Article Text

Abstract
Objective To estimate the impact of using the Aptima messenger RNA (mRNA) high-risk human papilloma virus (HR-HPV) assay versus a DNA HR-HPV assay in a primary HPV cervical screening programme.
Design One hypothetical cohort followed for 3 years through HPV primary cervical screening.
Setting England.
Participants A hypothetical cohort of women aged 25–65 years tested in the National Health Service (NHS) Cervical Screening Programme (CSP) for first call or routine recall testing.
Methods A decision tree parameterised with data from the CSP (2017/18) and the HORIZON study. Uncertainty analyses were conducted using data from the FOCAL and GAST studies, other DNA HPV tests in addition to one-way and probabilistic sensitivity and scenarios analyses, to test the robustness of results.
Interventions Aptima mRNA HR-HPV assay and a DNA HR-HPV assay (cobas 4800 HPV assay).
Main outcome measures Primary: total colposcopies and total costs for the cohort. Secondary: total HPV and cytology tests, number lost to follow-up.
Results At baseline for a population of 2.25 million women, an estimated £15.4 million (95% credibility intervals (CI) £6.5 to 24.1 million) could be saved and 28 009 (95% CI 27 499 to 28 527) unnecessary colposcopies averted if Aptima mRNA assays are used instead of a DNA assay, with 90 605 fewer unnecessary HR-HPV and 253 477 cytology tests performed. These savings are due to a lower number of HPV positive samples in the mRNA arm. When data from other primary HPV screening trials were compared, results indicated that using the Aptima mRNA assay generated cost savings and reduced testing in every scenario.
Conclusion Using the Aptima mRNA assay versus a DNA assay would almost certainly yield cost savings and reduce unnecessary testing and procedures, benefiting the NHS and women in the CSP.
- colposcopy
- health economics
- gynaecological oncology
- microbiology
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The first analysis of the estimated impact of using a messenger RNA (mRNA) versus DNA high-risk human papilloma virus (HPV) assay for primary HPV screening globally, in terms of the healthcare resources used and associated costs.
Extensive sensitivity analyses generated understanding around the robustness of the results, and the impact of certain parameters on the results (particularly HPV positivity).
Comprehensive scenario analyses ensure that the full range of possible results are explored.
A lack of data on DNA versus mRNA test results from the English primary screening programme means that data from trials in other countries are used and it is unknown which trial population best reflects that in England on which to base the model inputs.
No study has collected a complete set of recall data at 12 and 24 months, as will be seen in the English programme, therefore these simulated results will need to be validated once the programme has been fully rolled out.
Introduction
Cervical cancer screening can identify precancerous cervical abnormalities such as cervical intra-epithelial neoplasia (CIN), allowing for earlier treatment. Cervical screening has a large impact on cervical cancer prevention, therefore many developed countries have established national screening programmes.1 Genital infection with human papillomavirus (HPV) causes most cervical cancer cases.2 In the vast majority of cases, HPV infection is transient, asymptomatic and spontaneously cleared; however, persistent infection with defined high-risk (HR) HPV types in women increases the risk of developing cervical abnormalities.3
The English National Health Service (NHS) cervical screening programme (CSP) started to implement a new algorithm in March 2019, with full roll out expected in early 2020. Samples switched from being tested with cytology followed by HPV triage for certain groups of abnormal cytology samples, to primary HR-HPV testing with reflex cytology for positives. A number of recent studies have shown that primary HR-HPV screening detects persistent high-grade CIN earlier than primary cytology screening.4
Two types of HR-HPV assays are currently used in primary HPV screening programmes; DNA and messenger RNA (mRNA) tests. A positive HR-HPV DNA test indicates the presence of DNA above certain concentration in cervical cells.5 However, as HPV infection is often transient and can be spontaneously cleared, the presence of this DNA does not necessarily indicate that a precancerous abnormality will develop.6 The presence of HR-HPV E6/E7 mRNA in cervical cells has been shown to more accurately detect those at risk of developing CIN, and therefore at more at risk of developing cervical cancer, than the presence of HPV DNA.5 7
The Aptima HR-HPV mRNA assay and DNA HR-HPV assays both have high sensitivity in the detection of CIN. Non-inferiority criteria for HPV assays have been established that require assays to detect similar numbers of CIN2+ and false-positive tests as assays that have been validated in randomised controlled trials.4 8 Using these criteria, assays such as Aptima and the family of cobas tests have been validated for the purpose of primary cervical screening.9–11 Aptima also performed similarly in other cross-sectional and longitudinal studies with no significant difference in sensitivity found.12–18 However, the Aptima mRNA assay is more specific than DNA HPV assays,19 as it detects actively transcribing infections, as opposed to transient infections. Accepting that the use of Aptima mRNA over DNA HPV testing would result in fewer HPV positive tests in women that do not have CIN2+ (false-positive tests) the number of women progressing through the screening algorithm due to these false positives could be reduced, resulting in fewer reflex cytology tests, colposcopies and recall testing after 12 months. The reduction of those unnecessary tests could subsequently save costs in the screening programme and avoid women undergoing unnecessary testing and procedures.
