Article Text

Abstract
Objectives To compare the prevalence of different insomnia subtypes among middle-aged adults from Europe and Australia and to explore the cross-sectional relationship between insomnia subtypes, respiratory symptoms and lung function.
Design Cross-sectional population-based, multicentre cohort study.
Setting 23 centres in 10 European countries and Australia.
Methods We included 5800 participants in the third follow-up of the European Community Respiratory Health Survey III (ECRHS III) who answered three questions on insomnia symptoms: difficulties falling asleep (initial insomnia), waking up often during the night (middle insomnia) and waking up early in the morning and not being able to fall back asleep (late insomnia). They also answered questions on smoking, general health and chronic diseases and had the following lung function measurements: forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and the FEV1/FVC ratio. Changes in lung function since ECRHS I about 20 years earlier were also analysed.
Main outcome measures Prevalence of insomnia subtypes and relationship to respiratory symptoms and function.
Results Overall, middle insomnia (31.2%) was the most common subtype followed by late insomnia (14.2%) and initial insomnia (11.2%). The highest reported prevalence of middle insomnia was found in Iceland (37.2%) and the lowest in Australia (22.7%), while the prevalence of initial and late insomnia was highest in Spain (16.0% and 19.7%, respectively) and lowest in Denmark (4.6% and 9.2%, respectively). All subtypes of insomnia were associated with significantly higher reported prevalence of respiratory symptoms. Only isolated initial insomnia was associated with lower FEV1, whereas no association was found between insomnia and low FEV1/FVC ratio or decline in lung function.
Conclusion There is considerable geographical variation in the prevalence of insomnia symptoms. Middle insomnia is most common especially in Iceland. Initial and late insomnia are most common in Spain. All insomnia subtypes are associated with respiratory symptoms, and initial insomnia is also associated with lower FEV1.
- insomnia
- respiratory symptoms
- sleep medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The strengths of this study include the population-based nature of this large sample collected in the same manner at many centres in 11 different countries.
Another strength is the use of standardised and validated procedures and instruments.
One limitation of our study is the cross-sectional study design that cannot tell us the direction of the association found since the underlying causal pathways can only be obtained from longitudinal or intervention studies.
Another limitation is the fact that we only have information on insomnia symptoms but not the diagnosis of insomnia disorder.
Introduction
A good night’s sleep is vital for daily functioning, general health and well-being.1 Sleep disturbances are highly prevalent in the general population and often have considerable impact on health and quality of life.2–4 Insomnia is categorised as difficulty falling asleep (initial insomnia), waking up often during the night (middle insomnia) and waking up too early in the morning (late insomnia).
Insomnia is common and is associated with various negative consequences for health and well-being.5 Previous studies have shown geographical variation in prevalence of sleep disturbances. Léger et al6 reported sleep disturbances, including insomnia occurring in 6.6%–37% in four countries (France, Italy, Japan and USA). Previous studies conducted in Sweden, Iceland Belgium, Great Britain, Germany and Ireland found the prevalence rates of insomnia to range from 4% to 22%.7 8 Furthermore, a study by Dregan and Armstrong9 comparing sleep disturbances and their relationship to age among subjects from 23 European countries found substantial differences in sleep patterns across these countries. A similar result was obtained in a recent study of older European adults.10 However, these studies used a single item measure of sleep disturbances and could therefore not evaluate different subtypes of insomnia.
Several studies have shown associations between insomnia and respiratory symptoms.11–14 Having asthma has been associated with a higher prevalence of insomnia,15 16 and patients with chronic obstructive pulmonary disease (COPD) commonly report disturbed sleep, including symptoms of insomnia.17 There is, however, a lack of large epidemiological studies exploring the association between different insomnia subtypes and respiratory symptoms and between insomnia and lung function using standardised methodology in a large number of countries.
The aim of the present study was to compare the prevalence of different insomnia subtypes among middle-aged subjects from 23 centres in 11 countries as well as exploring the relationship of different subtypes of insomnia with respiratory symptoms and lung function.
