Article Text

Abstract
Introduction Although physical activity (PA) reduces cardiovascular disease (CVD) risk, physical inactivity remains a pressing public health concern, especially among African American (AA) women in the USA. PA interventions focused on AA women living in resource-limited communities with scarce PA infrastructure are needed. Mobile health (mHealth) technology can increase access to PA interventions. We describe the development of a clinical protocol for a multilevel, community-based, mHealth PA intervention for AA women.
Methods and analysis An mHealth intervention targeting AA women living in resource-limited Washington, DC communities was developed based on the socioecological framework for PA. Over 6 months, we will use a Sequential Multi-Assignment, Randomized Trial approach to compare the effects on PA of location-based remote messaging (named ‘tailored-to-place’) to standard remote messaging in an mHealth intervention. Participants will be randomised to a remote messaging intervention for 3 months, at which point the intervention strategy will adapt based on individuals’ PA levels. Those who do not meet the PA goal will be rerandomised to more intensive treatment. Participants will be followed for another 3 months to determine the contribution of each mHealth intervention to PA level. This protocol will use novel statistical approaches to account for the adaptive strategy. Finally, effects of PA changes on CVD risk biomarkers will be characterised.
Ethics and dissemination This protocol has been developed in partnership with a Washington, DC-area community advisory board to ensure feasibility and acceptability to community members. The National Institutes of Health Intramural IRB approved this research and the National Heart, Lung, and Blood Institute provided funding. Once published, results of this work will be disseminated to community members through presentations at community advisory board meetings and our quarterly newsletter.
Trial registration number NCT03288207.
- protocols & guidelines
- health informatics
- cardiology
- public health
- social medicine
- statistics & research methods
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- protocols & guidelines
- health informatics
- cardiology
- public health
- social medicine
- statistics & research methods
Strengths and limitations of this study
Community partnerships and a strong foundation of preliminary community-based participatory research studies establish trust and collaboration with the community, which are essential for acceptance and success of the community-based physical activity intervention.
This multilevel, technology-enabled approach to increase physical activity (PA) targets both individual motivations and barriers as well as neighbourhood resource utilisation.
As an adaptive behavioural intervention, PA goals are determined based on each participants’ individual baseline and adapt over time according to participants’ response.
This study assesses both clinical measures (body mass index, blood pressure, lipid profile, glucose levels, smoking status) and biological cardiovascular health mediators (metabolic, lipid and inflammatory pathways).
The statistical power is based on the primary objective to evaluate effects of tailored-to-place and standard remote messaging on PA; analysis is underpowered to evaluate changes in cardiovascular risk markers, but exploratory analyses will evaluate potential trends.
Introduction
The ubiquity of smartphone use presents an opportunity to expand mobile health (mHealth)-based cardiovascular interventions, including those focused on physical activity (PA), to broad community populations.1 A growing body of evidence suggests that mHealth technology-enabled interventions use text messaging, internet platforms or mobile applications (apps) to effectively promote PA, reduce sedentary behaviour and improve cardiovascular health.2–9 However, existing mHealth studies show conflicting results, are limited by small sample sizes, and focus on young, highly educated and high-income individuals.7 9 10 These samples do not reflect the populations at greatest risk for cardiovascular disease (CVD); research is needed to explore the utility of mHealth interventions within more diverse populations.
