Article Text

Abstract
Introduction The number of individuals with gender dysphoria seeking gender-affirming treatment is increasing. The short-term and long-term effects of masculinising treatment with testosterone are debated as serum testosterone increases up to 20-fold compared with cisgender women. We will investigate short-term and long-term effects of masculinising testosterone treatment on preclinical and clinical coronary disease, muscle strength and power, oxygen consumption (VO2) max, cardiac and respiratory function and quality of life including aggression in transgender men.
Methods and analyses Prospective, single-centre, observational cohort study at the Body Identity Clinic (BIC), Odense University Hospital, Denmark. Investigations are performed at inclusion and following 1, 3, 5 and 10 years of testosterone therapy. Non-calcified coronary plaque volume and calcium score are estimated by coronary CT angiography. CT is only performed at inclusion and following 1 and 10 years. Upper body muscle strength and power are measured by a ‘low row’ weight stack resisted exercise machine. Evaluation of aggression and quality of life is assessed by questionnaires, VO2 max is estimated by maximal testing on bike ergometer, and cardiac and respiratory functions are measured by echocardiography and spirometry, respectively. Markers of cardiovascular risk and inflammation and also cortisol and cortisone are assessed in blood, diurnal urine and/or hair samples. Our cohort (BIC), including dropouts, will be an embedded subcohort in a future national registry study in all individuals with gender dysphoria and controls. Data are available on International Statistical Classification of Diseases and Related Health Problems 10th version diagnostic codes, prescriptions, socioeconomics and causes of death.
Ethics and dissemination The Regional Committee on Health Research Ethics for Southern Denmark (S-20190108) and the Danish Data Protection Agency (19/27572) approved the study. Signed informed consent will be obtained from all participants. All findings will be published in peer-reviewed journals or at scientific conferences.
Trial registration number NCT04254354.
- general endocrinology
- coronary heart disease
- sex steroids & HRT
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Body Identity Clinic is a research clinic where this prospective longitudinal 10-year cohort study in transgender men will assess preclinical coronary disease by estimating non-calcified plaque volume and calcium score using coronary CT angiography.
The applied methods ensure important health-related and sport-related data on upper body muscle strength and power, aggression, oxygen consumption max, cardiac and respiratory function in transgender men, during short-term and long-term testosterone treatment.
A proper control group is missing, but it is unethical to perform a placebo-controlled randomised trial on long-term testosterone therapy in persons with gender dysphoria.
Results will only be available in transgender and non-binary individuals, treated with testosterone, however, a parallel study in transgender women and non-binary persons on feminising treatment is planned.
Introduction
Recent European studies report that 0.6%–0.8% of individuals assigned female at birth have incongruent gender identity or gender dysphoria.1 2 Testosterone treatment is the cornerstone of masculinising treatment and is initiated in transgender men and by request in non-binary individuals. Testosterone is an important androgenic and anabolic hormone. The androgen effects of testosterone include terminal hair growth and deepening of the voice, whereas the anabolic effects include muscle growth. Body shape changes from feminine to masculine during testosterone treatment, as subcutaneous fat is reduced3 and redistributed.4 5 The changes in sex hormones are quite dramatic in transgender men, as circulating testosterone concentrations increase up to 20-fold into the normal range for cisgender men,6 while estradiol levels are partly supressed.
Clinical coronary disease is rare in young persons,7 however, preclinical coronary disease is observed and testosterone treatment may accelerate non-calcified coronary plaque (NCP) formation. Both NCP and calcified plaques may be detected by the sensitive coronary CT angiography (CCTA)8 in combination with a semiautomated computer program.9 In a large cardiac CT registry study in younger (mean age 39 years) participants, 22% of cisgender men and 15% of cisgender women without cardiovascular symptoms, had coronary artery disease defined as any plaque formation (non-calcified or calcified).8 The association between testosterone treatment and NCP formation has been reported in ageing cisgender men after 1 year of testosterone treatment,10 with increased waist to hip ratio at baseline as the strongest predictor of NCP formation.11 There is a lack of knowledge regarding NCP formation in relatively young transgender men on masculinising testosterone therapy. We know that lipid status is deteriorated during masculinising testosterone treatment in transgender men, with an increase in low-density lipoprotein (LDL) cholesterol and a decrease in high-density lipoprotein (HDL) cholesterol12 and blood pressure may increase.13 14 However, studies on cardiovascular endpoints in transgender men are limited and conflicting. A fourfold increased OR for myocardial infarction in transgender men was reported, which was significant after adjusting for age, diabetes mellitus, hypertension, hypercholesterolaemia, chronic kidney disease, smoking and exercise levels.15 The study design was, however, cross-sectional, hence it was not possible to conclude on cause and effect. A retrospective study in transgender men reported no cases of myocardial infarction after 10 years of testosterone treatment,16 but the retrospective study design increased risk of selection bias due to lost to follow-up before 10 years.
