Article Text

Abstract
Introduction Percutaneous coronary intervention (PCI) aims to provide instant relief of symptoms, and improve functional capacity and prognosis in patients with coronary artery disease. Although patients may experience a quick recovery, continuity of care from hospital to home can be challenging. Within a short time span, patients must adjust their lifestyle, incorporate medications and acquire new support. Thus, CONCARDPCI will identify bottlenecks in the patient journey from a patient perspective to lay the groundwork for integrated, coherent pathways with innovative modes of healthcare delivery. The main objective of the CONCARDPCI is to investigate (1) continuity of care, (2) health literacy and self-management, (3) adherence to treatment, and (4) healthcare utilisation and costs, and to determine associations with future short and long-term health outcomes in patients after PCI.
Methods and analysis This prospective multicentre cohort study organised in four thematic projects plans to include 3000 patients. All patients undergoing PCI at seven large PCI centres based in two Nordic countries are prospectively screened for eligibility and included in a cohort with a 1-year follow-up period including data collection of patient-reported outcomes (PRO) and a further 10-year follow-up for adverse events. In addition to PROs, data are collected from patient medical records and national compulsory registries.
Ethics and dissemination Approval has been granted by the Norwegian Regional Committee for Ethics in Medical Research in Western Norway (REK 2015/57), and the Data Protection Agency in the Zealand region (REG-145-2017). Findings will be disseminated widely through peer-reviewed publications and to patients through patient organisations.
Trial registration number NCT03810612.
- continuity of care
- adherence to treatment
- health literacy
- healthcare utilisation
- percutaneous coronary intervention
- rehabilitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- continuity of care
- adherence to treatment
- health literacy
- healthcare utilisation
- percutaneous coronary intervention
- rehabilitation
Strengths and limitations of this study
The CONCARDPCI is an interdisciplinary, multicentre effort with the unique combination of data from hospital medical records, patient self-report and national registries providing opportunities to identify novel pathways for continuity of care that contribute to outcomes.
Although the linkage to national registers will ensure complete follow-up of the study population, potential challenges include response rate of patient self-report at follow-up.
Non-participants will be compared with participants on a limited number of registry variables to account for potential selection bias.
Introduction
The widespread commitment to involve patients in planning and service development has become a key element of current healthcare policy. Health literacy, as the ability to access, process and comprehend health information and services, can be used to complement both individual patient care and community-level development. Understanding the varying health literacy of patients, particularly in those who experience poor access and outcomes, is thereby pivotal.1 The American Heart Association (AHA) recently published a scientific statement2 addressing health literacy in cardiovascular disease as of fundamental relevance to primary and secondary prevention. European leaders in secondary prevention have called for action in the postacute aftercare of patients with coronary artery disease (CAD).3 Although CAD is the single most common cause of death in Europe, there has been an encouraging decrease in mortality ascribed to improvements in risk factor management, pharmacological treatment and revascularisation techniques.4 Since more people need to manage life with CAD as a chronic disease, modern developments in primary healthcare provision have led to increased interest in continuity of care as an essential element.5–7 Patients’ transition from hospital to home is particularly challenging because patients need to adjust their lifestyle, incorporate new medications and acquire additional sources of support.8 Although there is compelling evidence for secondary prevention following CAD, a large majority fail to achieve lifestyle changes and therapeutic targets set by the European Society of Cardiology guidelines.9 Therefore, adherence to treatment is also of concern. Non-adherence to medications is common for patients with cardiovascular diseases.10 Taking prescribed antiplatelet and other secondary preventive medication after percutaneous coronary intervention (PCI) is pivotal; however, it is unknown if non-adherence also applies for patients following PCI.
This paper describes a multicentre cohort study, the CONCARDPCI, that seeks to identify bottlenecks and hurdles in the patient journey and suggest the optimal timing of services and alignment with patient preferences for patients with CAD undergoing PCI. Of special interest are challenges with continuity of care, health literacy and self-management, adherence to treatment advice, costs at all care levels and associations with future short and long-term health outcomes.
