Article Text

Abstract
Objectives This study aimed to investigate the obesity prevalence in a population of Brazilian firefighters and the association of central obesity (CO) with sociodemographic, occupational, life habits, fitness and health status variables.
Design Cross-sectional study.
Settings The data were collected during annual health inspections of firefighters from the Military Fire Service of the State of Espírito Santo, a state in Southeast Brazil.
Participants The study encompassed 1018 active military firefighters. After exclusion criteria, 892 male firefighters were analysed.
Primary and secondary outcome measures The collected data included: sociodemographic, occupational, lifestyle, fitness and health status variables. The associations between these factors and CO were calculated by adjusted OR through a hierarchical logistic regression model.
Results Obesity estimation by body mass index indicated that 48.65% of the firefighters were overweight and 10.99% were obese. Concerning the body fat percentage, 26.23% of the participants were considered obese, while 18.61% of the firefighters were considered centrally obese or at risk using the waist circumference measure. After adjusted OR analysis, CO was more likely associated with the age range of 50 to 59 years old (OR 2.93; 95% CI 1.05 to 8.14), low self-reported physical activity (OR 1.95; 95% CI 1.14 to 3.34), low cardiorespiratory fitness (OR 5.15; 95% CI 3.22 to 8.23), hyperglycaemia (OR 1.70; 95% CI 1.07 to 2.72) and hypertriglyceridaemia fasting status (OR 3.12; 95% CI 1.75 to 5.55).
Conclusions Our study identified an overall high prevalence of overweight and obese individuals in the examined firefighter population. Age and cardiovascular risk factors were directly associated with CO among the firefighters. Cardiovascular risk factors should be routinely inspected within the Brazilian firefighters’ corporations in order to improve the health condition and wellness of these workers. These endeavours will improve the performance of the services provided to the population.
- obesity
- firefighters
- sociodemographic
- occupational
- cardiovascular risk
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study is the first to investigate sociodemographic, occupational, life habits, fitness and health status factors associated with central obesity in Brazilian firefighters.
We used a cross-sectional design with statistical analysis that allowed adjustments for calculating OR. This method eliminated the confounding variables and improved our understanding of the factors associated with central obesity in this group of workers.
This study used international guidelines as reference for variables categories. This design will allow for future comparison of the present results with studies in populations with a similar profile.
The studied population corresponded to male workers of the Military Fire Service of one state in Southeast Brazil, and, therefore, does not encompass the totality of Brazilian firefighters.
This study did not have a follow-up period. We intend to perform this examination in the coming years.
Introduction
Obesity has become a pandemic.1 2 In 2016, the WHO estimated that more than 1.9 billion adults were within the overweight and obese range.3 The main cause of overweight and obesity is the imbalance between calorie consumption and expenditure. An increased consumption of energy-rich foods combined with reduced levels of physical activity has been observed all over the world. These phenomena are often associated with environmental and societal changes.3 Brazil is also experiencing an important growth in the obesity scenario, with nearly a 7-fold increase in the obesity prevalence between 1975 and 2016.4
Occupational firefighting activities lead to the development of life habits that are closely related to an important profile of obesity.5 Caban and colleagues evaluated several worker categories within the USA and ranked firefighters among the occupational categories with higher obesity prevalence.6 Firefighting activity is also related to haematological and haemodynamic disturbances that increase the predisposition to sudden cardiac events in susceptible workers.7–10 Therefore, when obesity and other cardiovascular risk factors—developed from living habits or occupational stressors—are combined, the chances of a sudden cardiac event are increased.8 In particular, recent studies have highlighted that obesity measures indicative of visceral adiposity, such as central obesity (CO), have a linear relationship with mortality from cardiovascular disease (CVD).1 11–14 In Brazil, two studies reported a high prevalence of overweight and obesity among firefighters from the Federal District.15 16 However, there is no record of studies that investigated the obesity prevalence among other populations of Brazilian firefighters. Further, given the close relationship between CO and CVD, there are no studies that have investigated the factors associated with CO among the Brazilian firefighters’ occupational group.
