Article Text

Abstract
Objectives To assess delays to antiretroviral therapy (ART) initiation before and after the Universal Test and Treat (UTT) and the same-day initiation (SDI) of ART policy periods in Johannesburg, South Africa.
Design Prospective cohort study.
Setting Patients were recruited from six primary health clinics in Johannesburg.
Participants Overall, 1029 newly diagnosed HIV positive adults (≥18 years) were consecutively enrolled by referral from the testing counsellor between April and December 2015 (pre-UTT n=146), July and August 2017 (UTT, n=141) and October 2017 and August 2018 (SDI, n=742).
Main outcome measures Cox proportional hazards regression was used to assess predictors of 30 days ART initiation. Additionally, predictors of immediate ART initiation were evaluated using Poisson regression.
Results Overall, 30 days ART proportions were 71.9% overall, 36.9% pre-UTT (44.3% of those eligible), 65.9% under UTT and 79.9% under the SDI policy. The median days to ART initiation declined from 21 pre-UTT (IQR: 15–30) to 8 (IQR: 6–16) under UTT and 5 days (IQR: 0–8) under the SDI policy. However, only 150 (20.2%) of the SDI cohort-initiated ART immediately after HIV diagnosis. Living in a two-adult home (adjusted HR (aHR) 1.2 vs living alone, 95% CI 1.0 to 1.5) increased the likelihood of 30-day ART. Missing baseline cluster of differentiation four (CD4) data decreased the likelihood of 30 days ART by 40% (aHR 0.6 vs CD4 <350 cells/µL, 95% CI 0.5 to 0.7). More women took up immediate ART (adjusted relative risk (aRR) 1.3, 95% CI 1.0 to 1.9). Participants ≥40 years (aRR 0.6 vs 18–24 years, 95% CI 0.4 to 0.9) were less likely to start ART immediately after HIV diagnosis. However, immediate ART rates increased with longer policy implementation time (aRR 0.2 for <3 months vs >10 months, 95% CI 0.1 to 0.4).
Conclusions The study results highlight a positive move towards earlier ART initiation during the UTT and SDI periods and emphasise a need to increase same-day ART implementation further.
- HIV & AIDS
- public health
- primary care
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Cohorts enrolled across the three most recent antiretroviral therapy (ART) guideline implementation periods in South Africa, allowing observation of changes over time.
Participants were enrolled immediately after HIV diagnosis, allowing for observation of ART initiation and patient attrition from HIV diagnosis over time.
The results highlight a positive move towards earlier initiation of HIV treatment after the Universal Test and Treat policy implementation.
Although we demonstrate substantial reductions in delays to ART initiation (median of 21 to 5 days), ART initiation on the day of HIV diagnosis is limited and requires additional investigations to improve programmatic performance.
Increases in missing baseline laboratory tests at diagnosis reduce the strength of laboratory datasets as monitoring tools for the early steps of the HIV treatment cascade and delay the assessment of the appropriateness of the initial ART regiment.
Introduction
South Africa has the largest HIV epidemic in the world, with an estimated 7.9 million persons living with HIV.1 Over the years, the South African government gradually increased the cluster of differentiation four (CD4)-based antiretroviral therapy (ART) eligibility threshold from 200 cells/µL in 2004 to 350 cells/µL in 2010 and 500 cells/µL in January 2015.2–6 These thresholds both capped the number of persons initiating ART and negatively affected the retention of pre-ART patients. In the past, attrition from care after HIV diagnosis was also related to the number of assessment and counselling visits required before treatment initiation for eligible patients and the lack of systematic monitoring of and benefits for patients who were not offered ART.2–7 Additional pre-ART determinants of losses from the HIV treatment cascade include gender, the requirement for a treatment buddy/disclosure for ART initiation, HIV stigma and the high cost of attending clinic visits.7–14
In September 2016, South Africa removed the CD4 cell count threshold for ART eligibility and adopted the WHO 2015 Universal Test and Treat (UTT) policy, making all HIV positive patients eligible for ART at diagnosis.15–17 Clinical trials showed that, compared with patients who deferred ART, patients who started treatment immediately after HIV diagnosis had lower rates of AIDS-related adverse events and improved viral suppression rates with no difference in post-initiation attrition rates.18–21 Moreover, patients who started ART immediately after diagnosis were less likely to transmit HIV than patients who deferred ART.16 19 21 22
In September 2017, the general UTT policy was updated with a directive to initiate ART on the day of HIV diagnosis (same-day initiation—SDI).23 While widespread support for the UTT policy has created momentum for its promulgation, there remained reservations from primary healthcare (PHC) providers that health system capacity constraints may limit same-day ART policy assimilation and result in variations in implementation at facility-level.24 The policy was implemented amid concerns that, under UTT, health facilities in high burden settings, in particular, might struggle with the increased patient burden, potentially reducing the quality of care provided to new and existing patients.2–4 25 26 There were also concerns around patient acceptance of same-day ART, ART refusal and early patient disengagement from care or intermittent adherence after starting ART.27
In 2017, an estimated 4.4 million (55.7%) South African HIV-positive patients had started ART.1 While this constituted a major increase in the number of HIV positive patients initiated on ART (nearly 1 million additional patients started ART between 2016 and 2017), the proportions also suggested continued challenges with patient linkage to ART after HIV diagnosis.1 Furthermore, in addition to measuring programme success in terms of expanded access to ART, critical outcomes of the UTT policy include the initiation of patients with high CD4 (>500) count, reductions in delays to ART initiation and long-term retention in HIV care.
