Article Text

Abstract
Introduction Shared-housing arrangements (SHAs) are small, home-like care environments in Germany. Residents are predominantly people with dementia. The risk for all-cause hospitalisation is consistently higher for people with dementia compared with people without dementia and there is currently no evidence-based intervention to reduce the risk of hospitalisation. Thus, the DemWG study investigates whether a complex intervention is effective in reducing hospitalisation (primary outcome), behavioural and psychological symptoms of dementia and falls and for stabilising cognitive functioning and quality of life in people with dementia and mild cognitive impairment (MCI) in German SHAs.
Methods and analysis Based on the UK Medical Research Council framework ‘Developing and evaluating complex interventions’, a prospective, mixed-methods, multicentre, cluster-randomised controlled trial combining primary and secondary data analyses as well as quantitative and qualitative research methods is being conducted. The intervention consists of three parts: (A) education of nursing staff in SHAs; (B) awareness raising and continuing medical education (CME) of general practitioners; (C) multicomponent non-pharmacological group intervention MAKS-mk+ (‘m’=motor training; ‘k’=cognitive training; ‘+’=fall prevention) for people with dementia and MCI. Randomisation is stratified by the German federal states and type of setting (rural vs urban). Neither the trained professionals nor the participants are blinded. Data are collected at baseline and after 6, 12 and 18 months with standardised instruments. Quantitative data will be analysed by multivariate analyses according to the general linear model, qualitative data using qualitative content analysis. Recruitment is still ongoing until 31 December 2020.
Ethics and dissemination All procedures were approved by the Ethics Committee of the University of Bremen (Ref. 2019-18-06-3). Informed consent will be obtained before enrolment of participants. Due to findings of previous randomised controlled trials, serious adverse events are not expected. Results will be disseminated in peer-reviewed journal publications and conference presentations.
Trial registration number ISRCTN89825211.
- dementia
- delirium & cognitive disorders
- geriatric medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The internal validity of the study results should be high due to the use of a standardised manualised treatment and the allocation of the participating shared-housing arrangements (SHAs) (clusters) to the intervention and control groups by stratified cluster randomisation, which is an appropriate method for evaluating complex interventions in everyday practice.
The external validity of the study results should be high due to the ‘naturalistic setting’ in everyday practice in German SHAs, recruitment from all German federal states and the balanced ratio of urban-to-rural facilities.
Longitudinal data collection over 1.5 years will enable an examination of the implementation of the complex intervention into practice and the sustainability of effects.
Because we are investigating a complex non-pharmacological intervention that addresses multiple actors, neither the trained professionals nor the participants are blinded.
For organisational reasons, randomisation has to be completed and communicated before screening and participant enrolment; this can lead to recruitment bias due to different motivational levels that depend on group assignment.
Introduction
Dementia is one of the major causes of disability and dependency among older adults, affecting individuals and professional caregivers, families, communities and societies.1 In 2019, there were over 50 million people living with dementia worldwide, even though the number is rising rapidly due to an improved life expectancy, with an estimated number of 152 million people in 2050.2
Dementia (F00-F03) is defined as a syndrome due to disease of the brain, usually of a chronic or progressive nature. People with dementia have disturbances of multiple higher cortical functions, that is, memory, thinking, orientation, comprehension, calculation, learning capacity, language and judgement, whereby consciousness is not clouded. Cognitive impairments are commonly accompanied, and occasionally preceded, by deterioration in emotional control, social behaviour or motivation. Beyond that, People with dementia have significant impairments in activities of daily living (ADL).3 Therefore, dementia is strongly associated with institutionalisation, that is, admission to a nursing home.4 5 Nevertheless, findings suggest that care environments should be as homelike as possible so that they can have positive effects on residents’ behaviours and well-being.6 Thus, several concepts have been established worldwide in recent years, for example, ‘small-scale living arrangements’ in the Netherlands, ‘green houses’ in the USA and ‘shared-housing arrangements (SHAs)’ in Germany.7 8 All these concepts are defined as small and homelike environments that offer person-centred care, take into account residents’ needs and choices and offer a daily routine that is organised around meaningful activities that support the principle of normal living.7
Currently, there are about 3100 SHAs in Germany, most of which (about 690) are located in the German federal state of Berlin.9 10 The number of residents typically ranges from 6 to 8, with an average of 8 and a maximum of 12 residents per SHA.11–13 Residents are predominantly people with dementia, female, 80 years of age on average and can usually remain in the SHA until they die.13 Residents typically share one large apartment in an ordinary apartment building with an outpatient care service that provides 24-hour care.13 Care by the nursing service is occasionally accompanied by volunteer assistants who carry out social activities free of charge.9 A study found an increase in quality of life (QoL) as well as a decrease in behavioural and psychological symptoms of dementia (BPSD) during a 1-year follow-up in SHAs.14 Nevertheless, in line with previous international findings, no clear advantage of either SHAs or special care units in nursing homes could be found.14 15
A recent meta-analysis found that all-cause hospitalisation rates for people with dementia range from 0.37 to 1.26 per person per year in high-quality studies, with a 1.42 times higher risk compared with people without dementia, adjusted for age, sex and physical comorbidity.16 The most common causes for admissions in people with dementia are older age, multimorbidity, polypharmacy and a lower level of functional ability.16 Besides those, falls, infections, malnutrition, dehydration, chronic diseases (eg, heart failure, ischaemic heart disease) and BPSD are considered common causes.16–21 Hospitalisation often has negative effects on people with dementia, such as BPSD and declines in physical and cognitive function. Hospitalisation also poses a higher risk for: delirium, falls, dehydration, malnutrition, procedure-related complications, infections, death in hospital, nursing home admission and long length of hospital stay.22–25 Beyond that, the hospitalisation of people with dementia is also a burden on family members and nursing staff.24 26 Furthermore, the economic burden of hospitalisation is approximately 3 times greater for people with dementia compared with people without dementia due to the special needs of people with dementia and a higher risk of complications.27–30 In summary, hospital admissions of people with dementia should be reduced with a focus on avoiding the unnecessary hospitalisation of patients with ambulatory care sensitive conditions (ACSCs).17
ACSCs are defined as health conditions for which hospitalisation can be avoided by addressing them effectively in ambulatory primary care, for example, cardiovascular diseases (eg, ischaemic heart disease, heart failure), diabetes, hypertension or chronic obstructive pulmonary disease and bronchitis.17 31 Overall, about 20%–28% of all hospital admissions of people with dementia are caused by ACSCs.23 29 31 32
Nevertheless, two systematic reviews found that there is currently no effective non-pharmacological intervention for reducing the risk of hospitalisation in people with dementia.33 34 Both reviews therefore postulated that there is an urgent need for research with the primary aim of reducing hospital admissions in people with dementia with explicit attempts to reduce the most common causes.33 34 Beyond this, WHO considers the education of all health professionals on the management of ACSCs to be one key aspect for reducing hospitalisation.31 Therefore, to close this existing research gap, the DemWG study addresses both the common causes of hospitalisation and the education of health professionals on the management of ACSCs, by means of a non-pharmacological complex intervention based on evidence-based interventions.