Material and methods
Subjects
We studied participants in the third follow-up of the European Community Respiratory Health Survey III (ECRHS III; www.ecrsh.org), an international, population-based, multicentre cohort study of asthma and allergy, which was first performed in 1990. Detailed descriptions of the methods for ECRHS I and ECRHS II have been published elsewhere.18 19 Briefly, participating centres first randomly selected samples of 20–44 year old subjects. Participants completed a short postal questionnaire about asthma and asthma-like symptoms, and from those who responded, a random sample was selected to undergo a more detailed clinical examination. In addition, a ‘symptomatic sample’ reporting symptoms of waking with shortness of breath, asthma attacks or using asthma medication in stage 1 was also studied. In ECRHS II, subjects who had participated in the clinical phase of ECRHS I were invited to participate in the follow-up. The clinical phase of ECRHS I and II was performed between 1991–1994 and 1998–2002, respectively. ECRHS III is the second follow-up and was performed from February 2011 to January 2014.19 20 The present study is based on data from ECRHS III except for change in lung function which shows the change from ECRHS I- III (see below).
Questionnaires and measurements
Subjects answered the core ECRHS questionnaires that included questions on respiratory symptoms and smoking history. The following respiratory symptoms were assessed: wheeze, nocturnal chest tightness or attacks of breathlessness following activity, at rest or at night during and attacks of nocturnal cough the last 12 months as well as usually having to cough in the morning and usually bringing up phlegm in the morning.
Sleep-related symptoms were assessed by using the Basic Nordic Sleep Questionnaire,21 where participants were asked about frequency of insomnia symptoms. Answers were on a scale of 1–5: (1) never or very seldom, (2) less than once a week, (3) once to twice a week, (4) three to five times a week and (5) every day or almost every day of the week. Insomnia symptoms were defined using answers to three questions from the BSNQ: ‘I have difficulties falling asleep at night’ (initial insomnia), ‘I wake up often during the night’ (middle insomnia) and ‘I wake up early in the morning and can’t fall back asleep’ (late insomnia). Those who reported those symptoms of insomnia ≥3 times a week (scores 4 and 5) were considered to have the appropriate subtype. At ECRHS III, forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) were recorded prebronchodilation and postbronchodilation with 200 µg salbutamol, using the EasyOne NDD spirometer. All subjects made at least five forced expiratory manoeuvres, and maximal values with up to 150 mL reproducibility were used for analysis. Predicted values were calculated using data from the Global Lung function Initiative.22 In ECRHS I and II, spirometry data were recorded similarly, but no bronchodilation was performed. Change in prebronchodilatory lung function from ECRHS I to III was calculated as change in % of predicted between the surveys.
Height and weight were measured at the time of the spirometry, and body mass index (BMI) was calculated
Patient and public involvement
Patients and public were not involved in the designing process of this study. The purpose of this research was introduced to all participating patients, and informed consents were sought from all the participants. All participants completed this survey on the voluntary basis. No patient was asked for advice on interpretation or writing up of results. The results of the research will not be disseminated to the patients.
Statistics
Data are presented as number and percentage or mean±SD, depending on distribution. The random sample from ECRHS III was used when comparing prevalence between participants from different countries. The whole sample (random and symptomatic) was used for all other analyses as our aim in these analyses was to examine associations with respiratory symptoms and lung function and not to estimate incidence rates or prevalence in a representative population. For bivariate analysis, the χ2 test, t-test and one-way analysis of variance were used for nominal and continuous variables. Logistic regression was used for multivariable analyses to estimate the association between insomnia and respiratory symptoms after adjusting for potential confounders such as sex, age, BMI and smoking status. In a previous study in the same population, we found associations between nocturnal gastro-oesophageal reflux and respiratory symptoms, while habitual snoring was independently associated with both symptoms and lung function.23 We therefore performed a sensitivity analyses including nocturnal gastro-oesophageal reflux and snoring in the multivariable analyses. STATA V.15 was used for all statistical analyses.