Testosterone treatment is associated with dose-dependent increases in muscle mass17 18 and muscle strength5 17 in cisgender men. Muscle mass also increases during masculinising treatment with testosterone in transgender men,19 but there are limited data on changes in muscle strength before and during masculinising testosterone treatment. One study reported higher lower body muscle strength during gender affirming treatment with testosterone.20 Upper body muscles have higher number of androgen receptors than lower body muscles21 and characterising muscle strength and power in the large muscles of the arms and upper back during testosterone treatment in transgender men would be of interest. Grip strength was higher in transgender men compared with cisgender women.22 However, the study was cross-sectional, and hand grip strength only tests the small muscles of the hand and lower arm.
The World Professional Association for Transgender Health (WPATH)23 recommends to warn against elevated aggression levels as a psychological adverse effect of masculinising testosterone treatment in transgender men, however, this presumption was not supported by recent data.24 25 The term aggression covers a wide range of intercorrelated behaviours, thoughts and emotions. There is no uniform definition of aggression26 and studies reporting increased aggression scores during testosterone treatment27 had severe methodological problems and high risk of bias. Valid information on aggression constructs27 during short-term and long-term testosterone therapy is ensured in the present study by a questionnaire, which incorporates all dimensions of aggression28 and questionnaires containing information on anxiety, depression, testosterone dose, duration of treatment and physical health.
Low cardiorespiratory fitness has been associated with an increased risk of premature death from all causes, but cardiovascular disease is the most common cause of death in cisgender individuals.29 The maximum oxygen consumption (VO2 max), determined from a graded maximal exercise test, is an approved way of classifying cardiorespiratory fitness levels.30 VO2 max is generally higher in cisgender men compared with cisgender women,31 presumably due to differences in muscle mass, cardiac output, haematocrit and lung size. There are no prospective data on VO2 max during masculinising testosterone treatment in transgender men, but VO2 max is expected to increase, as testosterone increased muscle mass20 and haematocrit.14 Exogenous testosterone increased aerobic running time in young physically active cisgender women32; testosterone gel, 10 mg per day for 10 weeks, was used, the dose equals 20% of masculinising testosterone treatment.
Obstructive and restrictive estimates of respiratory function are estimated by spirometry and reference ranges for spirometry vary with gender assigned at birth, weight, height and age. Asthma is characterised by obstructively decreased respiratory function with airway hyper-responsiveness and inflammation. Asthma is much more prevalent in cisgender women compared with cisgender men33; however, we have no reference ranges for respiratory function in transgender men.34
Masculinising testosterone treatment in transgender men is for life and currently no prospective data are available on long-term morbidity. This study will provide important information on health issues regarding cardiovascular and respiratory health and upper body muscle strength and power. Aggression levels may be elevated during testosterone therapy, but the temporal relation has not been clarified. The combination of long-term clinical observational data and access to national registry data will provide further knowledge on benefits and risks of masculinising testosterone treatment.
Aim
To investigate short-term and long-term effects of masculinising testosterone treatment on preclinical and clinical coronary disease, muscle strength and power, VO2 max, cardiac and respiratory function and quality of life including aggression in transgender men.
We hypothesise that, in transgender men:
Masculinising testosterone treatment accelerates NCP development and progression.
Testosterone treatment will be associated with long-term increase in upper body muscle strength and power, VO2 max, cardiac and respiratory function.
Aggression scores will increase during initiation of testosterone treatment, but the aggression scores will return to baseline during long-term testosterone treatment.
Methods and analysis
Study population and recruitment
Participants are individuals assigned female at birth with a diagnosis of gender dysphoria treated with testosterone or approved to start treatment with testosterone. Only individuals associated with one of the three centres of gender identity in Denmark: Odense, Aalborg and Copenhagen are included. No individual with known use of ‘self-prescribed’ sex hormones is included. The inclusion period for the cohort (N=200) is estimated to last 2 years.