Uptake to cardiac rehabilitation (CR) is suboptimal,9 11 12 and few sufficiently powered real-world studies have been undertaken with the explicit purpose of investigating continuity of care and pathways of CR in patients after PCI. In addition to investigating factors associated with low referral, participation, health literacy and adherence rates among CR participants, studies are increasingly needed on evaluating alternative modes of providing CR. Follow-up of healthcare use, costs and predictors of costs following PCI in a non-clinical trial setting have been infrequently investigated.13 14 Thus, a large cohort of real-world observations that can ascertain interventions for future clinical trials is needed.15 The CONCARDPCI responds to this challenge. In CONCARDPCI, we hypothesise that continuity of care, Health literacy and self-management, and adherence to treatment in patients are directly associated to outcomes after PCI.
Aim of the research programme
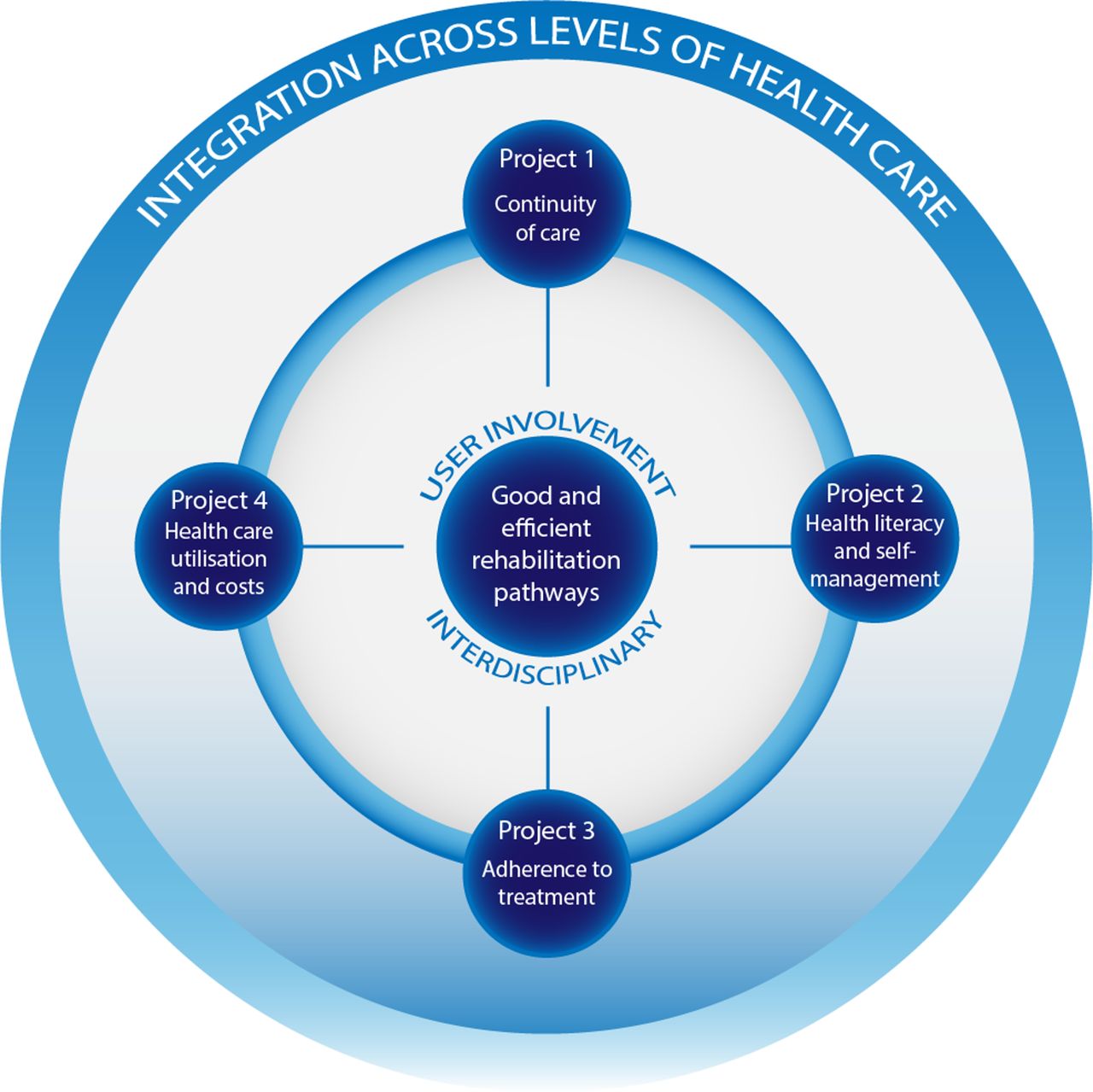
The overall aim of CONCARDPCI is to investigate (1) continuity of care, (2) health literacy and self-management, (3) adherence to treatment, and (4) healthcare utilisation and costs, to determine associations with future short and long-term health outcomes in patients after PCI. CONCARDPCI is organised into four thematic projects on continuity of care; health literacy and self-management; adherence to treatment; and healthcare use and costs (figure 1).

