Article Text

Abstract
Introduction People with diabetes are often associated with multifaceted factors and comorbidities. Diabetes management frameworks need to integrate a biopsychosocial, patient-centred approach. Despite increasing efforts in promotion and diabetes education, interventions integrating both physical and mental health components are still lacking in Malaysia. The Optimal Health Programme (OHP) offers an innovative biopsychosocial framework to promote overall well-being and self-efficacy, going beyond education alone and has been identified as relevant within the primary care system. Following a comprehensive cultural adaptation process, Malaysia’s first OHP was developed under the name ‘Pohon Sihat’ (OHP). The study aims to evaluate the effectiveness of the mental health-based self-management and wellness programme in improving self-efficacy and well-being in primary care patients with diabetes mellitus.
Methods and analysis This biopsychosocial intervention randomised controlled trial will engage patients (n=156) diagnosed with type 2 diabetes mellitus (T2DM) from four primary healthcare clinics in Putrajaya. Participants will be randomised to either OHP plus treatment as usual. The 2-hour weekly sessions over five consecutive weeks, and 2-hour booster session post 3 months will be facilitated by trained mental health practitioners and diabetes educators. Primary outcomes will include self-efficacy measures, while secondary outcomes will include well-being, anxiety, depression, self-care behaviours and haemoglobin A1c glucose test. Outcome measures will be assessed at baseline, immediately postintervention, as well as at 3 months and 6 months postintervention. Where appropriate, intention-to-treat analyses will be performed.
Ethics and dissemination This study has ethics approval from the Medical Research and Ethics Committee, Ministry of Health Malaysia (NMRR-17-3426-38212). Study findings will be shared with the Ministry of Health Malaysia and participating healthcare clinics. Outcomes will also be shared through publication, conference presentations and publication in a peer-reviewed journal.
Trial registration number NCT03601884.
- self-efficacy
- diabetes
- biopsychosocial
- self-management
- PRIMARY CARE
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study is a randomised controlled trial to assess the effectiveness of the intervention, including pretest and post-test effects to explore cause–effect relationships.
The intervention has been tested for construct validity during a thorough process of translation and cultural adaptation.
The intervention provides an innovative strength-based recovery-oriented framework employing collaborative therapy principles, aimed at addressing mental health issues and promoting overall well-being that goes beyond simply the provision of educational materials.
The study is limited to community healthcare clinics in Putrajaya, an urban state in Malaysia, which currently records high rates of health literacy in conjunction with high rates of diabetes and the highest prevalence of obesity in the country.
Introduction
Background and rationale
The incidence of diabetes mellitus (DM) is increasing globally, notably in low-income and middle-income countries, with significant impacts at both the individual and the population level.1
With the increasing awareness of psychosocial issues associated with DM over the last decade, there has been a greater demand for a shift from a principally reactive-based healthcare system to a proactive-based approach to management.2 Thus, the management of DM has evolved from an essentially biological approach to more holistic biopsychosocial models.3 Psychosocial elements are central to the management of DM, with an emphasis on collaborative partnerships and patient-centred care in achieving optimal health and well-being.4
Adding to the challenge of rapidly rising rate of DM, low-income and middle-income countries also have limited mental health resources.5 Hence, there has been a call to build the capacity of the healthcare systems especially within primary healthcare settings for the integration of mental health and DM care services.6 Despite increasing efforts in DM education and health literacy, with allocated diabetes educators in healthcare clinics and hospitals,7 improvements in DM care have been marginal.8 Diabetes educators and primary healthcare professionals are mainly trained in physical health and have excellent medical knowledge of the illness, but many do not have the skills and knowledge to address the emotional and psychological aspects comprehensively.9 These limitations have become a significant barrier to addressing mental health issues in patients with DM.9
Often diabetes care will set up the expectation for people with DM to hold the bulk of the control over their own illness throughout the course of their illness10; hence, self-efficacy has a vital role in the ability to manage diabetes effectively,11 including managing emotions and making a commitment to self-care behaviours.12
Self-efficacy has been found to correlate with self-management behaviours11–14 and to be negatively correlated with physical distress,15 depression12 and diabetes distress.16 The role of self-efficacy as a mediator between self-management behaviours and DM-related distress, depression and anxiety has also been reported.13 17 Therefore, an intervention that enhances self-efficacy would be expected to improve depression, diabetes distress, as well as enhance self-management behaviours. The inclusion of self-efficacy as a treatment outcome in a diabetes intervention programme is crucial, as this allows researchers to evaluate the effectiveness of the programme accurately.4
POHON SIHAT: cross-culturally adapted Malay Optimal Health P-rogramme
The Optimal Health Programme (OHP) is a biopsychosocial programme that promotes patients to be actively involved in their own healthcare and overall well-being. The aim of OHP is to improve individual self-efficacy and to build on strengths and values, which in turn enhances overall well-being. Initially developed to integrate physical and mental health, the OHP has been found to be effective in mental healthcare settings18 19 and has been extended to managing physical health and chronic illnesses.20 21 Having a platform to discuss the multiple areas of a person’s life and associated psychosocial barriers creates tremendous potential in the management of DM.
