Article Text

Abstract
Objectives To examine the associations of parental social and economic position with health-seeking behaviour for diarrhoea and acute respiratory infection (ARI) among under-5 children in Myanmar and explore potential underlying mechanisms.
Design A cross-sectional study.
Setting A secondary dataset from the nationwide 2015–2016 Myanmar Demographic and Health Survey (MDHS).
Participants All under-5 children in the sampled households with reported symptoms of diarrhoea and ARI during the 2-week period preceding the MDHS survey interview.
Primary and secondary outcome measures Four parental health-seeking behaviours: ‘seeking treatment’, ‘formal health provider’, ‘public provider’ and ‘private provider’ were considered. Social and economic positions were determined by confirmatory factor analysis. Multilevel logistic regressions were employed to examine the associations of social and economic positions with health-seeking behaviours for diarrhoea and ARI. Mediation analyses were conducted to explore potential underlying mechanisms in these associations.
Results Of the 4099 under-5 children from the sampled households in MDHS, 427 (10.4%) with diarrhoea and 131 (3.2%) with ARI were considered for the analyses. For diarrhoea, social position was positively associated with seeking treatment and private provider use (adjusted OR: 1.60 (95% CIs: 1.07 to 2.38) and 1.83 (1.00 to 3.34), respectively). Economic position was positively associated with private provider use for diarrhoea (1.57 (1.07 to 2.30)). Negative associations were observed between social and economic positions with public provider use for diarrhoea (0.55 (0.30 to 0.99) and 0.64 (0.43 to 0.94), respectively). Social position had more influence than economic position on parental health-seeking behaviour for children with diarrhoea. No evidence for a significant association of social and economic position with health-seeking for ARI was observed.
Conclusions Social and economic positions were possible determinants of health-seeking behaviour for diarrhoea among children; and social position had more influence than economic position. The results of this study may contribute to improve relevant interventions for diarrhoea and ARI among children in Myanmar.
- community child health
- public health
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first in-depth analysis of parental health-seeking for childhood diarrhoea and acute respiratory infection (ARI) in Myanmar.
This study shows the degree of influence of social position and economic position on parental health-seeking behaviour in Myanmar, which may contribute to improving relevant interventions.
Understanding socioeconomic gradients in health-seeking behaviour may help address socioeconomic disparities and reduce the burden of preventable deaths from diarrhoea and ARI among under-5 children in Myanmar.
Since the outcomes in this study depend on the mother’s self-report of child illness and health-seeking actions, the perception and accurate recall of illness may have some reliability and validity issues.
Introduction
Substantial progress has been made in reducing child mortality since 1990.1 The under-5 mortality rate has decreased by 58%, from 93 deaths per 1000 live births in 1990 to 39 in 2017 worldwide.1 Myanmar has achieved significant success in reducing under-5 mortality with a 50% reduction in the 2000s.2 However, this rate remains high at 50 per 1000 live births in 2015.2 Diarrhoea and acute respiratory infection (ARI) are leading preventable causes of under-5 mortality.3 4 In Myanmar, diarrhoea and ARI attributed to 20% of under-5 mortality in 2014.5