Projects in CONCARDPCI researching bottlenecks for good and efficient patient pathways across levels of healthcare.
Methods
Study design and setting
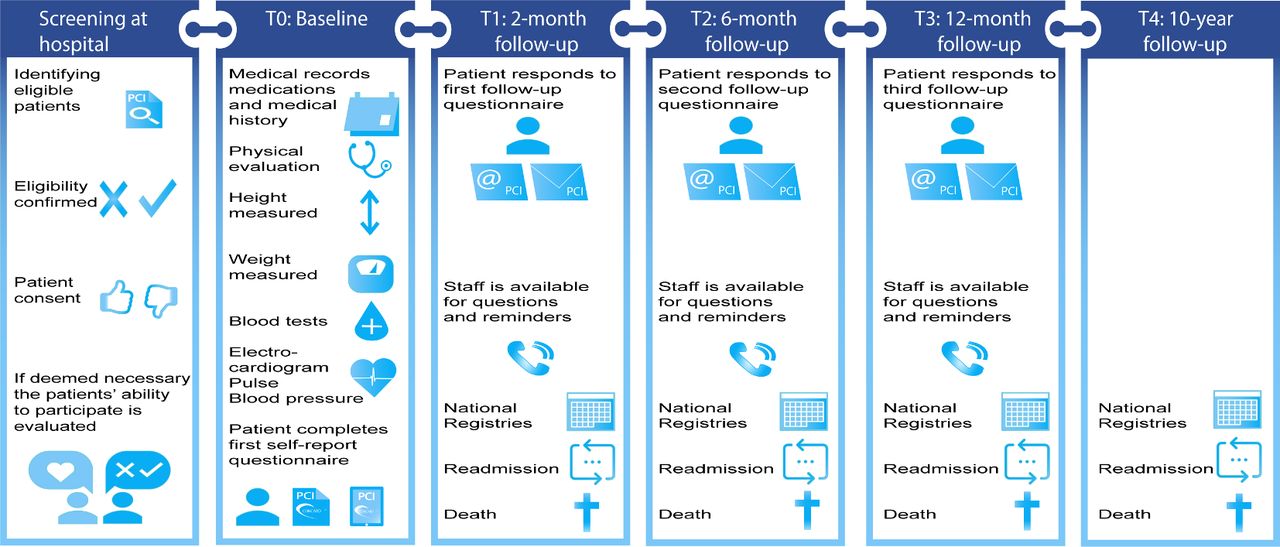
CONCARDPCI is a large-scale multicentre cohort study with serial prospective survey data collection, clinical data and register-based follow-up. We collect data from hospital medical records, patient self-report surveys and national registries (figure 2). Preliminary work has been performed including in-depth interviews on patients’ experiences of healthcare delivery to provide a context for the quantitative data and inform the content of the cohort survey questionnaires. Three follow-up surveys over 1 year are undertaken, and a 10-year follow-up for adverse events.