Study design
For study outline, please see figure 1. The study is a prospective single-centre observational cohort study at Body Identity Clinic (BIC), Odense University Hospital, Odense, Denmark of 10 years duration. Participants (aged 18 years and older) are invited for five visits (baseline, 1, 3, 5 and 10 years) after informed consent has been given. The participants will spend 1 day in BIC per visit and all examinations use the same equipment and study protocols (table 1). Ethical permission has been obtained for the use of registry data regarding International Statistical Classification of Diseases and Related Health Problems 10th version (ICD-10) diagnostic codes, medical treatment, socioeconomics and causes of death in all participants including participants lost to follow-up. The participants accept study participation by written informed consent. All individuals in Denmark have a civil registration number (CPR) reflecting binary gender. During legal transitioning individuals may change CPR and data from the two CPR numbers is merged. We will be able to compare study participants with participants lost to follow-up by combining the clinical outcomes with registry data (table 1, figure 1).

Study outline.
Overview of study outcomes and visits
Patient and public involvement statement
An advisory board of transgender men has been established. The participant advisory board meetings were arranged prior to application for ethical approval of the study to secure inputs in terms of relevance of research questions, recruitment, outcomes and participant time consumption. The participant advisory board has read and commented on the study material and will be contacted for continuous sparring.
Endpoints
Primary endpoint
NCP volume.
Secondary endpoints
Calcium score.
Upper body muscle strength and power.
Aggression and quality of life.
VO2 max.
Left ventricular muscle mass and function.
Respiratory function.
Serum levels of testosterone, estradiol and cortisol.
Circulating markers of cardiovascular risk and inflammation.
Diurnal urine and hair samples for assessment of cortisol and cortisone.
Outcomes
Outcomes and visits are outlined in table 1.
Coronary CT angiography
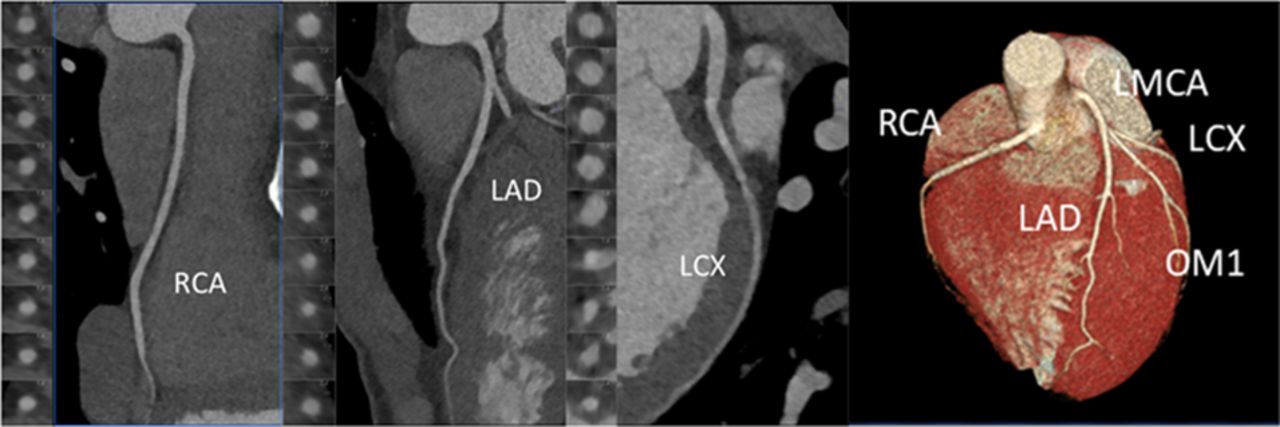
CCTA (high-end CT scanner) is conducted at the first visit, after 1 year and at 10-year follow-up (table 1) to examine the presence of NCP and calcified coronary plaques (figure 2). The scanning protocol depends on the patient heart rate. In patients with a stable heart rate above 60 beats per minute, orally or intravenously β-blocker are administered until the heart rate is appropriate (if possible below 60), and a prospectively gated protocol is used. Participants with a heart rate >70 bpm despite β-blocker pretreatment are subjected to a retrospectively gated scan with dose modulation. Additionally, sublingual nitrates are administered prior to the scan. Administrating of β-blocker and nitrates are in accordance to daily clinical practice. An experienced cardiologist performs data analyses of NCPs, calcium score/stenosis and pericardial fat using a semiautomatic program.9 Radiation amounts to 1.6 mSv per CCTA. We have ethical permission to perform three CCTAs during the study period of 10 years. Radiation from CCTA is lower than expected and we are applying for an additional CCTA at 5 years.