Results
Geographical variation
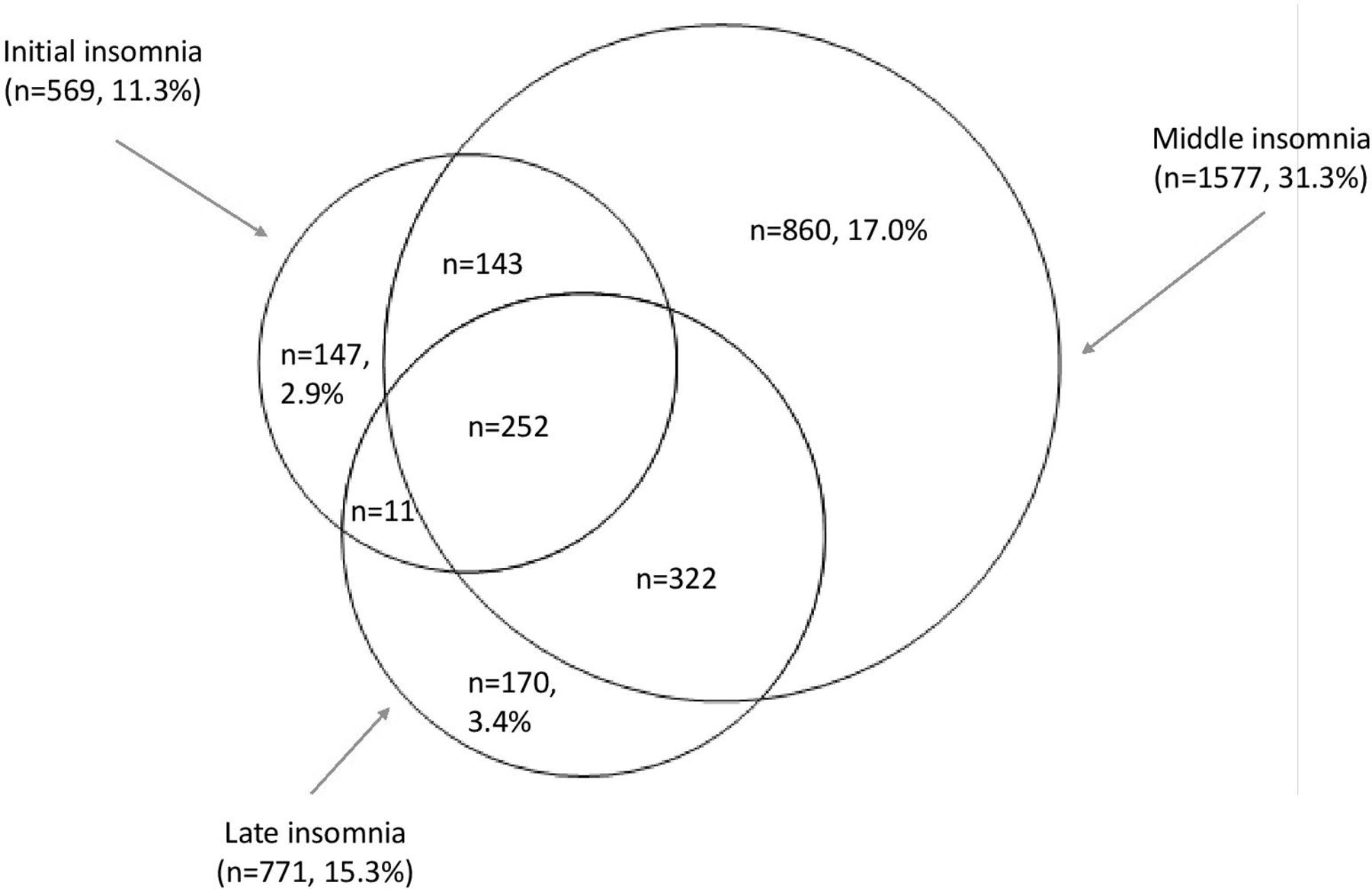
Data from 23 centres and 11 countries were gathered. Of the participants, 5043 were from the random sample.19 The overall prevalence of any insomnia symptom was 39.4%. Middle insomnia (31.3%) was the most common subtype followed by late insomnia (15.3%) and initial insomnia (11.3%) (figure 1). There was a considerable overlap between the three subtypes of insomnia (figure 1).