Measuring time points and data collection in the cohort study in CONCARDPCI.
Seven large referral PCI centres in Norway and Denmark were selected based on the following considerations: presence of a committed research team including CONCARDPCI study nurses and a local principal investigator, prior research experience including research infrastructure, geographical location and size. The PCI centres perform from 900 to >2000 (mean 1668) PCI procedures annually, are having 629–1400 beds (mean 943) and are referral centres for coronary angiography and PCI for a total of 37 local hospitals (figure 3, table 1). Haukeland University Hospital is the sponsor centre of this investigator-initiated research programme. For study organisation, see online supplementary appendix.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
H=PCI centres including the local hospitals in their catchment area.
Description of centres participating in CONCARDPCI
Study population
All patients undergoing PCI at seven large PCI centres are prospectively screened for eligibility. Screening is performed in the hospital setting by the site coordinator and trained CONCARDPCI study nurses. Daily admission records and the operating programme are reviewed to identify potentially eligible patients. Electronic medical records are reviewed to confirm eligibility according to the inclusion and exclusion criteria (table 2). When cognitive impairment is suspected by clinical or study personnel and there is no medical record of the problem, the Confusion Assessment Method16 and 4AT17 are used to investigate whether the patient must be excluded. Patients who are delirious or too clinically unstable to participate following PCI, who would otherwise be eligible, are reassessed until discharge. During the in-hospital assessment, participants provide informed consent. Because many of the questionnaires are designed for patient self-assessment, patients who need a complete proxy are ineligible. If participants need assistance in filling out the questionnaires, this is registered in the case report form (CRF). Regarding sample size and study power, see the Data analysis and sample size determination section.
Eligibility criteria for CONCARDPCI
Measurement and data collection
In CONCARDPCI a broad range of outcomes are measured and data are collected by physical assessment at baseline, review of the medical records, patient self-reported questionnaires (at baseline, 2, 6 and 12 months) and from national registries (table 3 and figure 2). A comprehensive data dictionary and CRF are provided to ensure standardisation of abstracted data. For the Danish centres, eCRFs are used. Patients included in the study undergo a brief physical assessment and complete the self-report questionnaires at baseline after PCI (T0) (table 3 and figure 2). A follow-up with postal or electronic questionnaires is distributed to all patients included in the study, 2 months after discharge (T1). The time interval ensures time for follow-up care to evaluate early postdischarge continuity of care. A consecutive subgroup of patients (n=100) at the Sponsor Coordinating Centre are approached for a retest of the eHealth Literacy Scale (eHEALS)18 and the Heart Continuity of Care Questionnaire (HCCQ)19 as part of the validation process of the instruments. All patients are followed up with postal or electronic questionnaires at 2 (T1), 6 (T2) and 12 (T3) months after discharge. Non-responders receive one reminder. Vital status is identified to avoid sending questionnaires to deceased patients or their family. Patient adverse events are followed through national registers for 10 years or until death (T4) (figure 2). Questionnaire packages are discussed with patient representatives and piloted at every measuring time point (T0–T3) before employed in the large-scale cohort study.
Sociodemographic, clinical and patient-reported measures, and timing of assessments in the CONCARDPCI prospective cohort study
To objectively assess adherence to therapy, serum levels of a wide panel of cardiac medications are measured. A consecutive subsample of 500 Norwegian patients from two centres will be invited to give a blood sample 1 year after the index procedure. The time is chosen as it corresponds to collection of patient-reported data on adherence. Moreover, adherence tends to diminish over time20; hence, the 1-year contact was chosen. Serum levels are submitted to an accredited clinical pharmacology laboratory, and quantified using liquid chromatography with mass spectrometry. Patients are labelled as non-adherent when serum level of at least one of the evaluated drugs is below the limit of quantification.