In line with the literature about common causes and interventions targeting hospitalisation,16 33 34 MAKS-mk+ (component C of the complex intervention), based on the modules ‘motor stimulation’ (m) and ‘cognition’ (k) of the evidence-based MAKS therapy,35 36 and on exercises for strengthen muscle and balance (+), derived from the evidence-based OTAGO exercise programme,37 38 focuses on BPSD and falls. Besides that also cognitive function, due to its association with risk of falling,39 40 and QoL, since it is considered as a primary objective in the care of people with dementia,41 are primarily addressed. The MAKS therapy has been shown to stabilise cognition and ADL, and reduce BPSD in people with mild cognitive impairment (MCI) and mild-to-moderate dementia in nursing homes and day care,35 36 42 whereas the OTAGO exercise programme for fall prevention is able to reduce the risk of falls in older adults.37 38
According to recommendations of WHO,31 two components (A and B) of the complex intervention focus on further education of health professionals on ACSCs.
We also decided to include people with MCI due to several reasons: MCI, defined as a cognitive impairment exceeding what would be expected for the individual’s age and level of education (score below 24 in the Montreal Cognitive Assessment (MoCA)),43 44 but without impairments in ADL, represents an early stage of Alzheimer-type dementia in many cases (conversion of 72% from MCI to dementia in 5-year follow-up).45 46 Beyond that, a previous study has shown that people with MCI could benefit from the non-pharmacological MAKS therapy.35
The objective of the present paper is to describe the study protocol of the DemWG study (‘Demenz’-‘WohnGemeinschaft’; in English ‘dementia’-‘shared-housing arrangement’), following the evidence-based reporting guidelines of the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement.47
Aims and hypotheses
The main aim of the DemWG study, which began in April 2019, is to investigate whether a complex intervention is effective in reducing hospital admissions, BPSD and falls and for stabilising the cognitive functioning and QoL in people with dementia and MCI in German SHAs.
Primary hypothesis
The complex intervention of the DemWG study will lead to a reduction in hospital admissions in the intervention group compared with the control group (‘treatment as usual’).
Secondary hypotheses
The complex intervention of the DemWG study will reduce BPSD in the intervention group compared with the control group.
The complex intervention of the DemWG study will reduce falls in the intervention group compared with the control group.
The complex intervention of the DemWG study will stabilise cognitive functioning in the intervention group compared with the control group.
The complex intervention of the DemWG study will stabilise the QoL in the intervention group compared with the control group.
Methods and analysis
Study design and setting
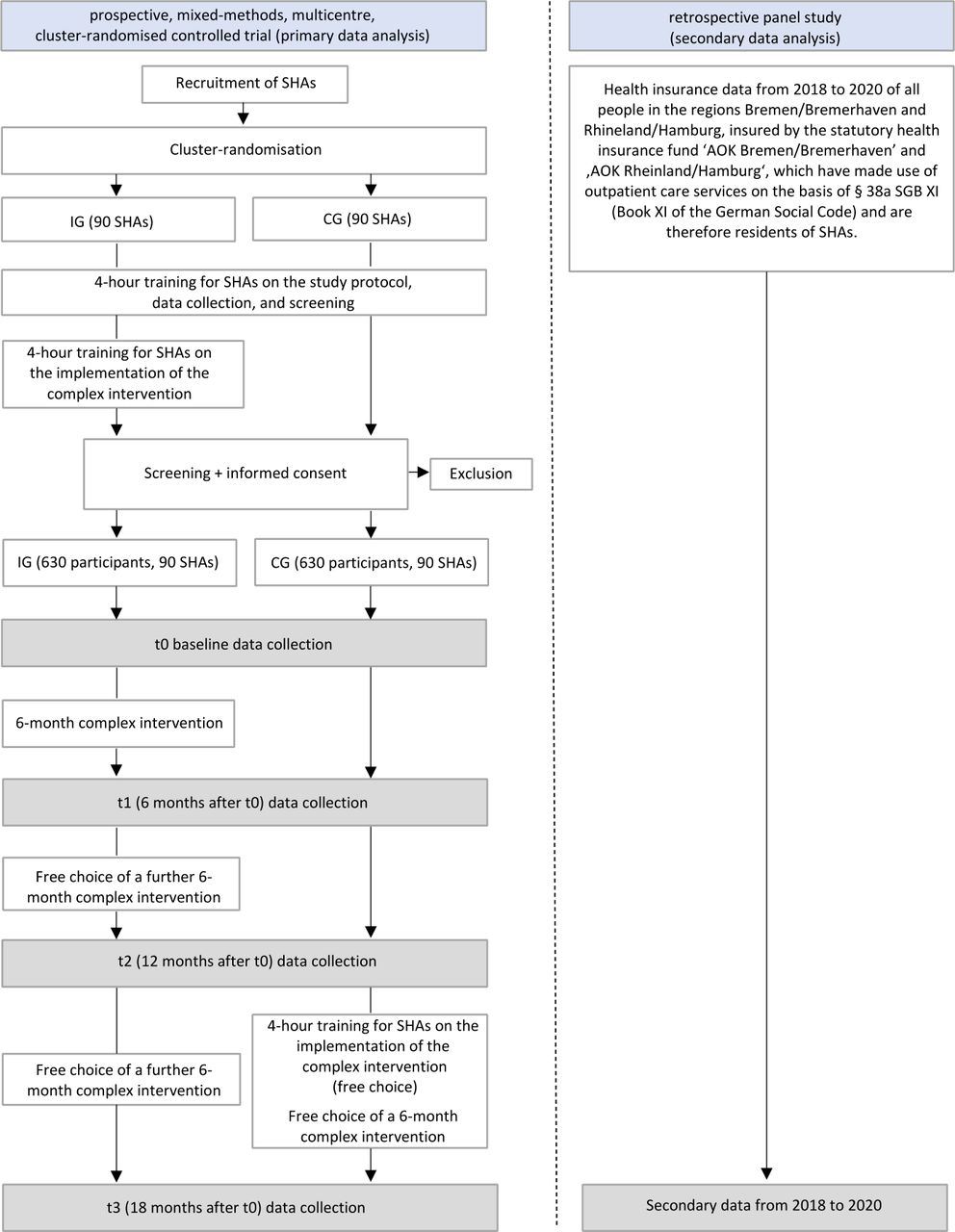
The study’s procedure is based on the UK Medical Research Council (MRC) framework ‘Developing and evaluating complex interventions’.48 49 Hence, a mixed-methods study combining primary and secondary data analyses and quantitative and qualitative research methods is being conducted. Figure 1 illustrates the entire study design.