In this study, we set out to measure ART initiation of newly HIV diagnosed adults in the first 30 days of HIV care (30-day ART) across the three recent ART guideline periods and examine factors associated with 30 days ART at six clinics in Johannesburg, South Africa. Additionally, we examined rates and predictors of initiating ART on the day of HIV diagnosis among patients diagnosed under the SDI policy.
Methods
Study setting and design
The city of Johannesburg is the largest of five health districts in the Gauteng province in South Africa. Johannesburg had an estimated HIV prevalence of 12.9% (>500 000 persons living with HIV) in 2017, with 60.7% of diagnosed persons currently receiving ART. Johannesburg comprises 108 PHCs subdivided into seven regions or subdistricts (denoted A-G) covering about 75% of the population (mainly uninsured). This study was conducted at six (of 13) conveniently selected public-sector PHCs in the Johannesburg health subdistrict A. PHCs in Johannesburg are mainly nurse-run with the support of one medical doctor and are responsible for HIV testing, ART initiation and primary-level management and monitoring of HIV positive patients.
We conducted a prospective cohort study, enrolling consenting newly diagnosed HIV positive adult (≥18 years) patients from April to December 2015 (CD4 <500 or pre-UTT period), July to August 2017 (UTT period) and October 2017 to August 2018 (SDI period) (summarised in table 1). Pre-UTT and UTT cohorts were only enrolled from two PHCs in Johannesburg while the SDI cohort included four additional PHCs serving similar populations in the same area in Johannesburg (table 2).11–14
Description of ART guideline changes over time in South Africa
Characteristics of the sample population by period of HIV testing
Participant enrolment co-occurred across sites until 100% sample size was attained at each site (figure 1). All patients were enrolled in the study after a new (self-reported) HIV-positive diagnosis (before ART eligibility determination) by trained study interviewers via referral from PHC-based lay HIV counsellors. We included newly diagnosed adult patients (18 years or older) who were able to speak English, Zulu and Sotho. Patients were eligible if they had entered HIV care after an HIV-positive diagnosis. Entering HIV care was defined as providing the first blood sample for baseline safety laboratory tests for the pre-UTT and UTT cohorts, and defined as having received the HIV positive test result for the same-day ART cohort because new clinic processes meant that patients were likely to start ART before the first blood collection. The first blood tests were necessary to determine patients’ CD4 count eligibility for ART and the appropriate initial ART regiment, hence the term ‘safety bloods’. Women who were pregnant at HIV diagnosis were excluded from the study because ART initiation and monitoring processes in antenatal care differ from that of non-pregnant populations. Study staff cooperated closely with lay HIV counsellors across sites and checked HIV testing records daily to ensure that all testers who were diagnosed with HIV were being referred to study staff for study eligibility assessment.

Participants flow from screening to ART initiation in the first 30 days of care by art policy periods. ART, antiretroviral therapy; UTT, Universal Test and Treat.
Study sample size
We assumed that 70% of HIV positive patients with CD4 counts >350 cells/µL would become lost from HIV care in the first year after HIV diagnosis compared with 60% among patients with CD4 ≤350.28 29 We further hypothesised a 20% reduction in overall attrition between the pre-UTT and UTT periods. Additionally, the sample size for the SDI cohort was increased to enable a separate assessment of ART refusal (hypothesised 20% refusal by 6-month post-HIV diagnosis) and attrition among participants who initiate ART with high CD4 count (>500 cells/µL).30 The ART refusal analysis will be presented in future manuscripts. The number of sites was also increased to six to allow comparison of the same-day ART across clinics.