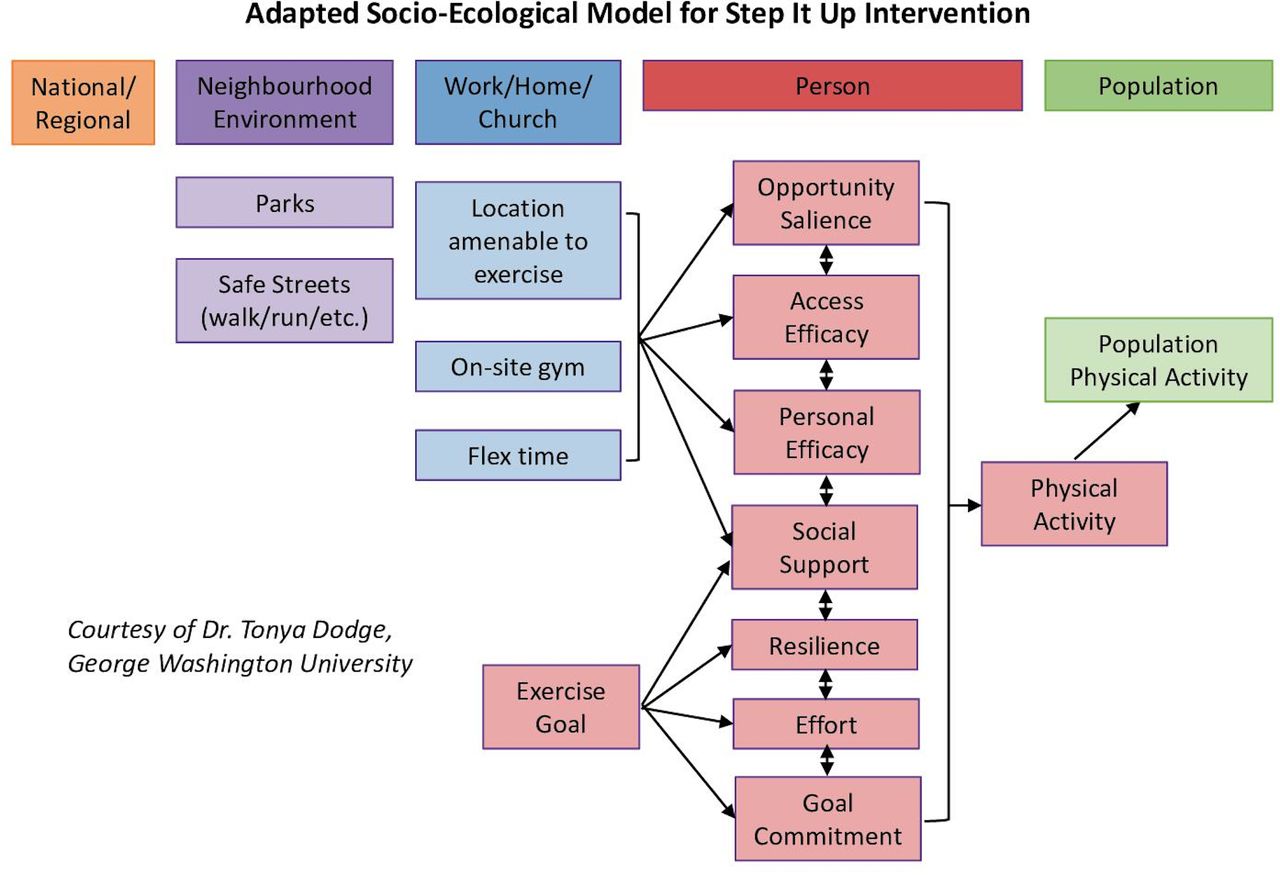
Among African American (AA) women, studies suggest that culturally appropriate interventions can effectively promote PA participation.11 12 CVD disproportionately impacts AAs, and PA reduces CVD risk.13 AA women, who more often live in resource-limited neighbourhoods, have higher rates of sedentary time than other racial/ethnic groups.14 15 According to the National Health Interview Survey 2018, 39.7% of AA women meet PA guidelines, compared with 43.8% of Hispanic women and 54.7% of White women.16 Interventions to increase PA can be made more effective by targeting multiple levels of a socioecological framework for PA, including individual, interpersonal and neighbourhood environment-level factors (figure 1).17 18 An important contributing factor to PA is the local built environment, including sidewalks, well-maintained parks, recreation centres and perceived safety.19–23 Lower socioeconomic status neighbourhoods have fewer PA facilities, and are less conducive to obtaining adequate PA.24 To create an effective behavioural health intervention to reduce CVD disparities, it is critical to partner with the target community, and develop culturally appropriate strategies to navigate the local built environment.11 12

Adapted socioecological model that accounts for various factors affecting an individual’s decision to engage in physical activity. Tailored-to-place messaging will focus on the neighbourhood environment and work/home/church levels of the socioecological model, while standard-remote messaging focuses on the person-level.
In this study, we introduce Step It Up, a community-based PA intervention targeting at-risk AA women residing in resource-limited communities in the Washington, DC metropolitan area. Community-based participatory research principles were used to partner with local community leaders and design a 6-month mHealth intervention aimed at increasing participants’ PA. We began with a health-and-needs assessment to determine feasibility of the intervention in our target population, followed by a pilot mHealth intervention tailored to the built environment of participants.25 26 The objective of this manuscript is to describe the study design and components, recruitment methods, proposed measurements, analysis plan, strengths and limitations.