{kind=link}
{kind=link}
The figure displays a coronary CT angiography. A semiautomatic programme detects non-calcified coronary plaque. LAD,left anterior descending artery; LCX, left circumflex artery; LMCA, left maincoronary artery; OM, obtuse marginal branch 1; RCA, right coronary artery.
Upper body muscle strength and power
A ‘low row’ weight stack resisted exercise machine (Technogym, Italy) tests arm and upper back muscles. The machine is adjusted to fit the individual participant relative to body height and arm length. Body weight, training history and age estimates initial loading. Warm-up is 3×10 and 1×5 repetitions at the estimated test load, with 1 min of rest in between sets. Subsequently maximal effort (one repetitions maximum, 1RM) is obtained using single repetitions with increasing load until task failure (the participant is unable to complete the full range of motion) with 2 min of rest in between sets. Hereafter participants are instructed to perform at least 3 sets of one repetition as forceful and fast as possible to evaluate muscle power with a load corresponding to 80% of 1RM and 2 min of rest in between sets. During each repetition, peak and mean power is measured. To evaluate muscle power we attach a PUSH V.2.0 inertial motion device (PUSH, Toronto, Canada) to the weight stack. The PUSH device includes a three-axis accelerometer and gyroscope, enabling measurements of human movement kinematics at a sampling rate of 1000 Hz. Previously, PUSH has been validated to evaluate power using resistance exercises.35 Peak and mean power (watt), respectively, are calculated based on kinematic data derived by the PUSH software.
Questionnaires
Buss-Perry Aggression Questionnaire, Quality of life: SF-36, Inventory of Interpersonal Problems, Gender Q (Development in progress), General Anxiety Disorder-7 and Patient Health Questionnaire-8.
Vo2 max
Measurement of VO2 max is performed on a bike ergometer and Vyntus CPS system. The resistance will start low and increase gradually until maximum capacity or exhaustion. At maximum capacity lactate is measured.
Echocardiography
A comprehensive transthoracic echocardiography is performed by a medical doctor. The recordings are stored digitally for blinded analysis. The followings are included: Size and mass of all cardiac chambers, left ventricle ejection fraction, global longitudinal strain, left ventricle diastolic function and heart valve function.
Respiratory function
Respiratory function is tested by a spirometer (Vyntus CPS system) measuring forced expiratory volume in 1 s, forced vital capacity and peak flow.
Blood, urine and hair samples
Testosterone, estradiol and cortisol levels and cardiovascular risk markers in blood and serum (HbA1c, lipids, haematocrit, adiponectin, soluble urokinase-type plasminogen activator receptor (suPAR)) are analysed along with inflammation markers in blood and serum (C reactive protein (CRP), interleukin 6 (IL-6)). Hormone levels are measured after an overnight fast between 8:00 and 9:00 hours by liquid chromatography tandem mass spectrometry (LC-MS/MS), which is calibrated by in-house prepared calibrators, and the relative SD is <10%. Quality for steroid hormones is assured by monthly participation in the external quality control programme for steroid hormones from The UK National External Quality Assessment Service (UK NEQAS). Sex hormone binding globulin is determined on serum samples by a Roche assay on Cobas e602 with a precision of 1.8 %−4.0% (14.9–21.9 nmol/L). Free testosterone levels are calculated assuming a plasma albumin concentration of 43 g/L.36
Haemoglobin is measured using a photometric analyser with a coefficient of variation (CV) of 2.8%. Plasma total cholesterol and HDL cholesterol are analysed by enzymatic colorimetric reactions (Modular P, Roche), and LDL cholesterol is calculated using the Friedewald equation.37 HbA1c is measured by high-performance liquid chromatography using Tosoh G8 (Medinor, Broendby, Denmark); the analytical CV is 0.9%. Adiponectin is determined by an in-house time resolved immunofluorometric assay,38 with intra-assay and interassay CV averaging 5% and 10%, respectively.
Plasma suPAR is measured with the suPARnostic ELISA (ViroGates A/S, Birkerød, Denmark) with a mean CV of 4%. CRP is analysed using latex based immunoanalysis (CRP Ultra, Sentinel Diagnostics, Milan, Italy) by an Architect c8000 instrument (Abbott). The intra-assay and interassay CVs are 0.8% and 1.9% for normal levels of CRP, respectively. Plasma IL-6 is measured with Quantikine HS-IL-6 ELISA (R&D Systems, Minneapolis, USA) with a mean CV of 8%.
