Article Text

Abstract
Introduction Two-thirds of women with symptoms of angina have ‘angina with no obstructive coronary artery disease’ (ANOCA). Growing evidence supports the use of coronary artery function testing for the diagnosis of ANOCA. Research into the prevalence of mental stress-induced myocardial ischaemia (MSIMI) among women with ANOCA is lacking. MSIMI is common in clinically stable patients with coronary artery disease. It is not associated coronary stenosis but is a prognostic risk factor. Here, we describe the rationale and protocol for a mechanistic clinical trial to test the following hypotheses: (1) that MSIMI is more common in women with ANOCA women than in age-matched and sex-matched controls, and (2) MSIMI is associated with mental stress-induced myocardial blood flow (MBF) change but not with adenosine vasodilator stress-induced MBF change.
Methods and analysis This is a mechanistic clinical trial. 84 women with confirmed ANOCA and 42 aged-matched healthy women (neither angina symptoms nor coronary stenosis) are to be recruited for mental and adenosine vasodilator stress tests. Positron emission tomography CT with ammonia N-13 will be used to evaluate the myocardial perfusion and MBF changes between stress and rest. MSIMI is defined as a summed difference score (SDS) of ≥3 and adenosine stress-induced myocardial ischaemia is defined as an SDS of ≥4. Other assessments include Reactive Hyperemia Index for microvascular endothelial function, peripheral arterial tonometry or digital vasomotor response, and a series of blood and psychometric tests.
Ethics and dissemination This mechanistic clinical trial was approved by the Ethics Committee of Guangdong Provincial People’s Hospital. Findings will be disseminated through peer-reviewed publications and conference presentations.
Trial registration number NCT03982901; Pre-results.
- mental health
- coronary heart disease
- ischaemic heart disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to compare the occurrence of mental stress-induced myocardial ischaemia (MSIMI) in symptomatic women who have no significant coronary artery stenosis and women who have no symptoms, no coronary artery stenosis and few risk factors of cardiovascular disease.
This study will demonstrate characteristics of myocardial perfusion and myocardial blood flow with tests of mental stress versus adenosine vasodilator stress in women without coronary artery disease.
This study will demonstrate features of vascular reaction in face of mental stress.
Mental stress tasks are delivered via virtual reality devices which may not reflect naturally occurring real-life stressors.
This study is designed to include only women with angina have no obstructive coronary artery disease (ANOCA), so it is not known if findings are generalisable to men with ANOCA.
Introduction
Approximately two-thirds of women with angina have no obstructive coronary artery disease (ANOCA). The causes of ANOCA are multifactorial but women with ANOCA are known to have an increased risk of death or non-fatal myocardial infarction (MI).1 Due to lack of evidence-based guidelines, ANOCA is difficult to evaluate, diagnose and manage. There is increasing evidence to support the use of coronary artery function testing (exercise and vasodilator stress) for the diagnosis of ANOCA.2 Exercise-induced ischaemia is demand-induced ischaemia, where myocardial blood flow (MBF) is insufficient to meet myocardial demand due to restrictive coronary stenosis. Vasodilator stress-induced ischaemia is due to a global decrease in coronary flow reserve.
There is a significant interplay between mental stress and coronary artery disease (CAD) in women.3 Mental stress in clinical and real-life scenarios have been shown to trigger myocardial ischaemia.4 Mental stress-induced myocardial ischaemia (MSIMI) is common and associated with poor outcomes in clinically stable patients with CAD, with the risk of major adverse cardiovascular events over 4–5 years are 2.5 times higher than in controls.5 Previous MSIMI studies have focused on patients with stable obstructive coronary heart disease. Evidence of MSIMI among women with ANOCA is lacking.
The mechanisms of MSIMI are multifactorial and related to vasoconstriction possibly caused by abnormalities in endothelial function, autonomic nerve regulation and/or platelet aggregation.6 Using intracoronary Doppler, Yeung et al have previously demonstrated notable changes in coronary blood flow (−48% to +42%) during mental stress testing in a group of patients with CAD.7 Furthermore, Schöder et al reported MBF increases of ~30% during mental stress testing of participants without CAD, as measured by positron emission tomography (PET), while patients with CAD exhibited attenuated blood flow.8
Here, we report on the rationale and protocol for a mechanistic clinical trial, currently underway to evaluate the effect of mental stress in women with ANOCA. The main objectives of the study are to evaluate the incidence of MSIMI in women with ANOCA, as compared with age-matched and sex-matched controls, and to measure the changes in MBF during mental stress compared with adenosine vasodilator stress. We hope that studying the role of mental stress in ANOCA will provide a better understanding of the aetiology of angina and drive improvements in the treatment of ANOCA.