Entire study design of the DemWG study. CG, control group; IG, intervention group; SHAs, shared-housing arrangements.
The study was prospectively registered on 16 July 2019 at ISRCTN registry (ISRCTN89825211). Table 1 shows the trial registration data set in accordance with recommendations of the SPIRIT statement.47
Trial registration data set of the DemWG study
The complex intervention of the DemWG study
Prospective, mixed-methods, multicentre, cluster-randomised controlled trial
The main part of the DemWG study is a prospective, mixed-methods, multicentre, cluster-randomised controlled trial with a waitlist control group design and longitudinal data acquisition.
All SHAs participating in the study (clusters) are recruited in all federal states of Germany, whereas the core study regions are Bavaria, Berlin, Bremen and Hamburg, since the two study headquarters are located in Bavaria and Bremen. The allocation to intervention and control group is determined by stratified cluster randomisation, which is an appropriate method for evaluating complex interventions in everyday practice in entire facilities.48 50 The clusters are randomly assigned to the intervention group and control group before baseline, stratified by the German federal states and type of setting (rural vs urban).51 Randomisation and allocation are performed externally by the Competence Center for Clinical Trials Bremen (KKSB, ‘Kompetenzzentrum für Klinische Studien Bremen’) with a computer-based system.
All SHAs are informed about their group allocation in written form by the study headquarters before the study team trains at least two people (usually nursing staff, occasionally volunteer assistants). This training consists of a 4-hour training on the study protocol, data collection and screening process, including a presentation of the central elements of the DemWG study, and active participation of the trainees in form of trial runs of