In a preliminary study that assessed the needs of OHP in Malaysia, the OHP was found to provide a promising framework for building the capacity of the local mental healthcare services.22 Following a process of translation and cultural adaptation, the Malaysian OHP programme was developed (henceforth referred to as Pohon Sihat). Being a culturally sensitive tool, Pohon Sihat is suited to use in local Malaysian clinical settings.
Objectives
Pohon Sihat is designed to address gaps in the management of mental health issues in diabetes care within a limited-resource context. This study will examine the effectiveness of this programme for patients with diabetes within a primary care setting in Malaysia.
The intervention will be offered to patients with DM who are currently attending healthcare clinics within the Putrajaya district. Specifically, this study aims to investigate the effectiveness of Pohon Sihat in addition to treatment as usual (TAU) as compared with TAU alone. It will examine the effectiveness of Pohon Sihat in reducing anxiety, depression and diabetes-related distress and in increasing self-care behaviours and glycaemic control.
Methods
Study design
This single-blind, randomised controlled trial will employ a stratified randomisation approach (stratified by size of the Healthcare Clinics). The trial will be carried out at four healthcare clinics in Putrajaya, Malaysia from February 2018 to August 2020. Participants will be individually randomised to one of two parallel groups: TAU or Pohon Sihat (OHP) plus TAU.
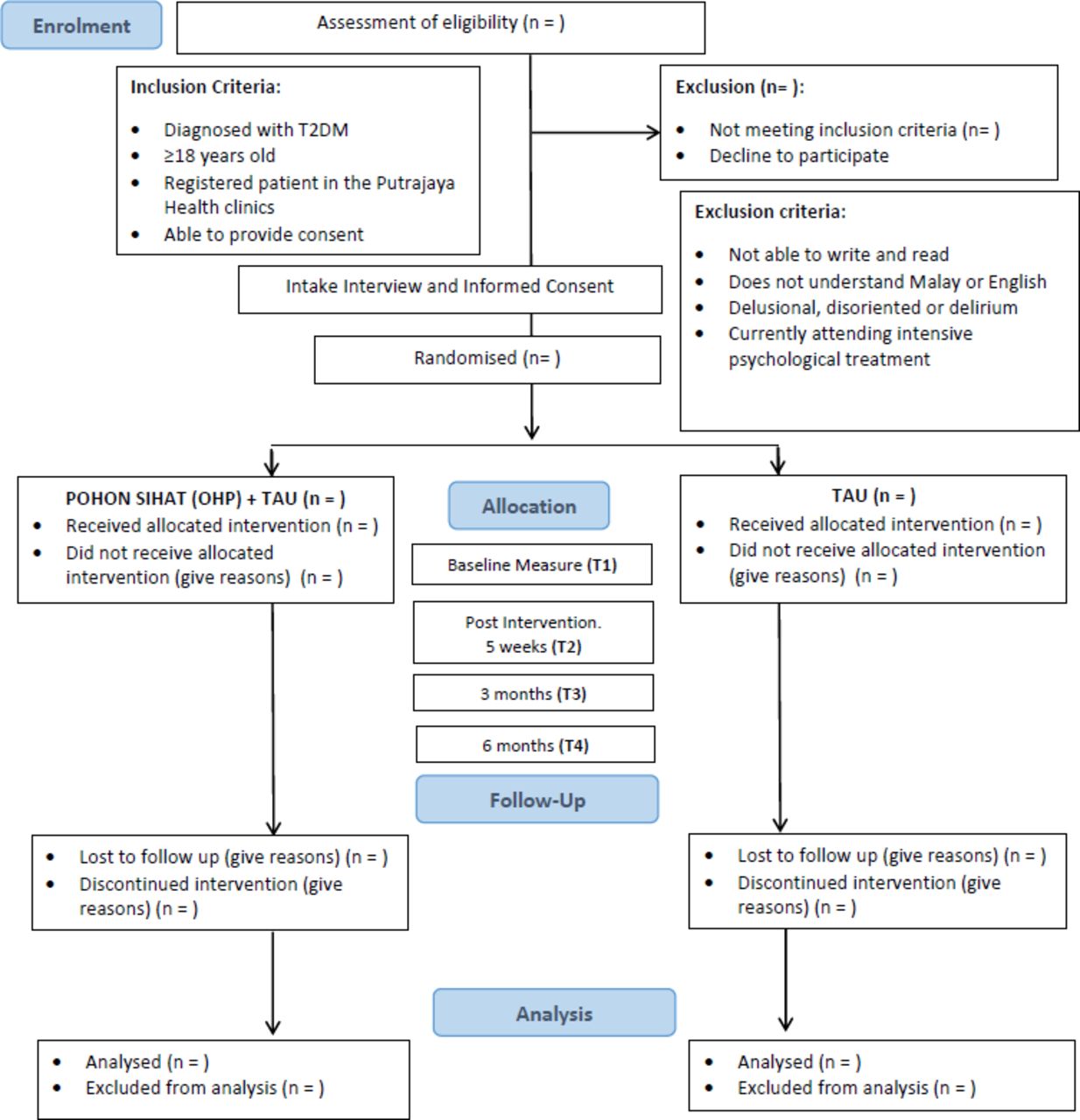
Figure 1 shows the flow chart of participants through the study and figure 2 shows the enrolment, interventions and assessments schedule.

