention is more likely to be acceptable to their needs and thus accepted into routine clinical patient care by healthcare professionals and consumers. It is anticipated that the pharmacist service will result in residents having less deterioration in physical and cognitive function, lower frailty burden and experiencing fewer adverse medicine events. If successful, the pharmacist service tested may provide a platform for a new standard of care which is likely to be easily integrated into existing practice, and which is readily accessible to residents in aged-care settings.
Ethics and dissemination
The study will be conducted in accordance with principles of the World Medical Association Declaration of Helsinki41 and the Australian National Statement of Ethical Conduct in Human Research.42 Ethics approvals have been obtained from the Human Research Ethics Committee of University of South Australia (ID: 0000036440) and University of Tasmania (ID: H0017022). The study protocol and related documents have been submitted, reviewed and approved by the ethics committees before the study initiated. During the study, any amendment to the study protocol or related documents will be submitted to the ethics committees for approval prior to implementation.
The study is registered with the Australian and New Zealand Trials Registry. Online supplementary additional file 1 lists the WHO trial registration data set for the ReMInDAR trial. Online supplementary additional file 2 lists the Standard Protocol Items: Recommendations for Interventional Trials.
Supplemental material
Supplemental material
A copy of the final report will be provided to the Australian Government Department of Health. All participating residential aged-care facilities, GPs and pharmacists may be provided with a summary of key findings. Participants and family members will be given a layperson summary if they wish to know the study results.
Acknowledgments
We would like to thank trial participants, pharmacists, general practitioners, the staff of residential aged-care facilities and research assistants for their support and participation. We would also like to thank members of the stakeholder advisory group and the consumer advisory committee for their valuable advice and support.
References
Footnotes
Twitter @DrRenly, @AndradeAQ
Contributors EER conceived the study and obtained grant funding. RL wrote the first draft of the manuscript. RL, LB, MC, LMKE, ACK, TM, GP, NLP, DR, ST, JW, JC, CS, MW and EER participated in the design of the study protocol. NLP and LK developed the statistical analysis plan. TM and CS developed the health economic analysis plan. RL, AQA and RB are involved in the development of training and implementation resources. All authors are involved in the implementation of the trial. All authors critically reviewed and approved the final manuscript.
Funding The reducing medicine-induced deterioration and adverse reactions trial is funded by the Australian Government as part of the Sixth Community Pharmacy Agreement pharmacy trial programme. The Australian Government Department of Health reviewed the manuscript before submission but played no role in the study design, data collection, management, writing of manuscript or decision to submit the paper for publication.
Competing interests The reducing medicine-induced deterioration and adverse reactions (ReMInDAR) trial is by the Australian Government. ACK is employed as a research assistant of the ReMInDAR trial. RB is employed as the ReMInDAR partnership engagement and trial manager to oversee the operations management for the trial.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.