Methods and analysis
Development of the Step It Up intervention: preliminary studies
Community engagement to design culturally appropriate interventions
Since beginning work in Washington, DC in 2013, our research team has sought to engage at-risk communities with limited access to resources for nutritious diet and PA. Washington, DC is divided into eight regions, called wards, for municipal purposes; our efforts focus on Washington, DC wards 5, 7, 8, and the contiguous Prince George’s County, Maryland (MD). These wards have the highest burden of CVD and lowest income in Washington, DC, with gentrification often pushing the population into Prince George’s County.27 28 These neighbourhoods also have fewer PA facilities compared with other parts the city, and 64%–91% of the population is AA.27 29 30
We established the DC Cardiovascular Health and Obesity Collaborative (DC CHOC), a community advisory board which includes representatives with expertise and/or interest in cardiovascular health from faith-based and community organisations.31 DC CHOC provides feedback on the development and implementation of all community-oriented projects, including Step It Up.32–34 We worked with DC CHOC to first determine the feasibility of using wearable technology to measure and promote PA in the community through the Washington, DC Cardiovascular Health and Needs Assessment (DC CHNA).34 Ninety-eight percent of participants recruited for the DC CHNA lived in Washington, DC Wards 5, 7, 8 or Prince George’s County, MD. Further, DC CHNA gave insight into setting an activity goal; evidence suggests that odds of all-cause mortality and metabolic syndrome are lowest in those taking >7500 steps/day, and 15 000 steps/day may maximise health benefits.35–37 From observations in DC CHNA, a goal of 10 000 steps/day was determined to be both feasible and beneficial. Incorporating community-based participatory research methods has helped to ensure our interventions are culturally appropriate and acceptable, increasing the likelihood of adoption.
Iterative user-centred development of Step It Up app
To optimise the app’s ability to facilitate improved health behaviours, end-user feedback was solicited from community focus groups (FGs) throughout the app development process.38 We worked with an app-development organisation (CHAI Core: Interventions, Chapel Hill, North Carolina, USA) to design an app that tracks PA levels by logging step counts, and provides users with culturally tailored motivational messages created in partnership with DC CHOC. We named the app ‘Step It Up’, in reference to the desired outcome of increasing the number of daily steps among participants.
Participants used this mobile phone app alongside a wearable PA tracker, the Fitbit Charge 2 (Fitbit, San Francisco, California, USA), for 20 days. Subsequently, FGs were conducted at a local partnering church to understand participants’ experiences using the app to overcome PA barriers and increase PA, described in previous work.38 These FG data were used to create a second iteration of the Step It Up app, subject to further user experience interviews and pilot testing. We learnt from one-on-one user experience interviews focused on wire-frame design that participants preferred bold colour schemes, audiovisual supplements such as instructional videos on stretching, and wanted an independent section for goal-setting and tracking progress. Users also felt this app could be used as a replacement or supplement to commercial fitness apps. This feedback was incorporated in a third iteration through a 21-day pilot, leading to development of the Step It Up app for the larger intervention.
Design and overview of Step It Up intervention
Sequential Multiple-Assignment Randomized Trial design
Our intervention uses a Sequential Multiple-Assignment Randomized Trial (SMART) design, a method for the development of rapid adaptive behavioural interventions.39 40 This method rerandomizes patients who have not reached the PA goal of 10 000 steps/day after 3 months to more intensive treatment (figure 2). SMART design investigates the impact of intensifying messaging on PA levels among initial non-responders.

Step It Up: A Sequential, Multiple-Assignment Randomised Trial targeting physical activity (PA) with standard and tailored remote messaging. Four intervention types are as follows: (1) TPM followed by TPM+face-to-face coaching, (2) TPM followed by TPM with increased messaging frequency, (3) SRM followed by SRM+face-to-face coaching, (4) SRM followed by TPM. Patients initially randomised to standard remote messaging (SRM) who do not reach goal of 10 000 steps/day by the end of 3 months will be rerandomised to receive tailored-to-place messaging (TPM) or SRM coupled with face-to-face coaching. Similarly, patients initially randomised to TPM who do not reach goal of 10 000 steps/day will be rerandomised to TPM supplemented with face-to-face coaching or increased messaging frequency. BMI, body mass index.