Methods and analysis
Study design
This study is currently taking place at the Guangdong Provincial People’s Hospital in Guangzhou, Guangdong, China. The study protocol and procedures were approved by the Ethics Committee at Guangdong Provincial People’s Hospital (number: GDREC2019298H(R3)). Eligible patients will be verbally educated on the nature and purpose of the study, and given time to decide whether or not to participate. Written informed consent will be obtained from study participants prior to their enrolment and all information will be treated as confidential.
Patients will be hospitalised for the duration of the study. All the laboratory tests will be conducted before 10:00 while the participants are fasting. After resting for 10 min in the supine position, the endothelial function test (EFT) at rest will be conducted. Following the EFT, the participants will rest for another 20 min and then complete a series of three mental stress tasks. At another day, the participants will receive adenosine stress test. All the stress tests will be conducted at the diagnostic PET-CT unit. Blood will be collected at rest, 5 min after the initiation of the mental stress test and 30 min after termination of the mental stress test. Blood will also be collected 24 and 72 hours after the mental stress test. Besides, peripheral vasoconstriction will be assessed at rest and during the mental stress test.
Patients
Female patients aged 18–75 years with angina symptoms but no obstructive CAD will be recruited. Age-matched women (control patients) without chest pain and coronary artery stenosis will be recruited from advertisement by WeChat, notice, internet and radio, not selected from a consecutive series. Control patients will complete a CT coronary angiogram to make sure they do not have obstructive CAD.
Key inclusion criteria include female sex, chest pain, aged 18–75 years and coronary artery stenosis less than 50%. Key exclusion criteria include male sex, chest pain caused by diseases other than the cardiac circulatory system, complications of other critical illnesses, such as pulmonary embolism, serious arrhythmias or aortic dissection, complications of severe valvular disease, a New York Heart Association Functional Classification IV, coronary artery obstructive MI within the past 1 month, apical ballooning syndrome within the past 1 month, substance abuse, such as alcohol and/or illicit drugs, use of antidepressants and/or antianxiety medicine in the 4 weeks prior to study enrollment, participation in other drug trials within the past 3 months, complications of severe mental illness, currently pregnant or breast feeding, current use of postmenopausal hormone therapy and current use of psychotropic drugs.
Cardiac drugs (including beta blockers and calcium channel blockers) that may interfere with stress tests are to be discontinued for 3–5 half-lives prior to study assessments. All patients will be asked if they have contraindications to adenosine, such as asthma or third-degree atrioventricular blockage (AVB). Patients must be haemodynamically and clinically stable for at least 48 hours before the study assessments begin. Any food or drugs containing caffeine must be discontinued at least 12 hours before the stress test. On the day of the study, patients with diabetes will be instructed to optimise their diet and insulin dosage.
Study procedures
Adenosine stress test
Two intravenous lines will be used to inject the radiopharmaceutical without interrupting the adenosine infusion. Adenosine will be infused with a syringe pump at a constant rate of 140 µg/kg/min for 6 min. Within the first 2–3 min, 700–900 MBq of 13NH3 (5 mL, a ‘bolus-like’ injection) will then be injected. For the patients at risk of complications (borderline hypotension, etc), a lower dose of 100–120 µg/kg/min will be infused. ECG and blood pressure monitoring will be carried out during the test. A 15-minute PET-CT image acquisition will be started after 13NH3 infusion. The total scan duration will be 15 min for rest and 15 min for the adenosine stress scans, with 30 min in between.