Diurnal urine samples: Participants are instructed to note the time for voiding in the morning before starting sample collection, and all urine collected until the morning of the second day. Urine samples are kept frozen at −20°C until analysis. Cortisol and cortisone are analysed by LC-MS/MS. Urine samples are solid phase extracted on an Oasis HLB 96-well plate after addition of deuterated internal standards; the analysis is calibrated by in-house prepared calibrators, and the relative SD is <10%. Quality is assured by monthly participation with satisfactory results in the external quality control programme for steroid hormones from the UK NEQAS.
Hair samples: A section of hair strands approximately 3 mm in diameter is cut as close to the scalp as possible from the posterior vertex area. Hair samples are stored in aluminium foil as previously described,39 the 4 cm hair segment closest to the scalp is used for analyses to represent cortisol secretion over the most recent 4-month period.40 The analyses will be carried out at Department of Psychology, Technical University of Dresden, Germany using LC-MS/MS.41
Whole-body dual X-ray absorptiometry and bone mineral density
Dual X-ray absorptiometry, Horizon A Discovery is used to measure whole-body lean body mass, fat mass and bone density. Radiation amounts to 0.1 mSv per scan.
Medical history
Chronic diseases, medication and supplements, alcohol, tobacco and abuse, gynaecological history, previous treatment with testosterone, information on diet and physical activity are recorded.
Physical examination
Height, weight, body mass index (BMI, kg/m2), blood pressure, waist and hip circumference and face and body hair (Ferriman-Gallwey Score) are recorded.
Sample size and statistics
The primary study endpoint is NCP. We have estimated the sample size, as no valid data exist for a proper power calculation regarding the primary endpoint, NCP. We aim to include 200 participants, including 50 men who are approved to start testosterone treatment based on the power calculation of the main secondary endpoint, upper body muscle strength and power. Sample size estimation for upper extremity muscle strength and power was based on data (mean baseline/SD) from a comparable cohort.42 The estimation was based on a 10% within-participant difference (deemed as functional relevant) with an alpha level of 0.05 and a statistical power of 0.80. On the basis of this data, a sample size of 39 was sufficient to detect within-participants differences with two-tailed comparison. To account for potential drop-outs (estimated to 20%) 50 individuals approved to start testosterone treatment will be recruited for the trial.
Normally and non-normally distributed data will be analysed using parametric and non-parametric statistics, respectively. Associations between testosterone and endpoints will be investigated with multiple linear regression modelling. Random mixed-effects linear regression models will be applied to investigate associations between testosterone and longitudinal repeated markers of assessed outcomes. We will collaborate with a statistician regarding random mixed-effects linear regression modelling.
A directed acyclic graph will be depicted in order to transparently identify a priori assumptions of causal relations between exposure, outcome, potential confounders, intermediate factors and selection bias. Missing data will be handled according to type. Depending on data, analyses will be performed based on either complete case analyses or, if appropriate, by imputing missing data in collaboration with the statistical department. Analyses will be conducted using STATA V.14 (StataCorp 2015). Post regression diagnostics/model validation will be performed. Assumptions of linearity between predictors and the outcome variable will be inspected by using scatter plots and augmented component-plus-residual plots. Normality of predicted residuals will be checked with quantile-normal and probability-normal plots. Homogeneity of variance (homoscedasticity) of the residuals will be investigated by plotting residuals against the fitted (predicted) values. Multicollinearity will be assessed using variance inflation factors. Open-ended questions will not be included. Data are anonymised according to Danish law and regulations (The Regional Committees on Health Research Ethics for Southern Denmark, Project-ID: S-20190108, The Danish Data Protection Agency, journal no. 19/27572), and therefore analyses will be performed through a remote VPN access to Statistics Denmark.
Data management
Data are stored and analysed electronically and unauthorised access denied. Original data are filed according to one participant number. Research Electronic Data Capture (REDCap) (www.project-redcap.org), hosted by Open Patient data Explorative Network (OPEN), is used for registration of data.43 44 REDCap meets the safety requirements set by the Danish Data Protection Agency for storage of person-sensible data. OPEN Analyse, a secure remote desktop solution hosted by OPEN, is used for storage and analyses of the pseudoanonymised data.