As the HR-HPV primary screening data from the English pilot screening programme did not record the type of HR-HPV test used,20 this study aims to model the use of the Aptima mRNA HR-HPV assay compared with a DNA HR-HPV assay in primary HPV screening for women in the English CSP. Sensitivity and scenario analyses are conducted to determine the impact of parameters and assumptions on the model.
Methods
Cervical screening algorithm
In England, women are invited for their first cervical cancer screening at the age of 25 and are recalled every 3 years until age 50 years if test results are normal. From ages 50 to 64, they are recalled for screening every 5 years. In the primary HPV screening algorithm,21 a cervical sample is taken, preserved in sample media (SurePath or ThinPrep) and sent to the lab for processing. First, the sample is tested for HR-HPV. Women with negative results are discharged to routine recall; positive HPV samples are then tested using liquid based cytology (LBC) to assess any cell changes. Women with normal cytology results are recalled in 1 year for follow-up (HPV with reflex cytology); while those with abnormal cytology are referred to colposcopy. Women who attend recall in year two follow the same pathway as in year one. In year three, all women with HPV positive samples are directly referred to colposcopy (cytology is performed but does not influence referral to colposcopy). There is no requirement for HPV genotyping in England.22 23 The full screening algorithm is shown in figure 1.
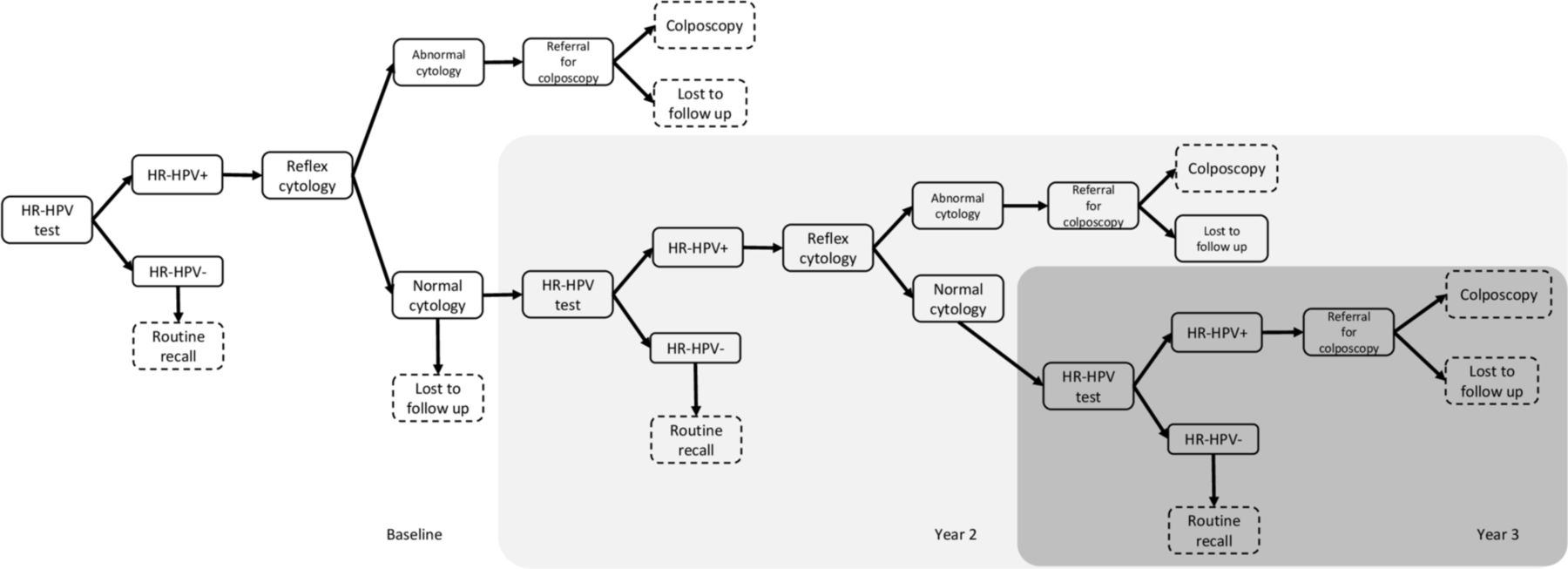
Structure of the decision tree model to simulate primary HR-HPV cervical screening in England; this structure was identical for both the mRNA and DNA testing arms. HR-HPV, high-risk human papilloma virus; mRNA, messenger RNA.
Abbott RealTime High-Risk HPV test, BD Onclarity, Cepheid Xpert, Hologic Aptima, Qiagen Hybrid Capture 2 (HC2) and Roche cobas 4800 and 6800/8800 tests are all approved for HPV primary screening in England, and regions may procure whatever test they want from the approved list.
Model type and structure