Flow chart of participants. OHP, optimal health programme; TAU, treatment-as-usual; T2DM, type 2 diabetes mellitus.

{kind=link}
{kind=link}
Schedule of enrolment, interventions and assessments. DES-SF, Diabetes Empowerment Scale-Short Form; DMSES, Diabetes Management Self-Efficacy Scale; GAD, General Anxiety Disorder; PHQ, Patient Health Questionnaire; SDSCA, Summary of Diabetes Self-Care Activities; HbA1c, haemoglobin A1c.
Study setting
The Federal Territory of Putrajaya is Malaysia’s federal administrative centre. Based on the National Health and Morbidity survey,8 Putrajaya has a high prevalence of DM (19.2%) and has the highest prevalence of overweight (37%), obesity (43%) and abdominal obesity (61.3%) in Malaysia.
Participants
Sampling frame
The sampling frame will be patients with type 2 DM (T2DM) registered at the primary healthcare clinics within the Federal Territory of Putrajaya. With easy accessibility and communal location, approximately 35% of the Malaysian population receives treatment within the government healthcare clinics located in the community.23
The services and facilities within the clinics differ according to the size of the clinics, which is based on the number of patient visits per day. Healthcare Clinic Presint 9 (KKP9) and Healthcare Clinic Presint 18 (KKP18) have 500–800 patient visits per day. These healthcare clinics are fully equipped with primary healthcare services, family medicine specialists, laboratory, diagnostic imaging, rehabilitation, dietary, pharmacy and dental services. Healthcare Clinic Presint 11 (KKP11) and Healthcare Clinic Presint 14 (KKP14) have fewer than 150 patient visits per day. These healthcare clinics are limited to outpatient services (non-complex cases and/or stable chronic cases) and pharmacy services.