Management of cohort and registry data
For the Norwegian centres, baseline (T0) data are transferred to the National Coordinating Centre for data entry and/or review. The forms are reviewed and queries sent to the centre for missing or incomplete items. All follow-up data are collected by postal mail and managed at the National Coordinating Centre. The paper version data are entered into electronic files by trained staff.
For the Danish centres, each centre registers patients who are screened, and either included or excluded in separate Microsoft Excel (V.2016) spreadsheets in a shared secure team site server hosted by the National Coordinating Centre. Data from medical records are entered into a shared SurveyXact (V.12.9) database at each study site and managed by the National Coordinating Centre. Patient self-reports at both baseline (T0) and follow-up are collected either electronically using a tablet via a SurveyXact link or by paper as requested by the patient. Paper version data are entered into the SurveyXact database by trained CONCARDPCI study nurses. All follow-up data are collected and managed by the National Coordinating Centre.
Every resident in Norway and Denmark has a unique personal identifier that allows data sets from national registries to be merged on an individual level. The data sets will be released in a coded and deidentified form, but with a unique identifier common to the data sets making individual merging possible. The heart registries, prescription registries,21 22 cause of death registries23 24 and administrative registries on social security microdata and healthcare utilisation25 26 are mandatory, and legally exempted from requirement of obtaining patient consent. Strict rules on how data can be used or linked are followed to secure privacy protection. Although these data are similar in composition, we are interested in contrasting and comparing Denmark with its high CR uptake to Norway with a lower uptake.
Data analysis and sample size determination
Descriptive statistics of the cohort by nation will be generated using proportions, means and SDs or medians and IQRs as appropriate. Cross-sectional analysis will be used for continuity of care (table 4) using multiple linear regression testing for a random effect for nation. For health literacy, there is a single follow-up and multiple linear regression testing for a random nation effect will be used. The cohort’s longitudinal observations over 1 year will be modelled using generalised linear mixed models (GLMM) that account for within-person correlation for adherence to medications, healthcare utilisation and cost (table 4). We will test whether patients clustered within nation is significant. If so, we will include it as a hierarchy in the GLMMs. For time to readmission, and time to major adverse cardiac event, we will use competing risk models to account for censoring by death. We will construct risk stratification models that predict the probability of each outcome for specific combinations of risk factors. We will establish internal validity by using bootstrapping techniques. We will test whether missing data are at random. If not, we will estimate the probability of missingness and include it as a weight or covariate factor in the models. For psychometric evaluation of translated instruments we evaluate the structural, discriminant and convergent validity, and reliability of the scales. For internal consistency, Cronbach’s alpha is used. Test–retest reliability is evaluated by using intraclass correlation coefficients of patients’ results obtained at a 2-week retest interval. Confirmatory factor analysis is used for evaluating the factor structure of the original eHEALS18 and HCCQ19 instruments.
Definition of outcomes in CONCARDPCI
Power calculations for the cohort study are based on time-to-first event outcomes, as these require the most patients. To maintain at family-wise type I error of 0.05% and 80% power using the method of Hsieh and Lavori27 for adjusted Cox regression models 2550 patients are needed. To adjust for losses to follow-up, we increased this estimate by 18% for a total of 3000 patients. Thus, all outcomes will have ≥80% power with alpha ≤0.05.
Ethics approval and consent to participate
The ethical guidelines of the World Medical Association, Declaration of Helsinki and the legislation in Norway and Denmark guide the study (Declaration of Helsinki, 2008). At inclusion, a detailed letter informing the potential participant of the study, and the right to withdraw from the study at any time without any reason is underlined. The identifying key is kept in a separate file from the data. The data are kept in strict confidence in locked files at research servers to protect the participants’ privacy. Approval by the Norwegian Regional Committee for Ethics in Medical Research in Western Norway has been granted (REK 2015/57), and from the Data Protection Agency in the Zealand region for the Danish centres (REG-145-2017). Written agreements between the Sponsor Coordinating Centre, and the local principal investigators and directors of the departments in each participating study centre, are signed before initiation of data collection. The study is registered at ClinicalTrials.gov.