The project ‘Bom Estar’ (‘Wellness Project’) is a pioneering endeavour among Brazilian firefighters. It was developed by the Military Fire Service of the State of Espírito Santo17 in 2017; it aims to perform primary prevention of cardiovascular risk factors, including obesity, among this work population. This project annually assesses all active military firefighters. The aim of our study was to investigate the obesity prevalence in a population of Brazilian firefighters and the association of CO with sociodemographic, occupational, life habits, fitness and health status variables.
Methods
Study design
This cross-sectional study utilised secondary data from the ‘Bom Estar’ project of the Military Fire Service of the State of Espírito Santo (CBMES), which analysed 1018 active military firefighters in 2018. The evaluations occurred between February 2018 and April 2018, in the quarters where each military serves. All measures were conducted by trained health professionals, including nurses, pharmacists, social assistants and physical education professionals, all of whom have academic degrees in their areas of expertise. Standard cut-off points were adopted for each variable according to the established international guidelines. Approval from the CBMES was also obtained to gain access to the data. The involved researchers provided assurances of confidentiality by signing a confidentiality term when submitting the project to the Ethics Committee.
Data were extracted from forms completed during the fitness and health status evaluation performed as part of the project. The forms contained four blocks of variables: sociodemographic (age range, family income, education, marital status and access to health insurance coverage), occupational (city of work, type of current activity and main operational function), lifestyle (religious and leisure practice and smoking habits) and results from fitness and health status evaluation (level of self-reported physical activity, cardiorespiratory fitness (CRF), obesity measured by the body mass index (BMI), body fat percentage (BF%) and waist circumference (WC), fasting total cholesterol, triglycerides and glucose). The CBMES also provided us with information regarding how the variables were collected in the evaluations.
Inclusion and exclusion criteria
Our analysis included all male firefighters, without an age restriction, who participated in the evaluations of ‘Bom Estar’ in 2018 and completed forms for all variables. Forms from military firefighters with incomplete data were excluded from the analysis. Additionally, data from female firefighters were not used in the analysis given the sex difference in cardiometabolic, obesity and physical performance parameters.
Sociodemographic variables
Age was categorised into the ranges: under 30, from 30 to 39, 40 to49 or 50 to59 years old. Education level was grouped into three categories: high school (when the firefighter completed high school), graduation (when the firefighter obtained a college/university degree) or postgraduate (when the firefighter obtained a master’s degree or a PhD). Family monthly income was converted into US dollars (US$) and separated in six categories: less than US$ 510.00, US$ 510.00 to 1020.00, US$ 1020.00 to 1530.00, US$ 1530.00 to 2040.00, US$ 2040.00 to 2550.00 or above US$ 2550.00. Marital status was categorised into three levels: married, including living with a partner, single or other, which included divorcees and widowers. Access to health insurance coverage was categorised as yes or no.
Occupational variables
The distribution according to the work location was categorised in the capital of Espírito Santo, Vitória, the main metropolitan cities, Vila Velha, Cariacica or Serra and inner cities. The type of current activity was grouped in two categories: operational activity, which includes militaries working in shifts and performing activities such as firefighting and paramedic transport, and administrative activity, which represents individuals working during business hours in administration activities. Given that Brazilian military firefighters exert several functions throughout their careers, the main operational activity performed during their career was also recorded in the forms. The categories of the main operational activity exerted included Rescue, that is, paramedic service, ABTS, an abbreviation from the Portuguese ‘Auto-Busca Tanque e Salvamento’, which represents military personnel who perform various tasks, such as firefighting, rescue at heights, land rescue and demobilisation and the category Other, which represents operational activity involving security diving, surveillance services and civil protection from disasters.
Life habits variables
In the forms completed during the annual firefighter inspections, there were some questions concerning religious practice, leisure and smoking habits. The first question referring to religious practice was if they had any religion. The possible answers included a list of religions as well as the option ‘other’ (if none of the choices corresponded to their religion). The answer ‘none’ was also available if the firefighter did not have a religion. If they reported a religion, the next question was whether they practice it. Based on the provided answers, the religious practice was categorised as yes, no or not applicable. This last option was marked by the firefighters if they selected ‘none’ for the first question. Concerning leisure practice, the question present in the forms was simply if they practice any kind of leisure activity. The possible answers were yes or no. Finally, the firefighters also reported whether they smoke. Thus, leisure and smoking habits were categorised as yes and no. Individuals were considered to be smokers regardless of the smoking frequency they reported.
