Article Text

Abstract
Objectives To examine and synthesise current evidence on the factors that affect recruitment, retention, participation and progression within the clinical academic pathway, focusing on equitable participation across protected characteristics including gender, ethnicity and sexual orientation.
Design Scoping review and meta-thematic synthesis.
Data sources Web of Science, Google Scholar.
Article selection We conducted a scoping review of English language articles on factors affecting recruitment, retention, progression and equitable participation in clinical academic careers published in North America, Australasia and Western Europe between January 2005 and April 2019. The most recent and relevant 39 articles were selected for meta-thematic synthesis using detailed inclusion/exclusion criteria.
Data extraction The articles were purposively sampled to cover protected characteristics and career stages and coded for factors related to equitable participation. 17 articles were fully coded. No new themes arose after nine papers. Themes and higher level categories were derived through an iterative consensual process.
Results 13 discrete themes of factors impacting on equitable participation were identified including societal attitudes and expectations; national and organisational policies, priorities and resourcing; academic and clinical workplace cultures; supportive, discriminatory and compensatory interpersonal behaviours and personal factors related to social capital, finances, competing priorities, confidence and ambition, and orientation to clinical, academic and leadership roles.
Conclusions The broad and often interconnected nature of these factors suggests that interventions will need to address structural and cultural factors as well as individual needs. In addition to standard good practice on equality and diversity, we suggest that organisations provide equitable support towards early publication success and targeted mentoring; address financial and role insecurity; address the clinical workplace culture; mitigate clinical–academic–personal role conflicts and overload; ensure that promotional structures and processes encourage diverse applicants and promote family-friendly, coherent and transparent national career pathways.
- medical education & training
- qualitative research
- health policy
- organisational development
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our review consolidates the full continuum of factors affecting equitable participation in clinical academia at all stages of the pipeline and across a range of protected characteristics.
Our findings will have limited relevance to nursing, midwifery, allied health professions or other geographies where there may be divergent issues in relation to gender, sexuality and ethnicity or the nature of clinical academia.
The majority of papers identified in the scoping review focused on gender, therefore the factors identified within each theme may not fully represent issues related to ethnicity and sexual orientation. No studies related to disability were identified.
Policy is in constant transition and it will need to be studied and addressed locally. This paper focused on current UK policy as an illustrative case.
Background
Clinical academics, also referred to as physician researchers, physician scientists or academic physicians, combine clinical practice with academic research and teaching. Their clinical practice informs their academic practice and vice versa, creating a synergy: their expertise in both areas drives innovation and supports the translation of research into clinical practice1 2; conversely, their clinical expertise guides their research.3 This breadth of skills is also important in training the next generation of medical professionals.4 The declining number of clinical academics, which has been observed internationally,5 6 is therefore concerning.
Issues with recruitment and retention within clinical academia affect certain demographic groups disproportionately. For example in the UK, women have outnumbered men entering medical school since 19967; however in 2017, the ratio of male to female clinical academics stood at 69% to 31% with the gender disparity even greater at professorial level.8 Several studies have demonstrated that women and minority ethnic clinical academics are also under-represented at senior levels in North America, Australasia and across Western Europe.9–11 Concerningly, there is evidence that representation of ethnic minorities actually declined in the USA between 1990 and 2016.12
A diverse clinical academic workforce is not only important from a values perspective, but it also drives innovation and excellence in research and teaching,13 14 for example training doctors to practice in culturally diverse environments,13 or research in health issues specific to under-represented communities.2 15 From an economic perspective, the attrition of a highly trained elite workforce due to potentially remediable factors warrants attention and investment.
The failure to achieve equitable participation in the clinical academic workforce has been discussed extensively in the literature for decades, however much of the empirical research is observational rather than explanatory, for example measuring promotion rates rather than exploring the underlying reasons for under-representation. There is also a body of literature that evaluates interventional programmes such as mentoring programmes or the Higher Education Equality Charters in the UK, including a recent review of interventions.11 There is a gap in the literature for a review of explanatory factors.
Review objectives
Past research in the area has often focused on a particular stage of career development,16 17 a particular population4 18 or a particular factor that affects equitable participation.19–21 Our aim is to examine this body of literature as a whole and to synthesise the full continuum of factors affecting equitable participation, retention and success in clinical academia at all stages of the pipeline. In doing so, we hope to inform researchers and policymakers on the range of factors that need to be considered, as well as supporting conversations about how some of these factors might be interlinked. We have not researched interventions or synthesised evidence on the relative importance of factors as we take the view that this type of knowledge is likely to be highly context-dependent and needs to be researched and addressed locally.
Methodology
Thematic analysis is an established method for meta-synthesis of exploratory rather than interventional research findings, bringing together and integrating findings of multiple studies.22 We used Thomas and Harden’s three-step framework for thematic synthesis.22
Phase 1 (long list and short list of papers, demonstration of saturation).