screening and data collection. Only the SHAs in the intervention group receive an additional 4-hour training on the implementation of the multicomponent, non-pharmacological group intervention MAKS-mk+ (component C of the complex intervention) by a research associate of the study headquarters for at least two people in each SHA (usually nursing staff, occasionally volunteer assistants) who are not involved in screening or data collection. This training consists of a presentation of the central elements of MAKS-mk+ as well as active participation of the trainees in form of role plays regarding an exemplary MAKS-mk+ session. Detailed written instructions and manuals enable further dissemination of both 4-hour trainings to other nursing staff who cannot attend the 4-hour trainings. All participating SHAs receive financial compensation for data collection, screening and implementation of the MAKS-mk+ intervention.
Afterwards, during the 6-month intervention phase, the SHAs in the intervention group receive component A and B (further education of nursing staff and general practitioners) of the complex intervention and are carrying out component C (MAKS-mk+). The SHAs in the CG do not receive project-specific treatment but continue ‘treatment as usual’.
For ethical reasons, 12 months after baseline, the SHAs in the CG also receive the complex intervention and the associated 4-hour training on the implementation of the multicomponent, non-pharmacological group intervention MAKS-mk+ by free choice.
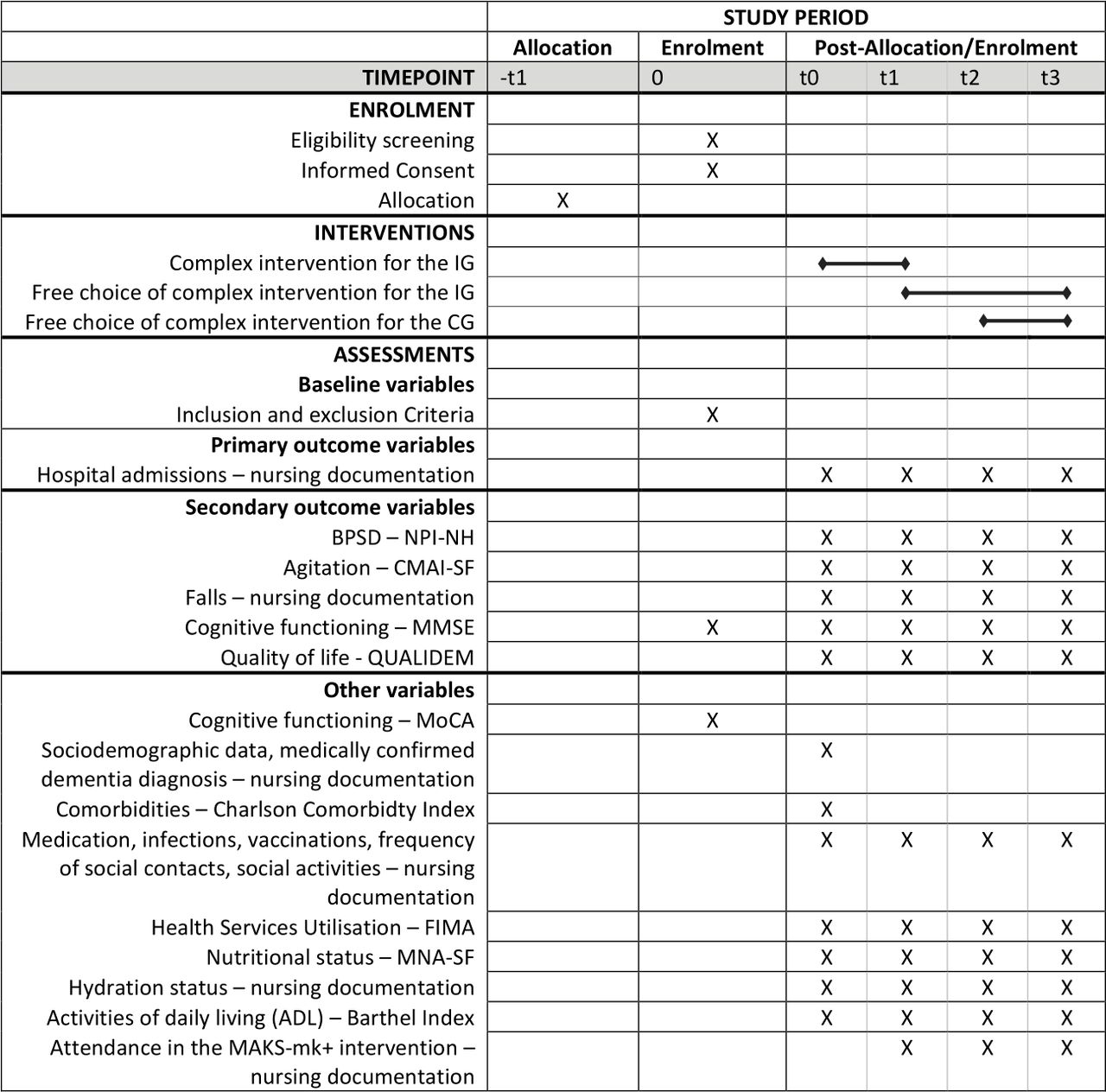
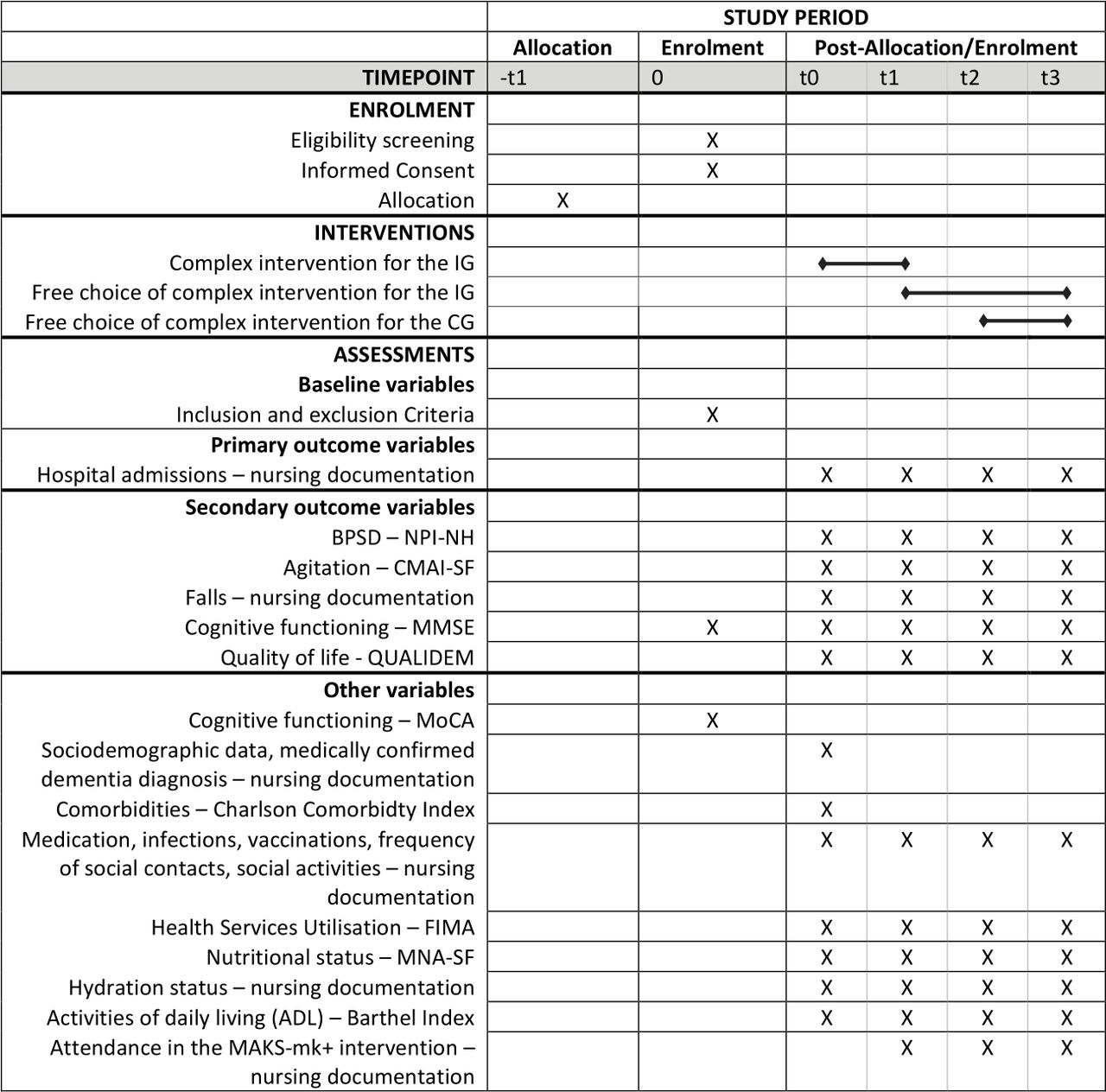
The follow-up period is 18 months with a total of four data collection points—baseline and after 6, 12 and 18 months. First baseline assessments are scheduled for June 2020, and the first SHAs are starting the intervention after the first round of data are collected in July 2020. The SPIRIT participant timeline is presented in figure 2.