This cost-consequence analysis simulated the English HPV primary screening algorithm that is currently being rolled out using a decision tree model constructed in TreeAge Pro 2018. A cost-consequence analysis was chosen as it will be most meaningful to decision makers to understand the short-term direct impact on women and services, and due to the short-term nature of these pathways, estimating the incremental cost-effectiveness ratio (ICER) is not necessarily the most suitable measure. As it was assumed that there was no difference in the diagnosis using colposcopy and management of true positive patients in the two arms (mRNA and DNA) due to equally sensitive tests,7 12–18 therefore, there was no need to model the longer-term progression of the disease and outcomes over time. It followed one cohort of women through screening over 3 years from baseline screen through two potential follow-up recall visits. The endpoint for women in the model was either discharge to routine recall (because of a normal result), referral to colposcopy, or loss to follow-up (LTF). Test of cure (TOC) was excluded from the model, allowing for a conservative estimate of the impact of testing.
The model simulated women aged 25–64 years who were tested (either first call or routine recall) in the CSP.24 Women who were tested due to previous abnormality, inadequate sample or who were screened outside of the programme were not included. Inadequate results were not explicitly modelled as the model assumed that all those who had an inadequate sample (ie, the prepared slide is considered inadequate for an HPV test) would have another sample collected and therefore, an adequate test result. This may underestimate the total cost of screening activities as it does not include the cost of retesting due to inadequate test results. However, this is probably of minor importance as the proportion of inadequate samples is very low (estimated at 0.3% in the English pilot).20
The model structure was the same for the two arms: mRNA and DNA, and all women were assumed to have either all mRNA or all DNA tests over the 3-year model (figure 1). As all women would have completed the screening round within 3 years, a longer time horizon was not needed, even if the interval between routine recall was longer (eg, 5 years in women aged over 50 years). mRNA assays referred to in this paper are assumed to be the Aptima HR-HPV assay, and in the basecase the DNA assay is the cobas 4800 HPV assay. A newer cobas system (cobas 6800) is now commercially available and has been approved for use in the English CSP. The literature, however, suggests a similar performance in terms of non-inferiority of screening outcomes between the different cobas versions.9 25 The model was audited internally.