Prompt diagnosis and appropriate management of diarrhoea and ARI is essential for reducing morbidity and mortality among under-5 children.6 Success in reducing childhood mortality needs more than the availability of adequate health services with well-trained health professionals.7 As families are the first people responsible for child care, improving parental health-seeking behaviour is important for successful and effective disease control for children.8 Not receiving prompt healthcare service makes diagnosis and disease management difficult in children in low-resource settings.7 8 However, today, globally only about 40% and 60% of children receive adequate healthcare when diarrhoea and ARI symptoms arise, respectively.3 4 Among those who receive necessary healthcare, service utilisation varies between the public and private sector.3 4 9 In Myanmar, public providers offer essential child health services free of charge according to national guidelines. Private providers can provide higher quality care, a broader range of services and offer more flexible hours with a wide range of consultation fees.2 However, the quality of the services from both private and public providers has not been well-monitored. Financial catastrophe as a result of payments for healthcare in Myanmar is common.10
Parental socioeconomic position plays a significant role in health-seeking decision-making for common childhood illnesses.9 11 According to the UNICEF, between 2011 and 2016, around 60% of children with symptoms of ARI from the richest quintile in the least developed countries (LDCs) were taken to a health provider.4 In contrast, only 40% of children from the poorest quintile were taken to a healthcare provider.4 This suggests socioeconomic inequalities in parental health-seeking behaviour. The 2017 World Bank Poverty Report found that almost one-third of the population in Myanmar lived below the poverty line in 2015.12 Half of the rural population were in the lowest household wealth quintile.12 The 2015–2016 Myanmar DHS report showed that 62% of under-5 children with diarrhoea and 63% of under-5 children with ARI whose mother had secondary education received appropriate treatment.13 It is well-understood that socioeconomic factors influence health-seeking behaviour. However, the relative importance of the influence of social or economic position on health-seeking behaviour varies among countries with different sociodemographic and economic contexts.11 14 15
In Myanmar, a large literature gap exists regarding socioeconomic disparities in parental health-seeking behaviours for children. This is the first nationwide study in Myanmar to examine the association between health-seeking behaviour with social position and economic position using adjusted analytical methods. The objectives of this study were twofold. The first objective was to examine the association of parental social position and economic status with health-seeking behaviour for diarrhoea and ARI in under-5 children in Myanmar. The second objective was to explore potential mechanisms underlying such associations by mediation analysis which enabled an assessment of relative importance of the influence of social or economic position on health-seeking behaviours.
Methods
Study design
This study is cross-sectional in design.
Data source (nationwide 2015–2016 Myanmar Demographic and Health Survey)
We used secondary data from the nationwide 2015–2016 Myanmar Demographic and Health Survey (MDHS). MDHS is a cross-sectional household survey implemented by the Ministry of Health and Sports, Myanmar.13 The 2015–2016 MDHS used a stratified two-stage sampling design.13 Data from the survey consists of 13 260 households from 4000 primary sampling units collected nationally, for urban and rural areas, and for each of the 15 administrative regions of Myanmar.13 According to the DHS, written informed consent was obtained from all participants before they enrolled in the survey.13 The overall response rate for women and household questionnaire were 96% and 98%, respectively.13
Population and measurement
Target population
This study included all under-5 children with reported symptoms of diarrhoea and ARI in the sampled households during the 2-week period preceding the MDHS survey interview. MDHS collected the information related to under-5 children health from the women’s questionnaire.13 This questionnaire asked the sampled households with mothers aged 15–49 years in the 5-year recall period.13 If the child had both symptoms of diarrhoea and ARI, he or she was included separately in each of the diarrhoea and ARI analyses.
Patient and public involvement
Patients and the public were not involved in this study as the data were extracted from the MDHS, which did not contain any personally identifiable information.