Data collection
Patients provided written consent for all study procedures and completed an interviewer-administered baseline questionnaire after HIV testing, on the day of HIV diagnosis. Additionally, participants were assured that participation in the study would in no way amend the care that they received at the clinic, including their future schedule of visits at the clinic. The consent process and interviews were conducted exclusively in English in the pre-UTT cohort because we assumed that the urban Johannesburg population would be conversant in English but later translated to Sotho and Zulu as well for the UTT and SDI cohorts. The interview included questions on demographic factors, socioeconomic status and health-seeking behaviour. The recency of the HIV diagnosis was determined from HIV testing history questions at baseline. Patients were passively followed up by paper and electronic (including laboratory data) medical record review up to 30 days after HIV diagnosis to determine ART initiation.
Person-time accrued from the date of HIV diagnosis (study enrolment) until ART initiation. We assumed that all patients for whom clinic files were created were in care for the first 30 days unless there was evidence of an official transfer or death in the first 30 days after HIV diagnosis. Trained data collectors captured routine clinical follow-up data of consenting participants from facility-based paper and electronic medical records, including laboratory test results from the National Health Laboratory Services. We defined baseline CD4 as the first CD4 result after HIV diagnosis. Trained data collectors captured all routine clinical follow-up data on the REDCap (Research Electronic Data Capture) systems (Vanderbilt University, Nashville, Tennessee, USA). All datasets were exported to STATA V.14 for the analysis.
Patient and public involvement
Patients of the current study were not directly involved in the design of this study or reimbursed for their participation in the study. However, information collected from patients in previous studies informed the design, data collection approaches and interpretation of study results.19 23 Also, the study implementation was guided by healthcare workers from the participating study sites. Study participants consented to a once-off direct data collection after HIV diagnosis and passive follow-up data collection via medical record review. Therefore, direct result dissemination to patients will not be possible. However, we plan to present study results to healthcare workers and policy-makers at participating PHC clinics and at other policy-relevant forums.
Outcome data and analysis
The primary exposure variable was the ART policy period at the time of HIV diagnosis, categorised as pre-UTT (policy active between January 2015 and August 2016), under the general UTT (active between September 2016 and August 2017) policy and the SDI policy (active from September 2017 onward).14 17 23 The primary outcome was ART initiation up to 30 days after HIV diagnosis (30-day ART), and the secondary outcome was ART initiation immediately after HIV diagnosis (immediate ART), both outcomes were coded Yes (1) or No (0). Final data analysis began in October 2018.
Continuous variables were described using medians and IQRs. Categorical variables were described using percentages. Kaplan-Meier analyses were conducted to assess time to ART initiation in the first 30 days of HIV care. Predictors of 30-day ART were modelled using Cox proportional hazards regression, reporting HRs. Variables with a p value <0.1 in crude analyses were entered in the multivariate model. Schoenfeld residuals were used to test the assumption of proportional hazards. Interaction terms with time-varying covariates were created for variables that violated the proportional hazards assumption. Variables were excluded from the model when the inclusion of the interaction term did not resolve the proportional hazards assumption violation. Missing data (where more than 5% of the data were missing), were accounted for by including a ‘not measured/missing’ category where necessary. Additionally, predictors of ART initiation on the day of HIV diagnosis (dichotomised) were evaluated using Poisson regression modelling, reporting relative risks (RR).
All multivariate analyses were adjusted for the time from the period-specific policy announcement to account for the varying lag periods between policy implementation and participant enrolment (policy-months at HIV diagnosis) across cohorts. Additionally, we tested the association between the highest level of education and ART initiation across guideline periods to account for the change in interview language options.
Results
Clinical and demographic characteristics at baseline
Although 1167 (100% of target sample) HIV positive adults enrolled in the study, this analysis was limited to 1029 (88.2%) for whom an outcome could be ascertained (medical data were available), 146 (98.6%) pre-UTT, 141 (97.9%) under UTT and 742 (94.5%) under the SDI policy (figure 1). The survival analyses included only participants who were eligible for ART at the time of HIV diagnosis (n=1004). The exclusive use of English questionnaires in the pre-UTT cohort was the most significant reason for participant non-eligibility (25.9% of total screened). However, the age and gender distributions were similar across cohorts (median 32.6 years for pre-UTT, IQR: 27.2–37.6; 32.3 years for UTT, IQR: 27.2–38.9; and 32.3 years for SDI, IQR: 28.4–39.5) (table 2). Women (median 32.6 years, IQR: 27.0–37.7) were slightly younger at HIV diagnosis than men (median 35.8, IQR: 32.1–41.5) (βfemale −3.4, 95% CI −4.4 to −2.4). The pre-UTT cohort had a marginally higher proportion of participants who completed grade 12 (33.6%) compared with 28.6% in the UTT and 26.1% in the SDI cohorts. Employment rates were also similar across cohorts (47.9% pre-UTT, 46.8% UTT and 54.5% SDI). Among the 146 pre-UTT participants, 122 (83.6%) were eligible for ART.