Vascular assessment
Peripheral vasoconstriction and microvascular function will be assessed using the Endo-PAT2000 (Itamar Medical), which measures the finger pulse volume amplitude (PVA) using volume plethysmography technology to reflect peripheral blood volume changes.9 Baseline average PVA will be determined during the 3 min preceding mental stress testing. The stress amplitude will be determined as the lowest PVA during the mental stress period. The peripheral arterial tonometry (PAT) ratio will be calculated as that of PVA during the mental stress period over baseline. A ratio <1 will signify a vasoconstrictive response. The EndoPAT device will be used to assess the Reactive Hyperemia Index (RHI) at rest and 30 min after the mental stress test to evaluate the peripheral microvascular function. For this test, the PVA will be obtained at rest and during reactive hyperemia elicited by the release of an upper arm blood pressure cuff inflated to suprasystolic pressure for 5 min. The RHI will then be calculated as the ratio of post deflation to the baseline pulse amplitude in the hyperemic finger divided by the ratio in the contralateral finger.
Mental stress test
Three mental stress tasks will be used in this study, administered consecutively using a virtual reality device. The night before the stress test, a researcher will teach each patient how to use the device and briefly describe the tasks.
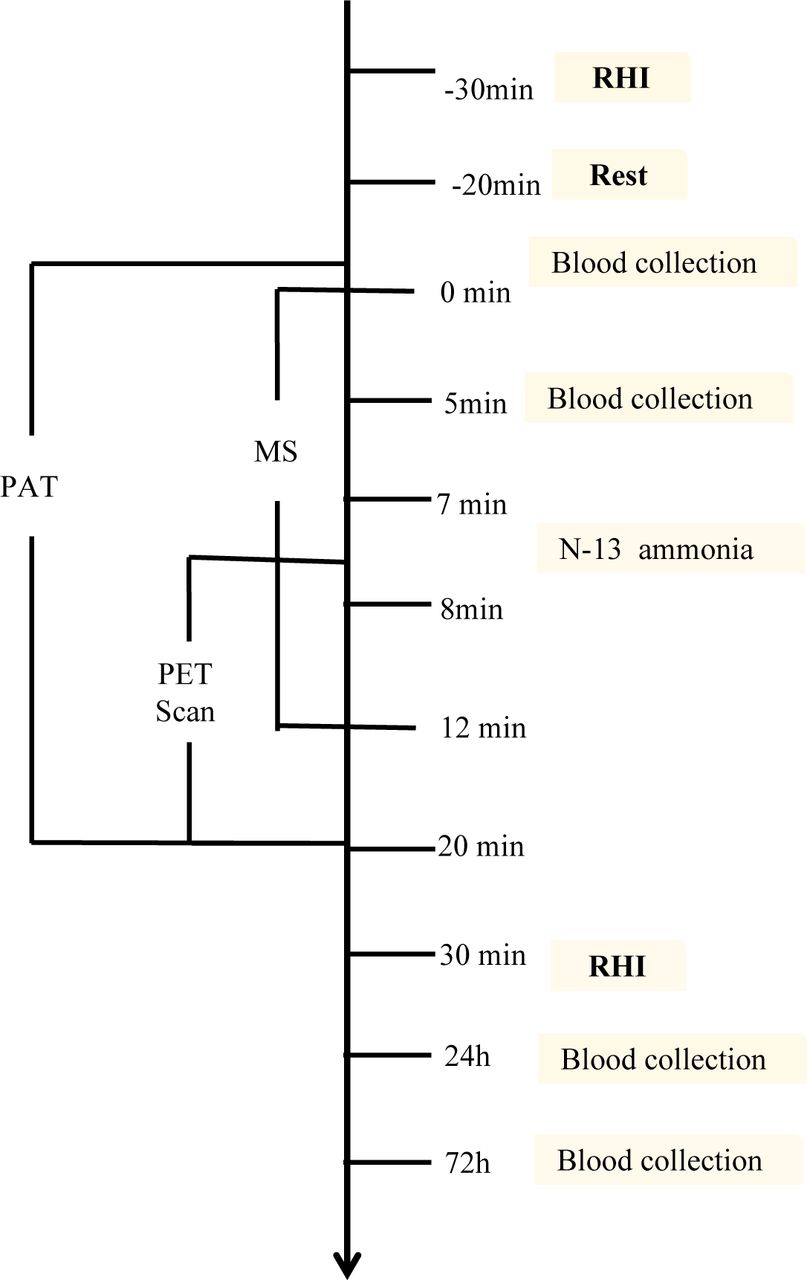
Each mental stress will last for 4 min without a break between tasks. The three mental tasks are: (1) the Stroop Color and Word Test; (2) a negative affect provoking event—patients will be asked to give a 3 min speech on a situation that has caused them anger, sadness or fear to three virtual reality doctors, after just 1 min of preparation time. Patients will be informed that their performance (eg, the clarity of their description, their thoughts and action and the result of the situation) will be evaluated. If they have nothing to say, the researchers will ask questions to obtain more information and complete the 3 min speech and (3) mental arithmetic test—patients will perform serial subtraction of 7 from a three-digit number, with encouragement to do the calculations as quickly as possible. The entire duration of the mental stress test will be 12 min. Seven minutes into the test, 700–900 MBq of 13NH3 (5 mL of 13NH3, a ‘bolus-like’ injection, followed by flushing with 10 mL of NaCl, 1 mCi=37 MBq) will be injected for PET scanning (figure 1).