Phase 2 (coding tree, and descriptive analysis of main themes, quotes).
Phase 3 (interpretative analysis tested against the underlying data).
Phase 1 began with a scoping review to determine the extent, range and nature of research in this area. Phase 2 involved a qualitative meta-thematic synthesis drawing together all the factors that these papers had identified. In phase 3, the resulting framework was used to create an integrated description and explanation of the subject under review.
The methodology of scoping reviews has an evolving literature base,23 with many definitions, some involving more evidence synthesis than others. Our methods were guided by our purpose, which was to rapidly and systematically map the key areas of research and the main types and sources of evidence available, so that we could identify appropriate papers for meta-thematic synthesis.
Munn et al stated that when a study is ‘interested in the identification of certain characteristics/concepts in papers or studies, and in the mapping, reporting or discussion of these characteristics/concepts’ a scoping review is the appropriate choice of methodology,24 and hence it was suited to our research.
Inclusion criteria
Our inclusion criteria are listed and justified in table 1.
Inclusion criteria and justification
Search strategy
We used a PICo ‘population, phenomenon of interest, context’ strategy25 to develop our question and search terms (listed in table 2) which is appropriate for exploratory rather than interventional reviews. The terms were derived from an analysis of commonly used words in the titles of papers related to equitable participation in clinical academic careers, iteratively expanded and systematically reapplied as the range of terms related to our subject of interest became apparent. We included a range of terms related to protected characteristics including gender, race, disability and sexual orientation. Social class was not included as the population is by definition classed within higher professional occupations.
Search terms
The literature in this area does not have a defined MESH term, topic category or keyword and there are many terms to describe clinical academia, including specialty specific terms such as academic diabetology. We therefore began with a search on Web of Science combining terms related to clinical academia, participation and equity (see terms in table 2). We systematically expanded this search using a forward snowballing approach26 using Google Scholar, to include relevant papers that had cited the 12 most commonly cited papers both in our original list and then again on the expanded list. This snowballing approach allowed us to identify literature that did not use standard terminology in the title or abstract and has been shown to be superior to searches based on fixed search terms if seeded from suitably influential and relevant papers.27 Web of Science was chosen and not expanded by Scopus as both have 100% coverage of PubMed which includes the core reputable journals relevant to clinical academia. Google Scholar was chosen for the snowballing step as it has superior citation coverage to both Web of Science and Scopus.28
Our criteria were ordered so that the more labour-intensive items were applied towards the end. As we were planning a meta-thematic synthesis, coding articles until thematic saturation had been achieved, we began by reapplying our criteria to the most recent 5 years of full-text articles. Having identified a manageable number of potential papers, our thematic synthesis began by purposively sampling these papers to ensure that we had covered the spectrum of gender, ethnicity and sexuality, and the pipeline from entry to training posts, completion of PhD, post-doctoral engagement and career progression to professorship.
Critical appraisal of research quality
In evidence synthesis through qualitative approaches, findings are not statistically weighted according to strength of evidence. The aim is to develop robust categories of research findings that fit across the full range of the relevant literature. Our appraisal of research quality was therefore not as detailed as for an appraisal of evidence to support an intervention. A single researcher (KL-G), who is an experienced reviewer, appraised the quality of each paper, informed by the relevant CASP checklist, across five grades (poor, moderate to poor, moderate, moderate to good or good). Methodologically poor papers were excluded, and moderate to poor papers were included with provisos detailed in table 3.
Methodological quality
Textual data extraction
We used a consensual qualitative research approach29 involving two independent coders, (CV) and (KL-G), and an auditor (SS). We uploaded the selected papers to analytical software (NVivo V.12, QSR International) purposively sampling papers that were potentially rich in factors and with diverse perspectives on the topic. (CV) and (KL-G) coded each paper’s research findings into core ideas (content coding), each representing a discrete factor impacting on equitable participation. Each coder cross-checked the other’s coding.
Textual data synthesis
Content codes were arranged into higher level themes through an inductive consensual process, involving team discussions and iteratively testing the thematic structure against new papers. Saturation of themes was demonstrated when no new themes had emerged for five consecutively coded papers. Our content coding, thematic structure and data saturation were audited by (SS) who had not been involved in the coding process. The structure was tested by (SS) against two further articles from our sample which were selected to challenge our framework by looking at different under-represented groups, different geographies and stages in the pipeline. Finally, these themes were categorised according to personal, interpersonal, organisational and societal factors, reflecting the multiple layers of influence on the career development of clinical academics.
Patient and public involvement
Patients were not involved in the design, planning and conception of this study.