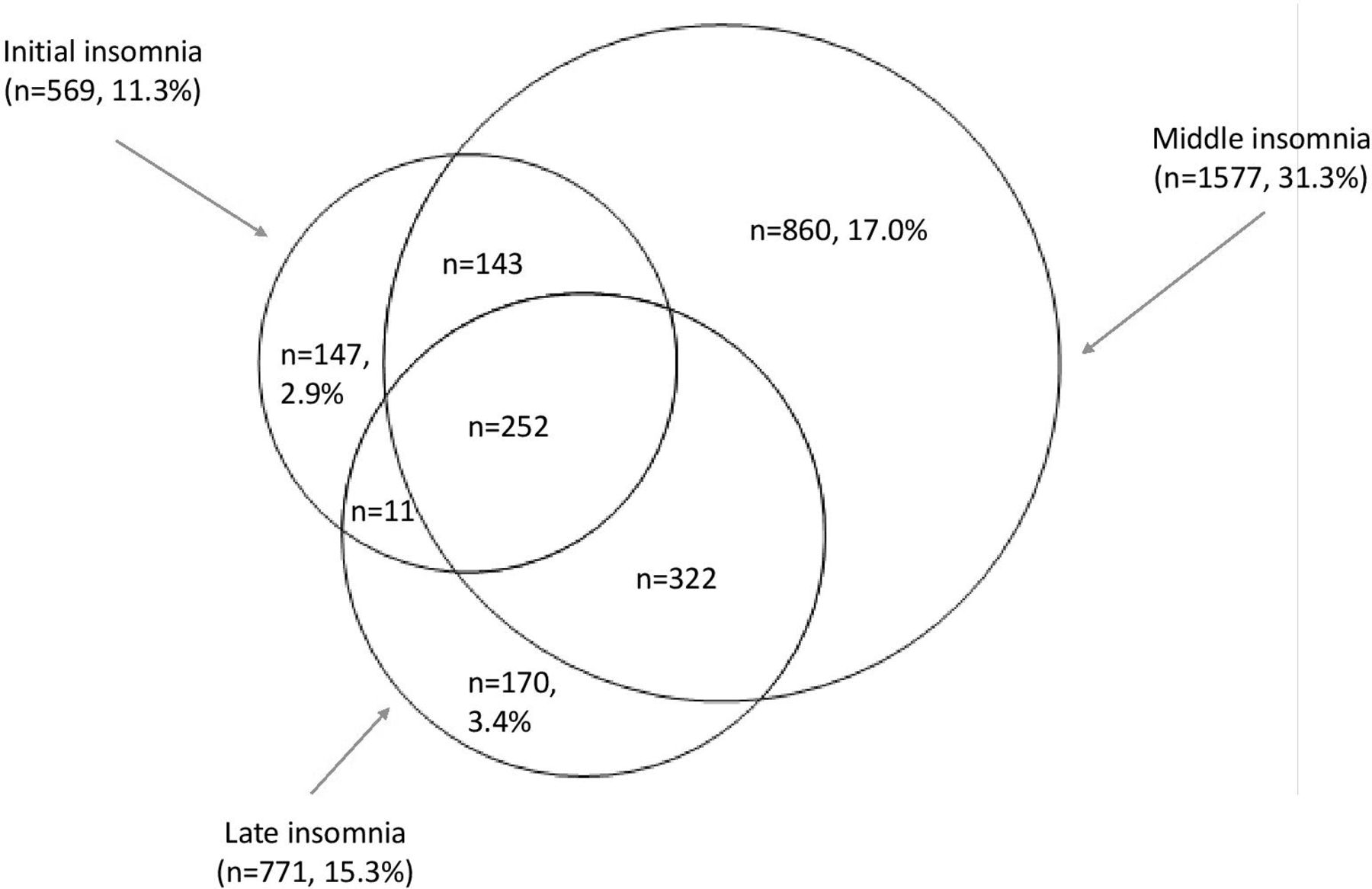
The number of subjects with different insomnia subtypes and the number with isolated insomnia subtypes in the random sample (n=5043).