Objectives of Step It Up intervention
The primary objective of this study is to determine if a SMART-designed adaptive mHealth intervention with remote messaging tailored to neighbourhood-environment resources (ie, tailored-to-place messaging (TPM)) will increase PA (measured as steps/day) more than standard remote messaging (SRM) (figure 2). This PA intervention will target overweight/obese AA women at risk for cardiometabolic disease with insulin resistance in resource-limited neighbourhoods of the Washington, DC metropolitan area.
A secondary objective is to examine which of four embedded adaptive interventions produces the largest PA increase over the 6-month study period. The four interventions are as follows (figure 2):
Intervention 1
First 3 months: TPM.
Second 3 months: TPM+face-to-face coaching.
Intervention 2
First 3 months: TPM.
Second 3 months: TPM with increased message frequency.
Intervention 3
First 3 months: SRM.
Second 3 months: SRM+face-to-face coaching.
Intervention 4
First 3 months: SRM.
Second 3 months: TPM.
Other secondary objectives include evaluating the feasibility of mHealth technology for remote capture of cardiovascular measures, including blood pressure, weight and blood glucose. Intervention effects on clinical markers (table 1) and how behavioural and psychosocial factors mediate the relationship between PA change and cardiovascular health will also be examined. Finally, exploratory analyses will examine the impact of changes in PA levels on metabolic and inflammatory pathways using blood samples collected at baseline, 3 and 6 months.
Clinical measures and biological markers
This study will include (1) cardiometabolic screening and measurements, (2) administration of a detailed survey tailored by community input41 and (3) deployment of the Step It Up mobile app and handheld mHealth technology to promote increased PA.38 All participants will receive counselling and written information regarding steps to improve their dietary intake in accordance with the Dietary Approach to Stop Hypertension dietary pattern on study enrolment.42 Online supplemental table 1 summarises protocol design.
Supplemental material
Recruitment of participants
Inclusion criteria
Overweight or obese (body mass index (BMI) ≥25 kg/m2) AA women aged 25–75 years with evidence of insulin resistance based on fasting plasma glucose (100–125 mg/dL) or haemoglobin A1c (HgA1c=5.7%–6.4%) living in Washington, DC Wards 5, 7, 8 or Prince George’s County, MD are eligible. Participants must have access to a smartphone compatible with the Step It Up mobile app. Participants must be able to provide informed consent independently and speak and read English at or above an eighth grade level.
Exclusion criteria
Prospective participants with the following characteristics will be excluded: (1) medical condition, including recent unintentional weight loss, which might prohibit safe participation in this intervention; (2) existing self-reported diagnosis of diabetes mellitus; (3) fasting blood glucose ≥126 mg/dL or haemoglobin A1c ≥6.5% without prior diagnosis of diabetes mellitus; (4) heart disease, as indicated by one of the following: history of myocardial infarction, documented disease on coronary angiography, coronary artery stent placement, congestive heart failure or significant structural heart disease; (5) hyperthyroid or hypothyroid by lab screening; (6) physically unable to perform PA for any reason; (7) pregnancy.
Methods of participant recruitment
Participants will be recruited through flyers and advertisements at partnering churches and community organisations in the target lower-resourced neighbourhoods. We will work with community partners in DC CHOC to promote community members’ participation, and encourage participants to invite friends and associates, especially those without current exercise routines. The National Institutes of Health (NIH) Intramural Institutional Review Board (IRB) approved this study and all participants will provide written informed consent (see online supplemental file 1), obtained with trained research staff, prior to participating in this study.
Supplemental material
Elements of the Step It Up mHealth PA intervention
mHealth app overview
All participants will receive a password-protected mobile app providing informational modules on the benefits of PA, potential barriers to PA and methods to overcome these barriers. The educational material within these modules is drawn from the Diabetes Prevention Programme curriculum, an evidence-based health behaviour change programme designed for individuals with insulin resistance, like Step It Up participants.43 The mobile app is linked to a wearable PA monitor, which assesses steps, sleep duration and heart rate; this data will inform custom daily messages encouraging participants to participate in PA (figure 3). Step goals will be based on a participant’s activity; each week, her step goal will be 110% of the prior week’s average daily step count, to a maximum of 10 000 steps.

Components of Step It Up app with (A) a dashboard featuring educational modules, daily motivational messages and awards, (B) a goal-setting page and (C, D) graphs to self-monitor physical activity (PA) and health metrics measured by Bluetooth-enabled PA monitor, scale, blood pressure cuff and glucometer. The app also includes a social forum, not pictured.