Results
We applied our search terms tightly (population AND phenomena of interest AND context in the title) to identify 73 papers that we were confidently had relevance to this area of research. The two-step forward snowballing process on Google Scholar generated 625 papers. Titles were screened according to our inclusion criteria, leaving 258 potential papers for inclusion since 2005. Note that the date range for the scoping review (2005–2019) was broader than the range considered for meta-thematic synthesis (2014–2019) where only the most recent 5 years were included. The initially wide time frame supported the identification of highly cited papers on this topic, which is necessary for effective forward snowballing (identification of related papers through citation indexes). The subsequent contraction to the most recent 5 years was a pragmatic way of reducing the large number of papers identified to a manageable number for full-text review and potential inclusion in the meta-thematic synthesis. As such, only full-text papers from the most recent 5 years were uploaded onto NVivo, which reduced the number or potential papers for inclusion to 72. Our criteria were reapplied to the full-text papers, reducing this number to 39. Our search results are summarised in figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Methodological quality
Our critical appraisal of papers included in the meta-thematic synthesis is presented in table 3.
Findings of the review
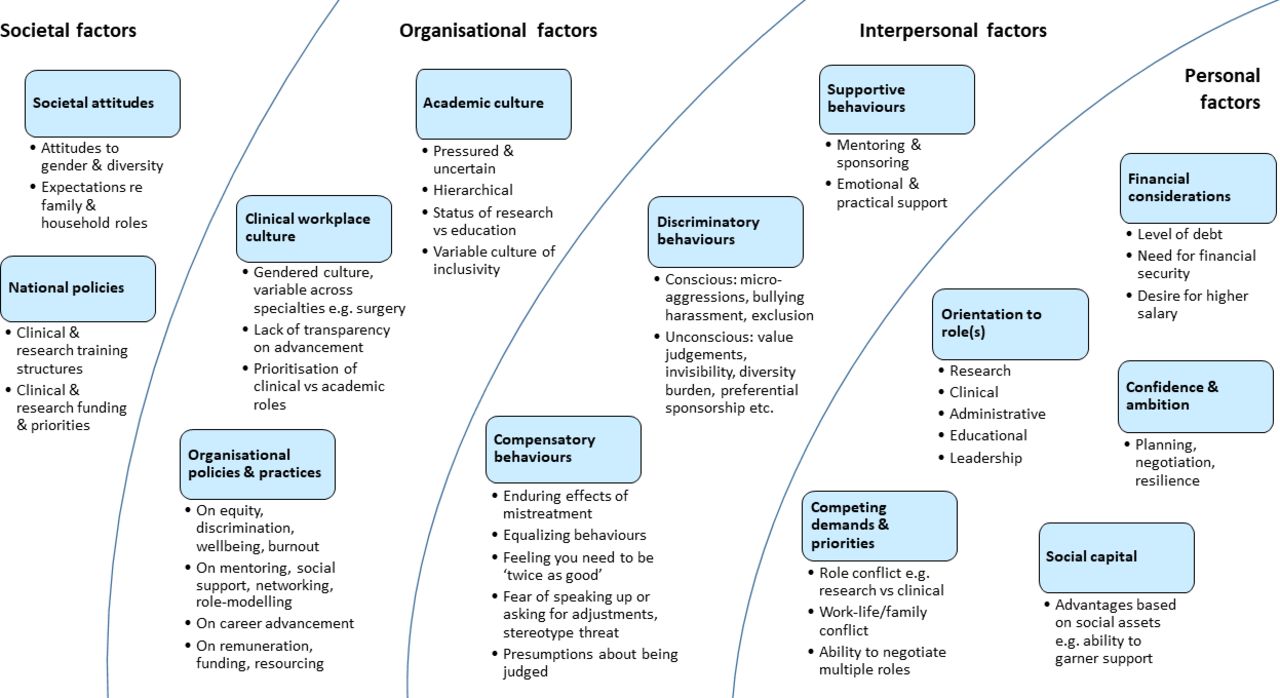
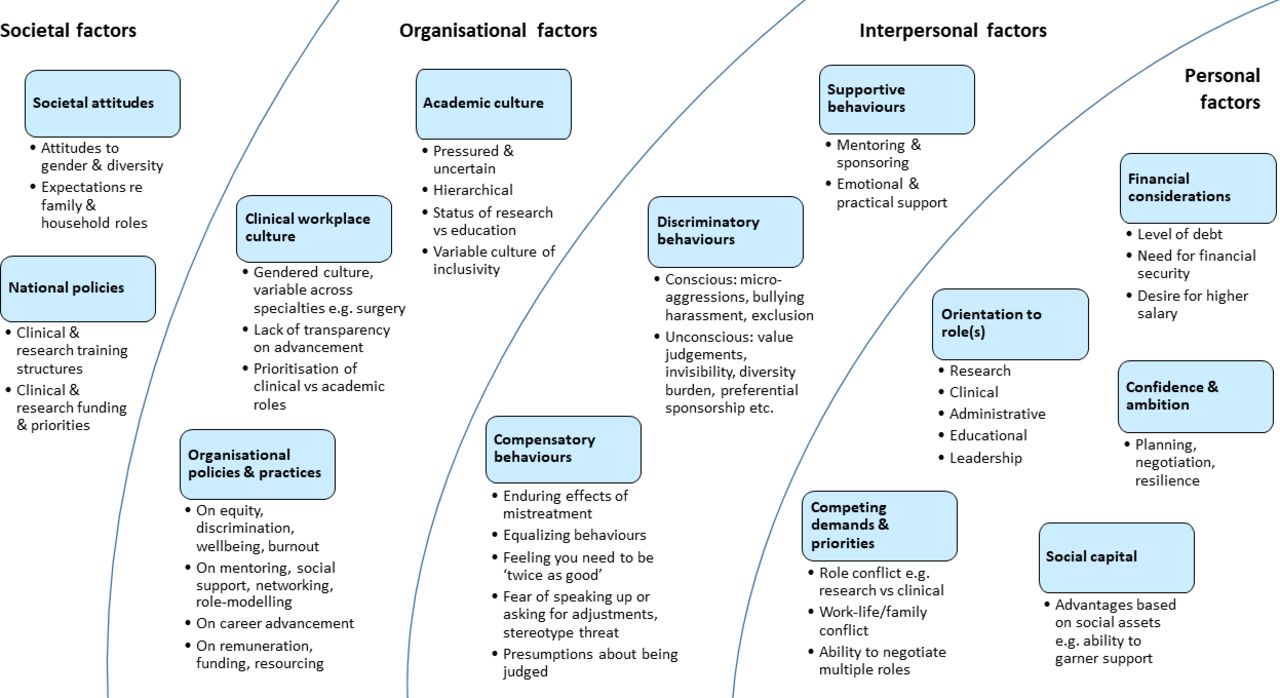
We identified 13 themes (figure 2), which we organised into personal, interpersonal, organisation and societal categories using a socioecological approach.30 The structure aimed to illustrate the dynamic inter-relations between personal attributes and multiple levels of contextual factors.
{kind=link}
{kind=link}
Factors related to retention, success and equitable participation in clinical academia.
Personal factors
Social capital
Advancement in clinical academia was described as inherently competitive,31 favouring participants with higher social capital who are more likely to be included within formal and informal academic networking,32–34 to garner support32 and to be aware of the mechanisms of advancement.35 Social capital was seen as related to tangible social assets such as gender and race which intersect to create multiple levels of disadvantage.32
Professional advancement, including promotion seeking, is tied to having informal networks and supports and to garnering sponsorship—someone in a position of power to advocate for one’s career advancement—and men are more likely to have more of these resources than are women.32
Confidence and ambition
Confidence and ambition were described as driving career advancement, favouring those (usually men) who strategically plan towards promotion,34 36 self-promote,37 38 negotiate their position35 or thrive on the politics of advancement.34 Resilience and the ability to grow through difficulties also support advancement.37 38 Conversely, ambition deters some senior clinicians from starting as junior researchers.38
… significantly more women (p=0.032) expressed the concern or frustration that they needed to self-promote or else were simply forgotten by their leaders.37
Competing demands and priorities
