Article Text

Abstract
Objectives We assess the relationship between distance to a woman’s assigned health clinic and obstetric care utilisation.
Design We employ a cross-sectional study design using baseline data from the evaluation of a conditional cash transfer programme to promote greater utilisation of maternal and infant health services. Data were collected between December 2016 and January 2017.
Setting The study is conducted in Ngäbe Buglé, the largest of Panama’s three indigenous territories, where maternal mortality is three times the national average.
Participants We analyse a representative sample of 1336 indigenous women with a birth in the 12 months prior to the survey.
Primary and secondary outcome measures Primary outcomes include obstetric care utilisation measures for prenatal, childbirth and postpartum events. Secondary outcomes include reasons for not receiving prenatal care, alarming symptoms, child weight at birth and stillbirths or miscarriages.
Results Compared with women in closest geographic proximity to a health centre (top quintile, Q1), women who lived farthest from a health centre (bottom quintile, Q5) had significantly lower obstetric care utilisation outcomes for critical prenatal, childbirth and postpartum events. Mothers in Q5 were 36 percentage points less likely to have had at least one prenatal care appointment in a hospital, health centre or clinic compared with mothers in Q1 (p<0.01), and 52 percentage points less likely to attend an institutional first appointment (p<0.01). The gap in institutional delivery and postnatal care between mothers in Q1 and Q5 was about 35 percentage points (p<0.01). All utilisation outcomes were negatively correlated with distance, and differences in obstetric care utilisation persisted even when controlling for household wealth, maternal age and maternal education.
Conclusion Distance is an important barrier to obstetric care utilisation, with women in more distant locations suffering significantly lower use of prenatal, childbirth and postpartum care compared with women in closer vicinity to a health establishment. Expanding the supply of healthcare and implementing demand side incentives to promote the use of health services in remote communities are relevant policies to reduce disparities in obstetric care utilisation.
Trial registration number AEA Registry (RCT ID AEARCTR-0001751).
- health economics
- international health services
- tropical medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We implement a novel approach to calculating distance as a barrier to care.
We analyse rich health utilisation data for a representative sample of 1336 indigenous mothers.
Limitations of the study include analysis of self-reported utilisation outcomes and a remote study area.
Introduction
Disparities in access to healthcare and its implications for maternal and child health are a concern worldwide. The Sustainable Development Goals include a target to ‘reduce the global maternal mortality ratio to less than 70 per 100 000 live births by 2030, with no country having a maternal mortality rate of more than twice the global average’.1 Though substantial progress was made between 1990 and 2015, with a decline in maternal mortality of about 44%, there is still a far way to go to achieve this target. In 2015, 303 000 women died from pregnancy-related causes, 2.7 million babies died during the first 28 days of life and 2.6 million babies were stillborn.2 These deaths, most of which could have been prevented, reflect inequalities in access to health services and income gaps. Developing countries account for 99% of all maternal deaths globally and have a maternal mortality rate of 239 per 100 000 live births—almost 20 times higher than in developed countries (12 per 100 000).1
Indigenous populations are particularly vulnerable. In Latin America and the Caribbean, the countries with the largest populations of indigenous people and Afro-descendants have the highest maternal mortality rates. Within countries, the maternal mortality rate among indigenous women is significantly higher than among non-indigenous women. According to the World Health Organisation (WHO), indigenous women in Latin America are three times more likely to die from causes related to pregnancy and childbirth than non-indigenous women living in the same communities.3 Women living in rural areas and in low-income communities are also disproportionally affected.1
Prenatal care during pregnancy, skilled care during childbirth and support in the weeks after childbirth can be the difference between life and death for both the mother and the newborn. Nearly 75% of all maternal deaths are due to severe bleeding, infections, pre-eclampsia or eclampsia, complications during delivery and unsafe abortions—conditions that have well-known methods for prevention and management.1 In addition to increased risk of death, inadequate prenatal care has been linked to poor birth outcomes, including low birth weight and preterm birth, which have lifelong effects on child development.4 5
Though the importance of prenatal care is well known, only 64% of pregnant women globally receive at least four prenatal care visits—the amount recommended by the WHO.1 In low-income countries, the rate is only 40%, and in rural areas and poorer communities, utilisation is much lower.2 Many studies in developing countries have identified an inverse relationship between distance to a health facility and the utilisation of health services.6–12 In a systematic review of 108 studies, 77% identified a distance decay association, where patients living further away from healthcare facilities had worse health outcomes than those who lived closer.13
For indigenous women and children in Panama, one of Latin America’s highest per-capita income countries, the disparities in health access and health outcomes are equally stark. This study assesses the relationship between distance to a health clinic and the utilisation of obstetric care among households in Ngäbe Buglé, Panama’s largest indigenous territory by both geographic extension and population. We analyse an original maternal–child health survey with rich healthcare utilisation data for a representative sample of 1336 indigenous women with children younger than 12 months and use precise geo-location data to accurately measure the travel distance between households and their assigned health clinic.