Social position and economic position
In this study, social and economic position (two latent variables) were estimated by using confirmatory factor analysis (CFA). This was done in order to separate the effects of household material resources and knowledge for further analyses. Briefly, social position reflects knowledge and capacity to access information and ability to interact with healthcare provider.11 16–18 Economic position captures the household-level material resources available which reflects the wealth of the household to meet the direct and indirect costs of care while household income data are not available.11 17 Social position is based on observed indicators from MDHS such as mother’s literacy and education, and the occupational status of mother and father. Similarly, economic position is based on household-level material resources data from MDHS such as household utilities, household assets and household service use.9 11 13 17
Health-seeking behaviour outcomes
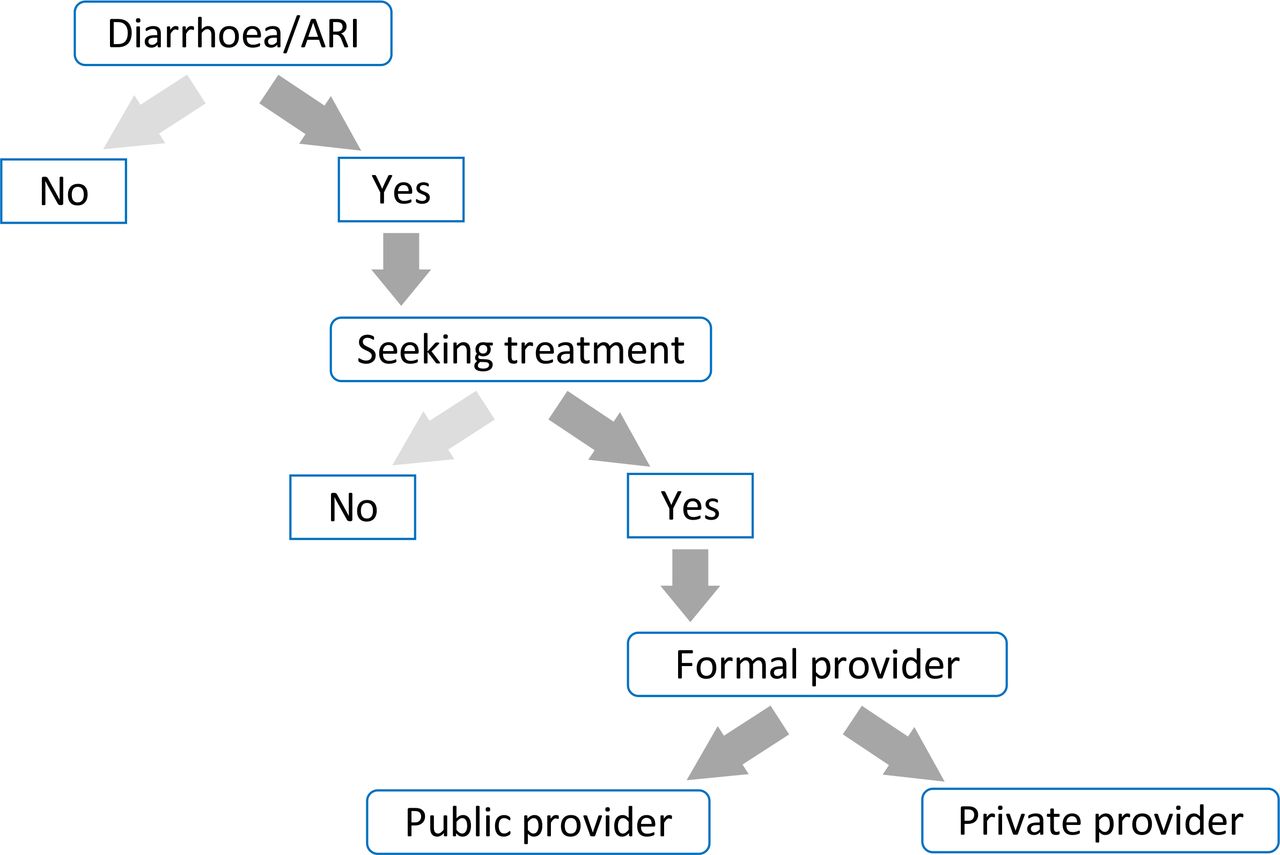
In order to assess health-seeking behaviours for diarrhoea and ARI, we first extracted reported cases of these illnesses among under-5 children (0–59 months of age) within the 2-week period before the survey interview. Diarrhoea was defined as the passage of three or more loose or liquid stools per day according to UNICEF.3 ARI was defined as cough accompanied by short, rapid breathing that is chest-related and/or difficult breathing that is chest-related according to the Myanmar Ministry of Health and Sports.13 The main health-seeking behaviour outcomes for this study were the following four binary outcomes, defined for each illness (diarrhoea and ARI) separately: whether treatment was sought; and if so, whether it was sought from formal health provider and whether it was sought from formal public provider or private provider—hereafter, ‘seeking treatment’, ‘formal health provider’, ‘public provider’ and ‘private provider’, unless indicated otherwise (figure 1).11 19 Seeking treatment was defined as the proportion of under-5 children who had symptoms of diarrhoea, ARI or both in the past 2-week period preceding the MDHS survey interview, for whom treatment was sought from formal or informal provider.13 Formal public and private health provider were defined as all public or private health clinics starting from community health workers to tertiary teaching hospitals.6 Other sources like shops, markets and traditional practitioner were not considered as formal public or private health provider.6

Dimensions of health-seeking behaviours for diarrhoea and acute respiratory infection (ARI) among under-5 children in Myanmar.