Competing demands and priorities included role conflict between competing clinical and research commitments; work–life conflict and family–work conflict. These were mitigated by an ability to negotiate multiple roles. Women were more likely to be affected by family–work conflict related to sociocultural expectations to prioritise family,39 the likelihood of having a partner with an equally demanding career36 37 39 and having to accommodate family geographical needs including their partner’s career decisions.32 36 40 A lack of control over career moves due to family commitments was felt to impact on women’s promotion and salary negotiations.36 They were discouraged by a lack of female role models with both a family and a successful clinical academic career.31 32 34 39
Family–work conflict was compounded by multiple barriers to returning to work including a lack of part-time posts with flexible working or support/incentives for returners,31 39 and difficulties in moving flexibly between research and teaching (in both directions).39 Clinical academia was perceived by many as a barrier to raising a family.31 32 34 35 39 41 Research training often coincided with child-rearing years leaving those who had taken a career break behind their peers on research outputs and career progression.35 39 41
There was a tendency to expect full-time outputs from part-time workers,35 and a tendency to stigmatise part-time workers as disinterested or under-committed.35
I think working part-time is a thing that hampers progression in your career, in general… Apparently people think: ‘OK, part-time means no ambition.’ Which is not true.35
Financial considerations
Financial considerations were a concern, exacerbated by levels of student debt31 39 42 and the concentration of research institutions into areas of high living cost.38 The cost of starting a family and lack of access to affordable childcare made this more acute for those with parenting responsibilities.35 38
In fact, working part-time is an alternative strategy to manage child care duties, sometimes chosen to avoid spending most of one’s salary on expensive services.35
There were pay inequalities between clinical and research pathways, leaving some clinicians with research ambitions taking pay cuts for funded doctoral studentships or even self-funding, affecting those with either a desire for higher pay or a need for financial stability.31 32 34 38 39 41
For both genders, debt was associated with the consideration of students leaving…39
Orientation to roles
Orientation towards administrative role
A dislike for administration was linked to burnout and avoidance of leadership responsibilities.37 38 Conversely an interest in the organisational aspects of research and education was linked to interest in academic medicine as a career.34
Orientation towards clinical care
A return to full-time clinical care was driven by wanting more patient contact, feeling deskilled by time away from patient care and a delay in reaching consultant status due to academic time commitment.37 38
Retention was supported by feeling that research made them a better clinician, either through alignment of their research to clinical needs or because their academic activities provided respite from full-time clinical care.37 38
Orientation to leadership
There were many personal factors contributing to a rejection of leadership roles by women. These included distancing from androcentric conceptions of leadership as related to power and conflict and seeing leadership as a distraction from clinical or research work or as unviable due to a lack of recognition of women, work overload and a perceived need to self-promote.32 37 A leadership culture of long hours and out-of-hours networking excluded many with parenting responsibilities.32 Promotion was seen as linked to grant funding and publication frequency, favouring those engaged in research rather than education,34 not only excluding some women but not producing the most competent leaders.43