Although the proportion of participants who tested with CD4 count <350/mm3 decreased from 65.8% pre-UTT to 39.7% in the same-day ART cohort, the percentage of patients with missing baseline CD4 count results increased from 3.4% to 34.7%, respectively. Among participant who had CD4 data, the proportion of patient with baseline CD4 count >500 cells/µL did not change substantially across guideline periods (20.0% during SDI vs 13.5% pre-UTT, RR=1.5 (95% CI 0.9 to 2.3) and RR=1.3 (95% CI 0.9 to 2.4) for SDI vs UTT (18.1%)).
Although most participants lived within 15 min of the diagnosing clinic (56.9%), a small proportion reported travelling over 30 min to the clinic (12.5% overall, 6.8% pre-UTT, 4.3% under UTT and 15.2% under SDI policies). Travel time varied across clinics such that <12% participants from five of the six recruitment sites reported travelling over 30 min to the clinics, but 46.4% of participants from PHC four reported >30 min travel time.
Time to ART initiation from HIV diagnosis across guideline periods
Overall, 71.9% participants initiated ART within 30 days of HIV diagnosis, 36.5% pre-UTT (44.3% of those eligible for ART), 65.9% under UTT and 79.9% in the SDI period. The overall median days to ART initiation declined from 21 days (IQR: 15–30) to 8 days (IQR: 6–16) after the implementation of the UTT policy. Time to ART start was further reduced to a median of 5 days (IQR: 0–8) after the SDI directive was given (figure 2), with most reductions observed 3 months after the SDI policy directive was given to PHCs.

Median time to ART start in the first 30 days of HIV care by art policy periods. ART, antiretroviral therapy; PHC, primary healthcare; UTT, Universal Test and Treat.
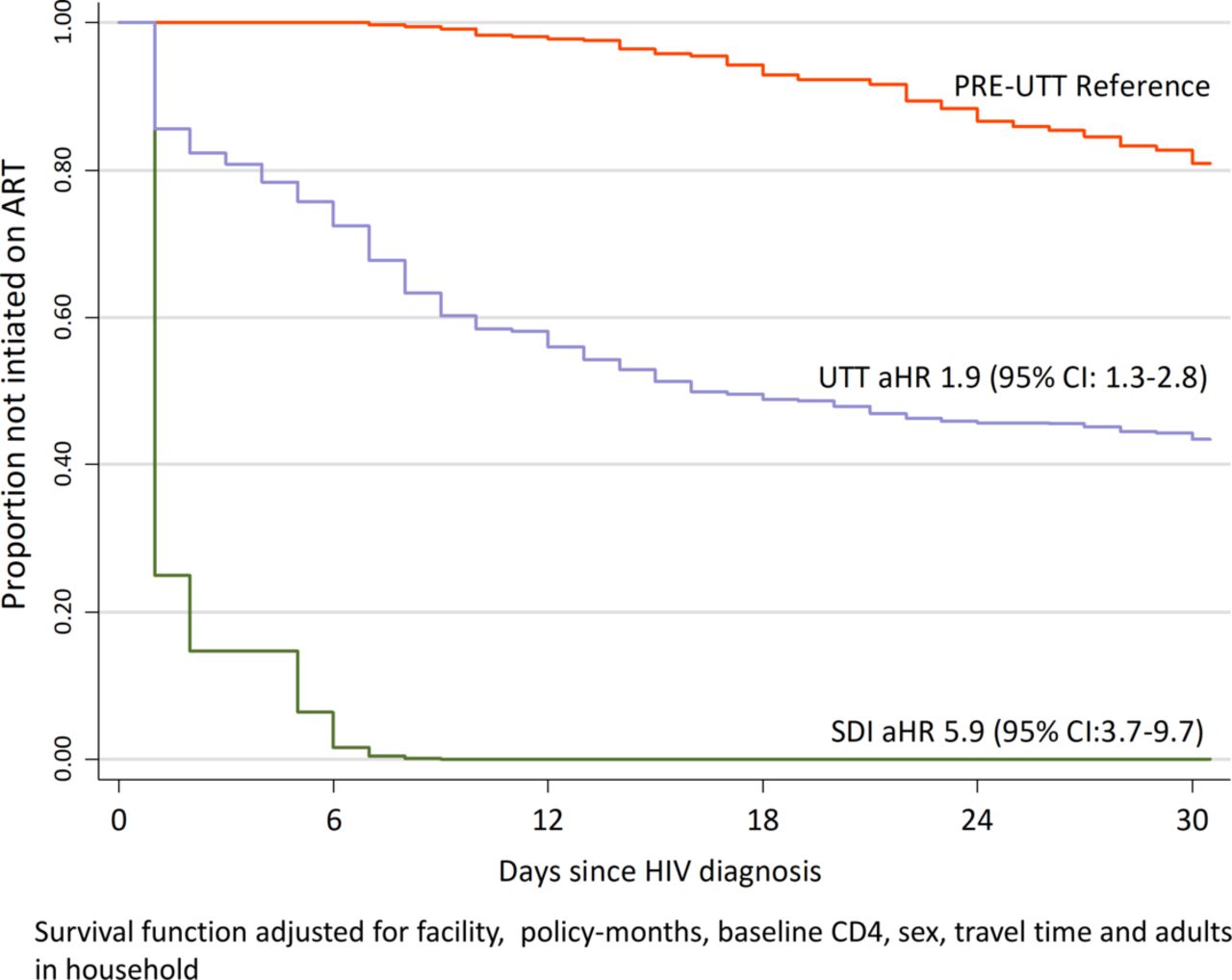