{kind=link}
{kind=link}
Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) participant timeline of the prospective, mixed-methods, multicentre, cluster-randomised controlled trial. BPSD, behavioural and psychological symptoms of dementia; CG, control group; CMAI-SF, Cohen-Mansfield Agitation Inventory-Short Form; FIMA, Fragebogen zur Inanspruchnahme medizinischer und nicht-medizinischer Versorgungsleistungen im Alter (‘questionnaire for the use of medical and non-medical services in old age’); IG, intervention group; MMSE, Mini-Mental State Examination; MNA-SF, Mini Nutritional Assessment-Short Form; MoCA, Montreal Cognitive Assessment; NPI-NH, Neuropsychiatric Inventory-Nursing Home Version; SHAs, shared-housing arrangements.
In addition, following the MRC’s recommendations,49 52 qualitative methods, that is, expert interviews and focus groups, during and after the implementation of the intervention will be conducted in order to evaluate the processes involved in implementing the complex intervention. They intend in particular to reveal further-reaching connections between conditions and reasons for the success or failure of reducing the risk of hospitalisation that cannot be assessed by means of quantitative methods. In this way, the complex intervention is illuminated from a subjectively reconstructive perspective and possible further questions can be generated from the discussions with experts. The topics of the expert interviews and focus groups are: attitudes towards intervention trials and health services research, taking into account barriers and facilitators; examination of the current practice of management of ACSCs; communication and cooperation in SHAs, especially with general practitioners; medical care delivered by general practitioners; feasibility of long-term implementation of interventions such as MAKS-mk+ in SHAs, taking into account barriers and facilitators; awareness of the economic, social and health consequences of frequent hospitalisation. These research questions may be supplemented and further detailed in the course of the project, as new expanding questions may arise. Four to six expert interviews and at least one focus group per region are planned in each of the four core study regions (Bavaria, Berlin, Bremen, Hamburg). Beyond that, qualitative methods for process evaluation are accompanied by quantitative methods: nursing staff of each SHA is asked to rate the feasibility of implementation and the subjectively perceived efficacy after the 6-month intervention period by means of a self-developed questionnaire.
Since we are investigating a complex non-pharmacological intervention addressing multiple actors, neither the trained professionals nor the participants are blinded. However, it is often not possible to conceal group allocation in complex and non-pharmacological interventions and in cluster-randomised controlled trials.50 52
Retrospective panel study
The DemWG study also includes a retrospective panel study analysing secondary data that are independent and not linked to the primary data collected in the cluster-randomised controlled trial. The purpose is to estimate the financial costs of hospital admissions of people with dementia and MCI living in SHAs, using anonymised health insurance data from 2018 to 2020. These average costs offer an indication of the maximum financial amount that could be saved by reducing hospital admissions in SHAs. The sample consists of all people in the Bremen/Bremerhaven and Rhineland/Hamburg regions insured by the German statutory health insurance funds ‘AOK Bremen/Bremerhaven’ and ‘AOK Rheinland/Hamburg’, who used outpatient care services on the basis of § 38a SGB XI (Book XI of the German Social Code) and are therefore residents of SHAs.
Sample size estimation
An a priori power analysis that was based on the primary outcome (hospital admissions) and the authors’ experiences in previous studies in the field of SHAs was computed.12 13 53 The calculation was based on an alpha error of 5%, a statistical power of 80% and an intraclass correlation coefficient of 0.017, estimated from data from a previous study on German SHAs.53
Regarding hospital admissions, a frequency of 9.4% is expected for the control group, taking into account previous research in German SHAs.53 The DemWG study aims to halve the number of hospital admissions, which means a 5% reduction in hospital admissions in the intervention group. Therefore, 840 participants from 120 SHAs (60 SHAs each in the intervention group and control group, based on the assumption of 7 participants per SHA), have to be included in the study.
Despite an average of 8 and a maximum of 12 residents per SHA in Germany,11–13 it can be assumed that not every person living in the SHAs will be eligible or will consent to participate in the study. Furthermore, results from a previous study in German SHAs suggest that about 30% of participants in SHAs will no longer participate after 1 year of study participation.53 Therefore, an over-recruitment of 50% is the goal, with a total of 1260 participants from 180 SHAs (90 SHAs each for the intervention group and control group).
Recruitment strategies
In order to reach the target number of 180 SHAs, we initially planned to recruit 120 SHAs in Berlin, 35 in Bavaria, 15 in Bremen and 10 in Hamburg, because about 690 SHAs are located in Berlin, 363 in Bavaria, 42 in Bremen and 35 in Hamburg.9 54 The recruitment of SHAs began in July 2019, whereas the recruitment of participants in SHAs started on 1 January 2020. The interest in study participation in Berlin was low, especially due to a shortage of personnel, participation in other research projects or internal changes (especially digitisation or the current establishment of further SHAs). Thus, we extended the recruitment region to the remaining federal states of Germany, and the recruitment period until 31 December 2020.
SHAs and their outpatient care services are identified by means of their websites or entries in information systems and databases. In addition, written information is sent to ministries and authorities of the different federal states, the local German Alzheimer’s Societies and nursing care bases (‘Pflegestützpunkte’) with a request to forward it to SHAs.
All identified SHAs receive written information about the project. If SHAs are interested, a telephone interview is conducted in order to exclude SHAs with a focus on intensive care, mental disorders, disability or neurological disease and to clarify whether the interested SHA has at least about three people with dementia or MCI who are able to participate in the planned complex intervention. A cooperation contract is signed with SHAs that meet the inclusion criteria described above and decide to participate in the study. Recruitment ends after the contract with the 180th SHA has been signed or on 31 December 2020.