The deans recommended re-evaluating traditional views of leader qualifications because the current standards do not necessarily parse out strong leaders and are more likely to exclude women candidates.43
There was a tendency for women to wait until they were overqualified for promotion, while men applied without meeting all the criteria.37 This was partly attributed to women feeling unready and partly to compensatory behaviours in response to discouragement.37 Some men also rejected leadership roles, which were described as not worth the time or stress.37
According to my mentors (usually chairs), before going up for promotion I always need one more thing even though there are many criteria for promotion, of which I have more than fulfilled. I have observed that this is not the case for several of my colleagues who are male.37
Women and other minority clinical academics were attracted to leadership roles as a way of influencing research agendas, of resolving conflict and of promoting diversity by becoming a visible role model.33 43
Orientation to research and academia
Orientation to research was supported by undergraduate research experiences, early training in research methods and training in a research-intensive university or hospital.33 39 40 42 Clinicians from diverse backgrounds were sometimes attracted to research by its relevance to women’s health, Lesbian Gay Bisexual Trans(gender) and related communities (LGBT+) health or underserved community needs.31 37 41
Early publication success was an important driving factor,37 39 42 favouring those who were more likely to benefit from mentoring, sponsorship and academic support.33 34 The benefits of academia were described as outweighing the difficulties: more interesting and less stressful than clinical service provision,38 offering academic freedom31 and a clearly structured career path,31 37 40 41 although not all were aware that the pathway existed.40 Attrition was driven by feeling unable to ‘switch-off’ from one’s academic role due to pressures to publish or apply for funding38 and by competing demands and priorities including clinical and personal commitments.35 38
Orientation towards education
Women were described as more interested in opportunities to teach than to conduct biomedical research; however gender differences were also linked to education’s flexibility, its historically lower status (deterring some men) and the competitiveness of the research pathway.39 Education encouraged women into academia, some discovering research after having begun as an educator.39
In two qualitative studies, female physicians (53 from the USA, seven from elsewhere) reflecting on their career choices reported that they were attracted to academic medicine by opportunities to teach, but with experience they also came to appreciate research more.39
An interest in education was partly driven by opportunity and experience and also by values: wanting to facilitate success in others, wanting to make a difference or stay up-to-date, wanting to build a diverse workforce or enact social change through teaching, attracting participants from diverse backgrounds.34 39
as a mentor, you can reach out to thousands of people who can … impact change (African–American male, medical student).34
Attrition from educational activities was driven by limited scope for progression, as well as competing clinical and personal demands and priorities.39
Interpersonal (behavioural) factors
Supportive behaviours
Supportive behaviours included mentorship, involving regular support designed to build self-efficacy through advice or coaching. This was contrasted to sponsorship, or the preferential treatment of a protégé.