{kind=link}
The process of mental stress test. MS, mental stress; PAT, peripheral arterial tonometry; PET, positron emission tomography; RHI, Reactive Hyperemia Index.
Criteria for terminating the stress tests
The test process will be supervised by qualified physicians. In addition to following the research protocol, they will have expertise in recognising signs of safety concerns and be certified in cardiopulmonary resuscitation.
Absolute termination criteria are a systolic blood pressure decrease ≥10 mm Hg in the presence of other signs suggestive of myocardial ischaemia; systolic blood pressure≥220 mm Hg; obvious angina pectoris; dizziness, presyncope or more severe neurological signs; cyanosis or paleness; ventricular tachycardia lasting more than 30 s; supraventricular tachyarrhythmia with negative haemodynamic effects; ST-segment elevation≥1 mm or depression>2 mm in two or more contiguous leads and patient’s request to terminate.
Relative termination criteria included a systolic blood pressure decreases ≥10 mm Hg without other signs of myocardial ischaemia; diastolic blood pressure>110 mm Hg; marked changes in the electrical axis (ie, ECG); second-degree or third-degree AVB; multifocal or frequent paired ventricular extrasystole and bradyarrhythmia.
Positron emission tomography CT
Images will be collected in list mode using a Siemens Biograph-16 TruePoint PET-CT (Siemens Healthcare, Knoxville, Tennessee, USA) with the TrueV option (a 21.6 cm axial field of view enabled). This three-dimensional system consists of a 16-slice CT, a PET scanner and four-ring lutetium orthosilicate detectors. After acquiring a topographic map (110 kVp and 25 mAs) for patient location, a CT transmission scan will be collected (130 kVp, 25 mAs (ref.) and pitch 0.95). Then, 700–900 MBq of 13NH3 (5 mL of 13NH3, ‘bolus-like’ injection, followed by flushing with 10 mL of NaCl, 1 mCi=37 MBq) will be injected into the patient and image acquisition will be completed over 20 min at rest.
After the stress imaging, a second CT transmission scan will be immediately performed (130 kVp, 25 mAs (ref.) and pitch 0.95). Static, dynamic and 16-bin ECG-gated images will be generated from the list mode data. The acquired emission data will be reconstructed using iterative reconstruction with a 168×168 matrix, zoom 2, a Gaussian filter with a full width at half-maximum of 5 mm, 2 iterations and 24 subsets for gated and dynamic images. CT-based attenuation, scatter, decay and random corrections will be applied to the reconstructed images. Dynamic, static and gated images will be reconstructed from each of the acquisitions. Dynamic rest images will be reconstructed from the part of the dataset that is acquired directly after the initiation of the first 13NH3 injection using 21 frames: 12×10, 6×30, 2×60 and 1×180 s. To reconstruct the gated and static rest images, the first 3 min of rest acquisition data will be skipped to allow for blood pool clearance and the subsequent 12 min of data will be used. Left ventricular ejection fraction and regional wall motion abnormalities will be assessed using the gated images, while myocardial perfusion will be analysed using the static images. The stress images will be reconstructed from the part of the dataset that is acquired from 30 s before initiation of the second 13NH3 injection (15 min after the beginning of each scan) and onwards using 21 frames for stress: 12×10, 6×30, 2×60 and 1×180 s. The last 12 and 17 min of the acquisition data will be used to reconstruct the gated stress and static images, respectively.