The study takes the perspective of NHS England. England does not follow the European guidelines for HPV primary cervical cancer screening, which recommends that it should not start before age 30.26
Patient and public involvement
No patients were involved in the design, or conduct, or reporting, or dissemination plans of this research.
Outcomes
The primary outcomes are the total cost of the screening programme for each arm and the number of colposcopies. The secondary outcomes are the number of HR-HPV and cytology tests and the number of women LTF. LTF occurs when women who are referred to colposcopy, or are recalled at years 2 and 3 for screening, do not attend. The cost outcome was reported separately from other outcomes as this is not a cost-effectiveness analysis. The difference between the outcomes in the two arms over the 3 years was calculated; a negative value indicates either cost-savings or fewer tests/procedures in the mRNA versus DNA arm.
Population
The model simulated a cohort of 2 247 439 representing the number of women tested in the NHS CSP in 2017–2018 (aged 25–64) (table 1).24 In the last 5 years, the number of women tested (first call and routine recall), has varied between 3.74 million and 2.18 million, however as there is no discernible trend in attendance the most recent available data was used. Probabilities from the HORIZON study were reported separately for ages 25–29 and 30–64, and therefore the model probabilities were age weighted to represent the age distribution of women in the CSP, as the prevalence of HPV varies by age.
Baseline model input parameters and the high and low values for each parameter used in the one-way sensitivity analysis (DSA)
Cost inputs
All costs (British Pounds) were inflated to 2016/2017 values using published inflation rates from the Personal Social Services Research Unit (PSSRU) (the most recent PSSRU values at time of writing).27 A micro-costing approach was taken to estimate the costs for screening in England; these were validated by clinicians. The cost of both mRNA and DNA tests included the initial costs for collecting and processing the sample (staff time, test kit and consumables, transport to the lab and results letter) as well as the test itself (including all reagents and other lab costs). The costs of the mRNA and DNA tests were assumed to be the same as there are no published data to suggest otherwise and they have the same level of automation. Published values from the literature were used for the cost of LBC.28
The cost of a colposcopy was calculated by weighting the cost of a colposcopy with a biopsy with the cost of a colposcopy without a biopsy, based on 2017/18 CSP data (percent of diagnostic biopsies out of total referrals) and the NHS National Tariff costs.29
A discount rate of 3.5% was applied to costs in the model, in line with the National Institute for Health and Care Excellence (NICE) guidelines.30
Treatment costs were not included in the model as due to the similar sensitivities of the tests modelled, similar numbers of cases of CIN/cervical glandular intra-epithelial neoplasia (CGIN) are expected to be seen at colposcopy, and therefore the number of treatments required would be similar.
Probability inputs
The primary HPV screening pilot in England did not record the type of HPV test used.20 As there is no gold standard for the detection of HPV, the model could not adopt a traditional structure that uses HPV prevalence and test performances, as any prevalence data would be influenced by the type of test used. Therefore, a comprehensive targeted literature review was conducted to identify the most representative, complete datasets with the data required for the model. This included contacting the study authors to request the data required for the model if it was not published in the format required for the model. Four studies were found that contained head to head data comparing the mRNA to DNA HR-HPV test in a primary screening manner: CERVIVA from Ireland,31 German AHPV Screening Trial (GAST) from Germany,15 FOCAL from Canada,14 and HORIZON from Denmark.32 33 The CERVIVA trial is ongoing and has not yet published baseline data; hence was not considered further. FOCAL data could not be used in the baseline model as the study referred to colposcopy any women that was HC2 positive or had abnormal cytology at baseline, and therefore the follow-up population did not mirror the English algorithm. Furthermore the follow-up period was 48 months, which makes an estimation of 12-month follow-up data less accurate. GAST only included women aged over 30 years, which would not be representative of the English population as HR-HPV positivity is significantly higher in women aged 25–29 years.34