Overall, 30-day ART rates increased with increasing lag time from the prevailing (at the time of participant’s HIV diagnosis) policy announcement (adjusted HR (aHR) 0.4 for ≤3 months vs ≥10 months, 95% CI 0.3 to 0.6). The highest level of education was not associated with 30-day ART uptake. After adjusting for the facility of diagnosis and lag time from the policy announcement, pre-UTT participants were 80% less likely to initiate ART in the first 30 days (aHR 0.2, 95% CI 0.1 to 0.3) compared with SDI participants (table 3). Similarly, patients diagnosed under the UTT policy were 70% less likely to start ART within 30 days of HIV diagnosis (aHR 0.3, 95% CI 0.2 to 0.5) compared with SDI participants (figure 3).
Demographic and clinical characteristics associated with initiating ART within 30 days of HIV diagnosis
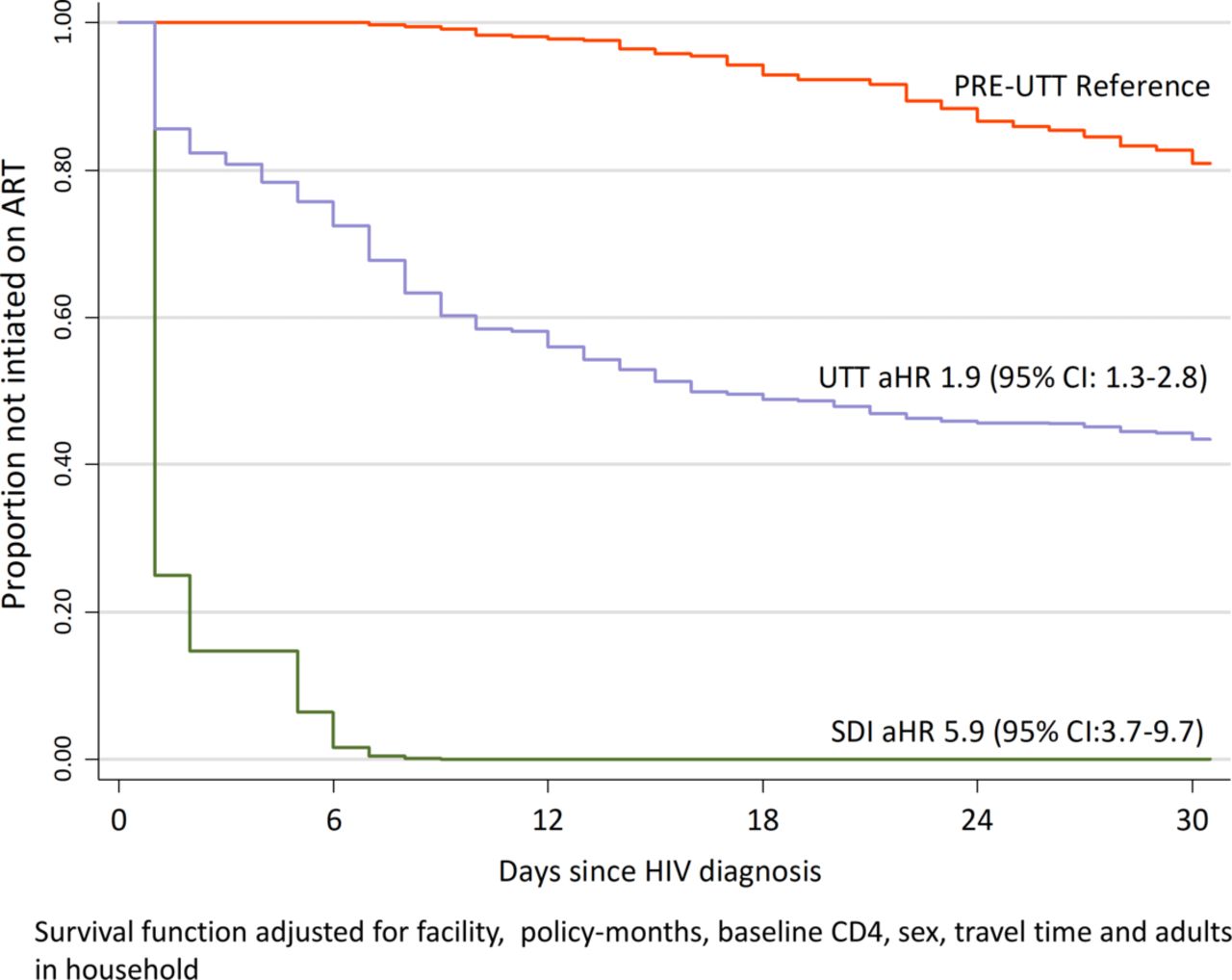
Kaplan-Meier curve of art initiation in the first 30 days of HIV care by art policy periods. aHR, adjusted HR; ART, antiretroviral therapy; CD4, cluster of differentiation four; SDI, same-day initiation; UTT, Universal Test and Treat.
While women had higher 30-day ART rates compared with men (aHR 1.2, 95% CI 1.0 to 1.4), there was no meaningful difference in the likelihood of 30 days ART initiation across age, marital status, travel time to the clinic or employment categories. Overall, compared with patients with baseline CD4 <350 cells/µL, participants with baseline CD4 >500 cells/µL had similar rates of 30-day ART. However, participants who were missing baseline CD4 counts were 40% less likely to start ART within a month (aHR 0.6, 95% CI 0.5 to 0.7). Participants who lived in a two-adult home had higher rates of 30-day ART than those who lived alone (aHR 1.2, 95% CI 1.0 to 1.5). Women were more likely to live with at least one other adult (RR 1.2, 95% CI 1.1 to 1.4) compared with men.