Perfusion evaluation
Images will be interpreted following the recommendations of the American Society of Nuclear Cardiology by two experienced readers blinded to the stress conditions (mental or adenosine).9 Before interpretation, errors such as patient movement, attenuation, reconstruction artefacts and low count density will be excluded. Perfusion will be calculated with commercially available and previously validated software (Cedars-Sinai software) using a 17-segment, 5-point scale (0=normal, 1=mildly reduced uptake, 2=moderately reduced uptake, 3=severely reduced uptake and 4=no uptake).
MBF evaluation
MBF (mL/min/g) will be automatically calculated at rest and under stress using Cedars-Sinai software and a two-compartment model.10 Myocardial flow reserve will be calculated as the ratio of stress MBF over rest MBF.11 All the images in this study will be analysed by two experienced readers blinded to the stress conditions and a consensus will be reached when there is disagreement.
Diagnostic MSIMI/pharmacological-induced myocardial ischaemia (PSIMI) criteria
MSIMI/PSIMI will be defined as new or worsening perfusion defects developing during the mental stress test compared with the resting baseline images. Using 99mTc-sestamibi myocardial perfusion imaging, a summed difference score (SDS) over the 17-segment model will be used to diagnose MSIMI/PSIMI, which is calculated based on the difference between the summed stress score and the summed rest score. MSIMI is defined as an SDS of ≥3.12 PSIMI is defined as an SDS of ≥4.13 In addition to using the SDS as the diagnostic criterion to evaluate the perfusion defects, the total perfusion deficit and ischaemia will also be used for assessment.
Haemodynamic measures and 12-lead ECG
Each patient’s blood pressure will be measured during the last 3 min of the 20 min calibration period, every minute during the 12 min mental stress test and 10–20 min after the mental stress test using a thigh sphygmomanometer (Tim Software, Beijing Co., Beijing, China). Standard 12-lead continuous ECG (Tim Software, Beijing Co., Beijing, China) monitoring will be conducted throughout the mental stress test. The patients’ heart rates and ST segments will be determined from their ECGs. Haemodynamic responses (systolic and diastolic blood pressure, heart rate and rate-pressure product) will be obtained by subtracting the mean level of the recorded values during the mental task from the baseline resting period. The difference in the blood pressure and heart rate from rest to each stress test will be considered the patient’s cardiovascular reactivity to the stress.
Blood collection and tests
On the day of the mental stress study, serial intravenous blood samples will be obtained at rest, 5 min after initiation of the mental stress test, 30 min after termination of the mental stress test and 24 and 72 hours after the mental stress test.
Blood collected at baseline, during the mental stress test and 30 min after will be analysed for cortisol, renin–angiotensin aldosterone system constituents, adrenocorticotropic hormone and thromboelastography. Blood collected at 24 hours will be analysed for hypersensitive troponin T, proteomics and metabolomics measurements. Blood collected at 72 hours will be analysed for proteomics and metabolomics measurements.
Supplemental analyses will be used to further examine our findings. We will evaluate the pathogenesis of MSIMI from the aspects of neuroendocrine mechanism, sex hormone level, the humoral immunity index and proteome expression.
Psychometric tests
Psychometric tests included the Canadian Angina Pectoris Scale (Canadian Cardiovascular Society (CCS) grade),14 Hospital Anxiety and Depression Scale,15 Eysenck Personality Scale,16 Stress Perception Scale (PSS-10),17 State-Trait Anxiety Inventory,18 Life Event Scale,19 Post-Traumatic Stress Disorder Checklist—Civilian Version20 and Type D Personality Scale (DS14).21
Primary and secondary outcomes
Our hypotheses are that: (1) MSIMI is more common in women with ANOCA than in age-matched and sex-matched controls, and (2) MSIMI is associated with changes in MBF that are not present under adenosine vasodilator stress.
All results were assessed in female patients with ANOCA and age-matched healthy women. Co-primary outcomes of the study are: (1) Percentage of participants with MSIMI during the three mental stress tests. The degree of perfusion will be scored from 0 to 4, with 0=normal, 1=possibly normal, 2=definitely abnormal, 3=severely abnormal and 4=no perfusion for each left ventricular segment. We will calculate the summed scores using a conventional method.22 The SDS will be yielded by the summed stress score minus the summed rest score. An SDS ≥3 will be defined as evidence of MSIMI. (2) Change in MBF via PET-CT during mental stress and adenosine vasodilator test.