The HORIZON study tested 4128 women for HPV and LBC in a primary screening algorithm in Denmark (full description in online supplementary information S1). The study collected the samples using SurePath, and samples were tested on four HR-HPV assays: Hologic Aptima HPV Test; Qiagen Hybrid Capture 2; Roche cobas 4800 HPV Test; and CLART HPV2 Assay. The CLART results were excluded from this model as the CLART assay detects a number of low-risk HPV genotypes in addition to the HR-HPV genotypes, and is not accepted for use in the CSP.35 36 The probabilities for the DNA arm were taken from the cobas 4800 HPV assay results from the HORIZON trial, as currently no laboratories in England use the HC2 test and the model aimed to reflect the current screening situation in England. The HORIZON results from HC2 were run through the model separately as a scenario analysis.37 Women with a positive HPV test and negative cytology were followed-up at 18 months and tested for HPV and then cytology reflex. In HORIZON, the follow-up cytology data was aggregated for all tests, therefore reflex cytology abnormal cases were assumed to be HPV positive in all HPV tests due to the high sensitivity of the HPV tests and as HPV+ concordance in cytology-abnormal women was not reported in HORIZON. As follow-up in England is at 12 months, HORIZON follow-up data was transformed into a rate, and then back into a probability to estimate the probability of testing positive at 12 and 24 months. The trend for persistence over time was assumed to be linear.38–40 See table 1 for baseline probabilities used in the model; additional data from HORIZON are shown in online supplementary information S2–S4.
Supplemental material
The positivity seen in the HORIZON trial was 20.2% and 12.3% when DNA and mRNA HPV tests were used respectively in women aged 23–65 years.32 33 The positivity seen in the English pilot screening programme, where women were screened between the ages of 25 and 64, was lower but still comparable at 12.7% (using a mix of DNA and mRNA tests, the breakdown is unknown).20 Furthermore, in order to determine the impact the positivity has on the results, extensive sensitivity and scenario analysis were carried out as outlined below, using data from other tests and trials (GAST and FOCAL) with lower positivity rates.
Uncertainty analyses
One-way analyses
One-way sensitivity analyses were carried out to determine the effect that changes in individual parameters had on the outcomes. The model was run selecting the high and low parameter values (table 1). Probabilities were varied by 25% of their baseline values. The costs were varied by values in the literature, except for the cost of the HR-HPV test (mRNA and DNA) which was varied between £10 and £20 based on discussions with experts. The low value for LTF was set at 0 to represent perfect compliance. The impact on costs and number of colposcopies are presented in a tornado graph, showing the difference in outcomes between mRNA and DNA testing.
Probabilistic sensitivity analysis
A probabilistic sensitivity analysis (PSA) was conducted to look at the robustness of results given a wide range of plausible inputs. Each input parameter was assigned a distribution based on data from the literature or an estimated distribution (online supplementary information S5 and S6). All probabilities were assigned a beta distribution to limit the values to between 0 and 1, with the alpha and beta values derived from the published data. For costs, a gamma distribution was assigned and the costs were varied by 20% to estimate the SD.
A Monte Carlo simulation was run using 1000 iterations of the model, with each run independently sampling from the distributions. For each iteration, all inputs that the mRNA and DNA arms shared were assigned the same value; all other inputs varied independently in the mRNA and DNA arms. This allows the difference in outcomes for each iteration using mRNA and DNA to be compared. The difference in the outcomes between DNA and mRNA testing were estimated, and these were used to estimate the 95% credibility intervals (CI).
Scenario analyses
We explored the impact of changing assumptions in the model as part of the scenario analyses.
The model was run using only the HC2 results from HORIZON to see the impact of the different test performance on the model results (online supplementary information S3).
As it is not known which dataset will be most similar to the English population, a number of scenarios were run using different datasets and the outputs compared.