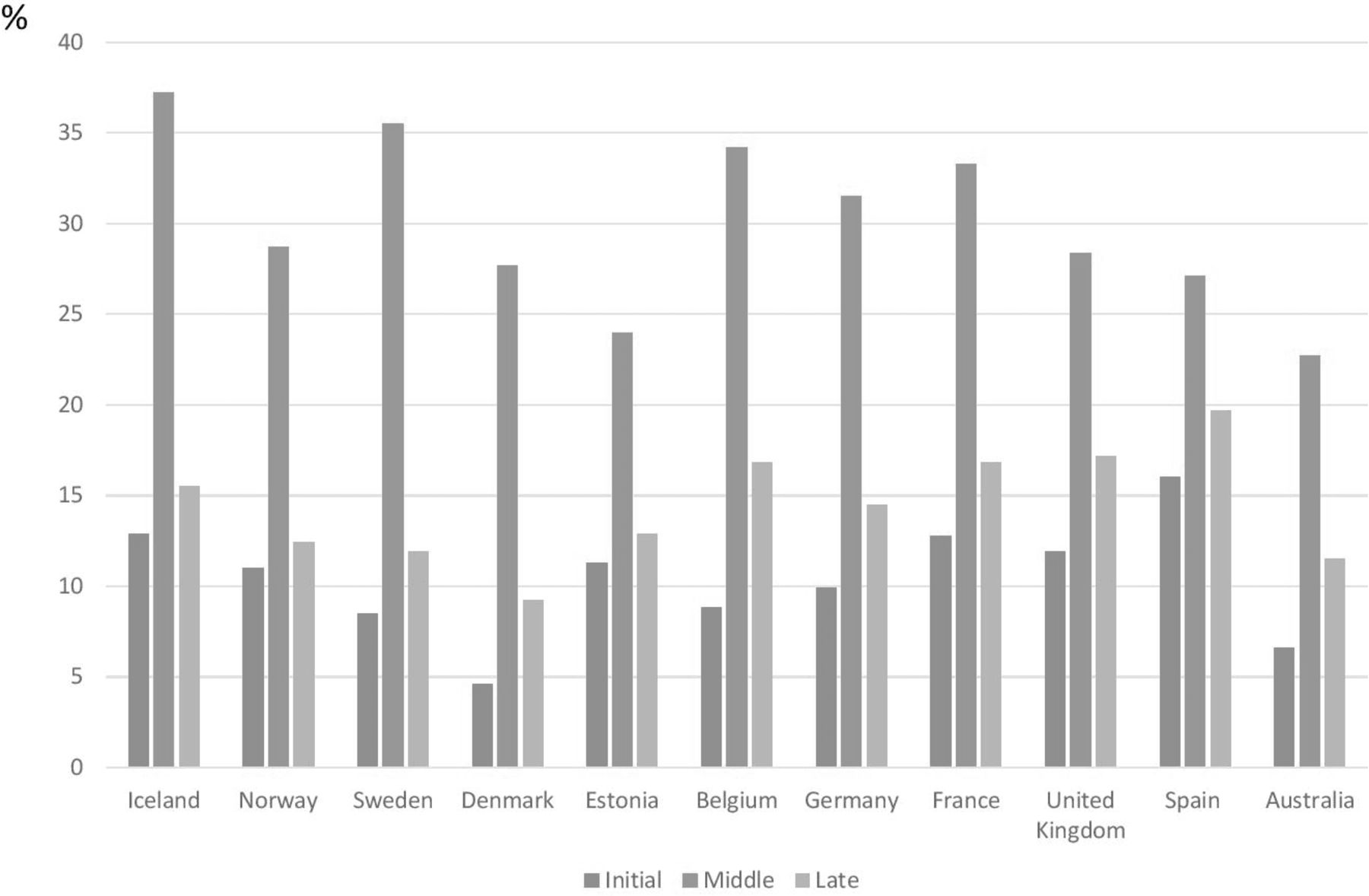
The highest prevalence of middle insomnia was found in Iceland and the lowest in Australia, while the prevalence of initial insomnia and late insomnia was highest in Spain and lowest in Denmark. The pattern of the prevalence of different subtypes was consistent across countries with initial insomnia being less common than late insomnia and middle insomnia being the most common subtype (figure 2).