According to the 2018 National Diabetes Registry, registered patients with DM (both type 1 and type 2) are unevenly distributed in terms of the type of the healthcare clinics, the facilities available and the services provided. The sizes of the diabetes clinic in each healthcare clinic differs, with KKP9 having the largest portion of patients with DM in Putrajaya (64%), and KKP11 having the smallest proportion (2%).
Eligibility criteria
Inclusion criteria
Eligible patients will have a diagnosis of T2DM as assessed by their attending physicians based on the Malaysian Clinical Practice Guidelines for T2DM24; be aged between 18 and 60 years; and currently registered to receive services in the healthcare clinics in Putrajaya. Patients also need to be able to provide informed consent to participate in the study.
The criteria for diagnosing T2DM are based on the Malaysia’s Clinical Practice Guidelines, namely being diagnosed with DM and having had/having a confirmed haemoglobin A1c test (HbA1c) level of ≥6.3% (45 mmol/mol) and fasting plasma glucose test (FPG) ≥7.0 mmol/L.
Exclusion criteria
Patients unable to read, write and speak Malay or English, those who are medically unstable or who cannot provide informed consent, will be excluded. Patients who are currently attending intensive psychological treatment will also be excluded from the study.
Withdrawal criteria
Participants can choose to withdraw at any time. Participants may be withdrawn if the research team deems that it is detrimental or risky for them to continue; arrangements will be made for their future care. Withdrawn participants will not be replaced and will be included in the intention-to-treat analysis.
Interventions
POHON SIHAT (OHP)
Participants randomised to the intervention group will receive TAU and will attend the OHP sessions. TAU refers to the pharmacological treatment received or prescribed by the patients’ attending doctor and educational session with diabetes educators at each visit. Diabetes educators facilitate knowledge on healthy eating, physical activity, medication usage and risk reduction practices.24 To improve standardisation of treatment, attending doctors and diabetes educators will be prompted to manage patients in accordance with the Malaysian Clinical Practice Guideline in Management of T2DM.24
The OHP will be delivered in groups consisting of 10–12 participants. The group sessions will be facilitated by at least two trained OHP facilitators. There will be at least one trained mental health practitioner (ie, clinical psychologist), and at least one trained diabetes care expert (ie, diabetes educator and medical practitioner).
Participants will attend 5 weekly OHP sessions (one session per week) and a booster session. The outline of sessions is shown in table 1. Each session will last for 2 hours. Sessions will be conducted outside of routine clinic follow-ups.
Outline of POHON SIHAT sessions for patients with diabetes
Participant’s treatment outcomes will be assessed before the start of the group programme (T1) at the end of the group session (T2), and at the booster session (T3), which is 3 months after T2. At 6-month follow-up (T4), participants will be asked to complete the final assessments, via mail (figure 2).
Control Group or TAU refers to the pharmacological treatment received or prescribed by the patients’ attending doctor and the education session with diabetes educators at each visit. Diabetes educators facilitate knowledge on healthy eating, physical activity, medication usage and risk reduction practices.24 To improve standardisation of treatment, attending doctors and diabetes educators will be prompted to manage patients in accordance with the Malaysian Clinical Practice Guideline in Management of T2DM.24
Outcomes
Primary and secondary outcomes as listed in figure 2 are self-reported outcomes that will be measured at four time points: (1) baseline (pre-treatment), (2) 5 weeks (post-treatment), (3) 3 months and (4) 6 months follow-up. Table 2 is a description of measurements that will be used.
Description of measurements
Primary outcomes
Self-efficacy will be measured by two scales: (1) eight-item Diabetes Empowerment Scale-Short Form25 26 and (2) 20-item Diabetes Management Self-Efficacy Scale.17 27
Secondary outcomes
Secondary outcome will include: (1) depression (Patient Health Questionnaire),28 (2) anxiety (General Anxiety Disorder-7 scale),29 (3) diabetes distress (Problem Areas in Diabetes-5)30 and (4) general well-being (WHO-5 Well-Being Index).31 Self-management behaviours will be measured by the Summary of Diabetes Self-Care Activities Scale.32 33
Data on glycaemic control will be collected from patient records while demographic details, comorbidities, duration and diabetes complications will be assessed using a standard questionnaire, once participants have been allocated to the treatment or control group.