Methods
Study area
Ngäbe Buglé, with 156 747 inhabitants according to the 2010 Census, is the largest of Panama’s three indigenous territories and has the highest multidimensional poverty index score of all the regions in the country (0.469).14 15 Geographically, it is very remote and comprised mostly of small and dispersed communities. Its mountainous terrain, numerous rivers and remote coastal geography make travel between communities and outside the region very difficult.16
Maternal and infant mortality and morbidity in Panama’s indigenous territories are much higher than the rest of the country. Ngäbe Buglé has an infant mortality rate of 21.4 per 1000 live births compared with the national rate of 13.9, and a maternal mortality rate more than three times the national average (162.5, 49.2, respectively).17 Prenatal care utilisation is also much lower. A qualitative study in Ngäbe Buglé identified lack of transportation, high transportation costs, high opportunity costs, lack of confidence in the quality of care, discordance between cultures and lack of empowerment as important barriers to prenatal care utilisation in the region.18
Data
We used baseline data from the evaluation of a conditional cash transfer programme implemented in Ngäbe Buglé to promote greater utilisation of maternal and infant health services. One thousand five hundred and forty-seven communities in Ngäbe Buglé were identified using the 2010 Census and all but six, which were part of an implementation pilot, were included in the sampling frame. Eight pairs of communities were very similar and geographically close to each other, therefore, for the purpose of the sampling, each pair was combined into one community to avoid contamination.
Of the eligible communities, a representative random sample of 304 communities was selected for the study. The sampling design was probabilistic, stratified and conducted in three stages. In the first stage, communities were grouped into 27 ‘population groups’ (PG), each of which was covered by a distinct health service provider. PGs were then stratified by size (greater or smaller than the median) and seven PGs were randomly selected per strata. In the second stage, communities in the selected PGs were clustered into a ‘central community cluster’ (CCC). Each CCC was comprised of one main community, the ‘central community’ (CC) and one or more smaller and more disperse communities, the ‘peripheral communities’ (PC), which were affiliated with the CC for provision of health services. A random sample of 150 CCCs, weighted by population size, was selected. In the final stage, the CC and one of its PC, in each of the 150 CCCs, were randomly selected (weighted by population), resulting in a total of 300 communities. Of these, four were among those combined to avoid contamination, so according to the Census, 304 communities in total were selected.
The baseline survey was conducted between December 2016 and January 2017 using Computerised Assisted Personal Interviews technologies. Of the 304 communities in the sample, 302 were successfully reached. The average size of each community was 163 people. All households with children younger than 12 months in each community were interviewed. Mothers were asked questions related to prenatal care, childbirth and postpartum care and their responses were recorded. One thousand three hundred and thirty-six mothers, in 274 communities and 1314 households, completed the survey and had a child younger than 12 months old. In the 28 remaining communities, there were no children younger than 12 months.
Obstetric care
The objective of this study is to understand the relationship between distance to a health facility and obstetric care utilisation before, during and after pregnancy. The primary outcomes of interest include the following utilisation measures as reported by the study subject in the baseline survey for the pregnancy of her child younger than 12 months old.
Total number of prenatal appointments.
Prenatal care, equal to 1 if mother went to at least one prenatal care appointment in a hospital, centre, or clinic and 0 otherwise.
Institutional first prenatal appointment, equal to 1 if first appointment was in a hospital, centre, or clinic and was attended by a doctor or nurse and 0 otherwise.
Number of weeks of pregnancy at first prenatal appointment.
Early and institutional first prenatal appointment, equal to 1 if first appointment was institutional and before 12 weeks of pregnancy and 0 otherwise.