Both FOCAL and GAST data were used in scenario analyses to estimate the outcomes that might be seen in England if only the year one screening data were used. A description of the FOCAL and GAST studies is in online supplementary information S7. Results from the GAST study were made available by one of the authors (TI), and the model was re-run using probabilities calculated from the GAST data, which was for a cohort of women aged 30–60 years tested using HC2 (online supplementary information S6). This was compared with results from the model using the equivalent population from the HORIZON study (data for women aged 30–64 years tested using HC2).
The HC2 test results in the HORIZON study showed a lower positivity than the averaged cobas and HC2 results, therefore the model was rerun using only the HC2 results for the DNA arm and compared with the mRNA arm results (online supplementary information S8). This positivity is very similar to the positivity recorded in the English primary screening pilot programme (15% and 12.3% in DNA and mRNA respectively, and 12.7% in the English pilot using a mix of tests),20 32 33 so it is expected that this iteration of the population would closely mirror the population in the English CSP.
Primary and secondary outcomes were also compared using the data from the FOCAL, HORIZON and GAST studies for year one for the mRNA and DNA testing arms (online supplementary information S9). The positivity seen in these trials were considerably lower than the positivity in the English programme (GAST: 6.1% and 4.9%, FOCAL: 9.4% and 8.1% for DNA vs mRNA, respectively).14 15
Results
Baseline results
The primary and secondary outcomes for the baseline model are shown in table 2. In the population of 2.25 million women in the NHS CSP programme, using an mRNA versus DNA test saved an estimated £15.4 million, averted an estimated 28 009 unnecessary colposcopies, 90 605 unnecessary HR-HPV tests and 253 477 unnecessary cytology tests. There were also 9536 fewer women LTF for their colposcopy referral, and 114 988 fewer women LTF for HPV recall in years 2 and 3 for mRNA versus DNA testing (online supplementary information S10).
The baseline results for the primary and secondary outcomes: total costs, and number of colposcopies, HR-HPV and cytology tests using an mRNA or DNA assay
The cost of HPV testing comprised the greatest proportion of the total costs: £71.7 million (76%)—mRNA versus £74.4 (68%)—DNA. A higher percentage of costs come from recall activities in the DNA arm, due to the higher initial HPV positivity. Colposcopy accounted for 11.6% (mRNA) and 19.9% (DNA), and cytology tests 12.2% (mRNA) and 18.1% (DNA) of the total costs, respectively.
One-way sensitivity analysis
The impact that varying each parameter has on the outcomes is shown in online supplementary information S11. Varying the costs of the HPV assays had the largest impact on the cost difference between the mRNA and DNA arm. Even using a low value of £10 for a DNA HPV assay, cost savings of £2.18 million were realised. Assuming perfect compliance for HPV recall testing had the largest impact on the number of colposcopies (67 041 fewer colposcopies when mRNA assay was used), however probability of a positive HPV test in year 1 also had a relatively large impact, with 21 030 fewer colposcopies in the mRNA arm when the low value was used (compared with a difference of 28 009 colposcopies at baseline).
Probabilistic sensitivity analysis
Results from the PSA are given in figure 2. For a mean difference in costs of £15.4 million, the 95% CI showed a range of £6.5 million—24.1 million. The 95% CI for the reduction in the number of colposcopies was 27 499–28 527. In 0.1% of iterations of the model the DNA arm is cost saving compared with the mRNA arm. There are no instances in which a strategy using DNA HR-HPV testing results in fewer colposcopies, HR-HV tests or LBC tests.

{kind=link}
{kind=link}
Results from the probabilistic sensitivity analysis, showing the difference between mRNA versus DNA over 1000 iterations. (A) difference in costs; (B) difference in colposcopies; (C) difference in HPV tests; (D) difference in cytology tests. HR-HPV, high-risk human papilloma virus; mRNA, messsenger RNA.
Scenario analysis
The full results for the scenario analyses are in online supplementary information S12–S14.
When the model was run using only HC2 results from the HORIZON study, £6.7 million saving and 18 426 fewer colposcopies were realised in the mRNA arm compared with the DNA arm (online supplementary information S12), which is less than the savings seen in the baseline results.