Sample size
Considering the study outcomes, the sample size is calculated based on a similar study34 by using the formula proposed by Zhong.35 As far as response rate is concerned, in studies using OHP, a 12-month follow-up protocol was associated with a 14% drop-out rate for patients with mental illness.36 Similarly, Moriyama et al 37 reported a 16% drop-out rate for a self-management programme in patients with diabetes. Other studies showed that at 6-month follow-up, a self-management programme in T2DM yielded an attrition rate that ranged between 10% and 20%.34 38 Within local government settings, the attrition rate was 10% for a 12-week follow-up education-based programme in patients with diabetes.39 Taking into consideration the duration of follow-ups and a conservative approach, this study will estimate a 30% attrition rate for the loss to follow-up at 6 months.
Based on the study by Wu et al,34 with an expected medium effect size of 0.40 (µ diff=16.19, SD=37.01), the sample size required in this study is calculated using a study-wide type 1 error rate (α) of 0.05 and a type 2 error rate (β) of 0.20 (power of 0.80). The current study will require a total of 59 participants for each group. With an expected attrition rate of 30%, the study aims to recruit a total of 172 participants, with 86 participants for each group.
Recruitment
Study procedure
Recruitment will take place at the healthcare clinics during a patient’s routine check-up, over a period of 6 months or until the required number of participants is achieved.
Based on the list of registered patients during a clinic day, patients with diabetes will be screened based on age and type of diabetes. Eligible participants will be asked for consent to be approached by a research assistant. Those who fulfil the criteria and are able to give written informed consent for participation will be included in the study.
After enrolment, participants will be given an opaque, sealed and numbered envelope containing allocation of groups, in numerical sequence. Each participant will be assigned into the intervention or control group based on the random sequence.
Allocation
Allocation sequence generation
To ensure concealment of allocation, randomisation will be conducted using digit random sampling. The randomisation sequence will be created with simple randomisation procedure and computerised random numbers using Excel 2010 (Microsoft, Redmond, Washington, USA) with participants assigned to either TAU or Pohon Sihat plus TAU.
The four healthcare clinics will first be stratified by the size of the clinic. To ensure a balanced representation of patients with DM within each healthcare clinic, randomisation procedure will be conducted based on the size of the diabetes clinics as reported in the National Diabetes Registry. KKP9 with the largest portion of registered patients with DM (64%) will be allocated 110 participants (64% of 172 participants), followed by KKP18 (31%) with an allocation of 53 participants, KKP 14 (3%) with an allocation of 5 participants and KKP11 (2%) with an allocation of 4 participants.
Allocation concealment mechanism and implementation of random allocation
To ensure that healthcare clinics are assigned with a balanced number of allocated intervention and control, two lists of randomisation sequences will be made (1) clinics with 500–800 patient visits per day—KKP9 and KKP18, and (2) clinics with fewer than 150 patient visits per day—KKP11 and KKP14.
Research assistants involved in the recruitment will be blinded to the sequence allocation. Sealed envelopes will only be opened after eligible participants provide and sign the informed consent form.
Contamination bias
To minimise contamination bias, the OHP plus TAU sessions will take place outside of the participating healthcare clinics. Intervention sessions will be conducted in either a community-based rehabilitation centre or a central health district centre situated within Putrajaya. Participants will also be informed of the study parameters, with directives not to discuss the content of the materials or to exchange materials with other diabetes patients outside of the group.
Blinding
Blinding will be adopted to reduce bias of participants performing better or worse when they are informed which group they are allocated to after the randomisation process. This study will thus incorporate a single blinding process. Participants will not know which group is considered the experimental group and the control group.
Statistical analysis
The intention-to-treat principle and per-protocol analyses will be performed. Any deviations from the random allocation and missing data will be fully reported as outlined in the Consolidated Standards of Reporting Trials statement.40
Any differences between individuals in the intervention and control conditions at baseline (sociodemographics, clinical details, psychosocial self-efficacy, diabetes management self-efficacy, anxiety, depression, diabetes-related distress, well-being, self-care behaviours and HbA1c) will be assessed using one-way analysis of variance (ANOVA) or χ2 test as appropriate. Assumptions of normality and homogeneity of variance will be assessed and adjusted accordingly.