Ethics and dissemination
All participants give written informed consent. The study results will be published in peer-reviewed journals, publication will be according to the International Committee of Medical Journal Editors recommendations and the investigators oblige themselves to publish both positive and negative findings. The study is performed in accordance with theDeclaration of Helsinki and regulations of the General Data Protection Regulation. It is approved by the Danish Data Protection Agency (journal no. 19/27572), the Regional Committees on Health Research Ethics for Southern Denmark (project-ID: S-20190108).
Discussion
Preclinical coronary disease is determined by NCP volume and calcium score in transgender men during this 10-year prospective cohort study at BIC. NCP volume is assessed by state-of-the-art CCTA and we use the lowest detectable change in NCP formation (1 mm3) as the clinically relevant difference.45 However, a proper power calculation regarding our primary endpoint cannot be performed as no previous data has been published. Therefore, distribution of data is unknown and the SD cannot be calculated. The possible lack of NCP development during 10 years is acknowledged, but this potential negative result would be reassuring and clinical relevant. In a large cardiac CT registry study in relatively young cisgender men (mean age 39±6 years), 424 out of 1143 participants did not have any cardiovascular symptoms.8 Experienced cardiologists assessed the CCTAs, reporting coronary plaque of any kind in 22% of asymptomatic 424 cisgender men.8 In our study, we increase the sensitivity of detecting NCPs by using a semiautomatic programme, which is comparable to Autoplaque.9
We also aim at providing new scientific evidence regarding upper body muscle strength and power in men on masculinising therapy. Upper body muscles are of special interest as the number of androgen receptors are higher in the upper body muscles compared with lower body.21 Also, our study will elaborate on interesting data on possible increased levels of aggression during testosterone therapy and the temporal relation between masculinising testosterone treatment and levels of aggression.27 Aggression is very relevant clinical issue in the context of the WPATH warning regarding aggression on testosterone therapy.23 We will report new data on VO2 max and cardiac function as improvements in cardiorespiratory fitness are associated with considerably reduced mortality risk and adverse cardiovascular event rates29; furthermore, data on respiratory function will add new knowledge and all the above-mentioned results are important for transgender men and non-binary individuals on testosterone therapy in health and sports.
Ethical permission is granted to access registry data from all participants including those, who leaves the clinical study part. Registry data will provide knowledge, regarding national ICD-10 diagnostic codes, medical treatment, socioeconomics and causes of death. Future access to national registry data in all individuals with registered gender dysphoria and controls will allow us to study our cohort (BIC) as an embedded subcohort including individuals, who remain in the 10-year study as well as dropouts. We have previously used this design in women with polycystic ovary syndrome.46 The gold-standard research design to assess benefits and risks of testosterone therapy in transgender persons is a long-term placebo-controlled randomised trial on masculinising therapy, however, it is deeply unethical to perform such a study, when gender dysphoria is present. Apart from the future registry study we will compare data from our cohort to results from Odense Androgen Study (OAS).6 47–49 OAS is a large cross-sectional study in 783 young healthy men (20–29 years old); data are available on BMI, waist circumference, muscle mass, fat mass, blood pressure, Hba1c, testosterone and estradiol levels, lipid status and VO2 max and a follow-up is planned (Ethical Committee Journal number, S-20130097). Our study is a non-representative cohort study with risk of selection bias regarding age, BMI, smoking, ethnicity, fitness level and morbidity. Data on health consequences regarding all aspects of gender affirming treatment is warranted, however, this study will only provide information on transgender men and non-binary persons on testosterone therapy. To counteract this unbalance, a parallel study has been planned in transgender women and non-binary persons on feminising treatment.
Acknowledgments
We would like to thank our collaborators: Per Aagaard, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark. Kaya Rössler, Department of Psychology, University of Southern Denmark, Odense, Denmark. Malene Hilden, Center of Gender Identity, Rigshospitalet, Copenhagen, Denmark. Astrid Højgaard, Center of Gender Identity, Aalborg University Hospital, Aalborg Denmark.
References
Footnotes
Contributors All authors meet the ICMJE criteria for authorship. MSA and JF: Conception and design of the study. LLC, MSA, DG, TTK, AD, JF and GT contributed in writing the protocol. All authors read and approved the final manuscript.
Funding Study funded by Odense University Hospital (Frontlinjepuljen). Award/grant number: N/A.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.