Fitness and health status variables
The completed forms also asked the firefighters about their physical activity. The first question was whether the participant practiced any physical activity. If the answer was yes, he or she had to report how many times a week and the duration of the activity. Based on those answers, duration and frequency of self-reported physical activity (SRPA) was computed in minutes/week and used to estimate the cardiovascular protection based on the American Heart Association (AHA) recommendations, which states that adequate protection requires 150 min of physical activity/week.18 According to this definition, the SRPA was categorised as protected or at risk.
Maximum oxygen consumption (VO2 max; mL.min-1.kg-1) was indirectly estimated based on the Cooper test and calculated according to a previously described equation.19 For this test, the distance reached by the participants within 12 min is recorded. The VO2 max is divided by 3.5 and converted into metabolic equivalents (METs)20 to estimate CRF. According to the National Fire Protection Association,21 for firefighting duties, a minimum of 12 METs of effort is recommended. Thus, we adopted this value as the CRF cut-off point (categories: ≥12METs and <12METs).
Obesity was estimated through BMI, BF% and WC. BMI was derived from the ratio between body weight and the squared height (kg/m2). Individuals were weighed on a scale (TANITA, model UM-080), with a 150 kg capacity and 0.1 kg precision. Height was measured with an inextensible tape (Microlife) with a 1 cm width and 1 mm precision, fixed in the vertical position with the aid of a rigid ruler. The obtained results were grouped as eutrophic (BMI <25 kg/m2), overweight (25≤ BMI <30 kg/m2) or obese (BMI ≥30 kg/m2). BF% was derived from thigh, abdomen and chest skinfold measurements and calculated as previously described.22 23 According to the WHO guidelines, which states a maximum limit of 25% of body fat for men,24 the individuals were categorised as non-obese (BF% <25%) or obese (BF% ≥25%).
CO was determined by measuring the WC with an inextensible tape. The obtained data were grouped as no risk (WC <94 cm) and at risk (WC ≥94 cm), according to cut-off points stated by the International Diabetes Federation.25 Given that the Brazilian Society of Cardiology has adopted CO for cardiovascular risk calculations,26 and as we were particularly interested in the association of personal, occupational, fitness and health status factors with an obesity index more strictly related to cardiovascular risk, this obesity measure was chosen as the outcome for adjusted OR calculation.
Capillary glycaemia after a 12 hours fast was evaluated with a portable blood glucose metre (INFORM II Roche) designed for hospital use.27 28 This variable was categorised as <100 mg/dL or ≥100 mg/dL.25 Fasting total cholesterol and triglycerides were measured with strips using equipment (Accutrend Plus, Roche) validated for cardiovascular screening purposes.29 Data from total cholesterol was categorised as <200 mg/dL or ≥200 mg/dL, while triglycerides data were grouped as <150 mg/dL or ≥150 mg/dL, according to the recommendations of the American Association of Clinical Endocrinologists and American College of Endocrinology.30
Statistical analysis
Descriptive analysis was used to characterise the variables. The results are presented in absolute and relative frequencies, means and SD. The association between CO (dependent variable) and the independent variables was analysed by the X2 test, with p<0.05 set at the level of significance. A hierarchical binary logistic regression model was performed according to the theoretical model described in figure 1. Block 1 represents the sociodemographic variables, followed by occupational (block 2), lifestyle (block 3) and fitness and health status (block 4) variables. Variables with p≤0.20 were included in the model by following the method ‘enter’. In the final model, only variables with p<0.05 were considered statistically significant. The Statistical Package for Social Sciences (SPSS) software (V.25) was used for statistical analysis.