Demographic and clinical characteristics associated with immediate ART initiation within the SDI cohort
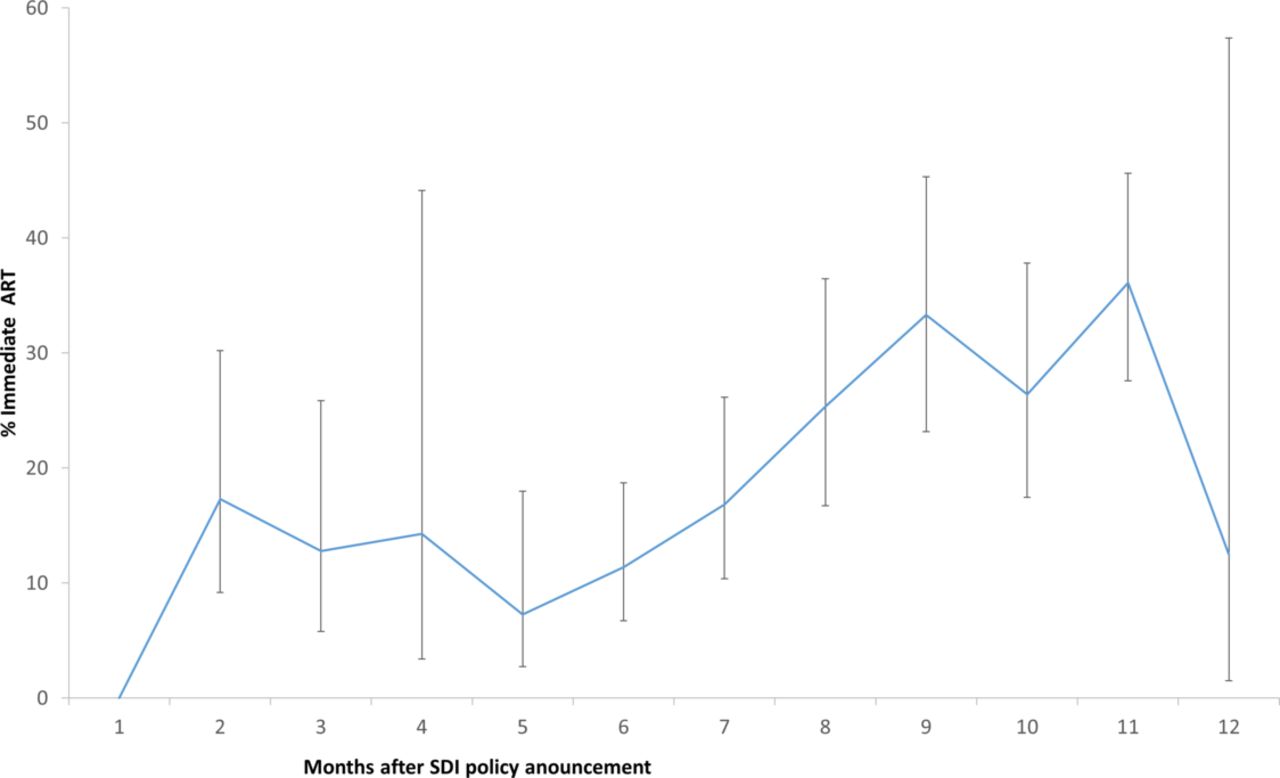
Within the SDI cohort, 150 (20.2%) participants initiated treatment on the day of HIV diagnosis (25.3% of those who initiated ART within 30 days). Women were more likely to take up immediate ART (aRR 1.3, 95% CI 1.0 to 1.9) than men. Older participants (aRR 0.6 for patients ≥40 years old compared with patients in the 18–24 age group, 95% CI 0.4 to 0.9) were less likely to start ART on the day of HIV diagnosis (table 4). In the SDI period, missing baseline CD4 data did not affect the likelihood of starting ART on the day of HIV diagnosis (aRR 1.5, 95% CI 0.5 to 3.7). We also describe a high variability in SDI policy implementation across sites (table 4). Clinic four had the highest proportion of same-day ART initiates and was used as the reference category across all analyses. Figure four illustrates the rates of immediate ART by SDI policy-month with 95% CIs for the proportions. However, immediate ART rates increased gradually with longer policy implementation time (aRR 0.2 for <3 months vs >10 months, 95% CI 0.1 to 0.4) (figure 4).
Demographic and clinical characteristics associated with initiating ART on the day of HIV diagnosis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immediate ART uptake in the first 12 months of the SDI policy implementation. ART, antiretroviral therapy; SDI, same-day initiation.
Discussion
This study highlights a marked reduction in time to ART initiation following the implementation of UTT guidelines, decreasing from a median of 21 days to 8 days, despite this policy not including a directive to modify ART initiation times. An additional decline in time to ART start was also observed after the same-day ART memorandum was sent to clinics. These declines in time-to-ART are consistent with the goals of the WHO HIV treatment guidelines: to initiate patients as early as possible to achieve better clinical outcomes.15 16