A mixed model ANOVA will be used to investigate the effectiveness of Pohon Sihat (OHP plus TAU) versus TAU on all continuous variables at four points (ie, baseline, 5 weeks, 3 months and 6 months). For all analysis of mixed effect, repeated measures, condition and time will be specified as fixed effects. A one-way analysis of covariance will be used to assess the effectiveness of the intervention compared with the control group, when covariates included duration of diabetes and diabetes complication are expected to impact on outcome measures.
Program assessment, treatment fidelity and cultural adaptation
Program assessment
The adaptation of the OHP for the Malaysian community was informed by1: review by Malaysia’s primary and mental healthcare professionals,2 structured translation3 and cultural adaptation of the programme.
The panel of reviewers included endocrinologist, family medicine specialists and physicians. The OHP was considered by this review to be a valuable engagement tool to further enhance the primary healthcare services and to be more inclusive of mental health needs.22 Following this feedback, the OHP underwent a thorough translation and adaptation process.
Translation and cultural adaptation
The translation and cultural adaptation process involved multiple stages1 with the development of a panel of experts from Malaysia and Australia,2 forward and back translation of the programme workbook,3 cultural adaptation through the review and comparison by both content and local experts, including revision and harmonisation of the workbook,4 pretesting the programme in a group of mental health practitioners, patient support group representatives as well as representatives from the Ministry of Health and finally5 proofreading and finalising the study design. Based on a thorough translation and adaptation process, the programme was assessed as matching the intention and the fidelity of the original programme
Training of diabetes educators
The facilitator training has been modified to include an additional day, taking into consideration minimal prior mental health training for diabetes educators, especially psychological strategies for engaging in effective health communication.9 The additional day includes collaborative therapy principles and motivational interviewing-based health coaching techniques. This modification ensures that the programme delivery will maintain fidelity and stay aligned with its intention.
Each group programme will be facilitated by a trained mental health practitioner and a diabetes care expert to further strengthen the programme’s fidelity.
Pilot study
A pilot study was conducted to assess the feasibility and accessibility of the culturally adapted OHP among patients with T2DM. Eight participants (n=8) were recruited, five completing all five sessions of the programme (three withdrew due to work commitments). Challenges were identified with: (1) recruitment process, (2) duration of the programme and (3) content of the material.
Generally, participants provided valuable feedback on the content of the workbook, structure of the programme and ease of delivery. Participants’ feedback suggested that the sessions be longer to allow more discussion. This was also echoed by the facilitators, who felt that additional time would allow greater coverage and improve ease of delivery. An additional information sheet on healthy eating habit and lifestyle tips was also suggested by participants.
The recruitment process was improved based on the feedback provided by participants and facilitators. During recruitment, participants were informed that an official letter and time slips would be provided to allow time off work to attend the programme.
Several groups programmes were offered throughout the week to allow people to attend the most convenient sessions. Logistical constraints were also improved by choosing venues with ample parking space. Sessions were extended from 1.5–2 hours. Content of the workbook was improved by additional health information such as the food pyramid and the local healthy eating habits. This additional information and some minor language changes improved the overall usability of the OHP Malay workbook.
Patient involvement
Patients were involved in the pretesting stage of the culturally adapted programme in which representatives from a patient support group were invited to review the materials and provide feedback. Feedback on the feasibility and accessibility of the culturally adapted OHP among patients with DM during the pilot study was obtained. The feedback provided served to enhance the content of the workbook, the structure of the programme and the delivery. The study results will be communicated to participating patients who have made a request.
Ethics and dissemination
Consent
The process of obtaining consent is in line with the Declaration of Helsinki. Information regarding the study, and random allocation of participants will be outlined in a patient information sheet as approved by the Ethics Committee (refer online supplementary file). The randomisation process will be clearly outlined to the eligible participants. A signed informed consent will be obtained from each participant. At the end of the study, participants in the control group (TAU) will be invited to participate in OHP.