Patient and user involvement
CONCARDPCI involves patients and stakeholders to target aspects of the patient journey to identify bottlenecks and carve out a user-friendly intervention. Patient involvement is carried out in several ways: two patient representatives with a history of CAD, and trained to be patient representatives both in healthcare and research settings,28 provide input to the planning, implementing and reporting of results from the study. Representatives from all healthcare levels will be end users of knowledge from the project and are actively involved in the project through the CONCARDPCI Expert Group (online supplementary appendix). Reporting of patient involvement will follow the GRIPP2 reporting checklists.29
Communication of results and transition of knowledge
The CONCARDPCI has a close-to-practice and clinical approach, which will be an advantage in dissemination and communication with end users. Results will be disseminated to patients through patient organisations, and to healthcare professionals in PCI treatment teams and CR teams, as well as in primary care through seminars and scientific meetings. Due to the comprehensiveness of the outcome measures in the thematic projects (table 4), numerous scientific papers are expected. Long-term follow-up will be reported as data become accessible. Authorship on publications from the study will be allocated using the guidelines for authorship defined by the International Committee of Medical Journal Editors and depends on personal involvement.
Discussion
While medicine has produced large advances in cardiac treatment, there is need for more consistent patient pathways and systematic follow-up care. In order to do so, bottlenecks in the patient journey need to be identified. CONCARDPCI aims to close knowledge gaps related to four main areas: (1) continuity of care, (2) health literacy and self-management, (3) adherence to treatment, and (4) healthcare utilisation and costs of care. Although landmark cohort studies have been carried out to describe the aftercare of patients after acute myocardial infarction (MI), less is described of the patient journey, specifically after PCI, and rarely have these included extensive self-report from patients. In the past decade, an increasing number of studies using patient-reported outcomes have been performed, but in a different setting, with shorter follow-up and targeting subgroups of patients with acute MI.30–34 The US-based SILVER-AMI study focused on older adults,30 the VIRGO study31 concentrated on younger women after acute MI, TRIUMPH32 was designed to examine racial differences after acute MI, Vanderbilt Inpatient Cohort Study33 included both patients after acute MI and patients with heart failure, and NOR-COR34 retrospectively surveyed patients below 80 years of age 2–38 months after the index event including also patients with coronary artery bypass surgery or no intervention. Age is of particular concern as it is documented that invasive strategies benefit clinically stable very old patients with non-ST-elevation acute coronary syndrome.35 In contrast, CONCARDPCI has an extended perspective by prospectively including adult patients with no age limit, engaging stakeholders throughout the study, applying a comprehensive interdisciplinary approach and including data from national registries. One great asset of the participating Nordic countries is infrastructure in research with access to demographics and health information through the national registries. The registries include all citizens, and a personal identifying number ensures no loss to follow-up. In addition to national compulsory registries on death (National Death Registry),23 24 readmission and use of healthcare services (National Patient Registry)25 26 and prescription and medication consumption (National Prescription Registry),21 22 the countries have disease-specific national medical quality registries (eg, the Norwegian Registry of Invasive Cardiology). With establishing national registries, opportunities for nationwide comparisons and quality improvement of healthcare service are created.
While the aforementioned studies30–34 also have detailed data abstracted from medical records and self-report, CONCARDPCI has a timely approach in the four thematic projects—one of which concerns health literacy, and specifically eHealth literacy is of particular relevance in information technology-driven societies. The AHA Scientific Statement on health literacy2 calls for studies examining health literacy and cardiovascular outcomes beyond 30-day readmission. It is suggested that health literacy can be evaluated as part of programmes aiming to improve secondary prevention in that health literacy influences dropout rates in CR. CONCARDPCI responds to this challenge.