Consistent with previous findings,31 we found a decrease in the proportion of patients presenting at PHCs for HIV diagnosis with CD4 <350 cells/µL but little improvement in the CD4 >500 cells/µL group between the pre-UTT and SDI periods. Overall, nearly two-thirds of participants who had baseline CD4 data were diagnosed with HIV with low CD4 counts (<350 cells/µL).
Over a third of the SDI cohort was missing baseline CD4 data. Missing baseline CD4 data in the SDI cohort could have resulted from the lack of clarity in the policy with regards to the need or timing of safety blood tests early in the same-day ART policy implementation or patient impatience with the drawn-out HIV testing and ART initiation processes on the day of HIV testing.17 24 32 It is unclear whether this is a result of the change in the definition of entry in HIV care (first blood draw vs HIV diagnosis) for the SDI cohort. However, this increase in missing baseline CD4 was observed from the pre-UTT cohort to the UTT cohort, at which point clinics already began to reduce time to ART start (to the first week of care for some patients). Nevertheless, having a missing baseline CD4 was associated with a reduced likelihood of 30-day ART compared with patients with lower baseline CD4 values. When we restricted the analysis to the SDI cohort, having a missing CD4 count was associated with a non-significant increase in immediate ART rates, which possibly also means that patients diagnosed under the SDI policy may start ART before the first blood draw and defer baseline CD4 tests. However, this finding requires further exploration.