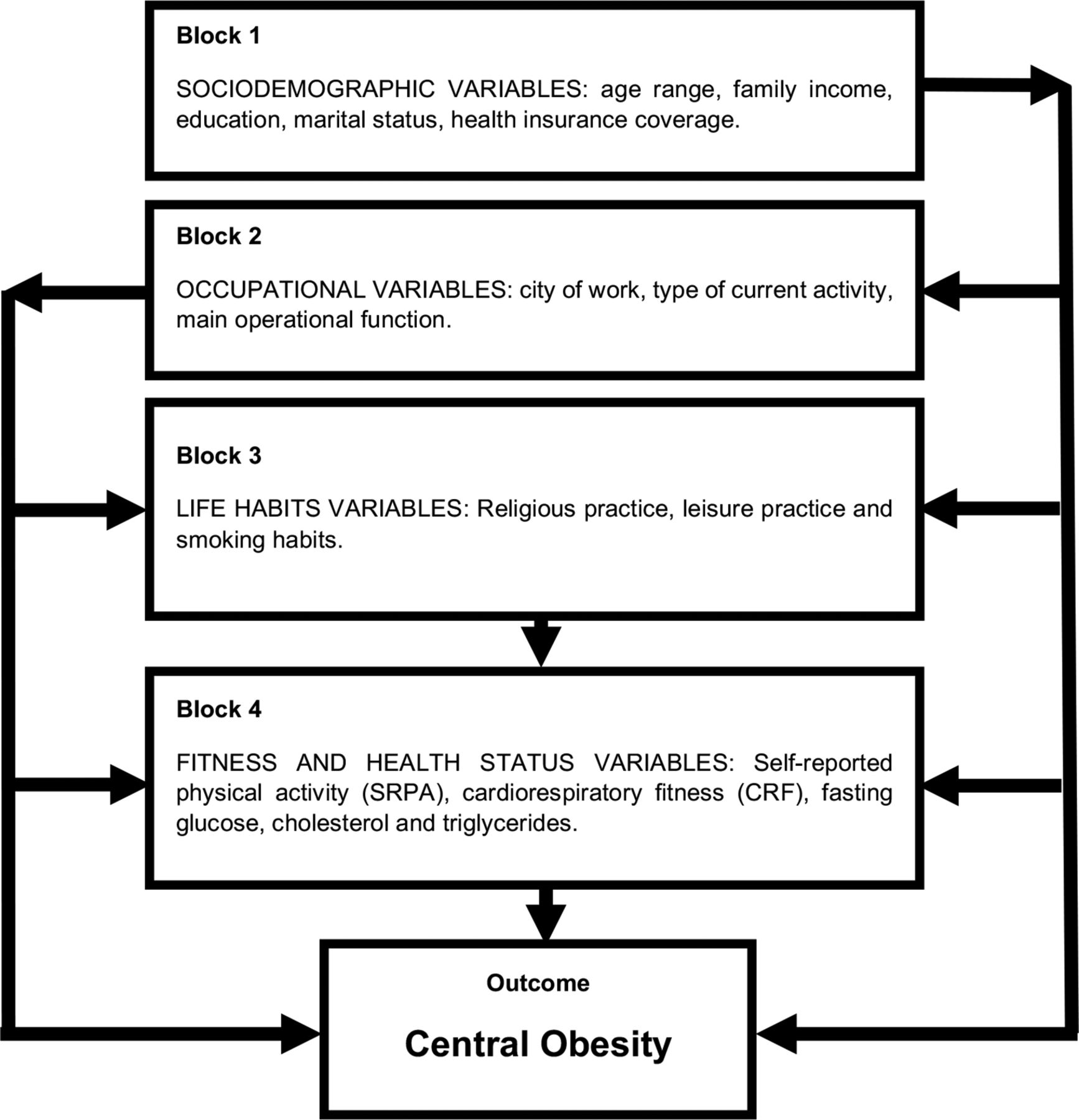
Theoretical model of variables associated with central obesity
Patient and public involvement
The evaluated participants were not involved in the development of the study, choice of outcome, adopted cut-off measures nor in planning or conducting this study. The results will be disclosed to the participants and the general public through the publication of this article as well as a technical report sent to the CBMES command.