There was concern that sponsorship tended to be preferentially available to those with characteristics that reflected incumbent clinical academics, disadvantaging minorities and women.32 37 Sponsorship included advocacy for advancement32 34 37 and preferential support for early publication.37
Mentoring on the other hand tended to be formalised and more equitably available.36 40 44 Supportive mentoring behaviours included altruistic guidance and clarity, building self-efficacy, encouraging continuity and supporting resilience in the face of difficulty, encouraging successful publication, guiding and critiquing academic work, supporting career planning and providing moral and institutional guidance.31 34 41 43
Discriminatory behaviours
Conscious discrimination was expressed as overt disrespect,35 38 39 disruptive behaviours,36 45 micro-aggressions,35 39 sexual harassment,35 36 39 social31 35 39 43 or cultural exclusion35 39 and deliberate sponsorship or preferential treatment of people of a chosen characteristic.35 36 38 43
… a senior colleague of clearly homosexual orientation. Despite being very prepared, he was marginalized by the group leader… He was placed in the ward, kept out of any possibility to publish and teach.35
Unconscious discriminatory behaviours, sometimes by women themselves, included judgemental attitudes towards women exhibiting ‘male’ characteristics such as ambition, aggression or assertiveness,39 simply being treated differently to colleagues,31 35 38 39 unconscious value judgements leading to academic invisibility or assumptions about status or role.35 36 39 43
When you have an outpatient clinic, you might be asked to go and fetch your own patients whereas the nurse might do that for the male intern, or you have to change your own paper on the examination bench … Just little things like that.35
The exclusion of women can be done in so many ways. It has been all the time actually. Also in meetings. [When you talk] they start to play with the phone or whatever… We had a meeting with the boss and I talked with him for 30 s; and then he said: ‘She is giving a monologue.’… Yes, subtle means.35
Indirect discrimination sometimes manifested as a diversity burden, where minority academics were disproportionately required to sit on selection panels, provide mentoring or to appear in public, detracting from their clinical research activities.43 44
diversity exhaustion for our [minority] faculty members … when people are asked to do so much to help recruit, retain, promote, support, mentor other people who look like themselves.44
Compensatory behaviours
Compensatory behaviours by those affected by discrimination included equalising behaviours, such as submissive or self-deprecating talk39; a fear of being seen to conform stereotype32; fear of speaking up or asking for adjustments31 35 and feeling that they needed to be twice as good to advance.35 39
Compensatory behaviours manifested even without active discriminatory behaviour due to the enduring effects of prior mistreatment.31 35 39
But in time, I learned to be silent, not to talk about it. Although I faced the problems, I did not mention anything about them. Because if I talk about the problems, they dislike me more.35
Organisational factors
Academic culture
In comparison with the clinical workplace, the academic workplace culture was described as respectful and inclusive31 34 36 43–46; however some found it competitive and unwelcoming.31 The broad spectrum of academic roles and responsibilities (teaching, research, mentoring, administration and leadership) was seen as attractive.34
Academia was frequently described as pressured and uncertain: pressure to apply for research grants, to publish regularly, with anxieties caused by fixed term or temporary research contracts, and an out-of-hours culture which effectively excludes those with parental responsibilities.35 38 43 46 The academic structure was described as hierarchical with limited prospects at senior levels, driving both excellence and exclusion.37
There was a perception of underappreciation of women’s contributions and criticism that promotion processes favoured self-promoters.37 Promotion criteria attributed low worth to teaching,31 disproportionately affecting women who are over-represented in education.39 Research into inclusivity was also seen as lower status disproportionately affecting minority researchers.33 39
Junior faculty valued institutions that were committed to their career development. They were discouraged by institutional failure to formally recognise their dedication to teaching and ambiguity regarding their pathway to promotion.31
Clinical workplace culture
The clinical workplace culture was described as pressuring clinicians to prioritise service provision over teaching or research.31 35 37 The gender culture in teaching hospitals varied across specialties and institutions and one study found it positive in a narrow range of specialties including neurology, pathology, internal medicine and paediatrics42; it was however perceived as negative in the majority of specialties including surgery.35 38 42 Where the clinical promotion pathway lacked transparency, there were also concerns about nepotism.35
All surgeons look at you… ‘Well, you are a woman, you will never be a good surgeon.’ … When I was a student, there were not a lot of female students specializing in surgical specialties. They stopped sometimes their education to become general practitioners.35
White male: [When I was in the other hospital] there was the head of internal medicine trumpeting the fact that he never wanted to have a woman in his ward. Firstly, because they get on his nerves; secondly, because he said that every time you have to discuss with them, they begin to cry and to view any remark as offending them personally; thirdly, because women become pregnant. Partially I found this attitude here too [in the hospital where I am presently working].35
Organisational policies and practices
On equity and discrimination, well-being and burnout
The authenticity of leadership’s commitment to diversity was seen as crucial, helped by the involvement of a diversity council or diversity champion with both resources and power.44 Rhetoric was converted to action through active monitoring, investment in unconscious bias training and zero tolerance on discrimination.39 44 45 A lack of critical mass of academics from diverse backgrounds discouraged new applicants.36 44 Some characteristics such as gender or race were felt to be more protected than others such as sexuality.33
They’re very good with cultural diversity training, but when it comes to LGBT concerns it’s kind of like they don’t talk about it. It’s like a brick wall.33
Essential family-friendly policies included the availability of flexible working31 32 35–38 40 43 45 or maternity/carer pay.35 36 41 Successful programmes enhanced this by actively addressing the out-of-hours culture bringing meetings and communication into working hours,38 40 and creating a culture of flexible working for all31 35 which some extended beyond childcare to cover, for example, unexpected personal or family crises.45