Women were more likely to start ART within 30 days than men. Interestingly, participants who lived in a two-adult home rather than alone were more likely to initiate ART within 30 days. This may also be indirectly associated with gender as men were more likely to live alone than women. However, participants who lived in larger households had similar 30-day ART rates to those who lived alone, suggesting persisting fear of confidentiality breaches within homes.5 9
Only 20.2% of patients diagnosed under the SDI policy started ART on the day of diagnosis, highlighting possible facility-level policy assimilation challenges. Rates of immediate ART and 30 days ART were also higher among non-pregnant women than men. Immediate ART has been available to South African HIV positive pregnant women since 2013 with relatively few patients or provider acceptability challenges.13 33–35 However, health provider concerns about the SDI policy for the general population may have affected the pace of the policy implementation.24 In a previous qualitative study, Healthcare providers expressed reservations about the acceptability of immediate ART for the majority of their patients and the feasibility of the strategy considering their current workload.24 However, immediate ART rates steadily increased over time, suggesting improvements policy assimilation, although with some variability across sites. While CD4 count did not influence immediate ART uptake, women were younger at HIV diagnosis than men, highlighting the persisting need for consistent efforts to increase early HIV testing and ART initiation younger men.1 33
The strength of these analyses lies in the three prospective cohorts, spanning three ART guideline periods in South Africa, allowing direct observation of the changes in ART uptake over time. This study improves on a possible retrospective review by the collection of extensive personal and contextual data that are not routinely collected. However, the study data are limited by the small number of health facilities assessed, limited information about additional facility-level interventions as well as the contributions by partner organisations in supporting policy assimilation and implementation. Therefore, a more representative facility survey is needed to better explain the facility-level variations in ART policy implementation and outcomes. Additionally, we only collected ART initiation data from testing facilities with a short follow-up period and were not able to determine if some participants went on to start ART elsewhere.
Furthermore, the reason for the higher ART uptake among same-day ART participants require further exploration around the ART initiation processes and their potential impact on ‘patients’ future health-seeking behaviour as well as long-term on-ART outcomes. The sample size did influence the duration of the enrolment process. However, the date of enrolment start depended on ethics approval. Unfortunately, we were negatively affected by university student protests that caused the Human Research Ethics department to stop operations for a while, resulting in a backlog of applications. To compensate for this, we adjusted all multivariate analyses by the lag period between the policy directive to the clinics and the date of patient’s HIV diagnosis.
Conclusion
Our results highlight a positive move towards earlier ART initiation after the implementation of the UTT and SDI policies. However, the results also emphasise a vital need to not only streamline processes to increase immediate ART implementation/uptake further but also ensure timeous baseline safety and monitoring blood tests. Going forward, the need to improve patient demand for early HIV testing remains pertinent to achieve the prevention and treatment benefits of ART.
Acknowledgments
We extend our gratitude to the staff of PHC clinics who supported the implementation of the study and our sincere thanks go to the patients attending these clinics for their willingness to participate and share the valuable information that made this study possible.
References
Footnotes
Contributors DO and MF conceptualised the study and paper. TS managed the study implementation and conducted the primary data analysis. TS, CH, IM implemented the study and contributed to the result interpretation. LCL and MM contributed to the interpretation of the results. All authors reviewed and approved the manuscript.
Funding This study has been made possible by the generous support of the American People and the President's Emergency Plan for AIDS Relief (PEPFAR) through US Agency for International Development (USAID) under the terms of Cooperative Agreements AID-674-A-12–00029 and 72067419CA00004 to HE2RO. The contents are the responsibility of the authors and do not necessarily reflect the views of PEPFAR, USAID or the US Government.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study protocol was reviewed and approved by the Institutional Review Boards of the University of Witwatersrand (M141103) in South Africa and Boston University (H-33516) in the USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Patient medical records are owned by the study site and the National Department of Health (South Africa) and governed by the Human Research Ethics Committee (University of Witwatersrand, Johannesburg, South Africa). All relevant data are included in the paper.