Compared with the results from the model using the GAST data, the HORIZON results showed a larger difference between the mRNA and DNA arms (online supplementary information S13). However, the GAST data still showed a £2.29 million saving over the 3-year model (compared with £5 million saving in the comparable HORIZON population) and 4803 fewer colposcopies (11 819 fewer colposcopies in the comparable HORIZON population).
Scenarios using data from all three trials for the first year only, always generated cost-savings and reductions in the number of unnecessary tests and procedures, and reduced LTF (online supplementary information S14). Both GAST and FOCAL data presented a smaller difference between the two arms, which is due to the significantly lower HR-HPV positivity for both DNA and RNA assays than in HORIZON. FOCAL and GAST data also showed variation in the difference between the two arms as FOCAL reported almost double the probability of abnormal cytology than GAST.
Discussion
Main findings
The baseline results of this model suggest that using the Aptima mRNA assay versus cobas 4800 HPV DNA assay in the new primary HPV screening algorithm in England is likely to result in a reduction in overall screening costs, unnecessary referral to colposcopy, unnecessary recall HR-HPV and cytology tests and reduced LTF. These reductions in resource use should not be associated with any subsequent reduction in identifying true positive women, as the sensitivity of the assays has consistently been shown to be similar.41 The results are robust across a range of inputs as shown by the one-way, PSA and scenario analyses. However, the exact magnitude of cost-savings and reduction in unnecessary resource use is unknown and additional data is needed from England.
Strengths and limitations
This is the first analysis to assess the impact of using the mRNA or DNA assays as part of HPV primary screening. These results can inform decision-makers as they plan for the organisation of screening in 2019 in England and may also apply to other countries. Although independent calibration data does not exist as results from the new algorithm in England are not available broken down by the test used, extensive uncertainty analyses indicated that the results are robust and consistently show that the use of the Aptima mRNA assay is favourable over using DNA assays for primary HPV screening. If results by type of test do become available, we recommend validating the results of the model. Furthermore, the newer cobas 6800 assay would decrease the hands on time needed to run the assay,25 which could decrease the cost of the assay. This is not reflected in this model, as the cobas 4800 assay is modelled, however the impact of a decreased DNA test price is modelled in the one way sensitivity analysis, with an extra cost of £2.18 million incurred with a £10 DNA test (compared with a cost of £15.43 for mRNA in the same iteration of the model).
As no data were available in England broken down by type of HPV test, data from the Danish HORIZON study were used. The HORIZON study followed women through their baseline screen and follow-up recall, following a similar testing algorithm and age range as will be employed in England. However, HORIZON displayed a higher absolute positivity rate (12%-mRNA, 20%-DNA) compared with FOCAL (8%-mRNA, 9%-DNA) and GAST (7%-mRNA, 9%-DNA) and the overall positivity in the English pilot programme (12.7%).20 32 33 Demographic characteristics of the women in the HORIZON, FOCAL and GAST trials may differ from what will be seen in England and the simulated population in the model, however without comparable data for England by test it is difficult to speculate. For example, the HORIZON study sampled a slightly younger and largely urban population with potentially an overall higher HPV positivity, while the GAST study did not include women under 30, which decreases the overall positivity.
In England, laboratories use either SurePath or ThinPrep media for sample collection. The collection media may have an impact on the number of samples that are identified as cytology abnormal or HPV positive.19 However, there is no conclusive evidence on the difference that the collection media could make when used in conjunction with mRNA versus DNA HR-HPV tests in a primary screening setting,42 so it is unclear how using the HORIZON data that used SurePath may impact on results.
Published data are not available for the head-to-head comparison of HR-HPV positivity in England using an mRNA and DNA assay, therefore it is unknown if HORIZON, GAST or FOCAL is most representative for England. Despite these differences, the results from scenarios using all datasets showed significant cost and resource savings when using mRNA HR-HPV testing.