Regardless of gender, faculty expressing [Role Overload] frequently worked part time (p=0.001) and had a spouse working outside the home (93%, p=0.043).37
Hiring and promotion practices such as diverse representation on selection panels were helpful,43 44 as long as they did not overly burden diverse individuals.44 Some promotion criteria were seen as actively disadvantaging women, such as a requirement to travel or the status of education compared with research.36 39 40 43
On mentoring, social support, networking, role modelling
The visibility of concordant role models was seen as important.31 34 35 37 39 40 43 Women wanted role models who were based on more than gender, such as modelling a work–life balance or balancing a successful career with family.31 32 34–36 39
I am shocked when I look around. Even if I think that things are going well, that people are not discriminated. … When you look around, there are always more men than women in leadership positions.35
Networking opportunities needed to feel inclusive, with sensitivity to culture and parental commitments.33
The availability of concordant mentoring was seen as important33 34 36 39 40 44 but not always achievable. Cross-gender mentoring was successful where there was an understanding of the unique challenges faced by women.32 Formal mentorship programmes to support the advancement of under-represented groups were described.36 40 44 There may be issues with women prioritising lower status but supportive mentors and men benefiting from mentors with higher status,39 and poor quality or inconsistently available mentoring.37 41
On active support for career advancement
Some institutions described active support for career planning aimed at promoting talent over ambition.31 32 34 37 38 40 Other measures included career pathways that include education,31 37 38 faculty development programmes,45 performance recognition schemes,44 leadership training37 for women,34 training career counsellors on the issues facing women in clinical academia34 and steps to increase the transparency of promotional pathways, policies and procedures.31 38 45
These gendered patterns of family–work dynamics, coupled with the association between organizational support and intent to leave, point to the organization’s responsibility and accountability in establishing practices that can facilitate embeddedness or a reason to stay, such as a positive promotion climate. It is worth noting that opportunities for advancement are necessary, but not sufficient to increase retention for all faculty members, as promotion climate was not a positive reason to stay for female respondents.32
On remuneration, funding and resources
The allocation of funding and resources also impacted on retention and success. Return to full-time clinical practice was driven by academic versus clinical salary discrepancies31 39 and the availability of funding, credit or loan repayment schemes39; see also the prior section on personal financial considerations. Clinicians needed protected research time and resources to backfill their clinical duties.31 36 46
There was a tendency for women to apply for funded PhDs which are a scarce resource and competitively allocated.39 The allocation of research funding was also felt to be overly competitive31 and gendered,42 as was the allocation of research space and administrative support.35 46 A gender and ethnicity-based pay gap was reported.35 36
In my clinic there are two men and they have two separate rooms, the other four female doctors are in one room. So, males have more opportunities than me [to do research].35
The ongoing pay gap (both for women and for expatriates) is exacerbated by salary negotiations which tend to favour local male professionals, as they are often more assertive.35
External (societal) factors
National clinical academic structures and funding
The availability of national and international research funding is affected by economic and political factors.31 Funding of higher education impacts on the number of senior academic positions and the availability of post-doctoral positions.38 40
National structures need to be studied locally as they are by definition situated in their time and context. We focus here on the current UK training pathway as a case example. National structures in the UK have led to discrepancies in research funding depending on whether the applicant is a trainee or consultant, which contributes to a disconnect at that transition,38 alongside structures preventing consultants from applying for clinical lectureships.40 There are calls for jointly funded positions to address this issue.40 There was a concern that the new trainee doctor contract with longer core hours will reduce research capacity, particularly for parents with care-giving responsibilities.38 The visibility of national research training opportunities to clinicians was an issue, particularly for those who were not on an integrated run-through pathway.38 41
Many participants … voiced their fears that the new junior doctor contract in the United Kingdom may financially penalize both female clinicians and those interested in pursuing an academic career, due to potential increases in working hours accompanied by a reduction in out-of-hours pay.38
… participants noted difficulty accessing information and guidance on training pathways and uncertainty about how to progress in a clinical academic career, particularly if they were ineligible for the integrated academic training pathway.38
Respondents [planning to leave clinical academia] … are particularly worried about the small number of senior academic appointments available as well as the difficulty of obtaining research grants and work–life balance.40
Societal attitudes to diversity and equity
Societal factors related to gender and diversity also impact on equitable participation in this demanding career.35 36 39 There are ongoing expectations for women to shoulder household chores and to be the primary caregiver, effectively doing a second shift after work. This may be giving way to an increasing acceptance of non-gendered household roles. Fewer people of either gender have a stay-at-home partner.35
We suggest that such a pattern reflects a general gender norm within society whereby women are more likely to hinder their careers because of family responsibilities and ‘second shifts’ than are men.36
It seems that younger couples try to share much more equally. I don’t know if that’s true for every aspect of life. But also many of my male colleagues leave early one or two days a week to go pick up the kids at the day care centre.35
Discussion
The objective of this review was to scope and synthesise current evidence on the factors affecting recruitment, retention, participation and progression within the clinical academic pathway, with a focus on equitable participation for under-represented groups. These factors, summarised in figure 2, reveal a multidimensional problem with individual, interpersonal and societal–institutional aspects, and nuances at different stages of the career pipeline.