Additional prenatal appointments, equal to 1 if mother went to another appointment after the first and 0 otherwise.
Institutional additional prenatal appointments, equal to 1 if additional appointments were in a hospital or health centre and attended by a doctor or nurse and 0 otherwise.
Institutional delivery, equal to 1 if the mother gave birth in a hospital or health centre and was attended by a doctor or nurse and 0 otherwise.
Postnatal care, equal to 1 if mother had a postnatal appointment within 2 days of childbirth and 0 otherwise.
Institutional postnatal care, equal to 1 if postnatal appointment was in a hospital or health centre and was attended by a doctor or nurse and 0 otherwise.
Neonatal care, equal to 1 if child had a neonatal exam within 2 days of birth and 0 otherwise.
Institutional neonatal care, equal to 1 if neonatal exam was in a hospital or health centre and was attended by a doctor or nurse and 0 otherwise.
In addition to these utilisation measures, we analysed secondary outcomes, including reasons for not receiving prenatal care, alarming symptoms during pregnancy, child weight at birth and percentage of stillbirths or miscarriages. All secondary outcomes were self-reported by mothers.
Distance calculation
All communities in Ngäbe Buglé were assigned to one of 13 public health centres located in the territory. We calculated the distance between households and their assigned health centre using Quantum Geographic Information System (QGIS) 2.18.1. First, we identified Ngäbe Buglé on Open Street Maps and downloaded a shapefile with the corresponding line network. While roads made up the vast majority of the network, the shapefile also included other polylines, such as rivers, canals, walls, pipelines, bridges and fences, among others. We kept all polylines, regardless of their type, in our calculation. We did this for two main reasons: (1) all the households are in very remote areas with a limited road network, so it is plausible that mothers travelled by water (river or canal) to reach their appointments, and (2) distances calculated from routes that follow a river, canal, fence, etc. rather than a road are likely to be closer to the true distance than the alternative option of using a linear path.
After creating three shapefiles with households, health centres and the road network, respectively, we used the QGIS Python Application Programming Interface (PyQGIS) to calculate the shortest route between each household and its assigned health centre. All overlapping lines were broken at the point of intersection. The shortest path was determined using the Dijkstra algorithm.19 20 In a few cases where the calculated routes appeared to be extremely unlikely, small gaps between road/line segments were manually connected and the routes were re-calculated. Given most households and health centres were not directly connected to any roads in the network, linear distances between the household or health centre and the edge of the calculated route were computed. The distance of the entire route, from the household to the health centre, was measured in kilometres. Route distances were then separated into quintiles, with average distances of 4.5, 12.4, 17.6, 24.9 and 50.4 km, respectively. Five households missing distance information were excluded from the analysis. A map of all the routes is shown in figure 1.

Computed routes between households and their assigned health clinics in Ngäbe Buglé, Panama.
Covariates
Wealth, age, education, number of pregnancies and empowerment are included as covariates in our regression models. Household wealth is based on self-reported data on asset ownership and housing characteristics such as floor, roof and wall materials, toilet facilities, source of drinking water, trash disposal, fuel, lighting, electricity and type of tenancy. These data were reduced into a wealth index score using principal component analysis (PCA). Mother’s age (years), education (years) and number of pregnancies were self-reported. Empowerment is a measure of a mother’s control over household decisions surrounding clothing, child education and health, finances, employment, contraception and obstetric care. An empowerment index from 0 to 1 was generated, representing the proportion of decisions the mother made out of 15 total categories.
Statistical analysis
We assessed the relationship between utilisation of obstetric care and distance by comparing mean differences in outcomes across distance quintiles. Using the computed distance for each route, we created distance quintiles in Stata 15, where Quintile 1 (Q1) corresponds to mothers in the closest 20% of households and Quintile 5 (Q5) to the furthest 20%. We analysed gaps in obstetric care between the top and bottom quintiles, in addition to gradients in healthcare utilisation across all five quintiles. Additionally, we conducted regression analysis to adjust for sociodemographic factors that may influence obstetric care outcomes. We ran an Ordinary Least Squares (OLS) regression model, specified as follows, for all outcomes:
 (1)
(1)
where  is a obstetric care outcome for mother i,
is a obstetric care outcome for mother i,  is a binary variable for the kth quintile of the distance distribution (where
is a binary variable for the kth quintile of the distance distribution (where  is the omitted reference category),
is the omitted reference category),  represents the difference in the average outcome obtained by the mothers in quintile k with respect to the average outcome in
represents the difference in the average outcome obtained by the mothers in quintile k with respect to the average outcome in  .