Participant randomisation
Prior to enrolment, research staff will assign each participant study number to one of the two starting interventions using computer-generated random numbers. The community research coordinator will enrol participants and assign a study number sequentially in order of enrolment. The research team and participants will not be blinded to the intervention or key outcomes.
Standard remote messaging
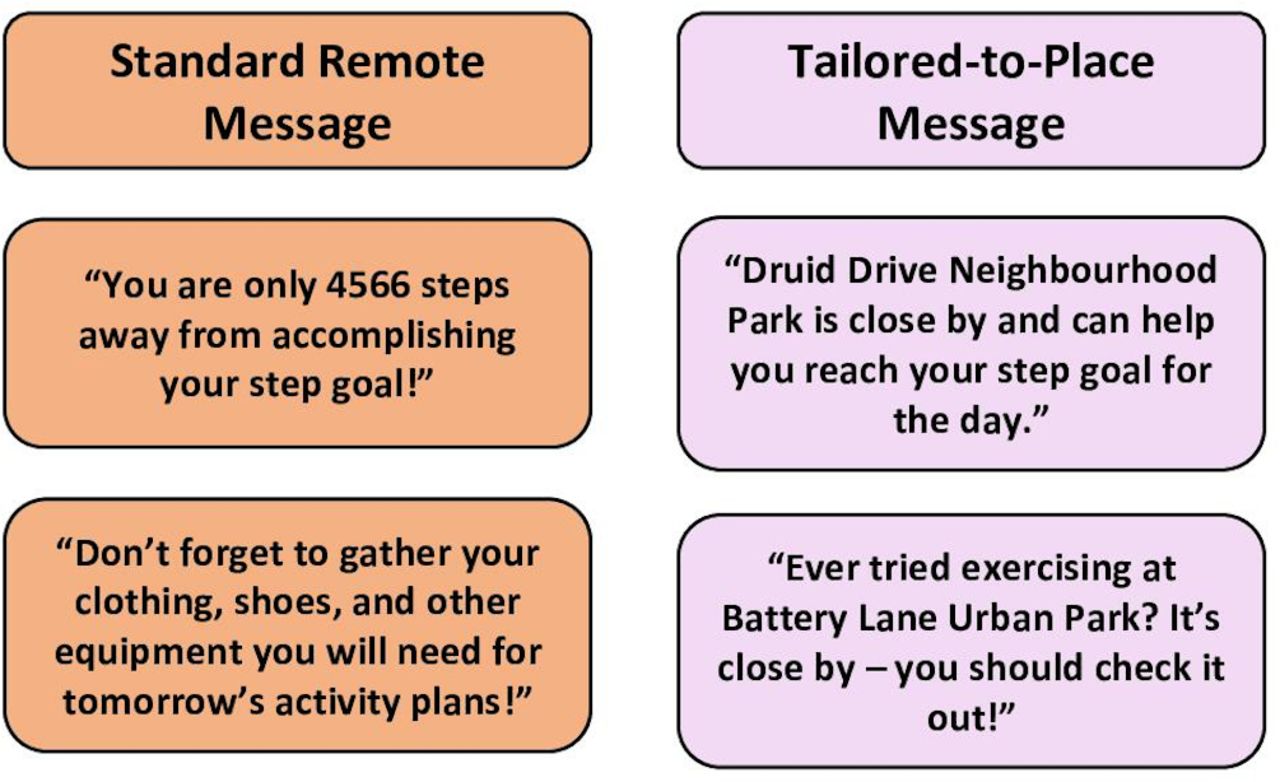
Participants randomised to SRM will receive the mHealth app with messages that promote PA by focusing on individual-level factors such as goal-setting and self-efficacy. Daily messaging was developed with input from the community advisory board, DC CHOC. A questionnaire was emailed to DC CHOC to solicit feedback about PA barriers, and members contributed motivational messaging promoting PA for the app. Their suggestions were followed up with phone interviews to further clarify and tailor messaging to AA women (figure 4), as described previously.38

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examples of standard remote messages, which are goal-based and time-based, in comparison to location-based tailored-to-place messages.