{kind=link}
{kind=link}
The prevalence of the different insomnia subtypes in the different countries.
Respiratory symptoms and lung function
After including the symptomatic sample, a total of 5800 subjects were included in the analysis. The characteristics of participants with or without insomnia symptoms are presented in table 1. Subjects reporting insomnia symptoms were more often women, older, more likely to be ex-smokers and had a higher BMI.
Characteristics of the participants in ECRHS III with data on sleep disturbances (mean±SD and %)
The prevalence of most respiratory symptoms increased with the number of insomnia symptoms (table 2). There was also a significant association between lung function and insomnia symptoms for most of the lung function variables.
Association between the number of insomnia symptoms, lung function and respiratory symptoms in adults from ECRHS III (mean±SD and %)
The association between isolated insomnia subtypes and lung function and respiratory symptoms is presented in table 3. All three subtypes were associated with a higher prevalence of most respiratory symptoms. Isolated initial insomnia was significantly associated with a low prebronchodilator and postbronchodilator FEV1 and a low prebronchodilator FVC (table 3).
Association between the isolated insomnia subtypes and lung function and respiratory symptoms (mean±SD and %)
Multiple variable analyses
There was a clear independent association between the number of insomnia symptoms and all respiratory symptoms, whereas there was no association to lung function or decline in lung function after adjustment for age, sex, BMI and smoking (table 4). All three subtypes of insomnia were associated with most of the respiratory symptoms. Isolated early insomnia was independently associated with both prebronchodilatory and postbronchodilatory FEV1, whereas no association to FEV1/FVC ratio or decline of lung function as measured as prebronchodilator was found for any of the insomnia subtypes. Most associations remained statistically significant also after including nocturnal gastro-oesophageal reflux and habitual snoring in the model (table 5).
Independent association between number of insomnia symptoms and also between the isolated insomnia subtypes and lung function and respiratory symptoms expressed as adjusted beta estimates (95% CI) and adjusted ORs (95% CI)
Independent association between number of insomnia symptoms and also between the isolated insomnia subtypes and lung function and respiratory symptoms expressed as adjusted beta estimates (95% CI) and adjusted ORs (95% CI)
Discussion
In the present study, almost one out of three subjects had symptoms of middle insomnia, 14% had late insomnia and 11% initial insomnia. We have reported such high prevalence of middle insomnia (especially related to obstructive sleep apnoea),13 while other general population based studies have not found middle insomnia to be the most prevalent subtype.24 All subtypes of insomnia were related to an increased prevalence of respiratory symptoms, and having initial insomnia was also related to lower lung function. The prevalence of middle insomnia was highest in Iceland, whereas the prevalence of early and late insomnia was highest in Spain.
Others studies have not compared the prevalence of insomnia subtypes between different countries in Europe and Australia, but they have however also reported geographical differences in sleep disorders.6–10 In our previous analyses of these data as used in this one,19 we found considerable differences in sleep duration between centres, and the highest percentage of short sleepers were in the Spanish centres. In the current study, we also found a trend in Spain where both initial and late insomnia subtypes are most common there. These differences might be explained by cultural differences, working hours, unemployment and other social or economic factors, but we lack comparative data to study that further.