Statistical analysis
Social and economic position were first estimated by CFA. Subsequently, we conducted descriptive, regression and mediation analyses for health-seeking behaviour for each illness (diarrhoea and ARI) with the four-binary health-seeking behaviour outcomes (‘seeking treatment’, ‘formal health provider’, ‘public provider’ and ‘private provider’). If a child had suffered from both diarrhoea and ARI, he or she was included in both analyses. We described the distribution of discrete variables by percentages and compared results using χ2 test. We summarised social position and economic position, continuous variables, using means, SEs and differences tested using the t-test. We accounted for the complex survey sampling design (clustering, stratification and sample weights) to adjust for the cluster sampling survey design since the MDHS used a multistage cluster sampling procedure.13
Confirmatory factor analysis for social and economic position
To separately assess the inequalities of social and economic status in health-seeking behaviours, two continuous latent variables, parental social position and household economic position, were estimated using CFA. CFA is a variant of structural equation modelling technique that can model the relationships between observed and latent variables simultaneously.20 The full information maximum likelihood method was used to estimate path coefficients and covariance matrices.20 Joint normality of all variables is assumed and missing values are assumed to be missing at random.20 Model fit was assessed with the comparative fit index (CFI), the Tucker-Lewis index and standardised root mean squared residual (SRMR).20 The summary statistics of observed variables and their factor loadings for social position and economic position are shown in online supplementary tables 1,2. The resulting latent measurement models for both social and economic position constructs had an acceptable fit to the data; the SRMR level was <0.08 and the CFI/TFI was ≥0.9 (online supplementary table 3).20
Supplemental material
Regression analysis
For both diarrhoea and ARI, we used multilevel logistic regression models to examine the association between the dependent variables (four binary health-seeking behaviours) and two main explanatory variables (latent continuous social position and economic position variables), adjusted for other covariates. Since MDHS data are hierarchically sampled, the models also adjusted for the random effects at household, cluster and region levels to control for the fact that data of the same households, clusters and regions were correlated.21
Covariates