Remote TPM
Participants randomised to TPM will receive the same mHealth app, with different messaging based on the socioecological model (figure 1). This model considers each individual’s behaviour to be influenced by a variety of interrelated institutional, environmental and community factors, thereby emphasising the importance of environmental context in behaviour change. TPM will reference certain locations within the participants’ neighbourhood environment, in close proximity to her work, home or church, which are suitable for PA (figure 4). As such, although all participants will have access to the same educational modules and goal-setting tools within the mHealth app, the TPM group will also receive messaging tailored to PA resources within each participants’ activity space, or geographic region where they spend time. Specifically, our technology will use GPS to determine when a participant comes near a designated PA venue,44 and the app will generate a real-time, TPM to notify the participant of this venue and encourage PA.
Geofencing
TPM uses real-time geospatial location information of the participant and known PA locations within the region studied. The mobile app connects to a registry of public locations suitable for PA, including community recreation centres and parks, in addition to PA locations provided to us by the participants themselves. The registry was created through a detailed search for PA opportunities in the Washington, DC metropolitan area, followed by discussion with the community advisory board. The mobile app sets a geofence, or geographic boundary, in a 0.75 mile (approximately 1200 m44) radius around each PA venue. This distance was selected because it represents a 10–15 min walk.45 46 When the study participant enters this boundary at a time designated to receive a message, the app will generate a TPM.
PA and sleep monitoring
To objectively measure PA and sleep duration, each participant will be provided with a commercially available wireless PA and sleep monitoring wristband device (Fitbit Charge 2, Fitbit), and encouraged to wear this device 24 hours/day, except when bathing or immersed in water. This device will enable participants to self-monitor PA, including active minutes as determined by heart rate, step count and sleep duration for the entirety of the trial. The Fitbit was chosen due to user preference and validity in measuring outcome variables. Prior FG users particularly enjoyed the Fitbit compared with other wearable PA-monitors for its comfort, features and ease-of-use.34 38 The Fitbit is validated to reliably measure step count, heart rate and sleep duration, which are assessed in this study.47–49 The Step It Up mobile app will connect with the PA-monitor, allowing participants to track their PA and sleep through the app.
Mobile health tools
We will provide a subset (up to 25) of participants with a wireless blood pressure monitor, a weight scale and/or a blood glucose monitor throughout the study period to test the feasibility of using other mHealth tools to remotely monitor cardiometabolic markers. Each device will have capability for wireless data upload to participants’ smartphone and the Step It Up app. Participants with these devices will be encouraged to measure blood pressure, weight or blood glucose at least once per week using the device, but device use will be optional and at the discretion of the participant.
Strategies for adherence and retention
To promote adherence, we adjusted the intervention based on feedback from the community advisory board, the Washington, DC CHNA, and pilot testing. Data will be collected as available in cases of non-adherence. Our community research coordinator is a liaison between community members, study participants and the research team, who promotes enrolment and checks in with participants to encourage adherence. Financial compensation for continuous participation in the study and minimal clinic visits for participant convenience are intended to promote retention.
Outcome measures and evaluation
Survey data
A survey instrument will be administered with items focusing on health history, access and the behavioural, psychosocial, cultural and perceived environmental factors that may influence the impact of the intervention (see online supplemental table 2).61–67 This survey was used in the Washington, DC CHNA, and tailored to the needs of the target community using group-based cognitive interviewing.68 Each participant will complete this survey instrument on beginning the study.
Supplemental material
Neighbourhood data
Objective neighbourhood environment measures including Walk Score, Active Neighborhood Checklist and Neighborhood Deprivation Index69 are determined based on census data and participant-provided locations for home, work and place of worship (see online supplemental table 2).61–67
mHealth data
Data from Fitbit, including step count, minutes of vigorous activity and sleep time, will be transferred to the Step It Up app. If participants use elective mHealth devices (scale, blood glucose monitor, blood pressure cuff) data will be collected from the associated apps, including weight, blood glucose and blood pressure.
Clinical data
Participants’ health measures related to the study will be collected at clinic visits at baseline, 3-month and 6-month follow-up (table 1). Adverse health events will be monitored and recorded in accordance with IRB protocol. We will also collect blood samples to evaluate effects of PA changes on immune cells involved in CVD and the chronic stress response. Specifically, we will perform flow cytometry panels to (1) characterise the overall immune cell profile,70 (2) analyse monocyte subsets and receptor expression (known to be critically involved with atherogenesis)71–73 and (3) identify natural killer cell subsets (known to be deactivated with social stress and obesity).74 We will profile immunoregulating proteins from participants’ serum alongside stress-induced neurotransmitters and other proteins associated with CVD progression (table 1).70 75 76
Sample size calculation
Sample size calculations for this intervention are based on determining the main effect of the initial treatment in the adaptive design at 80% power and for a standardised mean-difference effect size of 0.5. An equal number in each initial treatment group being compared is assumed. The sample size formula assumes normality and uses the standard formulae from a Student’s t-test. Based on these assumptions, the intervention will require 126 participants. We will recruit 180 residents from the targeted neighbourhoods, of which we assume 30% will not meet study criteria and/or will be lost to follow-up during the run-in period.