In the present study, we found an independent association between insomnia symptoms and respiratory symptoms. An association between insomnia and respiratory disorders such as asthma and COPD have been reported in previous studies,11 14 25 but to our knowledge, no data exist on the association between different insomnia subtypes and respiratory symptoms. A possible explanation for an association between poor respiratory health and insomnia could be some abnormal ventilatory mechanics and/or nocturnal respiratory symptoms such as cough and/or breathing difficulties.26 Within the rich ECRHS data set, we hope to be able to enlighten the ‘whole picture’ further by also evaluating the possible role of physical activity, worse general health and impaired quality of life among subjects with both insomnia and respiratory symptoms.
In accordance with previous studies, participants with insomnia symptoms in the present study had a higher BMI than subjects without insomnia.27 28 Obesity is also related to other disorders that influence sleep such as nocturnal gastroesophageal reflux (nGER) and obstructive sleep apnoea. The association between respiratory and insomnia symptoms remained significant also after adjusting for nocturnal gastro-oesophageal reflux and snoring. It further strengthens an independent association between insomnia and respiratory symptoms.
In the present study, we found that having isolated early insomnia was associated with lower FEV1. In a study by Budhiraja et al,17 FEV1 was the same among participants with insomnia compared with those without insomnia. Different insomnia subtypes were, however, not explored in their study. We did not find any significant association between insomnia symptoms and airflow obstruction (FEV1/FVC) or decline in lung function, but it is important to note that most subject in our sample had FEV1 within the normal range. These results are in line with the study of Budhiraja et al,17 although others have found an association of COPD-related variables with insomnia severity.29 Due to these conflicting results and a lack of data regarding this, further studies are needed on this topic. There are several limitations of this study that need to be considered. Our results are from a cross-sectional study, and deeper understanding of the direction of the association of underlying causal pathways can only be obtained from longitudinal or intervention studies. The questions used to assess insomnia can only provide information on insomnia symptoms, but we do not have enough information to make an insomnia diagnosis. Another limitation is that we have information about respiratory symptoms, but the occurrence of respiratory illness was not confirmed. The data on geographical variation were only obtained from a limited number of subjects from each country. The strengths of this study include the population-based nature of this large sample collected in the same manner at many centres in 11 different countries and the use of standardised and validated procedures and instruments.
Considering the prevalence and negative health consequences of both insomnia and respiratory disorders in general, these results have important clinical and public health implications. Having in mind that there is a 2–3 fold increase of reported insomnia among those with respiratory symptoms, both insomnia and respiratory symptoms should be kept in mind when either one is presented clinically. Prospective longitudinal studies need to be designed to ascertain the causality of the association between insomnia and respiratory symptoms. The traditional view is that poorly controlled respiratory symptoms cause insomnia,30 but the challenging question is whether both are contributing to a viscous circle and insomnia making respiratory symptoms like in asthma more pronounced. Awakening from sleep is associated with increased sympathetic activity and that can in turn cause airway inflammation, wheezing and coughing.30 Studies assessing the possible effect of interventions for comorbid insomnia among patients with respiratory symptoms (medications and/or cognitive behavioural therapy) might theoretically improve the clinical conditions among such patients.
To summarise, our results show a large geographical variation between different subtypes of insomnia. Symptoms of insomnia are related to respiratory symptoms and isolated initial insomnia is associated with lower FEV1. Whether improvement in insomnia affect respiratory health or whether treatment of respiratory symptoms affect insomnia is still to be investigated.
Supplemental material
Acknowledgments
The authors would like to thank all members of the research team at each centre for the patient advisers and for the assistance in data collection.
References
Footnotes
Contributors EB is the correspondence author and she drafted the paper, participated in manuscript preparation and was responsible for communication with authors and reviewing the paper in all its stages; TG and CJ participated in designing the study and in manuscript preparation; CJ performed the statistical analysis; they also reviewed the paper on several stages. EL, BB, VGL, KF, DJ, PD, JLP, JGA, SDA, JH, KT and RJ participated in data collection and reviewing the paper.