Secondary outcomes include: (1) consistency of MBF and peripheral blood flow during mental stress test; (2) change in MBF during adenosine vasodilator stress and (3) explore the pathogenesis of MSIMI from the aspects of neuroendocrine mechanisms, sex hormone levels, the humoral immunity index and proteome expression.
Sample size considerations
Using pilot data, we estimate the incidence of MSIMI in women with ANOCA to be ~25%. With a 2:1 ratio of women with ANOCA and healthy controls, and assuming MSIMI incidence at 25% and a precision of 5%, a total of 126 patients (84 with ANOCA and 42 controls) will be required to achieve 0.80 power at p=0.05 using theχ2 test. To maximise the power to detect group differences, we will also use analysis of variance to compare continuous perfusion scores or MBF changes between the two groups of patients.
Patient and public involvement
The patients will be involved in several stages of this study. First, the content of the questionnaires and time required to complete them are discussed. The patients are also invited to provide written feedback on the informed consent form, information leaflet and information video. We will also discuss the mental stress test and cardiac PET-CT scan with the subjects.
Discussion
ANOCA is prevalent in women but aetiology of ANOCA remains poorly understood. A better understanding of the mechanism underlying ANOCA will likely to lead to improved diagnosis and treatment for patients. Here, we describe the protocol and rationale for an ongoing study that aims to assess the incidence of MSIMI in women with ANOCA and elucidate its association with mental stress-induced and adenosine-induced MBF changes. Furthermore, we aim to find out more about the mechanism behind ANOCA and MSIMI in these women. It is our belief that this is the first study specifically designed to address these aims.
Two previous studies have demonstrated that MSIMI may be common in patients with CAD without a flow-limiting atherosclerotic plaque.7 23 These studies suggest that vasoconstriction, but not the severity of CAD, is the main underlying mechanism of MSIMI, and that MSIMI may represent dynamic coronary artery occlusion. Mental stress, similar to other sympathetic stimuli, induces a release of catecholamines from cardiac nerve endings and the adrenal medulla to activate receptors in the circulation system. In healthy individuals, coronary blood flow increases due to mental stress as a result of coronary microvascular dilation. In patients with CAD, this response can be attenuated or there is vasoconstriction.24 Although vasomotor tone in patients with ANOCA during mental stress testing is unknown, we speculate that a subgroup of patients may develop coronary vascular constriction under mental stress due to sympathetic nervous system activation. Such coronary vascular constriction may be caused by endothelial dysfunction. Increased levels of circulating catecholamines associated with mental stress may also increase systemic vascular resistance.25 Therefore, a change in the digital artery pulse volume using PAT is also related to MSIMI. By comparing PET measured MBF and PAT, our study demonstrates that PAT may be a useful diagnostic tool for the identification of patients at risk of MSIMI.
Ethics and dissemination
The study protocol and procedures were approved by the Ethics Committee of Guangdong Provincial People’s Hospital (number: GDREC2019298H(R3)).
Eligible patients will be verbally informed, by trained research personnel, regarding the nature and purpose of the study, and given time to decide whether or not to participate. Written informed consent will be obtained from study participants prior to their enrolment and all collected information will be treated as confidential. We intend to present the results of our study via scientific publication (peer reviewed) as well as through presentation to stakeholders including the public, patients, clinicians and policymakers, via appropriate avenues.
Acknowledgments
The authors thank Professor Ling Li for her help in statistics.
References
Footnotes
HM and LG contributed equally.
Contributors HM, QG and WJ conceived and designed the study. LG and SW recruited the participants, drafted and revised the manuscript. HF, HY and HW made substantial contributions to the conception and design of the project. BB and YL managed the clinical practice organisation, and finished the statistical analysis. All the authors critically revised the manuscript for important intellectual content and provided approval of the final version to be published.
Funding This work was supported by the High-level Hospital Construction Project of Guangdong Provincial People’s Hospital (DFJH201811 and DFJH201922). The study was also supported by the grant 20201008 from Guangdong Provincial Bureau of Traditional Chinese Medicine, and grant A2020017 from Guangdong Medical Science and Technology Research Foundation, and grant Y012018085 from Guangdong Provincial People's Hospital Clinical Research Fund.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.