Data analysis plan
The main objective is to test the primary hypothesis that an adaptive PA intervention with mobile app-based remote TPM will lead to greater PA levels than SRM over a 3-month period. To test this hypothesis, the daily step count from baseline to 6 months postrandomisation will be collected. An algorithm will examine minute-by-minute step count data from the PA monitor in blinded fashion to identify days when the PA monitoring device was not worn at all, worn for fewer than 10 hours/day, or was not working; those days will have missing values.77
A mean number of steps/day (Y) will be computed for each participant based on the available non-missing days for each week (T=−1 to T=26). If a subject is initially randomised to TPM, then A=1. If the subject is randomised to SRM, then A=0. If a subject with A=1 is rerandomised to TPM+face-to-face messaging, then B=1. If a subject with A=1 is rerandomised to TPM+increased messaging frequency, then B=−1. If a subject with A=0 is rerandomised to SRM+face-to-face messaging, then B=1. If a subject with A=0 is rerandomised to TPM, then B=−1. Otherwise, any subject not rerandomised has B=0 (see online supplemental table 3).
Supplemental material
Classify the subjects’ age at enrolment as AGE. We will fit the linear mixed model to the Y values (Y−1, Y0, Y1, …, Y26) using the function LME from the package NLME in R package V.3.178:

The effect of treatment for the primary comparison of TPM versus SRM is based on the fitted value of βA:T=13, the predicted model difference between the randomised arms will be at 13 weeks. We further hypothesise that, among TPM non-responders, face-to-face coaching will increase PA more than will increased messaging frequency. This comparison at 26 weeks is based on the fitted model as 2∙ βB:A=1,T=26. Further, we hypothesise that among SRM non-responders, SRM with face-to-face coaching will increase PA over TPM alone, based on the fitted model as 2∙ βB:A=0,T=26. Finally, at 26 weeks, contrasts will be constructed to estimate the differential effects of the four embedded treatment regime strategies. This comparison of embedded adaptive interventions is similar to the methods of Nahum-Shani et al.79
Sensitivity analyses will be performed to test for significant interactions between age and treatment, and if the relationship between Y, age and other covariates is non-linear. The distribution of cardiovascular health factors between randomisation groups using the χ2 test will be compared. We will also compare dietary intake and self-reported PA by psychosocial and environmental factors, including levels of social support, social isolation, perceived health, perceived spiritual locus of control and objective/perceived neighbourhood environment, using analysis of variance or Student’s t-test for continuous variables and χ2 testing for categorical variables.54–65
Patient and public involvement
The community advisory board, DC CHOC, consists of community leaders and potential participants. DC CHOC assisted in development of the research question, outcome measures and assessed the burden of the intervention through participation in DC CHNA. Community members (potential patients/participants) assisted with study design through FGs, iterative testing and reviewing intervention elements. DC CHOC advertised the study through partnering community organisations, and participants will be encouraged to recruit peers. Through the iterative process of developing the trial, we gathered feedback on the burden of the study from participants. Results and conclusions will be disseminated to participants and community members via a quarterly newsletter and presentations with DC CHOC.
Discussion
This novel mHealth PA intervention serves to better understand and reduce cardiovascular health disparities among AA women living in resource-limited communities.
Strengths
This intervention reaches an understudied population often left out from traditional healthcare models. The multilevel approach tailors the intervention to women living in and near Washington, DC by targeting the individual and neighbourhood levels; the goal is to help women shape perceptions about existing community resources and use their environment to increase PA.80 We established community partnerships and built on a strong foundation of preliminary community-based participatory research studies to ensure trust and collaboration with the community, which is essential for acceptance and success of the community intervention. We also leverage mHealth technology and Bluetooth-enabled devices to reach participants outside the scope of traditional medical settings. The bio-behavioural intervention design focuses on both clinical measures and biological mediators of cardiovascular health. Finally, the statistical approach for this study is unique from analyses of prior SMART-designed interventions and leverages the large quantity of PA data logged from the Fitbit device.