.  is a vector of controls for household wealth, mother’s age (years), mother’s education (years), number of pregnancies and mother’s empowerment. In the case of categorical outcomes, the OLS regression estimates a linear probability model where
is a vector of controls for household wealth, mother’s age (years), mother’s education (years), number of pregnancies and mother’s empowerment. In the case of categorical outcomes, the OLS regression estimates a linear probability model where  is the probability of Y=1 for mothers in distance quintile
is the probability of Y=1 for mothers in distance quintile  with respect to
with respect to  . Survey sampling design, including sample weights and clustering effects, was used for all analyses.
. Survey sampling design, including sample weights and clustering effects, was used for all analyses.
Patient and public involvement
Patients were not involved in the design, conception, planning, or conduct of this study.
Results
Descriptive statistics
Descriptive statistics for the 1336 mothers in our sample are presented in table 1. At the time of the survey, mothers were 26 years old, on average, and had completed 5 years of education. Only one mother was employed. Eighty-four per cent were married and the average number of pregnancies per mother was 3.6. Mothers were responsible for about 50% of household decisions as measured by the empowerment index. Those who lived closest to a health facility (Q1) were significantly wealthier and more educated than those in the farthest distance quintile (Q5) and had slightly fewer pregnancies on average.
Descriptive statistics
Gaps in obstetric care by distance
In this section, we present mean differences in obstetric care between the top and bottom distance quintiles. As seen in table 2, there are large, significant differences in all prenatal care outcomes between the two groups. Mothers in the furthest 20% of households (Q5) had 2 prenatal care appointments fewer, on average, and initiated prenatal care over 2 weeks later, than mothers in the closest 20% (Q1) of households. Additionally, mothers in Q5 were 36 percentage points less likely to have had at least one prenatal care appointment in a hospital, health centre, or clinic compared with mothers in Q1. There were also large differences of about 52 and 41 percentage points, respectively, in attending an institutional first prenatal appointment or an early and institutional first appointment between mothers in each group. The difference in attending more than one appointment was about 33 percentage points and the difference between attending more than one institutional appointment was about 43 percentage points. Reasons for not attending prenatal care were similar between groups, though mothers in Q5 were 13 percentage points more likely to consider prenatal care unimportant compared with mothers in Q1.
Gaps in obstetric care by distance. Differences in simple means
Significant gaps in delivery and postnatal care outcomes were also observed. The gap in institutional delivery between Q1 and Q5 was about 35 percentage points. Mothers in Q5 were 35 percentage points less likely to attend a postnatal appointment and 34 percentage points less likely to attend a neonatal exam within 2 days of childbirth compared with mothers in Q1. There were no significant differences in having complications or alarming symptoms during pregnancy.
The relationship between distance and final health outcomes, including child’s birth weight and per cent of stillbirths and miscarriages, is less clear. Of the 784 children who were weighed, there was no significant difference in weight between the two groups. However, there was a 38 percentage-point difference in the likelihood of being weighed between Q1 and Q5. A closer look shows that 97% of children who were weighed had an institutional delivery, which is much higher than the population average of 53.7%. This suggests that the birth weights of children who were not weighed may be systematically different from those who were. Given this is the case, we cannot adequately assess the relationship between distance and birth weight. We also found no significant differences between distance and per cent of stillbirths and miscarriages.
To assess the relationship between distance and health outcomes for different types of pregnancies, we compared gaps in utilisation between mothers with low-risk and high-risk pregnancies. Low-risk pregnancies are defined as pregnancies in women between 20 and 34 years old, inclusive, who have had three or fewer pregnancies. High-risk pregnancies include pregnancies in teens, women 35 and older and women who have had more than three pregnancies. Results are presented in online supplementary table A1. Most pregnancies in the population were high-risk (64.3%), and high-risk mothers had lower rates of utilisation than low-risk mothers. For both low-risk and high-risk mothers, there were significant gaps in utilisation between mothers in Q1 and Q5. The gaps by distance were slightly larger among high-risk mothers, but overall distance did not appear to have significant heterogeneous effects by type of pregnancy.