TOC was not modelled as it is not considered part of the screening algorithm but part of the treatment pathway. As TOC would involve more women being referred for HPV, cytology and therefore colposcopy based on their HR-HPV results, it is thought that excluding TOC data provides a more conservative estimate of the impact of using mRNA versus DNA HR-HPV tests.
Interpretation
Previous studies estimated that primary HR-HPV testing with reflex cytology will be more expensive than cytology testing with HR-HPV triage and will result in an increase in colposcopies in the short term.34 The increase in colposcopies in the short term is thought to be because cytologists will be more cautious in their diagnosis as they become familiar with the new programme and due to the earlier diagnosis of women. If a more specific HR-HPV assay is used, the unnecessary referrals to colposcopy and the burden on laboratories for testing can be reduced, alleviating some of the short-term challenges introduced from the switch to HPV primary screening. Additionally, the relative cost of HPV-based screening compared with cytology screening will be balanced by introducing longer screening intervals after a negative HPV test.
As previously stated, both the Aptima and cobas tests are acceptable for use in screening programmes, and Aptima has non-inferior sensitivity.12–18 The Meijer criteria which define these use a sample cohort of 60 CIN2+ cases, further studies would need to be conducted to determine whether this remains the same in a much larger cohort. This model uses the assumption that the assays have an equal sensitivity and does not take into account the differences in targeting strategies or assay design that could affect the proportion of women correctly or incorrectly identified as HPV positive and subsequently referred to colposcopy. Therefore the relative performance of the assays within the primary screening programmes needs to be monitored in future studies.
As women in England who were vaccinated against HPV are just beginning to enter the CSP,43 it is unclear how this might impact on the burden of screening and referrals. A decrease in positive HR-HPV tests as more people are vaccinated has been observed in Scotland, Canada and Australia, all of which have similar vaccination programmes, and in studies modelling the expected impact in England.44–47 Future economic models on this subject should be informed by real life data on the impact of vaccination in England.
While this paper sought to model the impact on healthcare services alone, there is also expected to be an impact on women’s quality of life. Cervical screening and colposcopy can have a negative impact on women’s quality of life when they receive positive screening results or are referred to colposcopy.48 By choosing the most specific test, the NHS can reduce the unnecessary stress and anxiety in women associated with unnecessary tests for false positives with no trade off in detecting CIN given that mRNA assays are as sensitive as DNA assays.19
Conclusion
Overall, results from the model suggest that using the Aptima mRNA HR-HPV assay is less expensive and avoids unnecessary HPV recall testing, cytology testing and colposcopies than using a DNA HR-HPV assay in the new primary HPV screening algorithm that was started to be introduced in England in March 2019. Extensive uncertainty analyses demonstrate that cost and resource savings will almost certainly be achieved despite using different data sources.
Acknowledgments
The authors would like to thank Matejka Rebolj for useful input on the HORIZON data used in this analysis, Alex Castanon for providing the raw GAST data and the authors of the FOCAL study for data and discussions.
References
Footnotes
Twitter @aquariusph
Contributors EJA designed the study and oversaw the project, MJH and GW constructed the model, GW ran the analyses and drafted the paper, CD identified data for the model and helped draft the paper, CF, MK and TI provided input on the analysis, helped interpret results and reviewed the article. TI also provided the raw data from the GAST study.
Funding Aquarius Population Health received funding from Hologic for this study; the design, results and interpretation of the study are independent and the authors’ own.
Competing interests EJA, GW, MJH and CD report grants from Hologic to their Employer (Aquarius Population Health) during the conduct of the study, and grants on diagnostics from Cepheid, Enigma Diagnostics, Jupiter Diagnostics, Binx, Momentum Bioscience, St Georges University of London, BIVDA and Roche Diagnostics, outside the submitted work. TI reports grants from Hologic and from Becton Dickinson, outside the submitted work to his institution (University Hospital Tuebingen) and personal speaker honoraria from Hologic Inc during the conduct of the study. MK received grants from Welcome Trust, NIHR, Genesis Trust, Imperial BRC, Imperial Charity outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data used in this study is already in the public domain.