Child age group, number of under-5 children living together in the household, place of residence, administrative regions and immunisation status were regarded as covariates in the regression modellings.11 14 15 Since the prevalence and health-seeking behaviour of diarrhoea and ARI varies between infants and children,11 14 15 22 we categorised child age group into two categories, 0–11 months age group (infant) and 12–59 months age group (child). We classified number of under-5 children in the same household into two categories: only one child and two or more children in the same household because number of under-5 children in the same household may influence the ability of parent to seek appropriate care.11 14 15 As availability and quality of health services varies with the place of residence and administrative regions,11 23 community-level covariates included place of residence (urban and rural) and administrative regions. Immunisation status was also analysed as a covariate because it is a preventable measure of childhood illnesses and it also correlates with health-seeking behaviour.24 25 If the child received BCG, polio, diphtheria-pertussis-tetanus/pentavalent, hepatitis B and measles/measles-rubella vaccines according to the national immunisation schedule according to their age, we regarded his or her immunisation status as complete and if not, incomplete. In addition, the presence of blood in stool was regarded as a proxy for illness severity in diarrhoea and adjusted as a covariate.11 22 23 Binary variables indicating whether the child suffered from ARI or fever during the 2-week period preceding the survey were included in the analyses for diarrhoea.11 22 23 Likewise, binary variables reflecting whether the child had fever or diarrhoea were also included in the analyses for ARI.11 22 23
Mediation analysis to explore underlying mechanisms
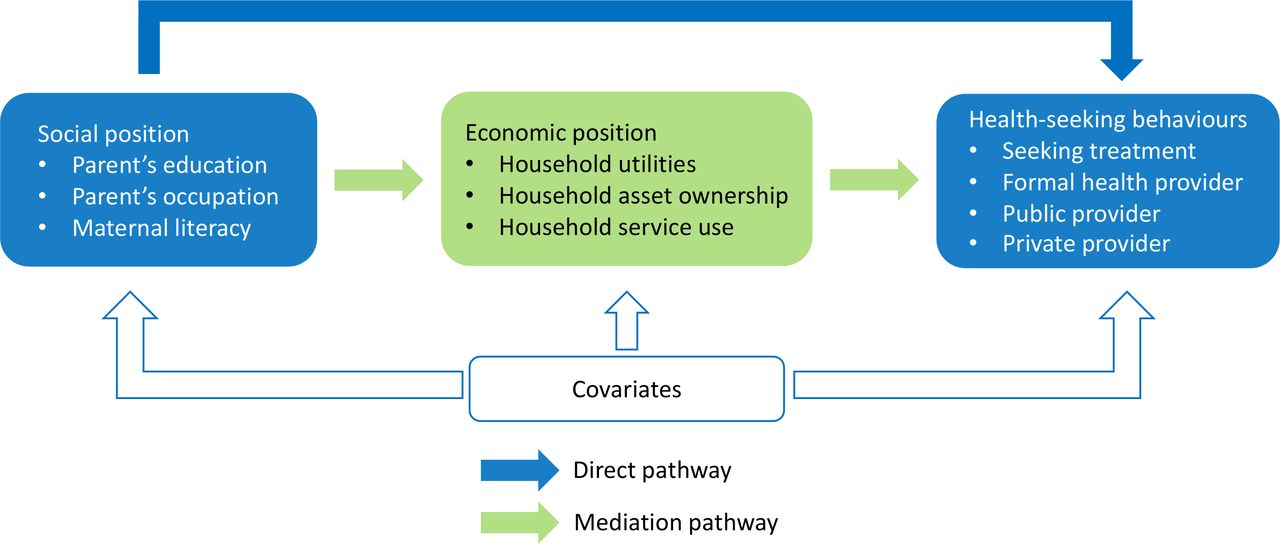
We conducted a mediation analysis to explore the influence of social position mediated by economic position on each of the health-seeking behaviours. Our mediation analysis model used two latent variables—parental social position and household economic position—capturing two constructs of socioeconomic status. Mediation analysis is an assessment to estimate the direct association between social position and health-seeking behaviour considering that the social position (independent variable) influences the economic position (mediator variable) which in turn influences the health-seeking behaviours (dependent variables).26 27 The conceptual mediation framework (path diagram) is presented in figure 2. The path diagram represents the statistical expression of the mediation model, where the total effect of social position is the sum of its direct (A) and indirect (B, mediated by economic position) effects.26–28 The estimation of the direct effect involves examining the changes in the outcome when changing values of the exposure while keeping the value of the mediator at a certain level.27 The indirect effect is estimated by fixing the value of the exposure at a certain level while examining the effect of changing the values of the mediator on the outcome.27 28 The sum of the direct and indirect effects is the total effect of the exposure.27 28

{kind=link}
{kind=link}
Conceptual path diagram for mediation analysis of social and economic position on health-seeking behaviour for under-5 children with diarrhoea and acute respiratory infection (ARI) in Myanmar.