Eligibility of participants
The screening and enrolment process is conducted by people working in SHAs (usually nursing staff, occasionally volunteer assistants) who were trained in a 4-hour training by a research associate of the study headquarters. All residents of each participating SHA are included in the screening process. In the first step, all residents fulfilling at least one of the exclusion criteria, described in table 1, are excluded. We decided to exclude people with severe dementia, since previous studies have shown that people with mild-to-moderate dementia and MCI, but not severe dementia, could benefit from the MAKS therapy,35 36 on which parts of the complex intervention of the DemWG study are based on. In the second step, the German versions of the Mini-Mental State Examination (MMSE)55 56 and the MoCA57 are administered to screen residents of SHAs for mild-to-moderate dementia and MCI. First, the MMSE is administered with a cut-off score of below 24 indicating dementia.58 59 The MMSE has a low sensitivity for detecting MCI.44 57 60 61 Therefore, when MMSE values range from 24 to 30, the MoCA is also administered with a cut-off score of below 24 points indicating MCI.43 44
Intervention
Development of the complex intervention of the DemWG study
The development of the complex intervention of the DemWG study followed the MRC’s recommendations.48 At first, a theoretical basis for the planned intervention based on empirical evidence in the literature on non-pharmacological interventions for reducing hospitalisation has been established: according to two systematic reviews and suggestions of WHO, the common reasons of hospitalisation as well as the management of ACSCs should be addressed.31 33 34
Afterwards, qualitative expert interviews and focus groups have been conducted with professional caregivers, operators of SHAs, general practitioners and other experts in the field of SHAs or scientists in the field of health services research, in order to define relevant intervention components and mechanisms, or to find potential barriers. The expert interviews and focus groups showed that relevant complex intervention components should be awareness raising measures for both general practitioners and nursing staff, and further education of general practitioners and nursing staff on ACSCs. Beyond that, evidence-based non-pharmacological interventions for people with dementia and MCI addressing falls, cognitive functioning, BPSD and QoL were also considered highly relevant. Potential barriers that were identified were costs, time capacities and reservations against research. Therefore, these aspects were explicitly taken into account in the development of the intervention and addressed in the recruitment interviews with the SHAs.
After developing the initial version of the intervention, the feasibility of delivering the intervention and acceptability to providers has been tested through several pretests of the intervention components in the respective settings. The pretests included peer review of the continuing medical education (CME) article for general practitioners before publication, and proof-reading of the education for nursing staff by an examined nurse. Since MAKS-mk+ is based on evidence-based interventions, no further pretests were needed. Beyond that, further qualitative expert interviews and focus groups with appropriate experts showed that there were no need for further amendments of the complex intervention.
The complex intervention of the DemWG study
The final complex intervention consists of three components: (A) education of nursing staff and other people working in SHAs by means of an information brochure; (B) awareness raising and CME of general practitioners by means of a CME-certified article, published in a peer-reviewed scientific journal62; (C) the multicomponent non-pharmacological group intervention MAKS-mk+ for people with dementia and MCI, consisting of the modules ‘motor training’ (m) and ‘cognitive training’ (k) of the evidence-based MAKS therapy,35 36 and exercises to strengthen muscles and balance (+) of the evidence-based OTAGO exercise programme for fall prevention.37 38
Components A and B of the complex intervention primarily address the management of ACSCs. In particular, an interaction between A and B is intended, since both encourage further communication between general practitioners and nursing staff. Component C (MAKS-mk+) focusses explicitly on cognitive functioning, BPSD, falls and QoL. Table 2 provides detailed information on all intervention components. To ensure that the further education of both nursing staff and general practitioners will be read, both are asked to fill out a reflection sheet and send it to the study headquarters. In addition, the amount of completed CMEs can be retrieved from the journal via the individual access key send out to general practitioners. An example weekly plan for MAKS-mk+ (component C of the complex intervention) is shown in table 3. The project does not exert any influence on pharmacological treatment or individual participation in other activities.
Example of a weekly plan for the MAKS-mk+ intervention (component C of the complex intervention of the DemWG study)
Measures
Primary outcome measure
The primary outcome hospital admissions is obtained by nursing documentation of the outpatient care services providing 24-hour care in the SHAs. The primary outcome covers all-cause hospitalisation, that is, planned as well as unplanned admission, admission to an emergency department and discharge back to the SHA at the same day. In addition to the frequency in the last 6 months, the duration (dates of admission and discharge), the specific reason, whether it was unplanned (acute) or planned and the discharge code of each hospital admission are recorded. Since nursing documentation is regularly controlled by external authorities, the primary outcome extraction should be complete and valid.
Secondary outcome measures
BPSD are assessed with the German version of the Neuropsychiatric Inventory-Nursing Home Version (NPI-NH).63 64 The NPI-NH was derived from the Neuropsychiatric Inventory (NPI),65 one of the most commonly used instruments for assessing BPSD.66 67 It is a proxy-based instrument for assessing the frequency (1–4) and severity (1–3) of 12 common BPSD: ‘delusions’, ‘hallucinations’, ‘agitation’, ‘depression’, ‘anxiety’, ‘apathy’, ‘irritability’, ‘euphoria’, ‘disinhibition’, ‘aberrant motor behaviour’, ‘sleep and night-time behaviour disorders’ and ‘appetite and eating disorders’. The total score, which ranges from 0 to 144, is obtained by adding symptom scores (frequency×severity). Higher scores indicate more pronounced BPSD. Validity and reliability has been established.64 66 68 69
Additionally, agitation is measured using a forward-backward German translation of the Cohen-Mansfield Agitation Inventory-Short Form (CMAI-SF),70 a proxy-based instrument that consists of 14 agitated behaviours of the original 29-item CMAI.71 The CMAI is one of the most widely used instruments for assessing agitation in people with dementia.72 The frequency of each item should be rated on a 5-point scale (1–5), with a total score ranging from 14 to 70. Higher scores indicate more pronounced agitation. The reliability and validity of the CMAI has been established in several studies.69 71 73
Falls are obtained from nursing documentation. In addition to the frequency in the last 6 months, the fall-related consequence of each fall (ie, no treatment necessary; medical outpatient treatment necessary; medical inpatient treatment necessary) is also recorded.