Limitations
Statistical power of the study was determined for the primary objective, to evaluate effects of TPM compared with SRM on PA, when delivered through mHealth technology. This study may be under-powered to evaluate changes in cardiovascular risk markers, but exploratory analyses will look for trends. If successful, we will consider a larger study powered to evaluate the impact of the technology-based intervention on BMI or waist-to-hip ratio as outcomes. We will also consider extending this study to other at-risk populations in Washington, DC, including AA men and other racial/ethnic groups, and to additional resource-limited, urban areas in the USA.
Ethics and dissemination
We submitted this proposed protocol to the National Heart, Lung and Blood Institute (NHLBI) IRB and received full approval for this study. All data will be stored securely, with password protection and encryption, in the electronic health system at the NIH, and will be shared only as needed with approved research personnel. All personal health information in the mHealth app, clinical information, survey and interview data will be de-identified. All biological specimens will be stored within a Food and Drug Administration-approved biospecimen tracking inventory system. Future use of biospecimens not defined in the research protocol will occur only after IRB review and approval, and participants may refuse to allow future use. This study is scheduled to start in 2021 with plans for completion by 2023. The COVID-19 pandemic, which likely alters activity space due to quarantine restrictions, has delayed enrolment. Further, geospatial data collected during the prepandemic pilot study can be compared with geospatial data in the protocol, to assess impact of the pandemic on activity space. Patients who suffer harm from trial participation will be treated according to best practices under the NIH Clinical Center. This study is low-risk, requiring no data-monitoring committee. The Principal Investigator will monitor accrual and safety data. The protocol will be reviewed and monitored annually by the IRB and the NHLBI Office of the Clinical Director’s Protocol Audit Team, with any amendments requiring IRB approval.
Results of this study will be analysed by the research team per IRB policy. Once publicly available, results and conclusions of the work will be shared with community members.
Acknowledgments
We acknowledge DC CHOC and all of the participants who have made this community-based research possible. This work was supported by the Division of Intramural Research of the National Heart, Lung, and Blood Institute and the Intramural Research Program of the National Institute on Minority Health and Health Disparities (National Institutes of Health). KT is supported by the 2019 Lenfant Biomedical Fellowship Award from the National Heart, Lung, and Blood Institute. Special thanks are given to RM and his staff (Dr Saxena and Dr Dagur) at the NHLBI Flow Cytometry Core. This research was also made possible by the National Institutes of Health (NIH) Medical Research Scholars Programme, a public–private partnership supported jointly by the NIH and generous contributions to the Foundation for the NIH from the Doris Duke Charitable Foundation, Genentech, the American Association for Dental Research, the Colgate-Palmolive Company, Elsevier, alumni of the student research programmes and other supporters via contributions to the Foundation for the National Institutes of Health. Additionally, this work was supported in part by the University of North Carolina at Chapel Hill’s Connected Health Applications & Interventions Core (CHAI Core) through a grant from NIH (DK056350) to the University of North Carolina Nutrition Obesity Research Center AND/OR from NCI (P30-CA16086) to the Lineberger Comprehensive Cancer Center.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
KT and NPV are joint first authors.
Twitter @nithyapv_
Contributors TP-W conceptualised the study. KT and NPV drafted the manuscript. KC, SJN, YB, CAG-H and BSC assisted in study design and revised the manuscript. VMM recruited participants and enrolled participants in this protocol and preceding works cited. TMPW designed the use of clinical data. YB, CAG-H, RI and BST performed all immune cell characterisation and biomarker profiling experiments. GRW, SL, PJM, TD and MD-B provided critical feedback on the concept and content. KGT, SG, RM and JZ developed the mHealth app. MA, JNC and SEC were involved in prior work for development of initial studies for the protocol and prior work cited. JFT contributed to statistical analyses and developed the unique statistical method applied. All authors contributed to study design, reviewed and approved the final draft of the manuscript.
Funding Funding for the Social Determinants of Obesity and Cardiovascular Risk Laboratory is provided through the Division of Intramural Research (DIR) of the NHLBI of the NIH, and through the Intramural Research Programme of the NIMHD of the NIH, under grant numbers ZIA-HL006168 and ZIA-MD000010.
Disclaimer The views of the present study are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute (NHLBI), the National Institute on Minority Health and Health Disparities (NIMHD), the National Institutes of Health (NIH) or the US Department of Health and Human Services.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.