Supplemental material
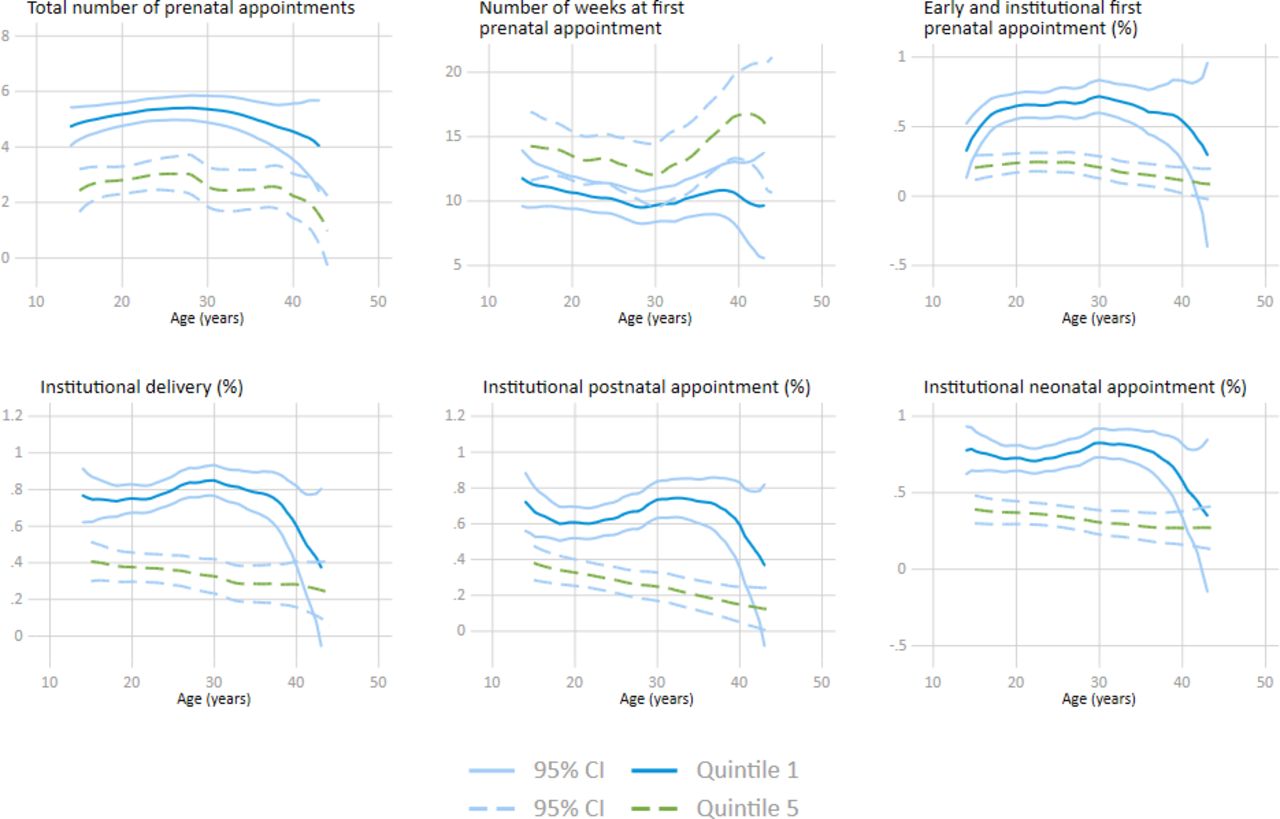
To understand how health gaps vary with regard to other key determinants, we analysed differences in obstetric care outcomes between the top and bottom distance quintiles by maternal age, education and household wealth. The results are presented in figures 2–4. In general, mothers in Q5 had inferior obstetric care outcomes across all ages, years of education and wealth levels compared with mothers in Q1. However, these gaps, especially those related to care-seeking behaviour, appear to be larger for mothers who were less educated and for mothers who lived in poorer households. Furthermore, the utilisation gap between higher and lower educated mothers was wider in Q5 compared with Q1, suggesting that distance may be a particularly salient barrier for less educated mothers. A similar trend is seen by wealth: differences in wealth among mothers in Q1 did not affect the utilisation of services much, but differences in wealth among mothers in Q5 resulted in stark inequities in utilisation. These finding suggests that mothers who were far from health centres, poor and less educated suffer the most from a lack of access.