Results
Descriptive characteristics
A total of 4099 under-5 children were identified in the 2015–2016 MDHS. Of these, 427 (10.4%) reporting diarrhoeal symptoms and 131 (3.2%) with ARI symptoms were included in the analyses. Table 1 shows the descriptive characteristics of the children included in this study. Among these under-5 children, 81.8% with diarrhoea and 88.6% with ARI were aged 12–59 months. Around 80% of the under-5 children with diarrhoea or ARI were living in rural areas. The complete immunisation status of children with diarrhoea (58.2%) and of children with ARI (43.7%) did not differ significantly from all children (52.8%). Among children with diarrhoea, 45.5% lived in households with medium social position and 45% with low economic position. The mean parental social and household economic position scores were lower in households of under-5 children with diarrhoea (1.19 and 1.55) and ARI (1.21 and 1.56) than households of all under-5 children (1.23 and 1.70).
Descriptive characteristics of demographic and socioeconomic variables among under-5 children in Myanmar, 2015–2016
Multilevel logistic regression
The associations of parental social position and economic position with health-seeking behaviours (‘seeking treatment’, ‘formal health provider’, ‘public provider’ and ‘private provider’) for diarrhoea are shown in table 2. Social position was positively associated with seeking treatment and private provider use. One unit increase in standardised score of social position resulted 1.60 (95% CI 1.07 to 2.38, p<0.05) times higher odds of seeking treatment (table 2) and 1.83 (1.00 to 3.34, p<0.05) times higher odds of private provider use (table 2). Economic position was also positively associated with private provider use; one unit increase in standardised score of economic position resulted in 1.57 (1.07 to 2.30, p<0.05) times higher odds of private provider use (table 2). Meanwhile, both social and economic position were negatively associated with public provider use: adjusted ORs 0.55 (0.30 to 0.99, p<0.05) and 0.64 (0.43 to 0.94, p<0.05), respectively (table 2). Social and economic position were negatively associated with public provider use and positively associated with private provider use. Because of the opposite direction of these associations and the effect size of combinations of public and private provider, no evidence of statistically significant associations between social and economic positions with health-seeking from formal health provider was observed.
Multilevel analysis for association of social and economic position with health-seeking behaviour for under-5 children with diarrhoea in Myanmar
Compared with children with diarrhoea from urban areas, children who were living in rural areas had a 3.86 (95% CI 1.40 to 5.65, p<0.05) times higher odds of receiving treatment from a formal health provider (table 2), while they had 0.41 (0.15 to 0.90, p<0.05) times lower odds of private provider use (table 2). Severity of illnesses like blood in stool and diarrhoea together with fever in the recall period was also positively associated with seeking treatment (OR 3.23 (1.09 to 5.14), p<0.05), formal health provider use (1.62 (1.26 to 4.38), p<0.05) (table 2) and private provider use (2.63 (1.58 to 6.98), p<0.05) (table 2). Similarly, children with diarrhoea who had fever during the 2-week recall period preceding the survey had 1.65 (1.04 to 2.25) (p<0.05), 1.42 (1.07 to 2.73, p<0.05) and 1.24 (1.03 to 2.94, p<0.05) times higher odds of seeking treatment, formal health provider and private provider use (table 2), respectively.
The relationships of parental social position and economic position with health-seeking behaviours (‘seeking treatment’, ‘formal health provider’, ‘public provider’ and ‘private provider’) for ARI are shown in online supplementary table 4. There was no evidence of statistically significant associations between social and economic position with health-seeking behaviours for ARI. However, children with ARI who developed severe symptoms like fever together with ARI had 1.32 (1.06 to 3.75), 1.84 (1.27 to 2.61) and 3.17 (1.45 to 6.52) times higher odds of seeking treatment and formal health provider and private provider use, respectively (online supplementary table 4).