Cognitive function is measured with the German version of the MMSE,55 56 the most widely used cognitive screening test for dementia.74 75 It is a psychometric performance test assessing the following five areas of cognitive function: ‘orientation’, ‘memory’, ‘registration’, ‘attention’, ‘calculation’, ‘recall’, ‘language’ and ‘ability to draw a complex polygon’. Scores range from 1 to 30, with lower scores indicating lower cognitive abilities. The reliability and validity of the MMSE has been established in numerous studies.58 59 75
QoL is measured using the German 37-item version of the dementia-specific proxy-based QoL instrument QUALIDEM.76 77 QoL is assessed on the basis of 37 items covering the following nine dimensions of QoL (subscales): ‘care relationship’ (seven items), ‘positive affect’ (six items), ‘negative affect’ (three items), ‘restless tense behaviour’ (three items), ‘positive self-image’ (three items), ‘social relations’ (six items), ‘social isolation’ (three items), ‘feeling at home’ (four items), ‘having something to do’ (two items). All items should be rated on a 7-point scale (0–6, ranging from ‘never’ to ‘very frequently’) regarding observed behaviour in the past week. The global score is calculated by adding and transforming scores into values that range from 0 to 100.78 Higher scores indicate a better QoL. Reliability and validity has been confirmed.76 77 79–82
Other measures
The German version of the MoCA is administered solely in the screening process to screen for MCI.57 The score ranges from 0 to 30, with lower scores indicating lower cognitive abilities. The MoCA is a commonly used, extensively validated, and a reliable screening tool for MCI.43 60
Sociodemographic data, the presence of a clinically confirmed dementia diagnosis as well as infections, prescribed medication, vaccinations, frequency of social contacts, attendance at the MAKS-mk+ intervention and other social activities within the last 6 months are obtained from nursing documentation.
Comorbidities are measured using the updated Charlson Comorbidity Index (CCI) by Quan et al.83 By weighting 12 medical diagnoses according to their mortality-associated severity, the total score ranges from 0 to 24. Higher scores indicate an increased 1-year mortality. The validity and reliability of the CCI has been confirmed.83–86
Health Services Utilisation within the past 6 months is measured using the German questionnaire for the use of medical and non-medical services in old age (FIMA).87 Besides the utilisation (yes/no), frequency is also assessed. The reliability and validity of the FIMA has been confirmed.88
Nutritional status is measured with the German version of the Mini Nutritional Assessment-Short Form (MNA-SF),89–91 one of the most widely used nutrition screening tools.91 92 The total score ranges from 0 to 14, with higher scores indicating better nutritional status.89 Reliability and validity has been confirmed.89 91 92
In addition, hydration status is measured using a self-developed rating of whether the participant drinks an average of ‘less than three glasses’, ‘three to five glasses’, ‘more than five glasses’ of alcohol-free beverages a day. The rating is based on nursing documentation.
ADL are measured using the German version of the Barthel Index.93 94 It is a widely used, reliable and valid instrument for assessing ADL capabilities and consists of 10 items with a total score ranging from 0 to 20.93–95 Higher scores indicate better ADL capabilities.
In addition, data regarding the structure and concept of each SHA (eg, number of residents; integrative vs segregative SHA; medical and therapeutic care by general practitioners; qualification of nursing staff and other people working in the respective SHA; specific dementia concepts) are obtained at 6-month follow-up with a self-developed questionnaire.
Data collection
Data are collected by the same trained individuals from the SHAs (usually nursing staff, occasionally volunteer assistants) conducting the screening who are not involved in carrying out the MAKS-mk+ intervention. If participants are no longer able to participate in the complex intervention, but are still residents of the SHAs and willing to participate in the study, data collection is continued. All data are collected in written form. After completion, paper case report forms (CRFs) are sent to the data monitoring committee at the KKSB.
Data quality management
The quality of data is guaranteed by our data monitoring committee at the KKSB across the entire period of data collection. Pseudonymised paper CRFs are read into the database automatically by software. Nevertheless, the data are subjected to ongoing plausibility checks regarding completeness, range and consistency over the entire study period. In the case of ambiguities, SHAs are contacted for clarification. All changes to the data are documented via an internal audit trail.
The key list for pseudonymisation is stored in a separate office in a locked steel cabinet to which only two individuals from the KKSB (‘trust authority’) have access. Electronic data are stored on encrypted hard disks within the KKSB’s internal network. This network is protected against unauthorised access from the outside through multiple measures in accordance with §64 of the German Federal Data Protection Act. Paper CRFs are stored in a separate office in a locked steel cabinet. The availability of data is ensured by several electronic backup measures.
Data analysis
Researchers at the study headquarters in collaboration with the KKSB (responsible for primary data analysis) and the SOCIUM Research Center of the University of Bremen (responsible for secondary data analysis) will analyse the data.
Primary data analysis
Most of the data analyses will be performed predominantly with the ‘IBM SPSS Statistics’ and the ‘SAS’ software. A missing data evaluation will be carried out, and missing metric values will be imputed by the expectation maximisation algorithm.96 The quality of the randomisation, that is, balanced parameters between both groups, will be assessed by examining the baseline data for statistically significant differences between the intervention group and control group (pretest equivalence). A drop-out analysis will be performed to compare differences between the drop-outs and the remaining participants. In line with international guidelines, the primary population for analysis is the intention-to-treat (ITT) sample.97 98 To assess the robustness of results, analyses are also computed with the per-protocol (PP) sample. If there is any discrepancy between ITT and PP study findings, possible reasons will be discussed.
The primary and secondary hypotheses will be tested by calculating multivariate analyses according to the general linear model. Beyond that, exploratory subgroup analyses and adjusted analyses controlling for potential confounding variables will be conducted.
Focus groups and expert interviews will be recorded on dedicated recording devices and transcribed. Qualitative data from expert interviews and focus groups will be analysed using qualitative content analysis, for example, summarising content analysis according to Mayring,99 since this is one of the most frequently used qualitative methods for text analysis, and useful if the content level of the data material is in the foreground: by reducing the material according to this approach, essential content is retained and a short manageable text can be generated.99–101
Secondary data analysis
For the evaluation of anonymised health insurance data from 2018 to 2020, the insured person’s time from 2018 to 2020 will be split into several episodes according to the following variables: need for long-term care, care level, dementia/MCI diagnosis, living in a SHA. Hospital admissions and costs will then be assigned to these episodes according to the day of admission. The final average total sum of hospital admission costs within 1 year will be estimated by weighting the determined values by the distributions of age and gender in the population of Germany.102
Patient and public involvement
The patients and the public were not involved in the development of hypotheses or design of the study. Nevertheless, interviews and focus groups with experts and stakeholders of the project (ie, local German Alzheimer’s societies, professional caregivers, operators of SHAs, general practitioners and statutory health insurance representatives) are organised to obtain advice on recruitment strategies, development of the intervention, implementation and dissemination of the results. The outcome measures are predominantly proxy-based, widely used and validated for application in our study population. Patient recruitment, screening, data collection and implementation of the MAKS-mk+ intervention is carried out by trained individuals from the SHAs (usually nursing staff, occasionally volunteer assistants), which receive financial compensation. These individuals are asked to rate the feasibility of the implementation and the subjectively perceived efficacy after the 6-month intervention period by means of a self-developed questionnaire. To improve adherence to the entire study, all participating SHAs are informed about the study process and the following steps in monthly newsletters.