Gaps in obstetric care by distance and maternal age.
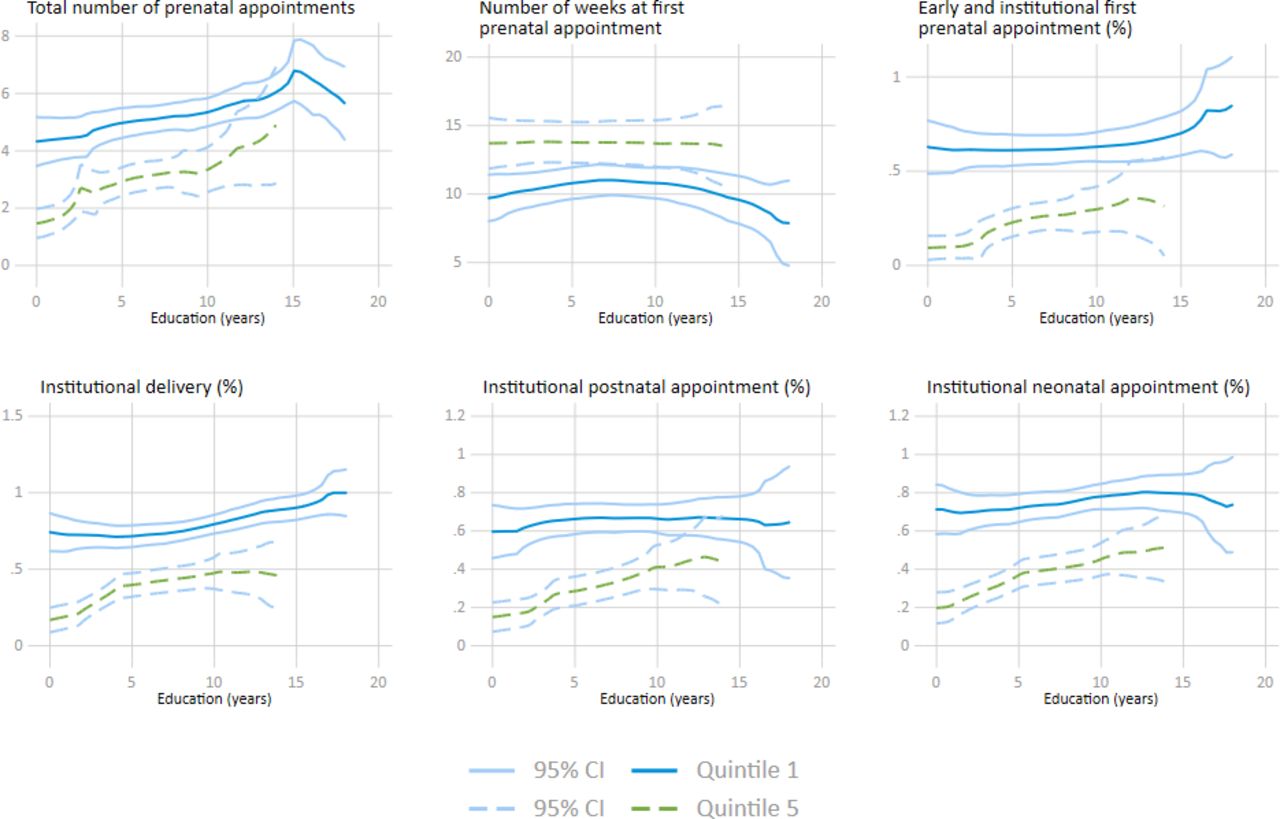
Gaps in obstetric care by distance and maternal education.

Gaps in obstetric care by distance and household wealth.
Gradients in obstetric care by distance
In addition to comparing mean differences in obstetric care outcomes for mothers in the top and bottom distance quintiles, we analysed differences in obstetric care outcomes across all five distance quintiles. As seen in figure 5, there is a strong gradient by distance among all obstetric care outcomes. With every additional quintile further away from a health centre, utilisation and early initiation of obstetric care declined.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Gradients in obstetric care across distance quintiles (Q).