Results
Data from 892 male firefighters were included in the final analysis (figure 2). In 2018, there were 1256 military firefighters registered in the corporation, but 238 missed the evaluations for various reasons. From the 1018 participants, 18 were excluded due to the incompleteness of their data. In order to allow comparison with other studies involving firefighters, which often evaluate males, 108 female firefighters were excluded from the analysis.

{kind=link}
{kind=link}
Characterisation of the studied population.
Tables 1 and 2 present the general characteristics of participants and results from fitness and health status evaluations. From the 892 analysed participants, 349 were 30 to 39 years old. The majority of individuals (32.96%) had a monthly income between US$1020.00 and US$1530.00, completed graduation or postgraduate courses (66.48%) and were married (70.40%). Further, a high proportion of firefighters (37.11%) did not have health insurance coverage.
Sociodemographic, occupational and lifestyle characteristics of male firefighters of the Military Fire Service of the State of Espírito Santo (CBMES)
Fitness and health status data of male firefighters of the Military Fire Service of the State of Espírito Santo (CBMES)
Considering the workplace distribution of participants, 51.91% of the firefighters worked within the capital and surrounding metropolitan cities of Espírito Santo, with 48.09% working in the inner cities. There was a slightly higher frequency of firefighters working in operational activities (56.73%). The average years of service at the corporation was 12.65±7.98. The main operational activity reported was ABTS (40.25%), which includes various tasks, such as firefighting, rescue at heights, land rescue and demobilisation. The time spent in the main operational activity was on average 6.96±5.48 years. The majority of the population reported religious (61.55%) and leisure (90.36%) practices, and the majority were non-smokers (97.2%).
Considering the SRPA and the criteria established by the AHA for cardiovascular protection based on frequency and duration of physical activity, 557 (62.44%) firefighters were classified as at risk. Despite these data, the majority of the corporation (65.02%) presented a CRF ≥12 METs.
The obesity estimation by BMI identified that 48.65% of firefighters were overweight and 10.99% were obese; the average BMI of the population was 26.16±3.32 kg/m2. When obesity was estimated based on the fat percentage, the frequency of firefighters considered obese was 26.23%; the mean value for BF% was 20.77±6.82. When analysing CO measured by the WC, the frequency of firefighters at risk was 18.61% (the mean WC in the population was 87.07±8.65 cm).
With regard to blood biochemical measurements, the prevalence of firefighters with levels above the recommended limits for cholesterol was 22.98%, 30.72% for glucose and 14.01% for triglycerides.
Table 3 presents the associations of sociodemographic, occupational, life habits, fitness and health status variables with CO. There was a significant association between CO and the age range, family income, marital status, SRPA, CRF and levels of total cholesterol, glucose and triglycerides. The frequency of individuals with CO increased in older age ranges. A lower family income was more prevalent within non-obese individuals. According to the marital status, the frequency of CO increased among married individuals and in the category other when compared with the single category. Education, access to health insurance coverage, occupational and life habit variables were not associated with CO. All fitness and health status variables were associated with CO, with lower frequencies of SRPA, lower CRF and higher levels of total cholesterol, glucose and triglycerides observed in individuals with CO.
Sociodemographic, occupational, life habits, fitness and health status variables association with central obesity in male firefighters of the Military Fire Service of the State of Espírito Santo (CBMES)
Table 4 presents the data from the binary logistic regression model with CO as the outcome. After adjustments, there were increased odds of CO for the age range of 50 to 59 years old (OR 2.93; 95% CI 1.05 to 8.14), for low physical activity (OR 1.95; 95% CI 1.14 to 3.34), for lower CRF (OR 5.15; 95% CI 3.22 to 8.23) and for higher levels of glucose (OR 1.70; 95% CI 1.07 to 2.72) and triglycerides (OR 3.12; 95% CI 1.75 to 5.55).
Crude and adjusted OR for central obesity
Discussion
Our study analysed data collected in a pioneering health programme developed among Brazilian firefighters that collects sociodemographic, occupational, lifestyle, fitness and health status variables. Based on the BMI results, there was a low prevalence of obesity among this firefighter population but an overall high prevalence of overweight and obese individuals. We also identified that CO prevalence increased with age and was more likely associated with low physical activity, low CRF, hyperglycaemia and hypertriglyceridaemia. These data are very important to provide a picture of this occupational group and to subsidy evidence-based interventions, given that obesity is a factor for worse professional performance in this category of workers. In addition, investigation of the factors associated with CO could point to important targets for prevention in this occupational group.