Supplemental material
Data management
All participant information will be treated as strictly confidential. Personal information will be coded to ensure the confidentiality of the participants and no individuals will be identifiable in any research material, reports or publications. No information collected will be shown to anyone apart from the research team. Data from the study will be stored securely in locked cabinets and electronic data will be kept on password-protected drives accessible only by the research team. Permission to share information with appropriate health professionals will be sought if health concerns arise for participants.
Dissemination plan
The findings of the study will be shared with stakeholders through publication and conference presentations. The outcomes of the study will be shared through publication within a peer-reviewed journal within 12 months of the last data collected. As part of the ethics approval requirements, the outcomes will be shared with the Malaysia Ministry of Health and participating healthcare clinics.
Discussion
The complexity of DM is associated with not just the patients’ physical health but also their emotional well-being and mental health, social, occupational and overall quality of life.41 The growing numbers of people with DM are associated with greater health impacts and increased psychosocial barriers for the individual, family and community. Moreover, even though Putrajaya as a state that ranks high in health literacy, the prevalence rates of diabetes and obesity are still the highest in the country. With its mediating role between health literacy and self-care behaviours,42 self-efficacy may be the missing link in understanding the dissonance between illness education and the ability to use the knowledge to commit to a healthy lifestyle.
The OHP is a self-efficacy enhancing psychological intervention that is low intensity, structured and can be delivered by trained facilitators. The recovery-based approach of the OHP emphasises the language of hope and well-being rather than illness and disease, and is suitable for a primary healthcare setting. Through a patient-centred, collaborative approach, the OHP may offer a platform for a wide range of primary healthcare providers to engage in a discussion with patients regarding their well-being. As a psychological intervention programme for primary healthcare providers, OHP can address mental health concerns and promote overall well-being for people experiencing chronic illness. The OHP will be the first engagement tool in Malaysia with potential to act in a curative and preventative role.
In addition to providing further understanding in the effectiveness of OHP as an add-on psychological intervention, the study will also provide information on the effectiveness of the current standard of practice within the primary healthcare as guided by the Malaysian Clinical Practice Guidelines in the Management of T2DM.
Trial status
Patient recruitment commenced October 2018 and data collection will continue until August 2020.
Acknowledgments
The OHP was developed at the Mental Health Research Institute of Victoria and St Vincent’s Hospital Melbourne. We would like to thank the Director General of Health Malaysia for his permission to publish this article.
References
Footnotes
Contributors AFS, NI, K-AT and UAS designed the study. AFS wrote the first draft of the manuscript and coordinated the development of the study protocol. BR, K-AT, GM and DJC contributed a thorough review of the manuscript which AFS revised in the second version. UAS, NI, K-AT and BR then provided further written feedback. All authors critically reviewed, revised and approved the final version of the manuscript to be submitted by AFS. AFS, K-AT, BR, UAS, GM and DJC further reviewed and contributed towards the revised versions of the manuscript.
Funding This work was supported partially by the UPM GP-IPS grant number GP-IPS/2018/9670500.
Competing interests DJC has received grant monies for research from Eli Lilly, Janssen Cilag, Roche, Allergen, Bristol-Myers Squibb, Pfizer, Lundbeck, Astra Zeneca, Hospira; Travel Support and Honoraria for Talks and Consultancy from Eli Lilly, Bristol-Myers Squibb, Astra Zeneca, Lundbeck, Janssen Cilag, Pfizer, Organon, Sanofi-Aventis, Wyeth, Hospira, Servier; and is a current Advisory Board Member for Lu AA21004: Lundbeck; Varenicline: Pfizer; Asenapine: Lundbeck; Bitopertin: Roche Aripiprazole LAI: Lundbeck; Lisdexamfetamine: Shire; Lurasidone: Servier. He has no stocks or shares in any pharmaceutical company.
Patient consent for publication Not required.
Ethics approval Ethical approval for this study has been obtained from the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia.
Provenance and peer review Not commissioned; externally peer reviewed.