We assessed the magnitude and significance of these differences using a regression model with controls for wealth, age, education, number of pregnancies and empowerment. As seen in table 3, there are strong and significant effects of distance on almost all outcomes. Compared with mothers in the closest quintile, mothers in Q3 were 8 percentage points less likely to attend at least one prenatal care appointment in a hospital or health centre, a relative difference of about 9%. This gap increased to 27 percentage points for mothers in Q5, a relative difference of 30%. Mothers in Q3 had about 0.6 fewer prenatal care appointments than mothers in Q1; in Q5, the gap increased to 1.5 appointments. The remaining prenatal care outcomes followed the same trend: utilisation and early initiation of prenatal care decreased with every further distance quintile.
Gradients in obstetric care by distance (OLS regression)
Among outcomes related to delivery and the postpartum period, there were strong differences between mothers in Q4 and Q5 with respect to mothers in Q1. Mothers in Q4, for example, were almost 15 percentage points less likely to have an institutional delivery compared with mothers in Q1, a relative difference of 24%. The difference increased to 34% in Q5. The difference in postnatal care between mothers in Q4 and Q5 compared with mothers in Q1 was 19 and 25 percentage points, respectively. A similar trend existed among mothers who attended a neonatal exam. We did not find strong evidence for an effect of distance on final health outcomes, though there is a strong relationship between the likelihood of a child being weighed and distance.
Discussion
The utilisation of care before, during and after childbirth is one of the most effective ways to prevent maternal and infant mortalities.1 21 However, widespread inequities in access to obstetric care in Latin America remain a major challenge to improving maternal and child health in the region.1 Indigenous and Afro-descendent populations and women in low-income and rural areas are particularly vulnerable.1 3
This paper builds on a large body of literature surrounding the effect of distance on health outcomes. Numerous studies in developing countries have shown that distance is inversely associated with utilisation of health services.6–12 In this paper, we assessed the relationship between distance to an assigned health clinic and the utilisation of obstetric care services among indigenous women in Ngäbe Buglé, the largest indigenous territory in Panama.
We found significant differences in the utilisation of obstetric care between mothers in the closest 20% of households (Q1) and mothers in the furthest 20% of households (Q5). More specifically, mothers in Q5 had fewer total appointments, initiated prenatal care later in pregnancy and were less likely to go to a hospital or health centre than mothers in Q1. They were also less likely to have an institutional delivery or to attend a postnatal care appointment. In addition to large differences between the top and bottom distance quintiles, we also found a strong gradient in obstetric care by distance. Utilisation of prenatal care and early initiation of care declined with every additional distance-quintile further away from a health centre, even when controlling for household wealth, maternal age, maternal education, number of pregnancies and empowerment. These findings are consistent with other studies that have found an association between distance and utilisation of health services and suggest that expanding access to healthcare in remote and under-served areas through supply or demand side interventions could be a valuable strategy to improving maternal and child health outcomes in developing countries.
We also found that the disparities in utilisation of services across distance quintiles were much more pronounced for women who are less wealthy and less educated. In fact, for women in Q1, wealth had little effect on utilisation, but for women in Q5, low wealth was a major deterrent to utilisation of obstetric care. This could be because travelling to a health centre from a farther distance requires a higher economic cost. For women in Q1, for example, the cost of transportation and the time spent to get to an appointment an average of 4.5 km away is substantially lower than for women in Q5, who had to travel an average of 50 km. In this sense, women who are poor and less educated suffered the most from being far from health facilities. The upfront costs required to get to appointments may be a significant barrier to accessing necessary care. In fact, the two most frequently reported reasons given for not accessing prenatal care were lack of money (41.4%) and health services being too far (67.1%).
To address the disparities in obstetric care utilisation for populations that are far from established health services, policymakers may consider supply and demand side interventions. Supply side alternatives such as the expansion of facility-based health centres or mobile clinics may be cost-effective solutions for more densely populated areas. However, in the context of Ngäbe Buglé, providing universal access to formal health services within a distance of 4.5 km (the average of Q1 in our sample) is unlikely to be cost-effective or feasible, as it would require large infrastructure investments and staffing of health personnel to serve a limited number of households in remote and highly dispersed rural areas. In these contexts, demand-side interventions such as conditional cash transfers or transportation vouchers could be alternative policy options to boost obstetric care utilisation. Conditional cash transfers, which condition monetary payments on health service utilisation, have been shown to effectively increase the utilisation of health services, including in rural and indigenous contexts.22–25 Transfer amounts could be set in relation to distance, with higher amounts in more distant communities to compensate for the opportunity cost of time and higher transportation costs. Further research to be conducted through a prospective randomised trial is required to measure the effectiveness of conditional cash transfers on obstetric care utilisation in the context of Ngäbe Buglé.