The prevalence of obese firefighters (BMI ≥30 kg/m2) in our study was lower (10.99%) compared with the prevalence reported in the Brazilian population of adult males (18.5%).4 Our study also showed a lower obesity prevalence when compared with firefighter populations of the USA9 31–35 and Canada.36 On the other hand, two studies that described obesity (using BMI) among Brazilian firefighters from the Federal District showed similar frequencies of obese firefighters compared with our study.15 16 The low prevalence of obesity among the Brazilian firefighters could be due to a phenomenon known as the ‘healthy worker effect’.37 38 Many workers, such as firefighters, police officers and the military in general, undergo exhaustive physical and resistance tests for health-based selection before admission to work.37 38 These selection criteria could contribute to lower obesity frequencies among this work population. By contrast, the overall frequency of overweight plus obese firefighters in our study was quite high (59.64%). This finding is similar to what has been described for other populations of firefighters within and outside of Brazil15 16 31 34 36 39 and surpasses the prevalence observed among the Brazilian adult man (BMI ≥25 kg/m2; 57.6%).4 There are two possible explanations for these apparently conflicting results. One possibility is that despite the health-based selection process, some occupational factors may contribute to worsen the health status and, consequently, increase the overweight prevalence in this occupational group. However, the high prevalence of overweight plus obese firefighters may reflect a problem related to the overweight estimation by BMI in this occupational group.
Some studies point out that the rate of overweight firefighters by the BMI can be overestimated.15 35 40 Similar results have been observed in other physically active population when estimating overweight through this parameter.41 42 In these populations, muscle hypertrophy tends to overestimate overweight (but not obesity) because the BMI does not differentiate the weight of fat mass (fat tissue) and lean mass (muscle tissue). In a study conducted among male firefighters from California,35 when the BMI overweight cut-off point was changed to 27.5 kg/m2, there was an increase in the agreement in adiposity classification by the BMI, WC and BF% measures. Porto and colleagues15 also observed that standardised BMI cut-off points were not useful to identify obesity in a group of firefighters with adequate CRF. Similarly, in a study conducted among 994 male US firefighters,40 there were higher frequencies of non-obese misclassification by the BMI when compared with the WC and BF% classification. On the other hand, Poston and colleagues31 showed low rates of obesity misclassification among firefighters by the three methods (BMI, WC and BF%). Therefore, given the evidence of overweight overestimation by BMI among firefighters and the close relationship between CO and cardiovascular disease risk and mortality,12 25 26 this obesity measure was chosen as the outcome in our study.
Our findings indicated that CO is more likely associated with age. Among the younger group (up to 30 years), the prevalence of CO was only 9.64%, compared with 36.59% in the 50- to 59-year-old population. In a study conducted by Choi and colleagues,35 age was positively correlated with obesity among firefighters. In a prospective cohort conducted in firefighters, there was a significant increase in weight during a 5-year period in this occupational group.43 The ageing effect on obesity has also been confirmed by other studies among firefighters.44 45 However, this increase in the obesity profile can be prevented by initiatives of health behaviour changes that should be monitored in annual health inspections.44 45 Considering the expected changes observed with ageing, prevention as well as intervention programmes would be important initiatives to improve the obesity scenario among this occupational population.
In our study, a low SRPA was more likely associated with obesity. These results are reinforced by the CRF results, where there was an increased OR of CO among individuals with lower performance. Porto and colleagues15 observed a clear trend for reduced physical fitness among Brazilian firefighters within the overweight and obese categories. Another study conducted among Brazilian firefighters16 also showed that less fit firefighters were more likely to have a poor body composition independent of the adopted obesity measure. Physical activity is an important cardiovascular protective factor for firefighters. Low levels of aerobic capacity may lead to failure in action. Aerobic fitness is of the utmost importance in the firefighting service because it increases the efficiency of the heart and improves many physiological parameters that are required to optimise the ability to perform work.9 Therefore, regular assessment of physical fitness should be conducted in this work population, allied to interventions devoted to improving this condition in this occupational group.