There are calls for interventions to target the organisational level rather than expecting individuals to adapt.47 Organisational changes are also within the control of local leadership and can therefore be more rapidly changed than wider external and societal factors. Interventions at this level will need to address the issues identified at the personal and interpersonal levels, while acknowledging the wider national and societal landscape; for example, addressing the out-of-hours working culture; ensuring that promotion pathways value education and rely less on self-promotion, and providing research support for part-time workers and those with parenting responsibilities to mitigate role overload. Policies to support gender equality may increasingly support both men and women as societal norms shift towards more equal family and household responsibilities.48
Many of these issues relate to work–family conflict or the advantages conferred by social capital, which are well documented and generic to a range of careers.49 50 We will therefore focus our discussion on the aspects that appear unique to clinical academia. Early publication success and research mentoring during medical school and early training were associated with entering the pipeline and opportunities need to be offered equitably, rather than through informal networking which may disadvantage minorities. Financial pressures related to debt accrued during extended medical training and poorly funded PhD programmes need to be addressed. Both deliberate and unconscious discriminatory behaviours were frequently discussed, particularly in the clinical context. This varied by specialty and institution, with discriminatory behaviours appearing to be driven by pressurised and hierarchical clinical workplaces, again suggesting that an organisational approach is needed. Our findings suggest that it may not be enough to address organisational culture on a single side of the research versus clinical divide. Research institute policies on equality, diversity and family-friendly working are unlikely to support this workforce unless they are also adopted and monitored within the clinical setting.
Interventions at the national policy level are needed to address transparency of the pathway, remuneration for doctoral education that reflects the particular needs and contribution of this highly skilled and mature workforce, the availability of post-doctoral posts, and transitions particularly at the trainee/consultant level. These findings reflect and confirm policy recommendations from the UK’s Medical Research Council.51
Past reviews in the area have focused on a particular stage of career decision-making,52 a particular population39 or a particular factor that affects equitable participation.53 Our methodology allowed us to examine and synthesise a broader range of literature. It also facilitated the creation of an integrated analysis of the factors that influence equitable participation in clinical academia at all stages of the pipeline, from recruitment to professorship.
A limitation of our study was the limited literature on equitable participation for ethnic minority and LGBT+ clinicians. Although relatively few papers on sexuality or on ethnicity were included, we found that they sat well within the 13 themes identified, particularly those related to social capital, interest in personally congruent research, interpersonal factors (discriminatory, supportive and compensatory behaviours) and policies and practices within organisations to address the workplace culture (supportive mentoring, networking and training). The infancy of research in this area, compared with gender-based papers, is a limitation of our findings. We did not identify any papers related to disability within the clinical academic career pathway. Class was excluded from this review, as the clinical academic population belongs by definition to the upper professional occupations. However, this does not take account of the socioeconomic background of students at the stage of selection into medical school which is likely to be a significant factor. Further research is needed to explore these gaps.
Conclusions
This review has identified 13 themes of factors impacting on equitable participation in clinical academia. Their broad and often interconnected nature suggests that interventions will need to address structural and cultural factors as well as individual needs. In addition to standard good practice on equality and diversity, we suggest that organisations provide equitable support towards early publication success and targeted mentoring; address financial and role insecurity; address the clinical workplace culture; mitigate clinical–academic–personal role conflicts and overload; ensure that promotional structures and processes encourage diverse applicants and promote family-friendly, coherent and transparent national career pathways.
References
Footnotes
Twitter @doctorkayleigh
Contributors Our team comprised an early career clinical academic (CV), an established educational researcher (KL-G) and a professor of medical education (SS), all experienced qualitative researchers with professional insights into the subject of enquiry. The Faculty of Medicine at Imperial College has a strong research interest in widening participation and its School of Medicine has more graduates entering the clinical academic pathway than any other UK medical school. These factors combined to stimulate our interest in identifying factors surrounding equitable participation in the clinical academic career pathway. All authors were involved in the conception and design of the study and in the acquisition, analysis and interpretation of our findings. CV and KL-G identified and coded the papers. SS audited the process and coding. All authors worked together to generate the themes and categories. CV and KL-G drafted the work, and KL-G created the results section and tables. All authors revised it critically for intellectual content. All authors gave approval to the final version and agree to be accountable for all aspects of the work. All authors undertake to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Research ethics committee approval was not required as this is a review paper.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Coding data are available from the corresponding author upon reasonable request.