Ethics and dissemination
All procedures have been approved by the Ethics Committee of the University of Bremen (Ref. 2019-18-06-3). Participation is voluntary, and participants are free to leave the study at any time without suffering any disadvantages. Before conducting the screening tests (MMSE, MoCA), each resident or, if applicable, the legal guardian is asked for verbal consent. All residents of SHAs fulfilling the criteria for inclusion after the screening receive detailed personal and written standardised information about the study and are informed according to the European Union data protection legislation and the corresponding German equivalent (DSGVO) by trained individuals from the SHAs (usually nursing staff, occasionally volunteer assistants). If a resident has a legal guardian, this person is also informed. In case of willingness to participate, a written informed consent of the resident or, if applicable, the legal guardian is being obtained. Only residents signing an informed consent form are enroled as participants of the DemWG study.
Due to findings from previous randomised controlled trials,35 36 38 serious adverse events are not expected. Thus, no stopping guidelines have to be defined.
Results from this study will be published in open-access, peer-reviewed scientific journals and will be presented at scientific conferences. For further details on data sharing, please see our data availability statement in our trial registry at ISRCTN.
In the case of important protocol modifications, we will update the trial registry and inform the Ethics Committee of the University of Bremen, the funder and the cooperating SHAs.
Acknowledgments
The authors would like to thank the Innovation Committee at the Federal Joint Committee (‘Innovationsausschuss beim Gemeinsamen Bundesausschuss’) for their financial support of the study. The authors would like to thank all cooperating SHAs and all study participants who will be providing data. The authors acknowledge the support provided by the German Research Foundation (DFG, ‘Deutsche Forschungsgemeinschaft’) and the Friedrich-Alexander University Erlangen-Nürnberg in the funding programme Open Access Publishing. The authors would like to thank the cooperation partners for their expertise and support: Competence Centre for Clinical Trials Bremen (KKSB, ‘Kompetenzzentrum für Klinische Studien Bremen’), especially Professor Dr Werner Brannath; SOCIUM Research Centre on Inequality and Social Policy of the University of Bremen, especially Professor Dr Heinz Rothgang; Nuremberg Institute of Technology (‘Technische Hochschule Nürnberg Georg Simon Ohm’) and genesis Systems gGmbH, especially Professor Dr Helmut Herold, Professor Dr Ethelbert Hörmann and Dipl.-Ing. (FH) Wolfgang Bergmann; ‘AOK Bremen/Bremerhaven’; ‘AOK Bayern’, especially Katrin Einhell, Alexander Günter and Margit Hermann; ‘AOK Rheinland/Hamburg’; Bavarian Association of Statutory Health Insurance Physicians (KVB, ‘Kassenärztliche Vereinigung Bayerns’), especially Dr Martin Tauscher and Dr Roman Gerlach; Bavarian Health and Food Safety Authority (LGL, ‘Bayerisches Landesamt für Gesundheit und Lebensmittelsicherheit’), especially Dr Julia Berendt; Institute for Biomedicine of Ageing (IBA) of the Friedrich-Alexander University Erlangen-Nürnberg, especially PD Dr Ellen Freiberger; Innovation of Learning Institute (ILI) of the Friedrich-Alexander University Erlangen-Nürnberg; German Alzheimer Society (‘Deutsche Alzheimer Gesellschaft e.V.’); ‘Koordinationsstelle ambulant betreute Wohngemeinschaften in Bayern’; ‘Anbieter-Verband qualitätsorientierter Gesundheitspflegeeinrichtungen e.V.’; ‘die ambulante PFLEGE Bremer Heimstiftung’; ‘Evangelischer Verband für Altenarbeit und pflegerische Dienste’; ‘Hamburger Koordinierungsstelle für Wohn-Pflege-Gemeinschaften STATTBAU’. The authors would like to thank ‘imbus AG’, ‘infoteam Software AG’, ‘ISO Professional Services GmbH’, ‘Lions Club Nürnberg Lug-ins-Land’, ‘Lions Club Bremen Unterweser’, ‘sepp.med GmbH’, ‘Siemens Healthineers AG’, ‘TRS – Technology Refresh Services AG’ for providing the necessary hardware (laptops and computers) to carry out the multicomponent non-pharmacological group intervention MAKS-mk+ in the participating SHAs. The authors would also like to thank the English-language editor, Dr Jane Zagorski. The present work was performed in partial fulfilment of the requirements for obtaining the degree ‘Dr. rer. biol. hum.’ at the Faculty of Medicine of the Friedrich-Alexander University Erlangen-Nürnberg (FAU) by André Kratzer (AK).
References
Footnotes
Contributors AK drafted the manuscript. AK, JS, KW-O, AS, KR, CD and EG are responsible for the conception and design of the study. JS, KW-O, AS, KR, CD and EG made substantial contributions to the manuscript and substantively and critically revised it. AK, JS, CD and EG developed the non-pharmacological group intervention MAKS-mk+ and the continuing medical education (CME) of general practitioners. KW-O, AS and KR developed the education of the nursing staff and other people working in shared-housing arrangements. All authors have read and approved the final version of the manuscript. All authors have agreed to be personally accountable for all aspects of the work and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated and resolved.
Funding The DemWG study is supported by grants from the German Innovation Committee at the Federal Joint Committee (‘Innovationsausschuss beim Gemeinsamen Bundesausschuss’, Gutenbergstraße 13, 10587 Berlin) with General Project Administration by the DLR Project Management Agency (‘DLR Projektträger’; Address: Heinrich-Konen-Straße 1, 53227 Bonn; Phone:+49 228 3821–1020, email: innovationsfonds-versorgungsforschung@dlr.de), grant number: 01VSF18054. The study protocol has been reviewed by the funding body.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Methods and analysis' section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.