CO was also more likely associated with elevated levels of glucose and triglycerides. It is also worth noting that there were individuals among the obese firefighters with adequate levels of total cholesterol, glucose and triglycerides; these subjects represent a profile described as metabolically healthy but obese.46 CO, elevated triglycerides, high fasting glucose levels and other cardiovascular risk factors can be used to define the presence of metabolic syndrome (MetS).25 Many studies have evaluated the metabolic profile of firefighters by addressing the presence of MetS.39 47 48 These studies showed a negative association between CRF and MetS within this occupational group.39 48 Unfortunately, the health screening tests performed by the ‘Bom Estar’ project did not provide all the components that are required to characterise the MetS profile. Inclusion of high-density lipoprotein cholesterol and insulin measurements among the annual health inspection performed by the corporation would definitely allow for a more adequate characterisation of the metabolic profile of this occupational group.
Strengths and limitations of the study
This study is the first to investigate the factors associated with CO in Brazilian firefighters. the adopted statistical analysis improved the understanding of the factors associated with this outcome. However, the absence of some biochemical measurements in the annual health inspections limited a more profound characterisation of this occupational group. Despite this deficit, the initiative of the ‘Bom Estar’ project should be acknowledged and adopted for all Fire Service Corporations within Brazil. Similar projects have been developed outside Brazil and proven to significantly improve a number of health dimensions.32 45 49 Despite the costs that a multidimensional annual health inspection may impose on the entire team, it might lead to a number of economic and lifesaving advantages. For example, it might reduce work-related injury, disability, absenteeism and the risk of fatal cardiac events. It could also potentially improve the quality of occupational performance, which can have direct impacts on the service provided to the population.
It is important to recognise some limitations of this study. First, the cross-sectional nature does not allow us to draw correlations or determine the association direction between the related variables. Second, we cannot extrapolate the results from our study to the whole population of Brazilian firefighters because it only refers to the male workers of one region of Brazil. Longer follow-up periods will be also required to adequately measure the impact of age on performance and obesity profile of this occupational population. Furthermore, it is important to state that the firefighters know in advance the CRF limit that should be reached. Therefore, it is possible that some firefighters might have performed below their full capacity during the test, and some individuals might have gone beyond their limits to reach adequate levels.
Conclusions
The prevalence of obesity in this firefighter population was below what has been described for firefighter populations in other countries, but there was a high frequency in the overall prevalence of overweight and obesity. Age, physical activity and cardiometabolic health variables were significantly associated with a higher prevalence of CO. Our study demonstrates the need for prevention and intervention programmes among military firefighters to avoid the progression of cardiometabolic disorders and obesity. This endeavour should help reduce the cardiovascular risk susceptibility for this group of workers.
Acknowledgments
We would like to thank Dr Antonio Francisco Gomes Louzada and Dr Willian de Sá Lessa for supporting the initial development of the study. We also want to thank the Lieutenant Colonel Adeilton Costa Pavani and the Fire Chief Commander of the CBMES, Colonel Carlos Marcelo D’Isep Costa, for their support during the entire development of the study.
References
Footnotes
Contributors FCD: Collected the data, developed the study, conducted a literature review, performed statistical analysis and drafted and revised the manuscript. TJB: Collected the data, helped with the literature review and study development and drafted and revised the manuscript. LRA: Helped with the development of the study, participated in the literature review and manuscript drafting and gave final approval of the manuscript. EZ: Co-supervised FCD and TJB, conducted statistical analysis, participated in the literature review and drafting the manuscript and gave final approval of the manuscript. KNS: Supervised FCD and TJB, designed the study, participated in the literature review and drafted, wrote and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethics Committee of Research in Humans (CEP-UFES, approval number CAAE 80483117.1.0000.5060) of the Federal University of Espírito Santo.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. The data analysed under the present study is not publicly available. Access to the data is conditioned on the approval of the command of the CBMES. Additionally, a 5-year follow-up study that uses the present data is also planned.