Mediation analysis
Table 3 shows the results of the mediation analysis with the adjusted models for health-seeking in response to diarrhoea and ARI. Among children with diarrhoea, social position was positively associated with seeking treatment, formal health provider and private provider use. The effect of social position on health-seeking behaviour has two components: direct effect without economic position and mediation effect of economic position. For instance, among children with diarrhoea, a one-unit increase in social position score was associated with an 11.7% (95% CI 3.8% to 19.8%) increase in the probability of seeking treatment. The direct effect of social position was 11.1% (2.4% to 19.8%) of this total effect and 0.5% (−2.8 to 4.0) was the mediation effect of economic position. Similarly, a one unit increase in the social position score was associated with a 14.3% (4.7% to 25.8%) and 9.8% (3.9% to 14.6%) increase in the probability of formal health provider and private provider use, respectively. The mediation effects of economic position in these total effects were 2.6% (1.3% to 6.8%) and 2.2% (0.2% to 5.5%) for formal health provider and private provider, respectively. Social position in contrast was negatively associated with public provider use. A one unit increase in the social position score was associated with a total 9.9% (3.4% to 14.8%) decrease in the probability of public provider use and 2.3% (0.0% to 5.4%) of it was mediated by economic position. Among children with ARI, neither social position nor economic position was significantly associated with health-seeking behaviours.
Mediation analysis of social and economic position on health-seeking behaviour for under-5 children with diarrhoea and ARI in Myanmar
Discussion
This study is the first analysis of parental health-seeking for diarrhoea and ARI based on the nationally representative 2015–2016 Myanmar DHS data. The associations between parental social position and economic position with health-seeking behaviours (seeking treatment, receiving treatment from formal health provider and receiving treatment from public or private provider) were examined for diarrhoea and ARI among under-5 children in Myanmar. This study showed that higher social position and economic position were positively associated with seeking treatment and private health provider use for diarrhoea. Social position had more influence than economic position on parental health-seeking behaviour for children with diarrhoea. There was no evidence of associations between social and economic positions with parental health-seeking behaviour for children with ARI.
Our study found that the higher the social position, the more likely to pursue desirable health-seeking behaviour. Similarly, studies in sub-Saharan Africa and India also indicated an association between low parental education and low health-seeking behaviour for childhood diarrhoea diseases.11 14 15 29 Women with higher education are more likely to use health services than uneducated women.30 31 Mother’s education level can be associated with an increased awareness of childhood illnesses and symptoms, and ability to timely interact with healthcare services.29–31 Thus, investment in education may result in better access to health information for appropriate health-seeking behaviours.
Our study showed that the children from households with higher economic position were more likely to be taken to a private rather than a public provider for treatment. The findings can be explained by high capability to cope with the cost of care among the households with higher economic position. A significant predictor of health-seeking behaviour for childhood illness is the household wealth status and lack of financial resources can create barriers to access healthcare services.11 15 17
Our study found that children from rural areas with either illness were less likely to be taken to private providers for treatment. This can be explained by the availability and quality of private health facilities in rural area. In urban areas, there was one medical doctor per 633 000 population, while, in rural areas there was one per 3 447 000 population in 2015–2016 in Myanmar.32 The healthcare professionals from public facilities (both urban and rural) also practice in private clinic. But the availability and quality of services from private health facilities are higher in urban than rural.32 Under the integrated Global Action Plan for Pneumonia and Diarrhea, nationwide interventions such as facility-based integrated management of neonatal and childhood illnesses (F-IMNCI) and community case management (CCM) of diarrhoea and ARI are being implemented in Myanmar.33 These interventions provide early diagnosis and prompt treatment with effective drugs to reduce morbidity and mortality due to these illnesses in under-5 children in Myanmar.33 Although essential child health services are provided free of charge in Myanmar, additional costs related to transportation and medication might be a challenge for household’s capacity to pay.3 4 7 However, private providers were more likely to be approached by families of children with more severe illness, regardless of social and economic position. This indicates the population’s preference for timeliness of receiving health services over cost. The monitoring report of the F-IMCI and CCM also found interventions covered <15% of the expected cases.33 34 This emphasises the need for improvement of these interventions to increase care-seeking behaviours favouring public providers.