Lack of continuity of care and low health literacy are likely to carry increased healthcare utilisation (eg, readmission to hospital) and increased cost.36 The potential need for rethinking CR based on patient preferences and in-built economic analysis is a relevant path to follow. Moving towards a more patient-centred care aims to maximise patients’ self-care abilities. Increased self-care is an overarching goal when healthcare expenditure rises to unaffordable levels. Further, in additional parameters, patient-reported outcomes can potentially identify patients at high risk of adverse outcomes and hospital readmissions,37 38 which is of importance both to patients and society.
The importance of increased patient involvement and shared decision-making at all levels of healthcare is underlined in policy documents at a governmental and regional level.39 Patient involvement is a unique feature of CONCARDPCI scarcely described in comparable large-scale studies. The use of standardised patient-reported outcome measures may provide information that can assist in this decision-making.37 38 In CONCARDPCI, we include patient-reported outcome measures on a global, generic and disease-specific level,40 and pose research questions related to patient pathways that concern a large group of patients. We anticipate that treatment outcome (adherence), safe communication (continuity and health literacy) and self-management will prove important to future healthcare.
However, the study has some limitations. We lack participating hospitals from northern Norway. The remoteness and distance to the PCI centre is a feature of that area and therefore of particular concern. However, travel time to the PCI centre from the most remote fjords in western Norway is also long and this catchment area is included in the study (figure 3). Further, we exclude patients with delirium and dementia due to ethical reasons regarding informed consent and logistical difficulties. Delirious patients and patients too clinically unstable to be included following the PCI procedure, who would otherwise be eligible, are reassessed until discharge. Non-participants will be compared with participants on a limited number of registry variables to account for potential selection bias. Extensive self-report is a feature of CONCARDPCI, and we use validated questionnaires and only a few de novo created questions based on patient interviews. Still, the response rate of follow-up (T1–T3) may be a potential limitation. However, previous methodological work in patients with CAD showed high acceptability of comprehensive questionnaires41 and patient representatives participating in planning of CONCARDPCI ensured relevance of the questionnaires.
Status
Data collection for the cohort study commenced on 12 June 2017 and is expected to continue until July 2020, with a 10-year follow-up until July 2029. The inclusion of patients for the blood sampling for objective medication adherence measurement has started.
Acknowledgments
We acknowledge the full group of CONCARD Investigators and our collaborators. A list of institutions and people involved can be found in the online supplementary appendix. The authors are grateful for the assistance provided by Marie Hayes for the development of the figures. We acknowledge the in-house contributions of all the cohort study centres.
References
Footnotes
Twitter @TNorekval, @CNRGCam, @Trond Røed Pettersen@EdTrond
Contributors TMN is the principal investigator of CONCARDPCI and was responsible for study conception, development of the project outline and ethical approval. HGA, GB, NF, TBH, TRP, IV and SR contributed to the development of the project outline. HGA is chairing the Scientific Advisory Board with CD, HH, RS and ADZ as contributing members. NF is the coordinator of the cohort study in CONCARDPCI with TBH as the national coordinator in Denmark, and AIL, BBe, BBo, PP, TBH and TBR are local principal investigators. CB and SI give specific input on transition of care. GB, TRP, TBH and IV are leaders of thematic projects. JS is a major contributor in design of studies on serum levels of cardiac medications and Project 3 in general. TMN wrote the first draft of the manuscript. All authors revised the manuscript critically, and read and approved the final manuscript. A more detailed description of the roles of all authors can be found in the online supplementary appendix.
Funding The CONCARDPCI is funded by a major grant from the Western Norway Health Authority (Grant No 912184). We also received funding from the Novo Nordisk Foundation (Grant No NNF17OC0030130), Zealand Regional Research Foundation (Grant No 15-000342), Bergen Health Trust grants 2016–2018 and the Copenhagen University Hospital, Rigshospitalet. HGA is supported in part by the NIH/NIA R01 AG047891, R33 AG057806 and P30 AG021342. TMN is supported in part by a Western Norway Health Authority research grant (Grant No 911870). TRP is supported by a Western Norway Health Authority PhD fellow grant for CONCARDPCI (Grant No 912295), and IV by a PhD fellow grant from the Western Norway University of Applied Sciences.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.