Study strengths and limitations
A major advantage of our study is our novel approach to calculating distances. While most studies use linear distances, which are unable to account for physical barriers and often underestimate the true distance, our study utilised the Dijkstra algorithm to approximate the distance of viable routes. In QGIS, we determined the shortest route from every household to its assigned health clinic—using a network of roads, rivers, canals and other polylines—and measured the associated distance. Compared with linear paths, this measure of distance is likely to be more accurate, especially in an extremely mountainous and remote area, where there are many physical barriers and limited infrastructure. Another advantage of this paper is our sample population. Our data includes utilisation and health outcome measures for a representative sample of 1336 indigenous mothers. While health disparities research is growing, there are still gaps in data collection and analysis of the health status of indigenous populations. Given indigenous people make up around 8% of the population in the region—45 million people in total—and often have much worse health outcomes compared with non-indigenous people, they are an important population to consider when making policy and programme decisions.26
A limitation of this study is that our analysis considers only distances between the household and its assigned health centre, while existing evidence suggests that women may travel to more distant facilities if they are perceived to be of higher quality.27 However, since the assigned health centre in Ngäbe Buglé is also the closest available health service, our ranking of households by distance quintile is likely to preserve the relative ordering of distance even if more distant facilities were also included in the analysis. Additionally, while we use a sophisticated method for calculating distances, there are possible inaccuracies. The study area is extremely remote, and the road network is sparse, so it is possible that some of the routes taken by families are not included in Open Street Maps. Another limitation is that outcome measures are based on self-reporting, which may introduce some measurement error relative to medical records. However, only mothers who gave birth within the last 12 months are included in the sample to help minimise recall bias.
Conclusions
This paper highlights the important relationship between distance to a health facility and the utilisation of obstetric care among indigenous women in Panama. The results presented in this paper provide evidence on a key barrier to health seeking behaviour and will inform the design of programme that may help reduce these barriers, including cash transfers, vouchers and the expansion of health infrastructure, among others. Rigorous testing of these interventions will be required to determine the most cost-effective types of interventions for reducing barriers related to distance, and, ultimately, improving maternal and child health outcomes.
Acknowledgments
We are grateful to the Ministry of Health in Panama, in particular to Dr. Tania Chung, for granting access to the baseline survey of PN-L1068 used for this study. We thank the staff at ECONSUL Consulting group, Carlos Alviar, Mario Navarrete and Fernando Ferreira for their work on the collection of the survey. All opinions in this paper are those of the authors and do not necessarily represent the views of the Government of Panama or the Inter-American Development Bank, their Executive Directors or the governments they represent.
Footnotes
Contributors Conceived and designed the study: PA, SM, LP. Wrote the paper: PA, SM and SW. Discussed, critically revised and approved the study protocol: PA, SM, LP. Responsible for the organisation and conduct of the study: SM, LP, ES-M. Supervised the study: PA, SM. Responsible for the statistical analysis: PA, SW, SM. Contributed to data analysis: SW. Drafted the first version of the report: SM, SW. Elaborated, discussed and approved the final version of the paper for publication: PA, SM, LP, ES-M and SW.
Funding The survey used in this study was financed by the Ministry of Health in Panama with support from the Inter-American Development Bank projects PN-L1068 and PN-L1115. All authors were IDB staff at the time of the study’s conception and implementation. The opinions in this paper are those of the authors and do not necessarily represent the views of the Ministry of Health of Panama, of the Government of Panama, or of the Inter-American Development Bank, its Executive Directors, or the governments they represent.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study analysed primary survey data collected as part of the evaluation of the Program for Community Support in Panama. The study, including the baseline survey, was approved by the National Committee of Research Bio-Ethics of Panama (IRB approval number EC-CNBI-2016-05-24) and was registered in the AEA RCT Registry (RCT ID AEARCTR-0001751). All subjects provided informed consent prior to the interview, and data were de-identified of personally identifiable information prior to analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All non-identifiable data will be made available through the Inter-American Development Bank’s publications website following publication of the randomised trials associated with the baseline data used for these analyses.