Our study showed that appropriate parental health-seeking behaviours—‘seeking treatment’, ‘formal health provider’, ‘public provider’ and ‘private provider’—were mainly attributed to the direct effects of social position rather than through a mediation effect of economic position. This clearly indicates that the social position (education, literacy and occupation) have more influence on health-seeking behaviours than the economic position. Investing in education would likely be a promising investment to achieve desirable health-seeking behaviours. This should be accompanied by improving the quality of health services among public providers.
In our study, health-seeking behaviour for ARI was not associated with either social or economic position. WHO and UNICEF joint report on F-IMNCI stated that, nearly one-third of ARI children were not taken to an appropriate provider.34 However, our study identified that when the child develops fever or becomes sicker, parental health-seeking improved. It may be related to the perceived vulnerability of the child and/or severity of illness.11 14 15
Strengths and limitations
This is the first nationwide study in Myanmar to examine the association between appropriate health-seeking behaviour with social position and economic position using adjusted analytical methods. Including mediation analysis enabled understanding the relative importance of the influence of social or economic position, rather than combined socioeconomic status, on parental health-seeking behaviour outcomes. However, this study has some limitations. First, our conceptual mediation framework did not consider possible reverse causality from economic position to social position. However, based on the associations of social and economic position with health-seeking behaviours for diarrhoea, the association of social position with health-seeking behaviour was stronger than that of economic position. Second, social and economic position (the two latent variables) were created from observed indicators in the sampled households with female respondents of reproductive age because the MDHS did not collect data for those children whose mother was not alive or not living in the same household.13 Therefore, this study only considered the children whose mothers were in this group and were alive. In Myanmar, reliable data on the children without living mothers are lacking, but it is likely that those children are more susceptible to illness and also have more barriers to get access to appropriate health services.11 Third, the main outcomes in this study depended on child illness and health-seeking actions reported by mothers. The perception and accurate recall of illness among young children may have some responder bias.11 Lastly, this study may have social desirability bias, a tendency of MDHS survey respondents (mothers) to answer questions in a manner that will be viewed favourably by others. Unfortunately, there was no data available to address this bias in the study.
Conclusion
Although both social and economic position were determinants of parental health-seeking behaviour for diarrhoea, social position had more influence than economic position. Moreover, mediation effect of economic position on social position in parental health-seeking behaviour for diarrhoeal was minimal. Understanding of socioeconomic gradients in health-seeking behaviour may simultaneously help to address socioeconomic disparities and reduce the burden of preventable deaths from diarrhoea among under-5 children in Myanmar. Further studies are needed to elaborate on parental health-seeking behaviour for ARI since there was no observed evidence for a significant association of social and economic position with health-seeking for ARI. Policy interventions targeting social position, such as awareness through mass media campaign, are promising to achieve appropriate parental health-seeking behaviour for under-5 children. Formal private healthcare provider has great potential for successful implementation to improve child health. Health policies should explore integrated public-private services to successfully address childhood illnesses.
Acknowledgments
The authors would like to thank Dr Eiko Saito, Dr Md. Mizanur Rahman, Dr Khin Thet Swe and Dr Su Myat Han for giving the utmost assistance and valuable suggestions.
Footnotes
Contributors All authors conceived and designed the study, and take responsibility for the accuracy of the data analysis. KSL, SN, DY, PU, SKA and KS analysed and interpreted the data. KSL conducted statistical analysis and drafted the article. All authors made the critical revision of the manuscript for important intellectual content and gave final approval for the manuscript.
Funding Ministry of Education, Culture, Sports, Science and Technology of Japan.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval for this study was not required as the data were extracted from the MDHS, which did not contain any personally identifiable information.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.