Funding Financial support for ECRHS III: Australia: National Health & Medical Research Council. Belgium: Antwerp South, Antwerp City: Research Foundation Flanders (FWO), grant code G.0.410.08.N.10 (both sites). Estonia: Tartu- SF0180060s09 from the Estonian Ministry of Education. France: (all) Ministère de la Santé. Programme Hospitalier de Recherche Clinique (PHRC) national 2010. Bordeaux: INSERM U897 Université Bordeaux segalen; Grenoble: Comite Scientifique AGIRadom 2011; Paris: Agence Nationale de la Santé, Région Ile de France, domaine d’intérêt majeur (DIM). Germany: Erfurt: German Research Foundation HE 3294/10–1; Hamburg: German Research Foundation MA 711/6–1, NO 262/7–1. Iceland: Reykjavik: The Landspitali University Hospital Research Fund, University of Iceland Research Fund, ResMed Foundation, California, USA, Orkuveita Reykjavikur (Geothermal plant), Vegagerðin (The Icelandic Road Administration (ICERA). The Icelandic Research found - grant no 1 73 701–052. Italy: all Italian centres were funded by the Italian Ministry of Health, Chiesi Farmaceutici SpA, in addition Verona was funded by Cariverona foundation, Education Ministry (MIUR). Norway: Norwegian Research council grant no 214123, Western Norway Regional Health Authorities grant no 911631, Bergen Medical Research Foundation. Spain: Fondo de Investigación Sanitaria (PS09/02457, PS09/00716 09/01511) PS09/02185 PS09/03190), Servicio Andaluz de Salud, Sociedad Española de Neumología y Cirurgía Torácica (SEPAR 1001/2010). Sweden: all centres were funded by The Swedish Heart and Lung Foundation, The Swedish Asthma and Allergy Association, The Swedish Association against Lung and Heart Disease. Fondo de Investigación Sanitaria (PS09/02457); Barcelona: Fondo de Investigación Sanitaria (FIS PS09/00716); Galdakao: Fondo de Investigación Sanitaria (FIS 09/01511); Huelva: Fondo de Investigación Sanitaria (FIS PS09/02185); and Servicio Andaluz de Salud Oviedo: Fondo de Investigación Sanitaria (FIS PS09/03190). Sweden: all centres were funded by The Swedish Heart and Lung Foundation, The Swedish Asthma and Allergy Association, The Swedish Association against Lung and Heart Disease. Swedish Research Council for health, working life and welfare (FORTE); Göteborg also received further funding from the Swedish Council for Working life and Social Research. Umea also received funding from Vasterbotten Country Council ALF grant. Switzerland: The Swiss National Science Foundation (grants no 33CSCO-134276/1, 33CSCO-108796, 3247BO-104283, 3247BO-104288, 3247BO-104284, 3247-065896, 3100-059302, 3200-052720, 3200-042532 and 4026-028099), The Federal Office for Forest, Environment and Landscape, The Federal Office of Public Health, The Federal Office of Roads and Transport, the Canton’s Government of Aargan, Basel-Stadt, Basel-Land, Geneva, Luzern, Ticino, Valais and Zürich, the Swiss Lung League, The Canton's Lung League of Basel Stadt/ Basel, Landschaft, Geneva, Ticino, Valais and Zurich, SUVA, Freiwillige Akademische Gesellschaft, UBS Wealth Foundation, Talecris Biotherapeutics GmbH, Abbott Diagnostics, European Commission 018996 (GABRIEL), Wellcome Trust WT 084703MA, UK: Medical Research Council (Grant Number 92091). Support also provided by the National Institute for Health Research through the Primary Care Research Network.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval for the study from local research ethics committees and written consent from participants were obtained. See online supplementary appendix 1.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The data that support the findings of this study are available on request from the corresponding author.